Urinary Metals Concentrations and Biomarkers of Autoimmunity among Navajo and Nicaraguan Men

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Analysis of Urinary Metals
2.3. Laboratory Analysis of Biomarkers of Autoimmunity
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
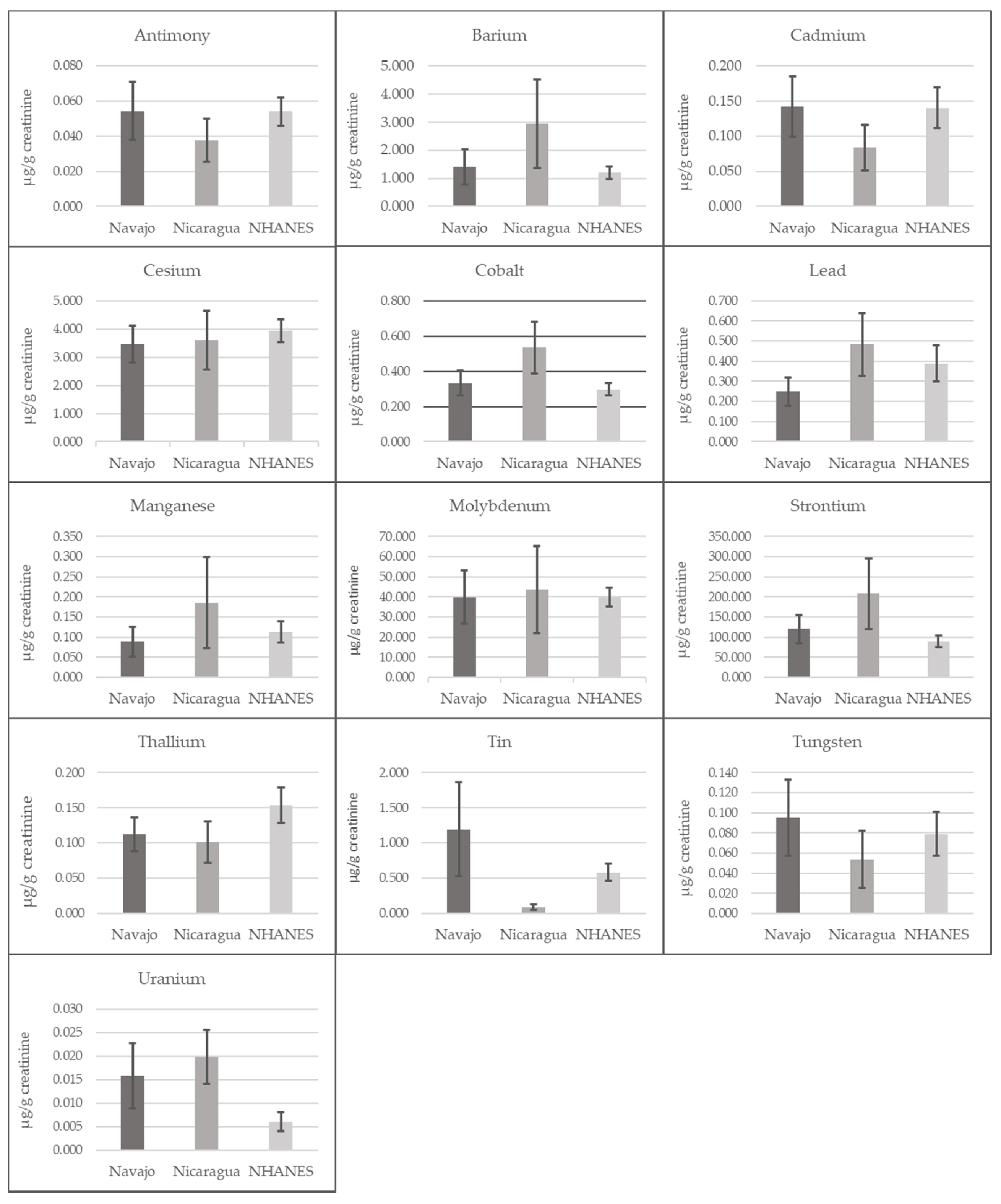
3.2. Urinary Metals
3.3. Autoimmune Biomarkers
3.4. Associations between Metals and ANA Positivity in Pooled Analyses (Table 3)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- National Institutes of Health. Report of the Director—National Institutes of Health: Fiscal Years 2014–2015; National Institutes of Health: Bethesda, MD, USA, 2013; pp. 1–322.
- Peschken, C.A.; Esdaile, J.M. Systemic lupus erythematosus in North American Indians: A population based study. J. Rheumatol. 2000, 27, 8. [Google Scholar]
- Morton, R.O.; Gershwin, M.E.; Brady, C.; Steinberg, A.D. The incidence of systemic lupus erythematosus in North American Indians. J. Rheumatol. 1976, 3, 186–190. [Google Scholar] [PubMed]
- Boyer, G.S.; Templin, D.W.; Lanier, A.P. Rheumatic diseases in Alaskan Indians of the southeast coast: High prevalence of rheumatoid arthritis and systemic lupus erythematosus. J. Rheumatol. 1991, 18, 1477–1484. [Google Scholar] [PubMed]
- Palmer Beasley, R.; Willkens, R.F.; Bennett, P.H. High prevalence of rheumatoid arthritis in yakima indians. Arthritis Rheum. 1973. [Google Scholar] [CrossRef]
- Harvey, J.; Lotze, M.; Stevens, M.B.; Lambert, G.; Jacobson, D. Rheumatoid arthritis in a Chippewa Band. I. Pilot screening study of disease prevalence. Arthritis Rheum. 1981. [Google Scholar] [CrossRef]
- Del Puente, A.; Knowler, W.C.; Pettitt, D.J.; Bennett, P.H. High incidence and prevalence of rheumatoid arthritis in pima Indians. Am. J. Epidemiol. 1989. [Google Scholar] [CrossRef]
- National Institutes of Health. Progress in Autoimmune Diseases Research. Available online: https://www.niaid.nih.gov/sites/default/files/adccfinal.pdf (accessed on 20 July 2020).
- Hopkinson, N.D.; Doherty, M.; Powell, R.J. Clinical features and race-specific incidence/prevalence rates of systemic lupus erythematosus in a geographically complete cohort of patients. Ann. Rheum. Dis. 1994, 53, 675–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapira, Y.; Agmon-Levin, N.; Shoenfeld, Y. Defining and analyzing geoepidemiology and human autoimmunity. J. Autoimmun. 2010. [Google Scholar] [CrossRef] [PubMed]
- Pollard, K.M. Environment, autoantibodies, and autoimmunity. Front. Immunol. 2015, 6, 60. [Google Scholar] [CrossRef] [Green Version]
- Arbuckle, M.R.; McClain, M.T.; Rubertone, M.V.; Hal Scofield, R.; Dennis, G.J.; James, J.A.; Harley, J.B. Development of autoantibodies before the clinical onset of systemic lupus erythematosus. N. Engl. J. Med. 2003. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, C.; Kokkonen, H.; Johansson, M.; Hallmans, G.; Wadell, G.; Rantapää-Dahlqvist, S. Autoantibodies predate the onset of systemic lupus erythematosus in northern Sweden. Arthritis Res. Ther. 2011. [Google Scholar] [CrossRef] [Green Version]
- Koenig, M.; Dieudé, M.; Senécal, J.L. Predictive value of antinuclear autoantibodies: The lessons of the systemic sclerosis autoantibodies. Autoimmun. Rev. 2008, 7, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Kronbichler, A.; Mayer, G. Renal involvement in autoimmune connective tissue diseases. BMC Med. 2013, 11, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinse, G.E.; Jusko, T.A.; Whitt, I.Z.; Co, C.A.; Parks, C.G.; Satoh, M.; Chan, E.K.L.; Rose, K.M.; Walker, N.J.; Birnbaum, L.S.; et al. Associations between selected xenobiotics and antinuclear antibodies in the national health and nutrition examination survey, 1999–2004. Environ. Health Perspect. 2016. [Google Scholar] [CrossRef]
- Yubin, Z.; Lawrence, D.A. Metals and Autoimmunity. In Encyclopedia of Immunotoxicology; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Leffel, E.K.; Wolf, C.; Poklis, A.; White, K.L. Drinking water exposure to cadmium, an environmental contaminant, results in the exacerbation of autoimmune disease in the murine model. Toxicology 2003. [Google Scholar] [CrossRef]
- Hudson, C.A.; Cao, L.; Kasten-Jolly, J.; Kirkwood, J.N.; Lawrence, D.A. Susceptibility of lupus-prone NZM mouse strains to lead exacerbation of systemic lupus erythematosus symptoms. J. Toxicol. Environ. Health Part A 2003. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.M.; Nyland, J.F.; Silva, I.A.; Ventura, A.M.; de Souza, J.M.; Silbergeld, E.K. Mercury exposure, serum antinuclear/antinucleolar antibodies, and serum cytokine levels in mining populations in Amazonian Brazil: A cross-sectional study. Environ. Res. 2010, 110, 345–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamycheva, E.; Goto, T.; Camargo, C.A. Blood levels of lead and mercury and celiac disease seropositivity: The US National Health and Nutrition Examination Survey. Environ. Sci. Pollut. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Marie, I.; Gehanno, J.F.; Bubenheim, M.; Duval-Modeste, A.B.; Joly, P.; Dominique, S.; Bravard, P.; Noël, D.; Cailleux, A.F.; Benichou, J.; et al. Systemic sclerosis and exposure to heavy metals: A case control study of 100 patients and 300 controls. Autoimmun. Rev. 2017. [Google Scholar] [CrossRef]
- Das, N.; Paul, S.; Chatterjee, D.; Banerjee, N.; Majumder, N.S.; Sarma, N.; Sau, T.J.; Basu, S.; Banerjee, S.; Majumder, P.; et al. Arsenic exposure through drinking water increases the risk of liver and cardiovascular diseases in the population of West Bengal, India. BMC Public Health 2012. [Google Scholar] [CrossRef] [PubMed]
- Recalcati, S.; Locati, M.; Gammella, E.; Invernizzi, P.; Cairo, G. Iron levels in polarized macrophages: Regulation of immunity and autoimmunity. Autoimmun. Rev. 2012, 11, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Pollard, K.M.; Hultman, P.; Kono, D.H. Toxicology of autoimmune diseases. Chem. Res. Toxicol. 2010, 23, 455–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, M.P.; Piconese, S. Regulatory T-cell inhibition versus depletion: The right choice in cancer immunotherapy. Nat. Rev. Cancer 2007, 7, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.W.; Alfredsson, L.; Costenbader, K.H.; Kamen, D.L.; Nelson, L.M.; Norris, J.M.; de Roos, A.J. Epidemiology of environmental exposures and human autoimmune diseases: Findings from a National Institute of Environmental Health Sciences Expert Panel Workshop. J. Autoimmun. 2012, 39, 259–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parks, C.G.; Miller, F.W.; Pollard, K.M.; Selmi, C.; Germolec, D.; Joyce, K.; Rose, N.R.; Humble, M.C. Expert panel workshop consensus statement on the role of the environment in the development of autoimmune disease. Int. J. Mol. Sci. 2014, 15, 14269–14297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, Y.; Peng, R.D.; Jones, M.R.; Francesconi, K.A.; Goessler, W.; Howard, B.V.; Umans, J.G.; Best, L.G.; Guallar, E.; Post, W.S.; et al. Metal mixtures in urban and rural populations in the US: The Multi-Ethnic Study of Atherosclerosis and the Strong Heart Study. Environ. Res. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EPA. Federal actions to address impacts of uranium contamination in the Navajo Nation: Five-year plan summary report. In Uranium Contamination in the Navajo Nation: Background and Cleanup Efforts; EPA: San Francisco, CA, USA, 2014; ISBN 9781633217102. [Google Scholar]
- Hoover, J.; Gonzales, M.; Shuey, C.; Barney, Y.; Lewis, J. Elevated arsenic and uranium concentrations in unregulated water sources on the Navajo Nation, USA. Expo. Health 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, J.; Hoover, J.; MacKenzie, D. Mining and Environmental Health Disparities in Native American Communities. Curr. Environ. Health Rep. 2017, 4, 130–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, J.; Erdei, E.; Rubin, R.L.; Miller, C.; Ducheneaux, C.; O’Leary, M.; Pacheco, B.; Mahler, M.; Henderson, P.N.; Pollard, K.M.; et al. Mercury, autoimmunity, and environmental factors on Cheyenne River Sioux Tribal lands. Autoimmune Dis. 2014. [Google Scholar] [CrossRef] [Green Version]
- Erdei, E.; Shuey, C.; Pacheco, B.; Cajero, M.; Lewis, J.; Rubin, R.L. Elevated autoimmunity in residents living near abandoned uranium mine sites on the Navajo Nation. J. Autoimmun. 2019. [Google Scholar] [CrossRef] [PubMed]
- McClintock, T.R.; Chen, Y.; Bundschuh, J.; Oliver, J.T.; Navoni, J.; Olmos, V.; Lepori, E.V.; Ahsan, H.; Parvez, F. Arsenic exposure in Latin America: Biomarkers, risk assessments and related health effects. Sci. Total Environ. 2012, 429, 76–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora, P. Outdoor and indoor dose assessment using environmental thermoluminescence dosimeters (TLDs) in Costa Rica. J. Radiol. Prot. 2003. [Google Scholar] [CrossRef] [PubMed]
- Queirolo, F.; Stegen, S.; Restovic, M.; Paz, M.; Ostapczuk, P.; Schwuger, M.J.; Muñoz, L. Total arsenic, lead, and cadmium levels in vegetables cultivated at the Andean villages of northern Chile. Sci. Total Environ. 2000. [Google Scholar] [CrossRef]
- Reagan, M.K.; Morris, J.D.; Herrstrom, E.A.; Murrell, M.T. Uranium series and beryllium isotope evidence for an extended history of subduction modification of the mantle below Nicaragua. Geochim. Cosmochim. Acta 1994. [Google Scholar] [CrossRef]
- Velasquez-Pereira, J.; McDowell, L.R.; Wilkinson, N.S. Soil, forage, and serum nutrient changes as affected by deposition of volcanic sediments in northwestern Nicaragua. Commun. Soil Sci. Plant Anal. 1996. [Google Scholar] [CrossRef]
- López, D.L.; Bundschuh, J.; Birkle, P.; Armienta, M.A.; Cumbal, L.; Sracek, O.; Cornejo, L.; Ormachea, M. Arsenic in volcanic geothermal fluids of Latin America. Sci. Total Environ. 2012. [Google Scholar] [CrossRef]
- Wijkström, J.; González-Quiroz, M.; Hernandez, M.; Trujillo, Z.; Hultenby, K.; Ring, A.; Söderberg, M.; Aragón, A.; Elinder, C.G.; Wernerson, A. Renal Morphology, Clinical Findings, and Progression Rate in Mesoamerican Nephropathy. Am. J. Kidney Dis. 2017. [Google Scholar] [CrossRef] [Green Version]
- Wijkström, J.; Leiva, R.; Elinder, C.G.; Leiva, S.; Trujillo, Z.; Trujillo, L.; Söderberg, M.; Hultenby, K.; Wernerson, A. Clinical and pathological characterization of mesoamerican nephropathy: A new kidney disease in central america. Am. J. Kidney Dis. 2013. [Google Scholar] [CrossRef]
- Narva, A.S. The spectrum of kidney disease in American Indians. Kidney Int. 2003, 63, S3–S7. [Google Scholar] [CrossRef] [Green Version]
- Hund, L.; Bedrick, E.J.; Miller, C.; Huerta, G.; Nez, T.; Ramone, S.; Shuey, C.; Cajero, M.; Lewis, J. A Bayesian framework for estimating disease risk due to exposure to uranium mine and mill waste on the Navajo Nation. J. R. Stat. Soc. Ser. A Stat. Soc. 2015. [Google Scholar] [CrossRef]
- Correa-Rotter, R.; Wesseling, C.; Johnson, R.J. CKD of unknown origin in Central America: The case for a mesoamerican nephropathy. Am. J. Kidney Dis. 2014, 63, 506–520. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Rubio, O.; McClean, M.D.; Amador, J.J.; Brooks, D.R. An epidemic of chronic kidney disease in Central America: An overview. J. Epidemiol. Community Health 2013, 67, 1–3. [Google Scholar] [CrossRef]
- Laws, R.L.; Brooks, D.R.; Amador, J.J.; Weiner, D.E.; Kaufman, J.S.; Ramírez-Rubio, O.; Riefkohl, A.; Scammell, M.K.; López-Pilarte, D.; Sánchez, J.M.; et al. Changes in kidney function among Nicaraguan sugarcane workers. Int. J. Occup. Environ. Health 2015, 21, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Laboratory Procedure Manual Method No. 3018.6-01, 3018A.4-01. Available online: https://www.cdc.gov/Nchs/Data/Nhanes/Nhanes_13_14/UM_UMS_UTAS_UTASS_H_met_HEAVY_METALS_TOTAL_ARSENIC.pdf (accessed on 20 July 2020).
- Verdon, C.P.; Caldwell, K.L.; Fresquez, M.R.; Jones, R.L. Determination of seven arsenic compounds in urine by HPLC-ICP-DRC-MS: A CDC population biomonitoring method. Anal. Bioanal. Chem. 2009. [Google Scholar] [CrossRef] [PubMed]
- Tonutti, E.; Bizzaro, N.; Morozzi, G.; Radice, A.; Cinquanta, L.; Villalta, D.; Tozzoli, R.; Tampoia, M.; Porcelli, B.; Fabris, M.; et al. The ANA-reflex test as a model for improving clinical appropriateness in autoimmune diagnostics. Autoimmun. Highlights 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baglaenko, Y.; Chang, N.H.; Johnson, S.R.; Hafiz, W.; Manion, K.; Ferri, D.; Noamani, B.; Bonilla, D.; Rusta-Sellehy, S.; Lisnevskaia, L.; et al. The presence of anti-nuclear antibodies alone is associated with changes in B cell activation and T follicular helper cells similar to those in systemic autoimmune rheumatic disease. Arthritis Res. Ther. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akmatov, M.K.; Röber, N.; Ahrens, W.; Flesch-Janys, D.; Fricke, J.; Greiser, H.; Günther, K.; Kaaks, R.; Kemmling, Y.; Krone, B.; et al. Anti-nuclear autoantibodies in the general German population: Prevalence and lack of association with selected cardiovascular and metabolic disorders-findings of a multicenter population-based study. Arthritis Res. Ther. 2017. [Google Scholar] [CrossRef] [Green Version]
- Silvy, F.; Bertin, D.; Bardin, N.; Auger, I.; Guzian, M.C.; Mattei, J.P.; Guis, S.; Roudier, J.; Balandraud, N. Antinuclear antibodies in patients with psoriatic arthritis treated or not with biologics. PLoS ONE 2015. [Google Scholar] [CrossRef] [Green Version]
- Hollingsworth, P.N.; Dawkins, R.L.; Peter, J.B. Precise quantitation of antinuclear antibodies on HEp-2 cells without the need for serial dilution. Clin. Diagn. Lab. Immunol. 1996. [Google Scholar] [CrossRef] [Green Version]
- Burlingame, R.W.; Rubin, R.L. Subnucleosome structures as substrates in enzyme-linked immunosorbent assays. J. Immunol. Methods 1990. [Google Scholar] [CrossRef]
- Burlingame, R.W.; Rubin, R.L. Enzyme-Linked Immunosorbent Assays for Diagnostically Important Antinuclear Antibodies; Rose, N.R., Hamilton, R.G., Detric, B., Eds.; American Society for Microbiology: Washington, DC, USA, 2002. [Google Scholar]
- Tan, E.M.; Feltkamp, T.E.W.; Smolen, J.S.; Butcher, B.; Dawkins, R.; Fritzler, M.J.; Gordon, T.; Hardin, J.A.; Kalden, J.R.; Lahita, R.G.; et al. Range of antinuclear antibodies in “healthy” individuals. Arthritis Rheum. 1997. [Google Scholar] [CrossRef]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary creatinine concentrations in the U.S. population: Implications for urinary biologic monitoring measurements. Environ. Health Perspect. 2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Fourth National Report on Human Exposure to Environmental Chemicals. Available online: https://www.cdc.gov/biomonitoring/pdf/fourthreport_updatedtables_feb2015.pdf (accessed on 20 July 2020).
- Navas-Acien, A.; Francesconi, K.A.; Silbergeld, E.K.; Guallar, E. Seafood intake and urine concentrations of total arsenic, dimethylarsinate and arsenobetaine in the US population. Environ. Res. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheer, J.; Findenig, S.; Goessler, W.; Francesconi, K.A.; Howard, B.; Umans, J.G.; Pollak, J.; Tellez-Plaza, M.; Silbergeld, E.K.; Guallar, E.; et al. Arsenic species and selected metals in human urine: Validation of HPLC/ICPMS and ICPMS procedures for a long-term population-based epidemiological study. Anal. Methods 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, M.; Shah, V.; Bobelu, A.; Qualls, C.; Natachu, K.; Bobelu, J.; Jamon, E.; Neha, D.; Paine, S.; Zager, P. Concentrations of surface-dust metals in Native American jewelry-making homes in Zuni Pueblo, New Mexico. Arch. Environ. Health 2004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toxicological Profile for Tin and Tin Compounds. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp55.pdf (accessed on 21 July 2020).
- Satoh, M.; Chan, E.K.L.; Ho, L.A.; Rose, K.M.; Parks, C.G.; Cohn, R.D.; Jusko, T.A.; Walker, N.J.; Germolec, D.R.; Whitt, I.Z.; et al. Prevalence and sociodemographic correlates of antinuclear antibodies in the United States. Arthritis Rheum. 2012. [Google Scholar] [CrossRef]
- Mariz, H.A.; Sato, E.I.; Barbosa, S.H.; Rodrigues, S.H.; Dellavance, A.; Andrade, L.E.C. Pattern on the antinuclear antibody-HEp-2 test is a critical parameter for discriminating antinuclear antibody-positive healthy individuals and patients with autoimmune rheumatic diseases. Arthritis Rheum. 2011. [Google Scholar] [CrossRef]
- Marin, G.G.; Cardiel, M.H.; Cornejo, H.; Viveros, M.E. Prevalence of antinuclear antibodies in 3 groups of healthy individuals: Blood donors, hospital personnel, and relatives of patients with autoimmune diseases. J. Clin. Rheumatol. 2009. [Google Scholar] [CrossRef]
- Mahler, M.; Parker, T.; Peebles, C.L.; Andrade, L.E.; Swart, A.; Carbone, Y.; Ferguson, D.J.; Villalta, D.; Bizzaro, N.; Hanly, J.G.; et al. Anti-DFS70/LEDGF antibodies are more prevalent in healthy individuals compared to patients with systemic autoimmune rheumatic diseases. J. Rheumatol. 2012. [Google Scholar] [CrossRef]
- Rubin, R.L. Drug-induced lupus. Expert Opin. Drug Saf. 2015, 209, 135–147. [Google Scholar] [CrossRef]
- Ramírez-Sandoval, R.; Luévano-Rodríguez, N.; Rodríguez-Rodríguez, M.; Pérez-Pérez, M.E.; Saldívar-Elias, S.; Gurrola-Carlos, R.; Avalos-Díaz, E.; Bollain-Y-goytia, J.J.; Herrera-Esparza, R. An animal model using metallic ions to produce autoimmune nephritis. J. Immunol. Res. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dangleben, N.; Skibola, C.; Smith, M. Arsenic immunotoxicity: A review. Environ. Health Glob. Access Sci. Source 2013, 12, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohsawa, M.; Takahashi, K.; Otsuka, F. Induction of anti-nuclear antibodies in mice orally exposed to cadmium at low concentrations. Clin. Exp. Immunol. 1988, 73, 98. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Pooled (n = 115) | Navajo (n = 68) | Nicaraguan (n = 47) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Demographics | |||||||||
| Male Sex, n (%) | 115 (100%) | 68 (100%) | 47 (100%) | ||||||
| Median Age, years (range) | 31.7 (23–51) | 31 (26–47) | 32.2 (23–51) | ||||||
| Seafood Consumed past 3 days, n (%) a | - | - | 12 (23.40%) | ||||||
| Urinary Metals | % Detect | Median (μg/g) | Range (μg/g) | % Detect | Median (μg/g) | Range (μg/g) | % Detect | Median (μg/g) | Range (μg/g) |
| Total Arsenic | 99.5% | 6.32 | (2.04–66.55) | 99% | 4.63 | (2.04–25.51) | 100% | 13.50 | (4.06–66.55) |
| Arsenobetaine | 34% | 0.88 | (0.18–46.59) | 8% | 0.60 | (0.18–17.92) | 60% | 2.04 | (0.27–46.59) |
| Arsenocholine | 24% | 0.07 | (0.02–1.03) | 3% | 0.06 | (0.02–0.88) | 45% | 0.11 | (0.02–1.03) |
| As (III) | 95.5% | 0.77 | (0.09–5.56) | 97% | 0.54 | (0.09–1.74) | 94% | 1.17 | (0.27–5.56) |
| As (V) | 24.5% | 0.47 | (0.11–6.29) | 6% | 0.40 | (0.18–6.29) | 43% | 0.54 | (0.11–4.44) |
| Dimethylarsonic Acid (DMA) | 89.5% | 4.18 | (0.78–19.76) | 90% | 2.86 | (0.78–15.21) | 89% | 7.57 | (2.54–19.76) |
| Monomethylarsonic Acid (MMA) | 93.5% | 0.87 | (0.16–9.31) | 91% | 0.55 | (0.16–2.41) | 96% | 1.77 | (0.54–9.31) |
| Antimony | 87% | 0.05 | (0.01–0.36) | 97% | 0.05 | (0.02–0.36) | 77% | 0.03 | (0.01–0.20) |
| Barium | 100% | 2.03 | (0.21–15.49) | 100% | 1.52 | (0.21–12.47) | 100% | 3.06 | (0.43–15.49) |
| Cadmium | 88% | 0.12 | (0.01–0.62) | 99% | 0.14 | (0.02–0.62) | 77% | 0.09 | (0.01–0.26) |
| Cesium | 100% | 3.59 | (0.55–8.75) | 100% | 3.35 | (1.64–8.75) | 100% | 3.85 | (0.55–8.6) |
| Cobalt | 100% | 0.42 | (0.13–1.55) | 100% | 0.34 | (0.13–1.55) | 100% | 0.55 | (0.13–1.45) |
| Lead | 100% | 0.31 | (0.09–2.36) | 100% | 0.24 | (0.09–0.70) | 100% | 0.47 | (0.14–2.36) |
| Manganese | 58% | 0.12 | (0.03–5.81) | 35% | 0.1 | (0.03–1.04) | 81% | 0.18 | (0.03–5.81) |
| Molybdenum | 100% | 44.24 | (1.87–213.89) | 100% | 39.89 | (13.81–146.8) | 100% | 54.58 | (1.87–213.89) |
| Strontium | 100% | 151.29 | (23.85–726.83) | 100% | 130.16 | (23.85–316.58) | 100% | 222.28 | (33.84–726.83) |
| Thallium | 98.5% | 0.11 | (0.02–0.28) | 99% | 0.12 | (0.04–0.28) | 98% | 0.10 | (0.02–0.27) |
| Tin | 73.5% | 0.38 | (0.02–6.54) | 99% | 1.22 | (0.08–6.54) | 48% | 0.08 | (0.02–0.51) |
| Tungsten | 91.5% | 0.07 | (0.01–1.80) | 96% | 0.10 | (0.02–0.51) | 87% | 0.05 | (0.01–1.80) |
| Uranium | 98% | 0.02 | (0.004–0.10) | 100% | 0.01 | (0.004–0.10) | 96% | 0.02 | (0.01–0.08) |
| Biomarkers | Pooled (n = 115) | Navajo (n = 68) | Nicaraguan (n = 47) | |||
|---|---|---|---|---|---|---|
| ANA Positivity (≥2), 1:160 dilution a | n | (%) | n | (%) | n | (%) |
| Any Site | 9 | (7.8%) | 5 | (7.4%) | 4 | (8.5%) |
| Nuclear Site | 5 | (4.4%) | 3 | (4.4%) | 2 | (4.3%) |
| Cytoplasmic Site | 3 | (2.6%) | 1 | (1.5%) | 2 | (4.3%) |
| Nucleolar Site | 1 | (0.9%) | 1 | (1.5%) | 0 | (0%) |
| ANA Positivity (≥2), 1:40 dilution a | n | (%) | n | (%) | n | (%) |
| Any Site | 76 | (66.1%) | 38 | (55.9%) | 38 | (80.9%) |
| Nuclear Site | 33 | (28.7%) | 19 | (27.9%) | 14 | (29.8%) |
| Cytoplasmic Site | 67 | (58.3%) | 32 | (47.1%) | 35 | (74.5%) |
| Nucleolar Site | 8 | (7.0%) | 8 | (11.8%) | 0 | (0%) |
| Specific AutoAntibody (SpAuAb) Elevation | n | (%) | n | (%) | n | (%) |
| Any SpAuAb | 13 | (11.3%) | 9 | (13.2%) | 4 | (8.5%) |
| Histone | 3 | (2.6%) | 2 | (2.9%) | 1 | (2.1%) |
| Chromatin | 3 | (2.6%) | 2 | (2.9%) | 1 | (2.1%) |
| dDNA | 10 | (8.7%) | 7 | (10.3%) | 3 | (6.4%) |
| nDNA | 2 | (1.7%) | 2 | (2.9%) | 0 | (0%) |
| Metals Tertiles | Any ANA Positivity (1:160 dilution) | Any ANA Positivity (1:40 dilution) |
|---|---|---|
| Metals | OR (95%CI) | OR (95% CI) |
| Total Arsenic—Tertile 1 (4.67μg/g) | REF | REF |
| Total Arsenic—Tertile 2 (11.14 μg/g) | 0.64 (0.21, 1.97) | 1.01 (0.55, 1.86) |
| Total Arsenic—Tertile 3 (66.55 μg/g) | 1.69 (0.41, 6.82) | 1.72 (0.68, 4.31) |
| Arsenobetaine—Tertile 1 (0.60 μg/g) | REF | REF |
| Arsenobetaine—Tertile 2 (1.52 μg/g) | 0.76 (0.25, 2.32) | 0.78 (0.43, 1.42) |
| Arsenobetaine—Tertile 3 (46.59 μg/g) | 1.02 (0.30, 3.42) | 1.55(0.72, 3.35) |
| Arsenocholine—Tertile 1 (0.05 μg/g) | REF | REF |
| Arsenocholine—Tertile 2 (0.10 μg/g) | 0.73 (0.24, 2.23) | 1.13 (0.63, 2.03) |
| Arsenocholine—Tertile 3 (1.03 μg/g) | 1.11 (0.38, 3.25) | 0.95 (0.49, 1.82) |
| As (III)—Tertile 1 (0.51 μg/g) | REF | REF |
| As (III)—Tertile 2 (1.08 μg/g) | 1.10 (0.32, 3.71) | 1.39 (0.76, 2.53) |
| As (III)—Tertile 3 (5.56 μg/g) | 1.01 (0.41, 2.48) | 0.48 (0.23, 1.03) |
| As (V)—Tertile 1 (0.36 μg/g) | REF | REF |
| As (V)—Tertile 2 (0.60 μg/g) | 1.05 (0.38, 2.92) | 1.40 (0.77, 2.56) |
| As (V)—Tertile 3 (6.29 μg/g) | 1.17 (0.42, 3.29) | 0.73 (0.39, 1.35) |
| DMA—Tertile 1 (2.95 μg/g) | REF | REF |
| DMA—Tertile 2 (6.37 μg/g) | 1.46 (0.56, 3.82) | 0.78 (0.43, 1.43) |
| DMA—Tertile 3 (19.76 μg/g) | 0.45 (0.10, 1.97) | 2.17 (0.85, 5.47) |
| MMA—Tertile 1 (0.57 μg/g) | REF | REF |
| MMA—Tertile 2 (1.32 μg/g) | 0.98 (0.37, 2.61) | 1.20 (0.65, 2.23) |
| MMA—Tertile 3 (9.31 μg/g) | 0.93(0.22, 3.86) | 1.08 (0.42, 2.75) |
| Antimony—Tertile 1 (0.03 μg/g) | REF | REF |
| Antimony—Tertile 2 (0.06 μg/g) | 1.46 (0.57, 3.78) | 2.25 (1.16, 4.35) * |
| Antimony—Tertile 3 (0.36 μg/g) | 1.12 (0.39, 3.25) | 1.09 (0.58, 2.03) |
| Barium—Tertile 1 (1.26 μg/g) | REF | REF |
| Barium—Tertile 2 (3.09 μg/g) | 1.15 (0.39, 3.39) | 1.48 (0.82, 2.66) |
| Barium—Tertile 3 (15.49 μg/g) | 2.33 (0.83, 6.55) | 1.00 (0.54, 1.86) |
| Cadmium—Tertile 1 (0.09 μg/g) | REF | REF |
| Cadmium—Tertile 2 (0.16 μg/g) | 1.04 (0.39, 2.80) | 1.65 (0.90, 3.03) |
| Cadmium—Tertile 3 (0.62 μg/g) | 1.60 (0.58, 4.35) | 0.91 (0.49, 1.67) |
| Cesium—Tertile 1 (3.08 μg/g) | REF | REF |
| Cesium—Tertile 2 (4.13 μg/g) | 0.39 (0.09,1.65) | 1.17 (0.65, 2.10) |
| Cesium—Tertile 3 (8.75 μg/g) | 2.98 (1.07, 8.25) * | 0.55 (0.30, 1.01) |
| Cobalt—Tertile 1 (0.33 μg/g) | REF | REF |
| Cobalt—Tertile 2 (0.52 μg/g) | 1.55 (0.55, 4.35) | 0.79 (0.45, 1.40) |
| Cobalt—Tertile 3 (1.55 μg/g) | 1.78 (0.59, 5.37) | 1.25 (0.65, 2.39) |
| Lead—Tertile 1 (0.24 μg/g) | REF | REF |
| Lead—Tertile 2 (0.43 μg/g) | 0.41 (0.10, 1.73) | 1.09 (0.61, 1.95) |
| Lead—Tertile 3 (2.36 μg/g) | 3.31 (1.09, 9.97) * | 0.89 (0.46, 1.72) |
| Strontium—Tertile 1 (122.36 μg/g) | REF | REF |
| Strontium—Tertile 2 (201.59 μg/g) | 0.47 (0.10, 2.16) | 1.08 (0.60, 1.93) |
| Strontium—Tertile 3 (726.83 μg/g) | 4.71 (1.34, 16.61) * | 1.17 (0.59, 2.29) |
| Thallium—Tertile 1 (0.09 μg/g) | REF | REF |
| Thallium—Tertile 2 (0.13 μg/g) | 1.34 (0.51, 3.53) | 0.83 (0.46, 1.49) |
| Thallium—Tertile 3 (0.28 μg/g) | 1.09 (0.39, 3.03) | 1.25 (0.68, 2.27) |
| Tin—Tertile 1 (0.14 μg/g) | REF | REF |
| Tin—Tertile 2 (0.89 μg/g) | 1.55 (0.59, 4.06) | 0.64 (0.34, 1.21) |
| Tin—Tertile 3 (6.54 μg/g) | 1.73 (0.41, 7.32) | 0.82 (0.36, 1.90) |
| Tungsten—Tertile 1 (0.05 μg/g) | REF | REF |
| Tungsten—Tertile 2 (0.11 μg/g) | 0.94 (0.27, 3.22) | 0.92 (0.51, 1.65) |
| Tungsten—Tertile 3 (1.80 μg/g) | 4.00 (1.11, 14.44) * | 1.56 (0.82, 2.94) |
| Uranium—Tertile 1 (0.01 μg/g) | REF | REF |
| Uranium—Tertile 2 (0.02 μg/g) | 0.98 (0.34, 2.89) | 0.86 (0.46, 1.62) |
| Uranium—Tertile 3 (0.10 μg/g) | 1.50 (0.58, 3.90) | 0.77 (0.42, 1.39) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scammell, M.K.; Sennett, C.; Laws, R.L.; Rubin, R.L.; Brooks, D.R.; Amador, J.J.; López-Pilarte, D.; Ramirez-Rubio, O.; Friedman, D.J.; McClean, M.D.; et al. Urinary Metals Concentrations and Biomarkers of Autoimmunity among Navajo and Nicaraguan Men. Int. J. Environ. Res. Public Health 2020, 17, 5263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155263
Scammell MK, Sennett C, Laws RL, Rubin RL, Brooks DR, Amador JJ, López-Pilarte D, Ramirez-Rubio O, Friedman DJ, McClean MD, et al. Urinary Metals Concentrations and Biomarkers of Autoimmunity among Navajo and Nicaraguan Men. International Journal of Environmental Research and Public Health. 2020; 17(15):5263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155263
Chicago/Turabian StyleScammell, Madeleine K., Caryn Sennett, Rebecca L. Laws, Robert L. Rubin, Daniel R. Brooks, Juan José Amador, Damaris López-Pilarte, Oriana Ramirez-Rubio, David J. Friedman, Michael D. McClean, and et al. 2020. "Urinary Metals Concentrations and Biomarkers of Autoimmunity among Navajo and Nicaraguan Men" International Journal of Environmental Research and Public Health 17, no. 15: 5263. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155263