Is It Weird to Enjoy Solitude? Relationship of Solitude Capacity with Personality Traits and Physical and Mental Health in Junior College Students


Abstract
:1. Introduction
2. Materials and Methods
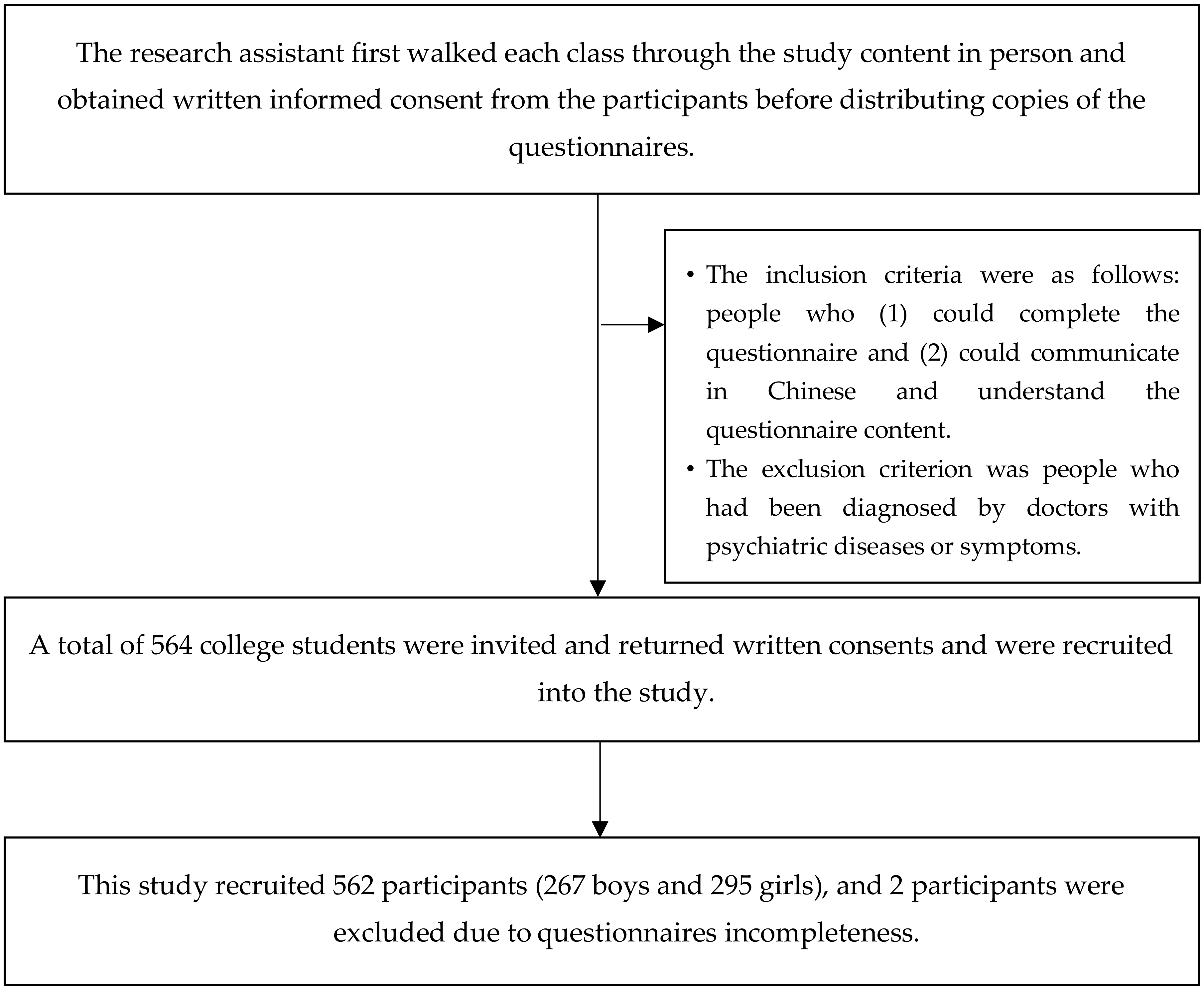
2.1. Study Participants
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Participants Demography
3.2. Pearson Correlation Coefficient Analysis
3.3. Multiple Regression Analysis
4. Discussion
4.1. Correlation between Solitude Capacity and Personality Traits
4.2. Correlations between Solitude Capacity and Physical and Mental Health
4.3. Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Larson, R.W.; Raffaelli, M.; Richards, M.H.; Ham, M.; Jewell, L. Ecology of depression in late childhood and early adolescence: A profile of daily states and activities. J. Abnorm. Psychol. 1990, 99, 92–102. [Google Scholar] [CrossRef]
- Larson, R.; Csikszentmihalyi, M.; Graef, R. Time alone in daily experience: Loneliness or renewal. In Loneliness: A Sourcebook of Current Theory, Research and Therapy; Wiley-Interscience: New York, NY, USA, 1982; pp. 40–53. [Google Scholar]
- Bruno, S.; Lutwak, N.; Agin, M.A. Conceptualizations of guilt and the corresponding relationships to emotional ambivalence, self-disclosure, loneliness and alienation. Personal. Individ. Differ. 2009, 47, 487–491. [Google Scholar] [CrossRef]
- Goosby, B.J.; Bellatorre, A.; Walsemann, K.M.; Cheadle, J.E. Adolescent loneliness and health in early adulthood. Sociol. Inq. 2013, 83, 505–536. [Google Scholar] [CrossRef] [PubMed]
- Cornwell, E.Y.; Waite, L.J. Social disconnectedness, perceived isolation, and health among older adults. J. Health Soc. Behav. 2009, 50, 31–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, T. Loneliness at Adolescence. Teoksessa LA Peplau & D. Perlman (toim.). In Loneliness: A Sourcebook of Current Theory, Research and Therapy; Wiley-Interscience: New York, NY, USA, 1982. [Google Scholar]
- Terrell-Deutsch, B. 2| The Conceptualization and Measurement. In Loneliness in Childhood and Adolescence; Cambridge University Press: New York, NY, USA, 1999; p. 11. [Google Scholar]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [Green Version]
- Goossens, L.; Marcoen, A. Adolescent Loneliness, Self-Reflection, and Identity: From Individual Differences to Developmental Processes; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Corsano, P.; Majorano, M.; Champretavy, L. Psychological well-being in adolescence: The contribution of interpersonal relations and experience of being alone. Adolescence 2006, 41, 341–354. [Google Scholar] [PubMed]
- Buchholz, E.S.; Catton, R. Adolescents’ perceptions of aloneness and loneliness. Adolescence 1999, 34, 203–204. [Google Scholar]
- Goossens, L.; Lasgaard, M.; Luyckx, K.; Vanhalst, J.; Mathias, S.; Masy, E. Loneliness and solitude in adolescence: A confirmatory factor analysis of alternative models. Personal. Individ. Differ. 2009, 47, 890–894. [Google Scholar] [CrossRef]
- Wang, J.M. Preference-for-solitude and depressive symptoms in Chinese adolescents. Personal. Individ. Differ. 2016, 100, 151–156. [Google Scholar] [CrossRef]
- Asendorpf, J.B.; Van Aken, M.A. Personality–relationship transaction in adolescence: Core versus surface personality characteristics. J. Personal. 2003, 71, 629–666. [Google Scholar] [CrossRef]
- Teppers, E.; Klimstra, T.A.; Damme, C.V.; Luyckx, K.; Vanhalst, J.; Goossens, L. Personality traits, loneliness, and attitudes toward aloneness in adolescence. J. Soc. Pers. Relatsh. 2013, 30, 1045–1063. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T. Personality in Adulthood: A Five-Factor Theory Perspective; Guilford Press: New York, NY, USA, 2003. [Google Scholar]
- Nestler, S.; Back, M.D.; Egloff, B. Psychometric properties of the two scales for assessing individual differences in preference for solitude. Diagnostica 2011, 57, 57–67. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C.; Ernst, J.M.; Burleson, M.; Berntson, G.G.; Nouriani, B.; Spiegel, D. Loneliness within a nomological net: An evolutionary perspective. J. Res. Personal. 2006, 40, 1054–1085. [Google Scholar] [CrossRef]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Personal. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef]
- Long, C.R.; Seburn, M.; Averill, J.R.; More, T.A. Solitude experiences: Varieties, settings, and individual differences. Personal. Soc. Psychol. Bull. 2003, 29, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.-T. Solitude Preference and Ability to Be Alone in Adolescent: The Moderating Effect of Mindfulness; Chung Yuan Christian University: Taoyuan, Taiwan, 2014. [Google Scholar]
- Savikko, N.; Routasalo, P.; Tilvis, R.S.; Strandberg, T.E.; Pitkälä, K.H. Predictors and subjective causes of loneliness in an aged population. Arch. Gerontol. Geriatr. 2005, 41, 223–233. [Google Scholar] [CrossRef]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef]
- Stickley, A.; Koyanagi, A.; Koposov, R.; Blatný, M.; Hrdlička, M.; Schwab-Stone, M.; Ruchkin, V. Loneliness and its association with psychological and somatic health problems among Czech, Russian and US adolescents. Bmc Psychiatry 2016, 16, 128. [Google Scholar] [CrossRef]
- Eccles, A.M.; Qualer, P.; Madsen, K.R.; Holstein, B.E. Loneliness in the lives of Danish adolescents: Associations with health and sleep. Scand. J. Public Health 2020. [Google Scholar] [CrossRef]
- Sharma, B.; Lee, T.H.; Nam, E.W. Loneliness, insomnia and suicidal behavior among school-going adolescents in Western Pacific Island countries: Role of violence and injury. Int. J. Environ. Res. Public Health 2017, 14, 791. [Google Scholar] [CrossRef] [Green Version]
- Sauter, S.R.; Kim, L.P.; Jacobsen, K.H. Loneliness and friendlessness among adolescents in 25 countries in Latin America and the Caribbean. Child Adolesc. Ment. Health 2020, 25, 21–27. [Google Scholar] [CrossRef]
- Zhou, J.; Li, X.; Tian, L.; Huebner, E.S. Longitudinal association between low self-esteem and depression in early adolescents: The role of rejection sensitivity and loneliness. Psychol. Psychother. Theory Res. Pract. 2020, 93, 54–71. [Google Scholar] [CrossRef] [PubMed]
- Okwaraji, F.E.; Obiechina, K.I.; Onyebueke, G.C.; Udegbunam, O.N.; Nnadum, G.S. Loneliness, life satisfaction and psychological distress among out-of-school adolescents in a Nigerian urban City. Psychol. Health Med. 2018, 23, 1106–1112. [Google Scholar] [CrossRef]
- De Oliveira Costa, R.P.; Peixoto, A.L.R.P.; Peixoto, C.C.A.L.; Falcão, D.N.; da Silva Farias, J.T.; Viana, L.F.P.; de Alencar Pereira, M.A.; Sandes, M.L.B.; Lopes, T.B.; Mousinho, K.C. Profile of non-suicidal self-injury in adolescents: Interface with impulsiveness and loneliness. J. Pediatr. 2020. [Google Scholar] [CrossRef]
- Herz, M.; Lalander, P. Being alone or becoming lonely? The complexity of portraying ‘unaccompanied children’as being alone in Sweden. J. Youth Stud. 2017, 20, 1062–1076. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.-C.; Chen, S.-F. Relationships among the Ability to be Alone, Subjective Life Stress and Mental Health in Junior gh School Students. Bull. Ofeducational Psychol. 2006, 38, 85–104. [Google Scholar]
- Larson, R.; Lee, M. The capacity to be alone as a stress buffer. J. Soc. Psychol. 1996, 136, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-T. A Study of Teacher’s Personality Traits Effect on Organizational Citizenship Behavior—Taking the Public Junior High Schools in Nantou County for Example; National Taiwan Normal University: Taipei, Taiwan, 2006. [Google Scholar]
- Hsieh, Y.-T. A Study on Singles’ Personality Traits and Capacity to be Alone toward Physical and Mental Health in Taipei Area; Chinese Culture University: Taipei, Taiwan, 2014. [Google Scholar]
- Chang, C. Study on University Entrance Examination Stress Syndrome. Taiwan J. Public Health 1987, 6, 43–55. [Google Scholar]
- Marquandt, D. You should standardize the predictor variables in your regression models. Discussion of: A critique of some ridge regression methods. J. Am. Stat. Assoc. 1980, 75, 87–91. [Google Scholar] [CrossRef]
- Creswell, K.G.; Chung, T.; Wright, A.G.; Clark, D.B.; Black, J.J.; Martin, C.S. Personality, negative affect coping, and drinking alone: A structural equation modeling approach to examine correlates of adolescent solitary drinking. Addiction 2015, 110, 775–783. [Google Scholar] [CrossRef] [Green Version]
- Amabile, T.M. Creativity in Context: Update to the Social Psychology of Creativity; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Yang, K.-S.; Lu, L. Social- and Individual-oriented Self-actualizers: Conceptual Analysis and Empirical Assessment of their Psychological Characteristics. Indig. Psychol. Res. Chin. Soc. 2005, 23, 71–143. [Google Scholar]
- Burger, J.M. Individual differences in preference for solitude. J. Res. Personal. 1995, 29, 85–108. [Google Scholar] [CrossRef]
- Larson, R.W. The solitary side of life: An examination of the time people spend alone from childhood to old age. Dev. Rev. 1990, 10, 155–183. [Google Scholar] [CrossRef]
- Storr, A. Solitude: A Return to the Self; Simon and Schuster: New York, NY, USA, 2005. [Google Scholar]
- Lasgaard, M.; Goossens, L.; Elklit, A. Loneliness, depressive symptomatology, and suicide ideation in adolescence: Cross-sectional and longitudinal analyses. J. Abnorm. Child Psychol. 2011, 39, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-Y.; Fu, S.-H.; Chen, K.-L.; Hsieh, P.-L.; Lin, P.-H. Relationships between depression, health-related behaviors, and internet addiction in female junior college students. PLoS ONE 2019, 14, e0220784. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.-Y.; Chen, K.-L.; Yang, S.-Y.; Lin, P.-H. Relationship of sleep quality, smartphone dependence, and health-related behaviors in female junior college students. PLoS ONE 2019, 14, e0214769. [Google Scholar] [CrossRef]
- Lin, P.-H.; Lee, Y.-C.; Chen, K.-L.; Hsieh, P.-L.; Yang, S.-Y.; Lin, Y.-L. The Relationship Between Sleep Quality and Internet Addiction Among Female College Students. Front. Neurosci. 2019, 13, 599. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Demographic Variables | Total |
|---|---|
| N = 562 | |
| Sex Male Female | 267 (47.5%) 295 (52.5%) |
| Age (mean ± SD) | 17.51 ± 1.27 |
| BMI (mean ± SD) | 20.68 ± 3.66 |
| Religion (n, %) | |
| No | 323 (57.5%) |
| Yes | 239 (42.5%) |
| Exercise per week 0–1 day 2–3 days ≥4 days | 296 (52.7%) 188 (33.5%) 78 (13.9%) |
| Money that can be spent each month | |
| <4000 NTD | 255 (45.4%) |
| 4000–5999 NTD | 136 (24.2%) |
| 6000–7999 NTD | 54 (9.6%) |
| ≥8000 NTD | 117 (20.8%) |
| Have a boy/girlfriend | |
| No Yes | 365 (64.9%) 197 (35.1%) |
| Living place | |
| Home | 381 (67.8%) |
| School dormitory | 54 (9.6%) |
| Off-campus rental house | 127 (22.6%) |
| Variable | Solitude Capacity Scale Total Score | Solitary Coping Subscale | Solitary Comfort Subscale |
|---|---|---|---|
| Personality Traits Scale | |||
| Neuroticism | −0.15 ** | −0.01 | −0.27 ** |
| Extraversion | −0.01 | −0.01 | −0.01 |
| Openness | 0.13 ** | 0.09 * | 0.15 ** |
| Agreeableness | 0.13 ** | 0.09 * | 0.16 ** |
| Conscientiousness | 0.16 ** | 0.17 ** | 0.12 ** |
| Physical and Mental Health Scale | |||
| Somatic symptoms | −0.08 * | −0.02 | −0.13 ** |
| Anxiety and Insomnia | −0.07 | 0.01 | −0.15 ** |
| Social dysfunction | −0.10 * | −0.03 | −0.15 ** |
| Severe depression | −0.12 ** | −0.06 | −0.16 ** |
| Independent Variable | Solitude Capacity Scale (Total Score) | |||||||
|---|---|---|---|---|---|---|---|---|
| R2 | Adjusted R2 | F | B | SE | Beta | 95% CI | p | |
| Personality Traits Scale | 0.11 | 0.09 | 5.00 | |||||
| Neuroticism | −0.19 | 0.06 | −0.14 | −0.31, −0.08 | <0.01 ** | |||
| Extraversion | −0.84 | 0.16 | −0.34 | −1.16, −0.53 | <0.01 ** | |||
| Openness | 0.35 | 0.18 | 0.11 | 0.00, 0.69 | 0.05 * | |||
| Agreeableness | 0.31 | 0.22 | 0.08 | −0.13, 0.74 | 0.17 | |||
| Conscientiousness | 0.63 | 0.15 | 0.28 | 0.34, 0.92 | <0.01 ** | |||
| Physical and Mental Health Scale | 0.04 | 0.02 | 1.78 | |||||
| Somatic symptoms | 0.02 | 0.14 | 0.01 | −0.27, 0.30 | 0.91 | |||
| Anxiety and Insomnia | 0.14 | 0.11 | 0.13 | −0.08, 0.36 | 0.22 | |||
| Social dysfunction | −0.11 | 0.15 | −0.07 | −0.41, 0.20 | 0.49 | |||
| Severe depression | −0.21 | 0.12 | −0.16 | −0.44, 0.03 | 0.09 | |||
| Independent Variable | Solitary Coping Subscale | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R2 | A R2 | F | B | SE | Beta | 95% CI | p | R2 | AR2 | F | B | SE | Beta | 95% CI | p | |
| Personality Traits Scale | 0.08 | 0.06 | 3.56 | 0.16 | 0.13 | 7.19 | ||||||||||
| Neuroticism | −0.01 | 0.03 | −0.02 | −0.08, 0.06 | 0.74 | −0.18 | 0.03 | −0.25 | −0.25, −0.12 | <0.01 ** | ||||||
| Extraversion | −0.41 | 0.09 | −0.30 | −0.59, −0.23 | <0.01 ** | −0.43 | 0.09 | −0.32 | −0.60, −0.27 | <0.01 ** | ||||||
| Openness | 0.09 | 0.10 | 0.05 | −0.10, 0.29 | 0.33 | 0.25 | 0.09 | 0.14 | 0.07, 0.43 | <0.01 ** | ||||||
| Agreeableness | 0.10 | 0.12 | 0.05 | −0.14, 0.35 | 0.40 | 0.20 | 0.12 | 0.10 | −0.03, 0.43 | 0.08 | ||||||
| Conscientiousness | 0.41 | 0.08 | 0.33 | 0.24, 0.57 | <0.01 ** | 0.23 | 0.08 | 0.19 | 0.08, 0.38 | <0.01 ** | ||||||
| Physical and Mental Health Scale | 0.03 | 0.01 | 1.44 | 0.06 | 0.04 | 2.60 | ||||||||||
| Somatic symptoms | 0.01 | 0.08 | 0.01 | −0.15, 0.16 | 0.95 | 0.01 | 0.08 | 0.01 | −0.14, 0.16 | 0.89 | ||||||
| Anxiety and Insomnia | 0.15 | 0.06 | 0.24 | 0.02, 0.27 | 0.02 * | −0.01 | 0.06 | −0.01 | −0.12, 0.11 | 0.91 | ||||||
| Social dysfunction | −0.06 | 0.09 | −0.08 | −0.23, 0.10 | 0.45 | −0.04 | 0.08 | −0.05 | −0.20, 0.12 | 0.61 | ||||||
| Severe depression | −0.14 | 0.07 | −0.20 | −0.27, −0.01 | 0.04 * | −0.07 | 0.07 | −0.10 | −0.20, 0.06 | 0.31 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, P.-H.; Wang, P.-Y.; Lin, Y.-L.; Yang, S.-Y. Is It Weird to Enjoy Solitude? Relationship of Solitude Capacity with Personality Traits and Physical and Mental Health in Junior College Students. Int. J. Environ. Res. Public Health 2020, 17, 5060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145060
Lin P-H, Wang P-Y, Lin Y-L, Yang S-Y. Is It Weird to Enjoy Solitude? Relationship of Solitude Capacity with Personality Traits and Physical and Mental Health in Junior College Students. International Journal of Environmental Research and Public Health. 2020; 17(14):5060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145060
Chicago/Turabian StyleLin, Pin-Hsuan, Po-Yu Wang, Ying-Lien Lin, and Shang-Yu Yang. 2020. "Is It Weird to Enjoy Solitude? Relationship of Solitude Capacity with Personality Traits and Physical and Mental Health in Junior College Students" International Journal of Environmental Research and Public Health 17, no. 14: 5060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145060