Return to Work and Quality of Life after Stroke in Italy: A Study on the Efficacy of Technologically Assisted Neurorehabilitation

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
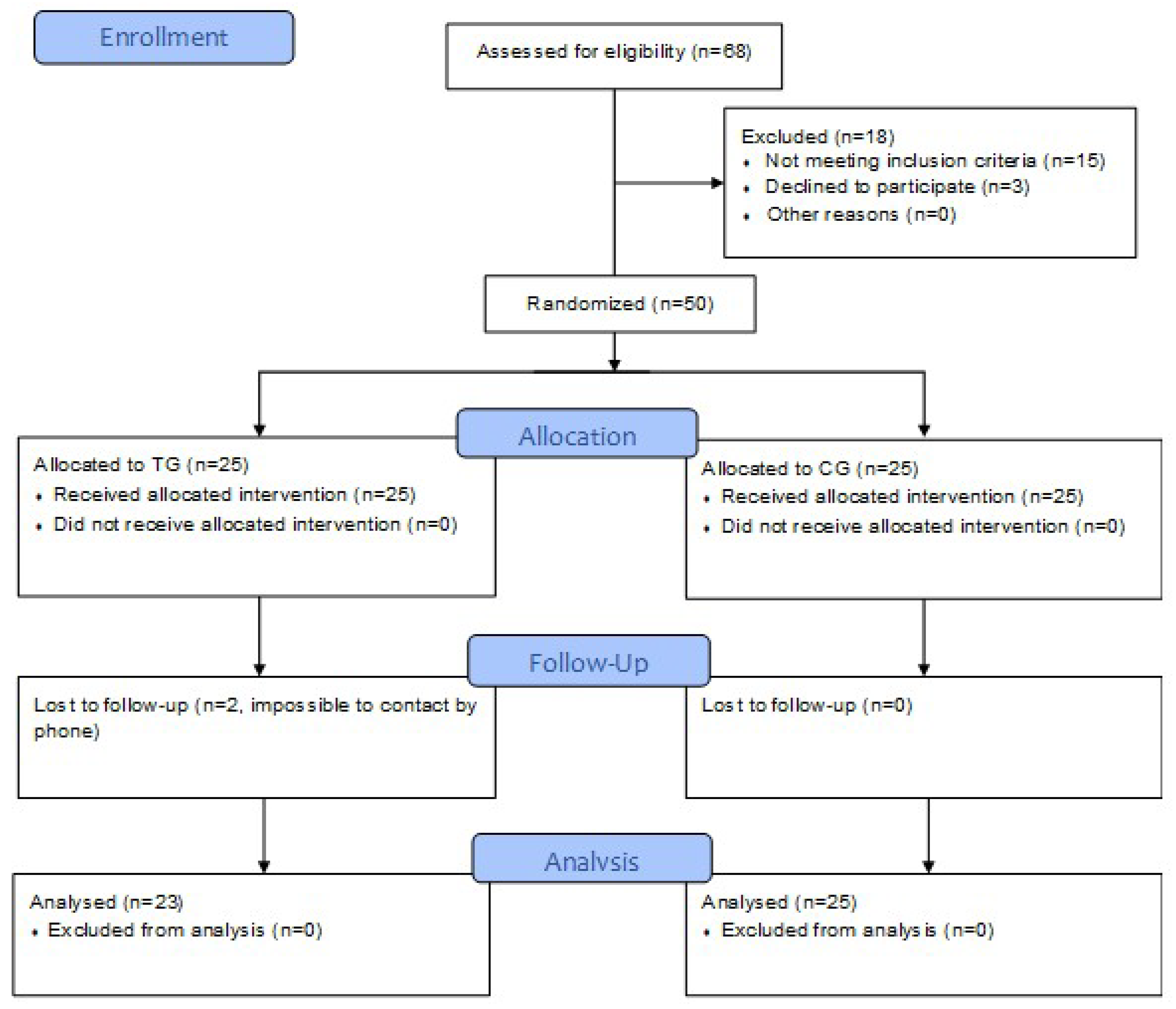
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Data Availability Statement
References
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef] [PubMed]
- Gallo, W.T.; Bradley, E.H.; Teng, H.M.; Kasl, S.V. The effect of recurrent involuntary job loss on the depressive symptoms of older US workers. Int. Arch. Occup. Environ. Health 2006, 80, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Edwards, J.D.; Kapoor, A.; Linkewich, E.; Swartz, R.H. Return to work after young stroke: A systematic review. Int. J. Stroke 2018, 13, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Treger, I.; Shames, J.; Giaquinto, S.; Ring, H. Return to work in stroke patients. Disabil. Rehabi. 2007, 29, 1397–1403. [Google Scholar] [CrossRef]
- Wolfenden, B.; Grace, M. Returning to work after stroke: A review. Int. J. Rehabil. Res. 2009, 32, 93–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, L.; Egbert, N.; Coeling, H.; Ayers, D. Returning to Work after the Onset of Illness: Experiences of Right Hemisphere Stroke Survivors. Rehabil. Couns. Bull. 2005, 48, 209–218. [Google Scholar] [CrossRef]
- Giaquinto, S.; Ring, H. Return to work in selected disabilities. Disabil. Rehabi 2007, 29, 1313–1316. [Google Scholar] [CrossRef]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Yue, Z.; Wang, J. Robotics in Lower-Limb Rehabilitation after Stroke. Behav. Neurol. 2017, 2017, 3731802. [Google Scholar] [CrossRef] [Green Version]
- Iosa, M.; Hesse, S.; Oliviero, A.; Paolucci, S. New technologies for stroke rehabilitation. Stroke Res. Treat. 2013, 2013, 815814. [Google Scholar] [CrossRef] [PubMed]
- Maceira-Elvira, P.; Popa, T.; Schmid, A.C.; Hummel, F.C. Wearable technology in stroke rehabilitation: Towards improved diagnosis and treatment of upper-limb motor impairment. J. Neuroeng. Rehabil. 2019, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Spitoni, G.F.; De Bartolo, D.; Ghanbari Ghooschchy, S.; Di Iulio, F.; Paolucci, S.; Zoccolotti, P.; Iosa, M. Rehabilitative devices for a top-down approach. Expert Rev. Med. Devices 2019, 16, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Belluscio, V.; Bergamini, E.; Iosa, M.; Tramontano, M.; Morone, G.; Vannozzi, G. The iFST: An instrumented version of the Fukuda Stepping Test for balance assessment. Gait Posture 2018, 60, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Belluscio, V.; Bergamini, E.; Tramontano, M.; Orejel Bustos, A.; Allevi, G.; Formisano, R.; Vannozzi, G.; Buzzi, M.G. Gait Quality Assessment in Survivors from Severe Traumatic Brain Injury: An Instrumented Approach Based on Inertial Sensors. Sensors 2019, 19, 5315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergamini, E.; Iosa, M.; Belluscio, V.; Morone, G.; Tramontano, M.; Vannozzi, G. Multisensor assessment of dynamic balance during gait in patients with subacute stroke. J. Biomech. 2017, 61, 208–215. [Google Scholar] [CrossRef]
- Tramontano, M.; Bergamini, E.; Iosa, M.; Belluscio, V.; Vannozzi, G.; Morone, G. Vestibular rehabilitation training in patients with subacute stroke: A preliminary randomized controlled trial. NeuroRehabilitation 2018, 43, 247–254. [Google Scholar] [CrossRef]
- Raglio, A.; Zaliani, A.; Baiardi, P.; Bossi, D.; Sguazzin, C.; Capodaglio, E.; Imbriani, C.; Gontero, G.; Imbriani, M. Active music therapy approach for stroke patients in the post-acute rehabilitation. Neurol. Sci. 2017, 38, 893–897. [Google Scholar] [CrossRef]
- Morone, G.; Tramontano, M.; Iosa, M.; Shofany, J.; Iemma, A.; Musicco, M.; Paolucci, S.; Caltagirone, C. The efficacy of balance training with video game-based therapy in subacute stroke patients: A randomized controlled trial. Biomed. Res. Int. 2014, 2014, 580861. [Google Scholar] [CrossRef] [Green Version]
- Lupo, A.; Cinnera, A.M.; Pucello, A.; Iosa, M.; Coiro, P.; Personeni, S.; Gimigliano, F.; Iolascon, G.; Paolucci, S.; Morone, G. Effects on balance skills and patient compliance of biofeedback training with inertial measurement units and exergaming in subacute stroke: A pilot randomized controlled trial. Funct. Neurol. 2018, 33, 131–136. [Google Scholar]
- Li, C.; Rusák, Z.; Horváth, I.; Ji, L. Influence of complementing a robotic upper limb rehabilitation system with video games on the engagement of the participants: A study focusing on muscle activities. Int. J. Rehabil. Res. 2014, 37, 334–342. [Google Scholar] [CrossRef]
- Colombo, R.; Raglio, A.; Panigazzi, M.; Mazzone, A.; Bazzini, G.; Imarisio, C.; Molteni, D.; Caltagirone, C.; Imbriani, M. The SonicHand Protocol for Rehabilitation of Hand Motor Function: A validation and feasibility study. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Prasad, K.; Kumar, A.; Misra, S.; Yadav, A.K.; Johri, S.; Sarkar, R.S.; Gorthi, S.P.; Hassan, K.M.; Prabhakar, S.; Misra, U.K.; et al. Reliability and validity of telephonic Barthel Index: An experience from multi-centric randomized control study. Acta Neurol. Belg. 2018, 118, 53–59. [Google Scholar] [CrossRef]
- Lungenhausen, M.; Lange, S.; Maier, C.; Schaub, C.; Trampisch, H.j.; Endres, H.G. Randomised controlled comparison of the Health Survey Short Form (SF-12) and the Graded Chronic Pain Scale (GCPS) in telephone interviews versus self-administered questionnaires. Are the results equivalent? BMC Med. Res. Methodol. 2007, 7, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apolone, G.; Mosconi, P.; Quattrociocchi, L. Questionario Sullo Stato di Salute SF-12. Versione Italiana; Guerini e Associati Editore: Milan, Italy, 2005; p. 85. ISBN 8883352017. [Google Scholar]
- Galeoto, G.; Colucci, M.; Guarino, D.; Esposito, G.; Cosma, E.; De Santis, R.; Grifoni, G.; Valente, D.; Tofani, M. Exploring Validity, Reliability, and Factor Analysis of the Quebec User Evaluation of Satisfaction with Assistive Technology in an Italian Population: A Cross-Sectional Study. Occup Ther Health Care 2018, 32, 380–392. [Google Scholar] [CrossRef] [PubMed]
- Wessels, R.; Persson, J.; Lorentsen, O.; Andrich, R.; Ferrario, M.; Oortwijn, W.; VanBeekum, T.; Brodin, H.; de Witte, L. IPPA: Individually Prioritised Problem Assessment. Technol. Disabil. 2002, 14, 141–145. [Google Scholar] [CrossRef]
- Wozniak, M.A.; Kittner, S.J. Return to work after ischemic stroke: A methodological review. Neuroepidemiology 2002, 21, 159–166. [Google Scholar] [CrossRef]
- Wang, Y.C.; Kapellusch, J.; Garg, A. Important factors influencing the return to work after stroke. Work 2014, 47, 553–559. [Google Scholar] [CrossRef]
- Lindstrom, B.; Roding, J.; Sundelin, G. Positive attitudes and preserved high level of motor performance are important factors for return to work in younger persons after stroke: A national survey. J. Rehabil. Med. 2009, 41, 714–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Toyonaga, T.; Hashimoto, H. Functional and occupational characteristics predictive of a return to work within 18 months after stroke in Japan: Implications for rehabilitation. Int. Arch. Occup. Environ. Health 2014, 87, 445–453. [Google Scholar] [CrossRef] [Green Version]
- Singam, A.; Ytterberg, C.; Tham, K.; von Koch, L. Participation in complex and social everyday activities six years after stroke: Predictors for return to pre-stroke level. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Barker-Collo, S.; Feigin, V.L.; Parag, V.; Lawes, C.M.M.; Senior, H. Auckland stroke outcomes study. part 2: Cognition and functional outcomes 5 years poststroke. Neurology 2010, 75, 1608–1616. [Google Scholar] [CrossRef]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masiero, S.; Armani, M.; Rosati, G. Upper-limb robot-assisted therapy in rehabilitation of acute stroke patients: Focused review and results of new randomized controlled trial. J. Rehabil. Res. Dev. 2011, 48, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Masiero, S.; Coiro, P.; De Angelis, D.; Venturiero, V.; Paolucci, S.; Iosa, M. Clinical features of patients who might benefit more from walking robotic training. Restor. Neurol. Neurosci. 2018, 36, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Morone, G.; Cherubini, A.; Paolucci, S. The Three Laws of Neurorobotics: A Review on What Neurorehabilitation Robots Should Do for Patients and Clinicians. J. Med. Biol. Eng. 2016, 36, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morone, G.; Bragoni, M.; Iosa, M.; De Angelis, D.; Venturiero, V.; Coiro, P.; Pratesi, L.; Paolucci, S. Who may benefit from robotic-assisted gait training? A randomized clinical trial in patients with subacute stroke. Neurorehabil. Neural Repair 2011, 25, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Iosa, M.; Bragoni, M.; De Angelis, D.; Venturiero, V.; Coiro, P.; Riso, R.; Pratesi, L.; Paolucci, S. Who may have durable benefit from robotic gait training? A 2-year follow-up randomized controlled trial in patients with subacute stroke. Stroke 2012, 43, 1140–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolucci, S.; Iosa, M.; Toni, D.; Barbanti, P.; Bovi, P.; Cavallini, A.; Candeloro, E.; Mancini, A.; Mancuso, M.; Monaco, S.; et al. Neuropathic pain special interest group of the Italian Neurological Society. Prevalence and Time Course of Post-Stroke Pain: A Multicenter Prospective Hospital-Based Study. Pain Med 2016, 17, 924–930. [Google Scholar] [CrossRef]
- Iosa, M.; Lupo, A.; Morone, G.; Baricich, A.; Picelli, A.; Panza, G.; Smania, N.; Cisari, C.; Sandrini, G.; Paolucci, S. Post Soft Care: Italian implementation of a post-stroke checklist software for primary care and identification of unmet needs in community-dwelling patients. Neurol. Sci. 2018, 39, 135–139. [Google Scholar] [CrossRef]
- Han, J.; Lee, H.I.; Shin, Y.-I.; Son, J.H.; Kim, S.-Y.; Kim, D.Y.; Sohn, M.K.; Lee, J.; Lee, S.-G.; Oh, G.-J.; et al. Factors influencing return to work after stroke: The Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) Study. BMJ Open 2019, 9, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bragoni, M.; Broccoli, M.; Iosa, M.; Morone, G.; De Angelis, D.; Venturiero, V.; Coiro, P.; Pratesi, L.; Mezzetti, G.; Fusco, A.; et al. Influence of psychologic features on rehabilitation outcomes in patients with subacute stroke trained with robotic-aided walking therapy. Am. J. Phys. Med. Rehabil. 2013, 92, e16–e25. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographical and Clinical Data | TG (N = 23) | CG (N = 25) | p-Value | Riablo (N = 10) | SonicHand (N = 13) | p-Value | Test |
|---|---|---|---|---|---|---|---|
| Age (years) | 51.0 ± 11.8 | 52.5 ± 10.5 | 0.648 | 47.5 ± 9.1 | 54.0 ± 13.3 | 0.221 | t-test |
| Months from stroke | 27.0 ± 13.2 | 21.7 ± 12.2 | 0.156 | 26.6 ± 6.5 | 27.0 ± 16.9 | 0.902 | t-test |
| Male sex | 14 (60.9%) | 17 (68.0%) | 0.606 | 7 (70%) | 7 (53.8%) | 0.431 | χ2-test |
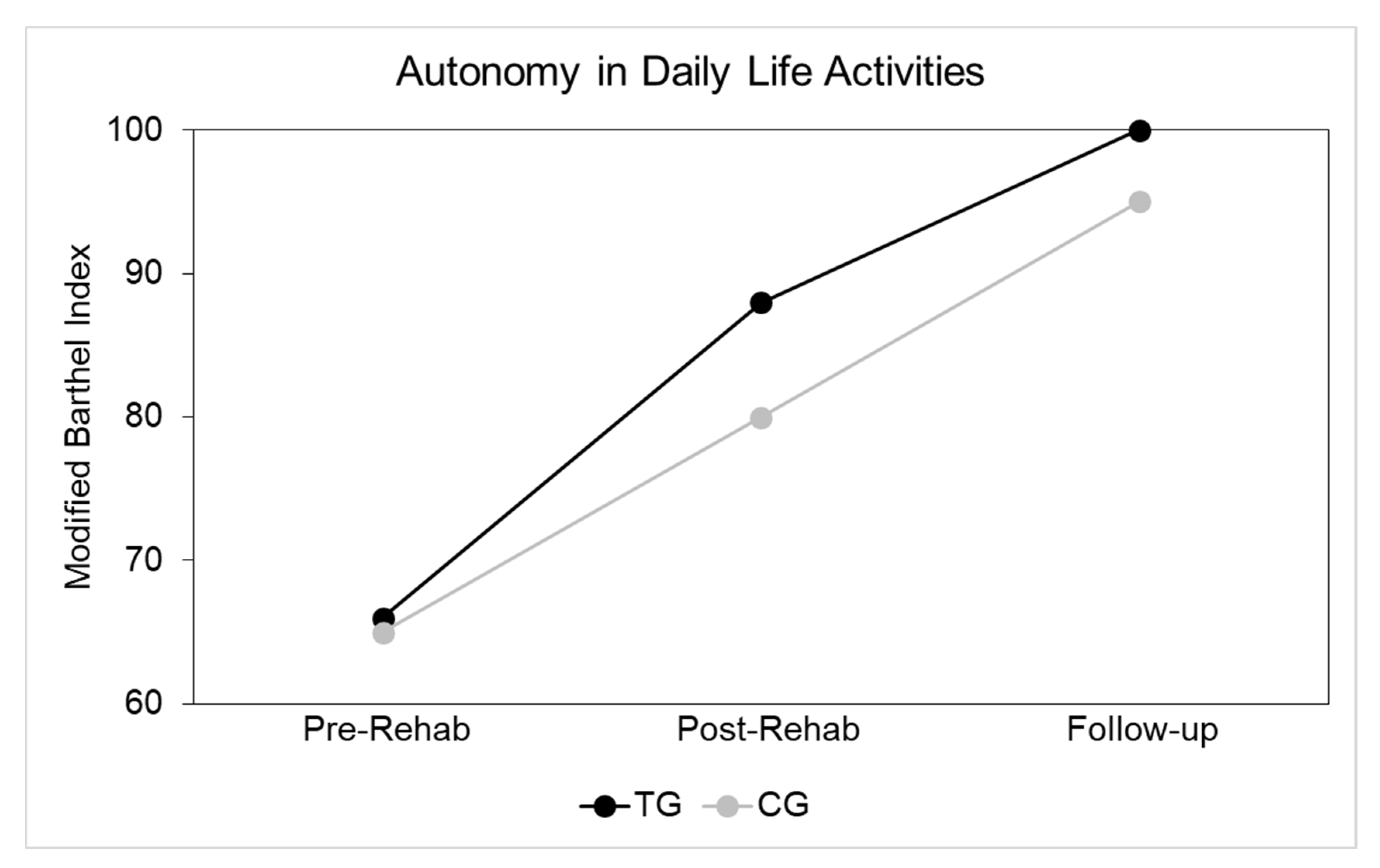
| MBI Pre-Rehab | 66 (41;78) | 65 (19; 75) | 0.793 | 79 (74; 82) | 45 (25; 60) | 0.002 | u-test |
| MBI Post-Rehab | 88 (72;98) | 80 (65; 90) | 0.391 | 98 (95; 100) | 80 (65; 87) | 0.005 | u-test |
| MBI follow-up | 100 (82;100) | 95 (85;100) | 0.450 | 100 (100; 100) | 90 (65; 100) | 0.016 | u-test |
| SF-12 total | 94 (83;106) | 97 (84; 104) | 0.543 | 104 (87; 109) | 92 (75; 109) | 0.343 | u-test |
| SF-12 physical | 47 (39;54) | 43 (36; 49) | 0.190 | 48 (45; 53) | 43 (31; 54) | 0.563 | u-test |
| SF-12 mental | 51 (42;58) | 58 (48; 59) | 0.599 | 55 (47; 59) | 50 (38; 56) | 0.284 | u-test |
| P. with assistive devices | 5 (21.7%) | 8 (32.0%) | 0.424 | 2 (20%) | 3 (23.1%) | 0.859 | χ2-test |
| QUEST 1 (N = 13) | 4.7 (4.4;5.0) | 4.8 (4; 4.8) | 0.602 | 4.7 (4.6; 4.9) | 4.7 (4.6; 4.9) | 0.767 | u-test |
| QUEST 2 (N = 13) | 5 (0.0;5.0) | 2.5 (0; 4.6) | 0.194 | 2.4 (1.2; 3.6) | 5 (5; 5) | 0.053 | u-test |
| IPPA 1 (N = 13) | 20 (19;23.3) | 23 (18.4;25.0) | 0.303 | 19.5 (19.2;19.7) | 20 (15; 21.6) | 0.767 | u-test |
| IPPA 2 (N = 13) | 10 (8;10.5) | 15 (10.5; 20) | 0.107 | 11.5 (11.2;11.7) | 7 (6.8; 8.5) | 0.083 | u-test |
| IPPA Difference (N = 13) | 8.0 (5.0;10) | 7.8 (5; 10.2) | 0.605 | 8 (8; 8) | 10 (6.5;13.3) | 0.554 | u-test |
| P. with fall events | 5 (21.7%) | 4 (16.0%) | 0.611 | 0 (0%) | 5 (38.5%) | 0.026 | χ2-test |
| Return to Work | 11 (47.8%) | 9 (36.0%) | 0.406 | 7 (70%) | 4 (30.8%) | 0.062 | χ2-test |
| Demographical and Clinical Data | Entire Sample | Returned to Work | Not Returned to Work | p-Value | Test |
|---|---|---|---|---|---|
| Number of subjects | 48 | 20 (42%) | 28 (58%) | 0.248 | χ2-test |
| Age (years) | 51.8 ± 11.1 | 53.9 ± 8.6 | 50.3 ± 12.5 | 0.264 | t-test |
| Time from stroke (months) | 24.2 ± 12.8 | 25.6 ± 12.0 | 23.2 ± 13.5 | 0.528 | t-test |
| Male sex | 31 (64.6%) | 13 (65.0%) | 18 (64.3%) | 0.959 | χ2-test |
| MBI follow-up | 100 (91;100) | 100 (100;100) | 100 (70;100) | 0.018 | u-test |
| SF-12 total | 96 (83;107) | 100 (87;109) | 93 (77; 105) | 0.143 | u-test |
| SF-12 physical | 45 (36;51) | 48 (44; 55) | 43 (33; 48) | 0.009 | u-test |
| SF-12 mental | 52 (42;59) | 53 (41; 59) | 52 (43; 58) | 0.983 | u-test |
| Patients with assistive devices | 13 (27.1%) | 1 (5.0%) | 12 (42.8%) | 0.004 | χ2-test |
| QUEST 1 (N = 13) | 4.7 (4.1;5.0) | 4.8 | 4.7 (4.4;5) | 0.683 | u-test |
| QUEST 2 (N = 13) | 4.5 (0.0;5.0) | 0 | 4.6 (0.7;5) | 0.209 | u-test |
| IPPA 1 (N = 13) | 20 (17.8;24.1) | 25 | 20 (18.4;23.3) | 0.227 | u-test |
| IPPA 2 (N = 13) | 11.3 (7.5;18.9) | 20 | 11.2 (7.7;13.7) | 0.228 | u-test |
| IPPA Difference (N = 13) | 8.0 (5.0;10.5) | 5 | 8.0 (7.0;10.3) | 0.346 | u-test |
| Patients with fall events | 9 (18.7%) | 2 (10.0%) | 7 (25.0%) | 0.189 | χ2-test |
| Technological treatment | 23 (47.9%) | 11 (55.0%) | 12 (42.9%) | 0.406 | χ2-test |
| Return to Work Data | Entire Sample of Returned to Work | Technological Treatment Group | Conventional Treatment Group | p-Value | Test |
|---|---|---|---|---|---|
| Number of subjects | 20 | 11 | 9 | 0.655 | χ2-test |
| Working Hours | 32.6 ± 9.3 | 33.7 ± 9.0 | 31.1 ± 10.1 | 0.552 | χ2-test |
| People with any kind of adaptation | 9 (45.0%) | 4 (36.4%) | 5 (55.5%) | 0.888 | χ2-test |
| People with job adaptation | 4 (20.0%) | 1 (9.1%) | 3 (33.3%) | 0.391 | χ2-test |
| People with time adaptation | 7 (35.0%) | 4 (36.4%) | 3 (33.3%) | 0.178 | χ2-test |
| People with tools adaptation | 0 (0%) | 0 (0%) | 0 (0%) | - | - |
| People with assistive devices | 1 (5.0%) | 0 (0%) | 1 (11.1%) | 0.257 | χ2-test |
| Dependent Variable | Variables into the Model | OR | p-Value | CI95% | Explained Variance | Variables out of the Model |
|---|---|---|---|---|---|---|
| Return to work | MBI f-up | 7.5 | 0.002 | 2.04; 27.59 | 72.9% | Age: p = 0.527 Gender: p = 0.805 Treatment: p = 0.728 Time from stroke: p = 0.610 MBI pre-R: =0.128 MBI post-R = 0.740 |
| SF-12 Total score | Work as before (job type and time) | 6.6 | 0.026 | 1.2; 34.9 | 64.6% | Age: p = 0.459 Treatment: p = 0.449 Time from stroke: p = 0.174 Gender: p = 0.497 Return to work: p = 0.613 MBI pre-R: p = 0.331 MBI post-R: p = 0.269 MBI f-up: p = 0.383 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghanbari Ghoshchi, S.; De Angelis, S.; Morone, G.; Panigazzi, M.; Persechino, B.; Tramontano, M.; Capodaglio, E.; Zoccolotti, P.; Paolucci, S.; Iosa, M. Return to Work and Quality of Life after Stroke in Italy: A Study on the Efficacy of Technologically Assisted Neurorehabilitation. Int. J. Environ. Res. Public Health 2020, 17, 5233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145233
Ghanbari Ghoshchi S, De Angelis S, Morone G, Panigazzi M, Persechino B, Tramontano M, Capodaglio E, Zoccolotti P, Paolucci S, Iosa M. Return to Work and Quality of Life after Stroke in Italy: A Study on the Efficacy of Technologically Assisted Neurorehabilitation. International Journal of Environmental Research and Public Health. 2020; 17(14):5233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145233
Chicago/Turabian StyleGhanbari Ghoshchi, Sheyda, Sara De Angelis, Giovanni Morone, Monica Panigazzi, Benedetta Persechino, Marco Tramontano, Edda Capodaglio, Pierluigi Zoccolotti, Stefano Paolucci, and Marco Iosa. 2020. "Return to Work and Quality of Life after Stroke in Italy: A Study on the Efficacy of Technologically Assisted Neurorehabilitation" International Journal of Environmental Research and Public Health 17, no. 14: 5233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145233