Effects of an Alternative Sports Program Using Kin-Ball in Individuals with Intellectual Disabilities

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
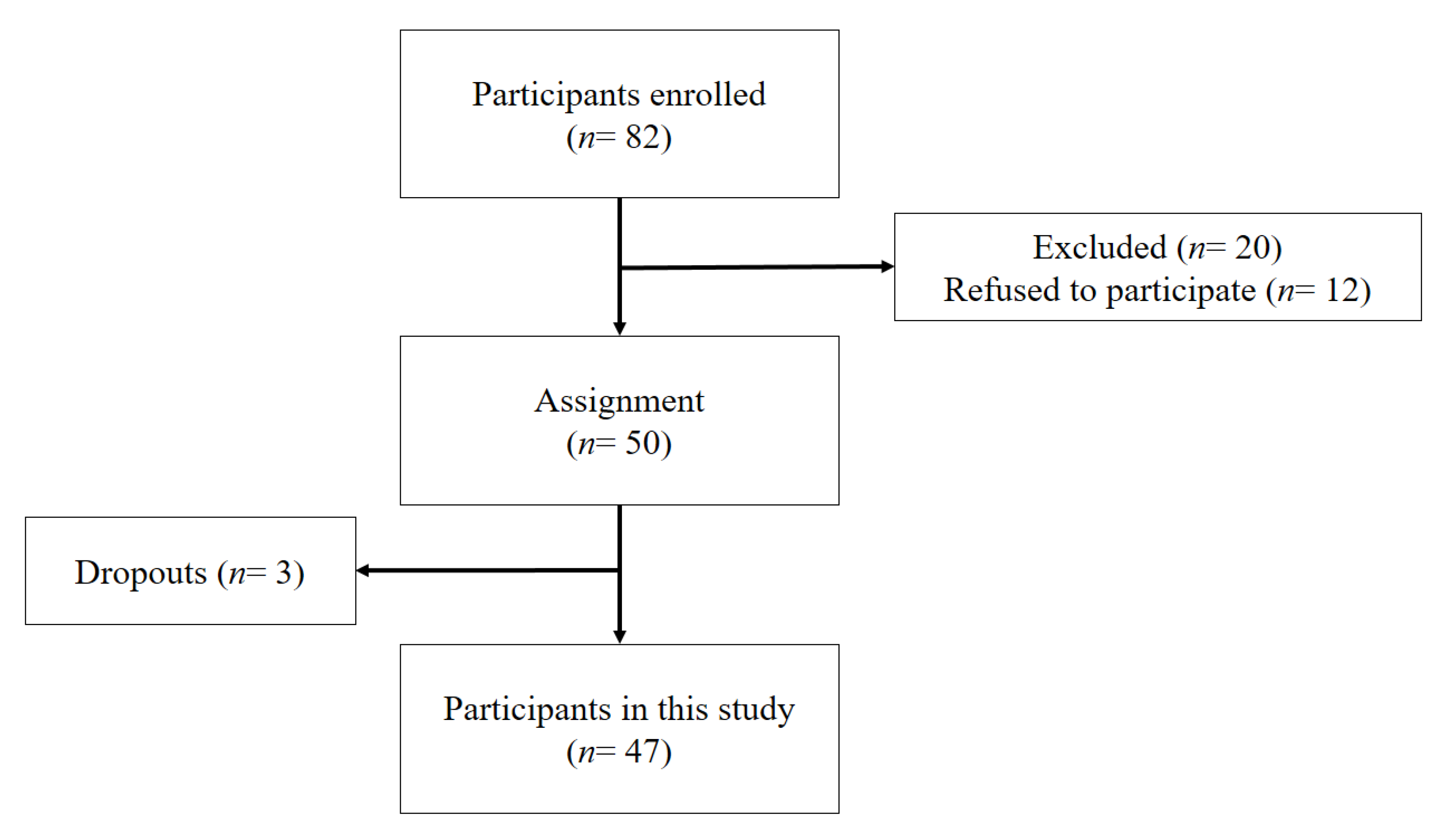
2.1. Participants and Procedures
2.2. The Kin-Ball Program
2.3. Variables and Instruments
2.3.1. Body Composition
2.3.2. Physical Qualities
2.4. Procedures
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Skowroński, W.; Horvat, M.; Nocera, J.; Roswal, G.; Croce, R. Eurofit special: European fitness battery score variation among individuals with intellectual disabilities. Adap. Phys. Act. Q. 2009, 261, 54–67. [Google Scholar] [CrossRef]
- Hsieh, K.; Rimmer, J.H.; Heller, T. Obesity and associated factors in adults with intellectual disability. J. Intellect. Disabil. Res. 2014, 589, 851–863. [Google Scholar] [CrossRef]
- Vázquez, A.; Jenaro, C.; Flores, N.; Bagnato, M.J.; Pérez, M.C.; Cruz, M. Intervenciones de salud electrónica para adultos y personas de edad con discapacidad intelectual: Una revisión. Front. Psychol. 2018, 9, 1–7. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). World Report on Disability; WHO Press: Geneva, Switzerland, 2011. [Google Scholar]
- Instituto Nacional de Estadística (INE). El Empleo de las Personas con Discapacidad 2013; INE: Madrid, Spain, 2015. [Google Scholar]
- Bartlo, P.; Klein, P.J. Physical activity benefits and needs in adults with intellectual disabilities: Systematic review of the literature. Am. J. Intellect. Dev. Disabil. 2011, 116, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Hinckson, E.A.; Curtis, A. Measuring physical activity in children and youth living with intellectual disabilities: A systematic review. Res. Dev. Disabil. 2013, 34, 72–86. [Google Scholar] [CrossRef]
- Emerson, E. Underweight, obesity and exercise among adults with intellectual disabilities in supported accommodation in Northern England. J. Intellect. Disabil. Res. 2005, 49, 134–143. [Google Scholar] [CrossRef]
- Durstine, J.L.; Gordon, B.; Wang, Z.; Luo, X. Chronic disease and the link to physical activity. J. Sport Health Sci. 2013, 2, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Agiovlasitis, S.; Yun, J.; Jin, J.; McCubbin, J.A.; Motl, R.W. Physical activity promotion for persons experiencing disability: The importance of interdisciplinary research and practice. Adapt. Phys. Act. Q. 2018. [Google Scholar] [CrossRef]
- Heller, T.; McCubbin, J.A.; Drum, C.; Peterson, J. Physical activity and nutrition health promotion interventions: What is working for people with intellectual disabilities? Intellect. Dev. Disabil. 2011, 49, 26–36. [Google Scholar] [CrossRef]
- McGarty, A.M.; Penpraze, V.; Melville, C.A. Accelerometer use during field-based physical activity research in children and adolescents with intellectual disabilities: A systematic review. Res. Dev. Disabil. 2014, 355, 973–981. [Google Scholar] [CrossRef]
- Einarsson, I.T.; Olafsson, A.; Hinriksdottir, G.; Hinriksdottir, G.; Johannsson, E.; Daly, D.; Arngrimsson, S.A. Differences in physical activity among youth with and without intelectual disability. Med. Sci. Sports Exerc. 2015, 47, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.; Staples, K. The role of physical activity in improving physical fitness in children with intellectual and developmental disabilities. Res. Dev. Disabil. 2017, 69, 49–60. [Google Scholar] [CrossRef]
- Yilmaz, A.; Karakas, G.; Kaya, H.B.; Kacay, Z. The effects of sportive exercises on physical fitness of children with specific learning disability. Acta Kinesiol. 2017, 11, 88–93. [Google Scholar]
- Barr, M.; Shields, N. Identifying the barriers and facilitators to participation in physical activity for children with Down syndrome. J. Intellect. Disabil. Res. 2011, 55, 1020–1033. [Google Scholar] [CrossRef] [PubMed]
- Oviedo, G.; Travier, N.; Guerra-Balic, M. Sedentary and physical activity patterns in adults with intellectual disability. Int. J. Environ. Res. Public Health 2017, 149, 1027. [Google Scholar] [CrossRef] [PubMed]
- Luiselli, J.K. Training care-providers to implement exercise, physical activity, and sports participation interventions. Int. J. Sport Psychol. 2017, 485, 543–554. [Google Scholar] [CrossRef]
- Pérez-Cruzado, D.; Cuesta-Vargas, A.I.; Vera-García, E.; Mayoral-Cleries, F. Physical fitness and levels of physical activity in people with severe mental illness: A cross-sectional study. BMC Sports Med. Rehabil. Sci. 2017, 917, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogg-Groenendaal, M.; Hermans, H.; Claessens, B. A systematic review on the effect of exercise interventions on challenging behavior for people with intellectual disabilities. Res. Dev. Disabil. 2014, 357, 1507–1517. [Google Scholar] [CrossRef]
- Johnson, C.C. The benefits of physical activity for youth with developmental disabilities: A systematic review. Am. J. Health Promot. 2009, 23, 157–167. [Google Scholar] [CrossRef]
- Barry, V.W.; Baruth, M.; Beets, M.W.; Durstine, J.L.; Liu, J.; Blair, S.N. Fitness vs. fatness on all-cause mortality: A meta-analysis. Prog. Cardiovasc. Dis. 2014, 564, 382–390. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Dickinson, A.; Water, T.; Sands, M.; Penman, L. Physical activity, dietary habits and overall health in overweight and obese children and youth with intellectual disability or autism. Res. Dev. Disabil. 2013, 34, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Boddy, L.M.; Downs, S.J.; Knowles, Z.R.; Fairclough, S.J. Physical activity and play behaviours in children and young people with intellectual disabilities: A cross-sectional observational study. Sch. Psychol. Int. 2015, 36, 154–171. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Cruzado, D.; Cuesta-Vargas, A.I. Changes on quality of life, self-efficacy and social support for activities and physical fitness in people with intellectual disabilities through multimodal intervention. Eur. J. Spec. Needs Educ. 2016, 314, 553–564. [Google Scholar] [CrossRef]
- Harris, L.; Hankey, C.; Murray, H.; Melville, C. The effects of physical activity interventions on preventing weight gain and the effects on body composition in young adults with intellectual disabilities: Systematic review and meta-analysis of randomized controlled trials. Clin. Obes. 2015, 5, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Kuijken, N.M.J.; Naaldenberg, J.; Nijhuis-van der Sanden, M.W.; Schrojenstein-Lantman de Valk, H.M.J. Healthy living according to adults with intellectual disabilities: Towards tailoring health promotion initiatives. J. Intellect. Disabil. Res. 2016, 603, 228–241. [Google Scholar] [CrossRef]
- Melville, C.A.; Mitchell, F.; Stalker, K.; Matthews, L.; McConnachie, A.; Murray, H.M. Effectiveness of a walking programme to support adults with intellectual disabilities to increase physical activity: Walk well cluster-randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 125. [Google Scholar] [CrossRef] [Green Version]
- Van Schijndel-Speet, M.; Evenhuis, H.M.; Van Wijck, R.; Montfort, K.; Echteld, M.A. A structured physical activity and fitness programme for older adults with intellectual disabilities: Results of a cluster-randomised clinical trial. J. Intellect. Disabil. Res. 2016, 611, 16–29. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Burghardt, A.R.; Lloyd, M.; Tiernan, C.; Hornyak, J.E. Physical activity benefits of learning to ride a two-wheel bicycle for children with Down syndrome: A randomized trial. Phys. Ther. 2011, 91, 1463–1477. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F. The feasibility of a physical activity program for young adults with Down syndrome: A phase II randomised controlled trial. J. Intellect. Dev. Disabil. 2015, 40, 115–125. [Google Scholar] [CrossRef]
- Van Schijndel-Speet, M.; Evenhuis, H.M.; Van Empelen, P.; Van Wijck, R.; Echteld, M.A. Development and evaluation of a structured programme for promoting physical activity among seniors with intellectual disabilities: A study protocol for a cluster randomized trial. BMC Public Health 2013, 13, 746. [Google Scholar] [CrossRef] [Green Version]
- Abellán, J.; Sáez-Gallego, N.M.; Olivares, S.C. Boccia as an adapted and sensitizing sport in physical education in secondary education. Sport-TK 2018, 72, 109–113. [Google Scholar] [CrossRef]
- Lobenius-Palmér, K.; Sjöqvist, B.; Hurtig-Wennlöf, A.; Lars-Olov, L. Accelerometer-assessed physical activity and sedentary time in youth with disabilities. Hum. Kinet. J. Sport 2018, 351, 1–19. [Google Scholar] [CrossRef]
- Hall, N.; McDonald, G.K.; Hay, J.; Defries, D.; Pryce, R. Effect of activity type on youth physical activity during structured activity sessions. Health Behav. Policy Rev. 2016, 36, 546–556. [Google Scholar] [CrossRef]
- Hastie, P.A.; Langevin, F.; Wadsworth, D. Effects of age and experience on physical activity accumulation during kin-ball. Res. Q. Exerc. Sport 2011, 821, 140–144. [Google Scholar] [CrossRef] [PubMed]
- International Kin-Ball Sport Federation. Official KIN-BALL® Sport Rules; IKB: Montreal, QC, Canada, 2018. [Google Scholar]
- Hawkins, R.O.; Haydon, T.; Denune, H.; Larkin, W.; Fite, N. Improving the transition behavior of high school students with emotional behavioral disorders using a randomized interdependent group contingency. Sch. Psychol. Rev. 2015, 44, 208–223. [Google Scholar] [CrossRef]
- Lum, J.; Radley, K.C.; Tingstrom, D.H.; Dufrene, B.A.; Olmi, J.; Wright, S.J. Tootling with a randomized independent group contingency to improve high school classwide behavior. J. Posit. Behav. Interv. 2019, 212, 93–105. [Google Scholar] [CrossRef]
- Thomson, A.; Bridges, S.; Corrins, B.; Pham, J.; White, C.; Buchanan, A. The impact of physical activity and sport programs on community participation for people with intellectual disability: A systematic review. J. Intellect. Dev. Disabil. 2020. [Google Scholar] [CrossRef]
- Díaz-Amate, R.; Alcántara, F.; Torres, G.; Lara, A. Time and gestural structure of Kin-Ball. Apunts 2015, 1202, 36–42. [Google Scholar] [CrossRef]
- Mullor, D.; Gallego, J.; Cangas, A.J.; Aguilar-Parra, J.M.; Valenzuela, L.; Mateu, J.M.; López-Pardo, A. Efectividad de un programa de actividad física en personas con trastorno mental grave. Int. J. Med. Sci. Phys. Act. Sport 2017, 1767, 507–520. [Google Scholar] [CrossRef] [Green Version]
- Wouters, M.; Evenhuis, H.M.; Hilgenkamp, T. Physical fitness of children and adolescents with moderate to severe intellectual disabilities. Disabil. Rehabil. 2019. [Google Scholar] [CrossRef]
- Ganley, K.J.; Paterno, M.V.; Miles, C.; Stout, J.; Brawner, L.; Girolami, G.; Warren, M. Health-related fitness in children and adolescents. Pediatr. Phys. Ther. 2011, 23, 208–220. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Lobstein, T. Defining obesity risk status in the general childhooh population: Which cut-offs should we use? Int. J. Pediatr. Obes. 2010, 5, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Nasuti, G.; Stuart-Hill, L.; Temple, V.A. The six-minute walk testfor adults with intellectual disability: A study of validity and reliability. J. Intellect. Dev. Disabil. 2013, 381, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Boer, P.H.; Moss, S.J. Test–retest reliability andminimal detectable change scores of twelve functional fitness tests in adults with Down syndrome. Res. Dev. Disabil. 2016, 48, 176–185. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, MI, USA, 1988. [Google Scholar]
- Kristensen, P.L.; Moeller, N.C.; Korsholm, L.; Kolle, E.; Wedderkopp, N.; Foberg, K.; Andersen, L.B. The association between aerobic fitness and physical activity in children and adolescents: The European youth heart study. Eur. J. Appl. Physiol. 2010, 110, 267–275. [Google Scholar] [CrossRef]
- Burgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study Ballabeina. Int. J. Obes. 2011, 35, 937–944. [Google Scholar] [CrossRef] [Green Version]
- Frey, G.C.; Stanish, H.I.; Temple, V.A. Physical activity of youth with intellectual disability: Review and research agenda. Adapt. Phys. Act. Q. 2008, 25, 95–117. [Google Scholar] [CrossRef]
- Tint, A.; Thomson, K.; Weiss, J.A. A systematic literature review of the physical and psychosocial correlates of Special Olympics participation among individuals with intellectual disability. J. Intellect. Disabil. Res. 2017, 614, 301–324. [Google Scholar] [CrossRef]
- Bazzano, A.T.; Zeldin, A.S.; Diab, I.R.; Garro, N.M.; Allevato, N.A.; Lehrer, D. The Healthy Lifestyle Change Program: A pilot of a community-based health promotion intervention for adults with developmentaldisabilities. Am. J. Prev. Med. 2009, 37, 201–208. [Google Scholar] [CrossRef]
- Harris, L.; Hankey, C.; Jones, N.; Pert, C.; Murray, H.; Tobin, J. A cluster randomised control trial of a multi-component weight management programme foradults with intellectual disabilities and obesity. Br. J. Nutr. 2017, 118, 229–240. [Google Scholar] [CrossRef] [Green Version]
- Jeng, S.C.; Chang, C.W.; Liu, W.Y.; Hou, Y.J.; Lin, Y.H. Exercise training on skill-related physical fitness in adolescents with intellectual disability: A systematic review and meta-analysis. Disabil. Health J. 2017, 10, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Sze, T.; Yu, J.J.; Loprinzi, P.D.; Xiao, T.; Yeung, A.S.; Li, C. Tai chi as an alternative exercise to improve physical fitness for children and adolescents with intellectual disability. Int. J. Environ. Res. Public Health 2019, 16, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schrojenstein, H.M.J.; Van de Akker, M.; Maaskant, M.A.; Haveman, M.J.; Urlings, H.F.J.; Kessels, A.G.; Crebolder, J.K. Prevalence and incidence of health problems in people with intellectual disability. J. Intellect. Disabil. Res. 2007, 411, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Shin, I.S.; Park, E.Y. Meta-analysis of the effect of exercise programs for individuals with intelectual disabilities. Res. Dev. Disabil. 2012, 33, 1937–1947. [Google Scholar] [CrossRef]
- Currie, T.; McKenzie, K.; Noone, S. The experiences of people with an intellectual disability of a mindfulness-based program. Mindfulness 2019, 10, 1304–1314. [Google Scholar] [CrossRef] [Green Version]
- Pérez, C.A.; Carral, J.M.C.; Costas, A.Á.; Martínez, S.V.; Martínez-Lemos, R.I. Water-based exercise for adultswith Down syndrome: Findings from a preliminary study. Int. J. Ther. Rehabil. 2018, 25, 20–28. [Google Scholar] [CrossRef]
- Archer, T. Health benefits of physical exercise for children and adolescents. J. Nov. Physiother. 2014, 4, 203–205. [Google Scholar] [CrossRef]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Beh. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- Vílchez-Polo, I.; Ramírez-Granizo, I.A.; Ubago-Jiménez, J.L. The SLOC, as a new inclusive sport: A didactic proposal. ESHPA Educ. Sport Health Phys. Act. 2019, 33, 324–335. [Google Scholar]
- Van Der Ploeg, H.P.; Van Der Beek, A.J.; Van Der Woude, L.H.V.; Van Mechelen, W. Physical activity forpeople with a disability: A conceptual model. Sports Med. 2004, 34, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Hocking, J.; McNeil, J.; Campbell, J. Physical therapy interventions for gross motor skills in people with an intellectual disability aged 6 years and over: A systematic review. Int. J. Evid. Based Health 2016, 14, 166–174. [Google Scholar] [CrossRef] [PubMed]
- McMurray, R.G.; Harrell, J.S.; Deng, S.; Bradley, C.B.; Cox, L.M.; Bangdiwala, S.I. The influence of physical activity, socioeconomic status, and ethnicity on the weight status of adolescents. Obes. Res. 2000, 82, 130–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labree, L.J.; Van de Mheen, H.; Rutten, F.F.; Foets, M. Differences in overweight and obesity among children from migrant and native origin: A systematic review of the European literature. Obes. Rev. 2011, 125, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Wilmore, J.H.; Costill, D.L.; Kenney, W.L. Physiology of Sport and Exercise, 4th ed.; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]


{kind=link}
| Characteristics | Session | |||||
|---|---|---|---|---|---|---|
| 1–2 | 3–4 | 5–6 | 7–8 | 9–10 | 11–12 | |
| Activity | Tag | Tag | Wall | Tag | Wall | Wall |
| Relay run | Omnikin | Indiana Jones | Relay run | Together | Tag | |
| Centipede | Together | Centipede | Indiana Jones | Tripod | Indiana Jones | |
| Together | Relay run | Tripod | Omnikin | Omnikin | Omnikin | |
| Tripod | Match | Match | Match | Match | Match | |
| Development | Centipede: Lying on the floor they pass the ball | |||||
| Indiana Jones: A person within the circle of players avoiding being touched by the ball | ||||||
| Match: Kinball match simulations | ||||||
| Omnikin: Ball hits with hands | ||||||
| Relay run: Ball handling in couples and trios | ||||||
| Tag: Touching a partner with the Omnikin ball | ||||||
| Together: At the signal “together” they have to touch the ball | ||||||
| Tripod: Holding the ball among three people | ||||||
| Wall: One player with the ball blocks others from passing from one zone to another | ||||||
| Variables | M | SD | Standard Error Average | Sig | ES (d) | 95% CI |
|---|---|---|---|---|---|---|
| BMIpre | 25.22 | 4.468 | 0.651 | 0.000 | 0.034 | (−0.538, 0.606) |
| BMIpost | 25.07 | 4.385 | 0.639 | |||
| Strepre | 19.38 | 6.101 | 0.890 | 0.000 | 0.279 | (−0.296, 0.853) |
| Strepost | 21.06 | 5.958 | 0.869 | |||
| Balpre | 24.31 | 19.748 | 2.880 | 0.000 | 0.410 | (−0.168, 0.988) |
| Balpost | 32.53 | 20.363 | 2.970 | |||
| Spepre | 11.25 | 2.099 | 0.306 | 0.000 | 0.281 | (−0.294, 0.856) |
| Spepost | 10.66 | 2.118 | 0.308 | |||
| Endpre | 478.73 | 76.816 | 11.204 | 0.000 | 0.295 | (−0.280, 0.870) |
| Endpost | 500.70 | 72.244 | 10.537 | |||
| Coopre | 70.57 | 19.142 | 2.792 | 0.000 | 0.779 | (0.186, 1.372) |
| Coopost | 85.68 | 19.670 | 2.869 |
| Variables | IMCpre | Strpre | Balpre | Spepre | Endpre | Coopre |
|---|---|---|---|---|---|---|
| BMIpre | 1.000 | |||||
| Strpre | −0.136 | 1.000 | ||||
| Balpre | −0.066 | 0.187 | 1.000 | |||
| Spepre | 0.075 | −0.160 | −0.355 * | 1.000 | ||
| Endpre | −0.242 | 0.046 | −0.064 | −0.009 | 1.000 | |
| Coopre | 0.197 | 0.111 | 0.011 | −0.050 | 0.106 | 1.000 |
| Variables | BMIpost | Strpost | Balpost | Spepost | Endpost | Coopost |
|---|---|---|---|---|---|---|
| BMIpost | 1.000 | |||||
| Strpost | −0.079 | 1.000 | ||||
| Balpost | −0.147 | −0.003 | 1.000 | |||
| Spepost | 0.149 | −0.109 | −0.279 | 1.000 | ||
| Endpost | −0.205 | 0.133 | −0.142 | 0.076 | 1.000 | |
| Coopost | 0.073 | 0.105 | 0.073 | −0.157 | 0.196 | 1.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zurita-Ortega, F.; Ubago-Jiménez, J.L.; Puertas-Molero, P.; Ramírez-Granizo, I.A.; Muros, J.J.; González-Valero, G. Effects of an Alternative Sports Program Using Kin-Ball in Individuals with Intellectual Disabilities. Int. J. Environ. Res. Public Health 2020, 17, 5296. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155296
Zurita-Ortega F, Ubago-Jiménez JL, Puertas-Molero P, Ramírez-Granizo IA, Muros JJ, González-Valero G. Effects of an Alternative Sports Program Using Kin-Ball in Individuals with Intellectual Disabilities. International Journal of Environmental Research and Public Health. 2020; 17(15):5296. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155296
Chicago/Turabian StyleZurita-Ortega, Félix, José Luis Ubago-Jiménez, Pilar Puertas-Molero, Irwin Andrés Ramírez-Granizo, José Joaquín Muros, and Gabriel González-Valero. 2020. "Effects of an Alternative Sports Program Using Kin-Ball in Individuals with Intellectual Disabilities" International Journal of Environmental Research and Public Health 17, no. 15: 5296. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155296