The Intentional Self-Medication of 9/11-Related PTSD Symptoms with Alcohol: 15 Years after the Disaster

Abstract
:1. Introduction
2. Materials and Methods
2.1. Exposures
2.2. Outcome
2.3. Confounders
2.4. Data Analysis
3. Results
3.1. Description of Analytic Sample
3.2. PTSD Symptomology and ISMA
3.3. Number PTSD Symptom Clusters Endorsed and ISMA
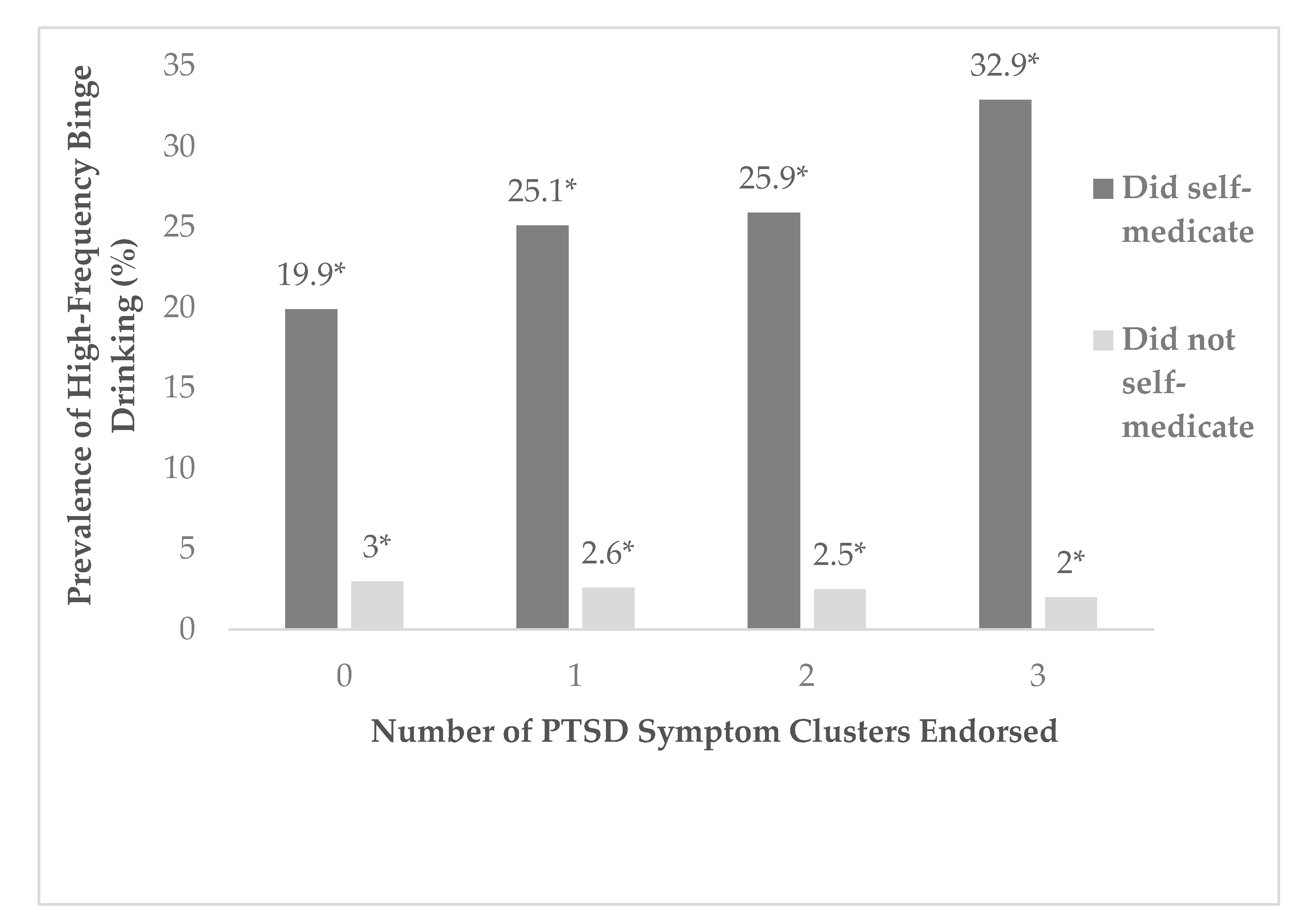
3.4. Binge Drinking, PTSD Severity, and ISMA
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| In the Last 30 Days, How Much Have You been Bothered by the Following Problems? | |||||
|---|---|---|---|---|---|
| Not at All | A Little Bit | Moderately | Quite A Bit | Extremely | |
| a. Repeated, disturbing memories, thoughts, or images of the events of 9/11 |  | | | | |
| b. Repeated, disturbing dreams of the events of 9/11 |  | | | | |
| c. Suddenly acting or feeling as if the events of 9/11 were happening again (as if you were reliving it) | | | | | |
| d. Feeling very upset when something reminded you of the events of 9/11 | | | | | |
| e. Having physical reactions (e.g., heart pounding, trouble breathing, sweating) when something reminded you of the events of 9/11 | | | | | |
| f. Avoiding thinking about or talking about the events of 9/11 or avoiding having feelings related to it | | | | | |
| g. Avoiding activities or situations because they remind you of the events of 9/11 | | | | | |
| h. Trouble remembering the important parts of the events of 9/11 | | | | | |
| i. Loss if interest in activities that you used to enjoy | | | | | |
| j. Feeling distant or cut off from other people | | | | | |
| k. Feeling emotionally numb or being unable to have loving feelings for those close to you | | | | | |
| l. Feeling as if your future will somehow be cut short | | | | | |
| m. Trouble falling or staying asleep | | | | | |
| n. Feeling irritable or having angry outbursts | | | | | |
| o. Having difficulty concentrating | | | | | |
| p. Being “super alert” or watchful or on guard | | | | | |
| q. Feeling jumpy or easily startled | | | | | |
References
- Neria, Y.; DiGrande, L.; Adams, B.G. Posttraumatic stress disorder following the September 11, 2001, terrorist attacks: A review of the literature among highly exposed populations. Am. Psychol. 2011, 66, 429–446. [Google Scholar] [CrossRef] [PubMed]
- Lowell, A.; Suarez-Jimenez, B.; Helpman, L.; Zhu, X.; Durosky, A.; Hilburn, A.; Schneier, F.; Gross, R.; Neria, Y. 9/11-related PTSD among highly exposed populations: A systematic review 15 years after the attack. Psychol. Med. 2018, 48, 537–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, S.H.; Mitchell, T.L.; Wright, K.D.; Loba, P. The relations of PTSD symptoms to alcohol use and coping drinking in volunteers who responded to the Swissair Flight 111 airline disaster. J. Anxiety Disord. 2004, 18, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Flory, K.; Hankin, B.L.; Kloos, B.; Cheely, C.; Turecki, G. Alcohol and cigarette use and misuse among Hurricane Katrina survivors: Psychosocial risk and protective factors. Subst. Use Misuse 2009, 44, 1711–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boscarino, J.A.; Adams, R.E.; Galea, S. Alcohol use in New York after the terrorist attacks: A study of the effects of psychological trauma on drinking behavior. Addict. Behav. 2006, 31, 606–621. [Google Scholar] [CrossRef] [PubMed]
- DiMaggio, C.; Galea, S.; Li, G. Substance use and misuse in the aftermath of terrorism. A Bayesian meta-analysis. Addiction 2009, 104, 894–904. [Google Scholar] [CrossRef]
- Keyes, K.M.; Hatzenbuehler, M.L.; Hasin, D.S. Stressful life experiences, alcohol consumption, and alcohol use disorders: The epidemiologic evidence for four main types of stressors. Psychopharmacology 2011, 218, 1–17. [Google Scholar] [CrossRef]
- Welch, A.E.; Caramanica Zweig, K.; McAteer, J.M.; Brackbill, R.M. Intensity of Binge Drinking a Decade After the September 11th Terror Attacks Among Exposed Individuals. Am. J. Prev. Med. 2017, 52, 192–198. [Google Scholar] [CrossRef]
- Cerda, M.; Tracy, M.; Galea, S. A prospective population based study of changes in alcohol use and binge drinking after a mass traumatic event. Drug Alcohol Depend. 2011, 115, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Jacobsen, L.K.; Southwick, S.M.; Kosten, T.R. Substance use disorders in patients with posttraumatic stress disorder: A review of the literature. Am. J. Psychiatry 2001, 158, 1184–1190. [Google Scholar] [CrossRef]
- Kessler, R.C.; Nelson, C.B.; McGonagle, K.A.; Edlund, M.J.; Frank, R.G.; Leaf, P.J. The epidemiology of co-occurring addictive and mental disorders: Implications for prevention and service utilization. Am. J. Orthopsychiatry 1996, 66, 17–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic stress disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef] [PubMed]
- McDevitt-Murphy, M.E.; Murphy, J.G.; Monahan, C.M.; Flood, A.M.; Weathers, F.W. Unique Patterns of Substance Misuse associated with PTSD, Depression, and Social Phobia. J. Dual. Diagn. 2010, 6, 94–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najavits, L.M.; Weiss, R.D.; Shaw, S.R. The link between substance abuse and posttraumatic stress disorder in women. A research review. Am. J. Addict. 1997, 6, 273–283. [Google Scholar]
- Simmons, S.; Suarez, L. Substance Abuse and Trauma. Child. Adolesc. Psychiatr. Clin. N. Am. 2016, 25, 723–734. [Google Scholar] [CrossRef]
- Ullman, S.E.; Relyea, M.; Peter-Hagene, L.; Vasquez, A.L. Trauma histories, substance use coping, PTSD, and problem substance use among sexual assault victims. Addict. Behav. 2013, 38, 2219–2223. [Google Scholar] [CrossRef] [Green Version]
- Villagonzalo, K.A.; Dodd, S.; Ng, F.; Mihaly, S.; Langbein, A.; Berk, M. The relationship between substance use and posttraumatic stress disorder in a methadone maintenance treatment program. Compr. Psychiatry 2011, 52, 562–566. [Google Scholar] [CrossRef]
- Chilcoat, H.D.; Breslau, N. Posttraumatic stress disorder and drug disorders: Testing causal pathways. Arch. Gen. Psychiatry 1998, 55, 913–917. [Google Scholar] [CrossRef] [Green Version]
- North, C.S.; Nixon, S.J.; Shariat, S.; Mallonee, S.; McMillen, J.C.; Spitznagel, E.L.; Smith, E.M. Psychiatric disorders among survivors of the Oklahoma City bombing. JAMA 1999, 282, 755–762. [Google Scholar] [CrossRef]
- Leeies, M.; Pagura, J.; Sareen, J.; Bolton, J.M. The use of alcohol and drugs to self-medicate symptoms of posttraumatic stress disorder. Depress. Anxiety 2010, 27, 731–736. [Google Scholar] [CrossRef]
- National Institute on Alcohol Abuse and Alcoholism. National Epidemiologic Survey on Alcohol and Related Conditions-II (NESARC-II). Available online: https://www.niaaa.nih.gov/research/nesarc-ii (accessed on 1 February 2018).
- Dworkin, E.R.; Wanklyn, S.; Stasiewicz, P.R.; Coffey, S.F. PTSD symptom presentation among people with alcohol and drug use disorders: Comparisons by substance of abuse. Addict. Behav. 2018, 76, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.H.; Conrod, P.J.; Pihl, R.O.; Dongier, M. Relations between posttraumatic stress symptom dimensions and substance dependence in a community-recruited sample of substance-abusing women. Psychol. Addict. Behav. 1999, 13, 78. [Google Scholar] [CrossRef]
- Yu, S.; Walker, D.; Brackbill, R.; Maslow, C.; Wu, D.; Osahan, S.; Yarnell, S. World Trade Center Health Registry W4 Data File User’s Manual; New York City Department of Health and Mental Hygiene: New York City, NY, USA, 2019.
- Farfel, M.; DiGrande, L.; Brackbill, R.; Prann, A.; Cone, J.; Friedman, S.; Walker, D.J.; Pezeshki, G.; Thomas, P.; Galea, S.; et al. An overview of 9/11 experiences and respiratory and mental health conditions among World Trade Center Health Registry enrollees. J. Urban Health 2008, 85, 880–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statisitcal Manual of Mental Disorders (4th edn, Text Revision); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD Checklist (PCL). Behav. Res. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. In Proceedings of the Annual Convention of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 24 October 1993. [Google Scholar]
- Turner, S.; Mota, N.; Bolton, J.; Sareen, J. Self-medication with alcohol or drugs for mood and anxiety disorders: A narrative review of the epidemiological literature. Depress. Anxiety 2018, 35, 851–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lejoyeux, M.; Lehert, P. Alcohol-use disorders and depression: Results from individual patient data metanalysis of the acamprosate-cont, rolled studies. Alcohol Alcohol. 2011, 46, 61–67. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services, Sunstance Abuse and Mental Health Services Administration. National Survey on Drug Use and Health Wave 2; DHHS, Ed.; RTI International: Rockville, MD, USA, 2005.
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Ghuman, S.J.; Brackbill, R.M.; Stellman, S.D.; Farfel, M.R.; Cone, J.E. Unmet mental health care need 10–11 years after the 9/11 terrorist attacks: 2011–2012 results from the World Trade Center Health Registry. BMC Public Health 2014, 14, 491. [Google Scholar] [CrossRef] [Green Version]
- Brissette, I.; Cohen, S.; Seeman, T.E. Measuring social integration and social networks. In Social Support Measurement and Intervention: A Guide for Health and Social Scientists; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Caramanica, K.; Brackbill, R.M.; Stellman, S.D.; Farfel, M.R. Posttraumatic Stress Disorder after Hurricane Sandy among Persons Exposed to the 9/11 Disaster. Int. J. Emerg. Ment. Health. 2015, 17, 356–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahran, H.S.; Kobau, R.; Moriarty, D.G.; Zack, M.M.; Holt, J.; Donehoo, R. Health-related quality of life surveillance—United States, 1993–2002. Mmwr. Surveill. Summ. 2005, 54, 1–35. [Google Scholar] [PubMed]
- Bolton, J.; Cox, B.; Clara, I.; Sareen, J. Use of alcohol and drugs to self-medicate anxiety disorders in a nationally representative sample. J. Nerv. Ment. Dis. 2006, 194, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Jakupcak, M.; Tull, M.T.; McDermott, M.J.; Kaysen, D.; Hunt, S.; Simpson, T. PTSD symptom clusters in relationship to alcohol misuse among Iraq and Afghanistan war veterans seeking post-deployment VA health care. Addict. Behav. 2010, 35, 840–843. [Google Scholar] [CrossRef]
- Chou, K.L.; Liang, K.; Sareen, J. The association between social isolation and DSM-IV mood, anxiety, and substance use disorders: Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2011, 72, 1468–1476. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- Kessler, R.C.; McLeod, J.D. Social Support and Mental Health in Community Samples; Academic Press: Cambridge, MA, USA, 1985. [Google Scholar]
- Khantzian, E.J. The self-medication hypothesis of addictive disorders: Focus on heroin and cocaine dependence. Am. J. Psychiatry 1985, 142, 1259–1264. [Google Scholar] [CrossRef]
- Peters, E.N.; Khondkaryan, E.; Sullivan, T.P. Associations between expectancies of alcohol and drug use, severity of partner violence, and posttraumatic stress among women. J. Interpers. Violence 2012, 27, 2108–2127. [Google Scholar] [CrossRef] [Green Version]
- Starzynski, L.L.; Ullman, S.E.; Filipas, H.H.; Townsend, S.M. Correlates of women’s sexual assault disclosure to informal and formal support sources. Violence Vict. 2005, 20, 417–432. [Google Scholar]
- Khantzian, E.J. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv. Rev. Psychiatry 1997, 4, 231–244. [Google Scholar] [CrossRef]
- Fisher, R.J.; Katz, J.E.J.P. Social-desirability bias and the validity of self-reported values. Soc. Mark. 2000, 17, 105–120. [Google Scholar] [CrossRef]
- Gargano, L.M.; Locke, S.; Li, J.; Farfel, M.R. Behavior problems in adolescence and subsequent mental health in early adulthood: Results from the World Trade Center Health Registry Cohort. Pediatr. Res. 2018, 84, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Nguyen, A.; DiGrande, L.; Brackbill, R.M. Mental health status of World Trade Center tower survivors compared to other survivors a decade after the September 11, 2001 terrorist attacks. Am. J. Ind. Med. 2016, 59, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Welch, A.E.; Stellman, S.D. Substance use in adolescents 10 years after the World Trade Center attacks in New York City. J. Child Adolesc. Subst. Abus. 2017, 26, 66–74. [Google Scholar] [CrossRef]
- Hirst, A.; Miller-Archie, S.A.; Welch, A.E.; Li, J.; Brackbill, R.M. Post-9/11 drug-and alcohol-related hospitalizations among World Trade Center Health Registry enrollees, 2003–2010. Drug Alcohol Depend. 2018, 187, 55–60. [Google Scholar] [CrossRef]

| Intentional Self-Medication with Alcohol | |||||||
|---|---|---|---|---|---|---|---|
| Variable | Total N | % | Yes, N | % | No, N | % | p-Value * |
| Sex | |||||||
| Female | 11,582 | 40.0 | 2233 | 19.3 | 9349 | 80.7 | <0.001 |
| Male | 17,353 | 60.0 | 3728 | 21.5 | 13,625 | 78.5 | |
| Race/Ethnicity | |||||||
| White, Non-Hispanic | 20,568 | 71.1 | 4468 | 21.7 | 16,100 | 78.3 | <0.001 |
| Black or African American | 2598 | 9.0 | 470 | 18.1 | 2128 | 81.9 | |
| American Indian/Alaska Native Hawaiian or Other Pacific Islander; Asian; Other | 5769 | 19.9 | 1,023 | 17.7 | 4746 | 82.3 | |
| Age Group at Wave 4 | |||||||
| 18–34 Years | 1098 | 3.8 | 273 | 24.9 | 825 | 75.1 | <0.001 |
| 35–44 Years | 4064 | 14.0 | 1032 | 25.4 | 3032 | 74.6 | |
| 45–64 Years | 17,651 | 61.0 | 3916 | 22.2 | 13,735 | 77.8 | |
| 65+ Years | 6122 | 21.2 | 740 | 12.1 | 5382 | 87.9 | |
| a Education Level at Wave 4 | |||||||
| High School/GED or Less | 4367 | 15.2 | 780 | 17.9 | 3587 | 82.1 | <0.001 |
| At Least Some College or Technical Degree | 8458 | 29.4 | 1684 | 19.9 | 6774 | 80.1 | |
| Bachelor Degree | 8408 | 29.3 | 1871 | 22.3 | 6537 | 77.7 | |
| Post Graduate Degree | 7459 | 26.1 | 1589 | 21.2 | 5906 | 78.8 | |
| Eligibility Group | |||||||
| RRWs | 13,145 | 45.4 | 2689 | 20.5 | 10,456 | 79.5 | 0.578 |
| Other Enrollees | 15,790 | 54.6 | 3272 | 20.7 | 12,518 | 79.3 | |
| Intentional Self-Medication with Alcohol | |||||||
|---|---|---|---|---|---|---|---|
| Total N | % | Yes, N | % | No, N | % | p-Value * | |
| a Number of Sources of Social Integration at Wave 4 | |||||||
| 0 | 217 | 0.8 | 54 | 24.9 | 163 | 75.1 | <0.001 |
| 1 | 1366 | 4.8 | 345 | 25.3 | 1021 | 74.7 | |
| 2 | 12,250 | 43.4 | 2905 | 23.7 | 9345 | 76.3 | |
| 3 | 9596 | 34.0 | 1883 | 19.6 | 7713 | 80.4 | |
| 4 | 4793 | 17.0 | 657 | 13.7 | 4136 | 86.3 | |
| b Social Support Score (0–20) | |||||||
| Mean | 13.9 | 12.5 | 14.2 | <0.001 ** | |||
| Standard Deviation | 5.3 | 5.3 | 5.2 | ||||
| c Life Satisfaction | |||||||
| 1 | 6905 | 24.1 | 903 | 13.1 | 6002 | 86.9 | <0.001 |
| 2 | 16,902 | 59.0 | 3441 | 20.4 | 13,461 | 79.6 | |
| 3 | 4068 | 14.2 | 1323 | 32.5 | 2745 | 67.5 | |
| 4 | 773 | 2.7 | 234 | 30.3 | 539 | 69.7 | |
| Endorse Re-Experiencing Cluster | |||||||
| Yes | 10,947 | 37.8 | 2967 | 27.1 | 7980 | 72.9 | <0.001 |
| No | 17,988 | 62.2 | 2994 | 16.6 | 14,994 | 83.4 | |
| Endorse Avoidance Cluster | |||||||
| Yes | 6844 | 23.7 | 2441 | 35.7 | 4403 | 64.3 | <0.001 |
| No | 22,091 | 76.3 | 3520 | 15.9 | 18,571 | 84.1 | |
| Endorse Hyperarousal Cluster | |||||||
| Yes | 10,929 | 37.8 | 3525 | 32.3 | 7404 | 67.7 | <0.001 |
| No | 18,006 | 62.2 | 2436 | 13.5 | 15,570 | 86.5 | |
| Numbers of Clusters Endorsed | |||||||
| 0 | 13,790 | 47.7 | 1696 | 12.3 | 12,094 | 87.7 | <0.001 |
| 1 | 6376 | 22.0 | 1340 | 21.0 | 5036 | 79.0 | |
| 2 | 3963 | 13.7 | 1182 | 29.8 | 27,81 | 70.2 | |
| 3 | 4806 | 16.6 | 1743 | 36.3 | 3063 | 63.7 | |
| History of Alcohol/Drug Problem | |||||||
| Yes | 1433 | 5.0 | 782 | 54.6 | 651 | 45.4 | <0.001 |
| No | 27,502 | 95.0 | 5179 | 18.8 | 22,323 | 81.2 | |
| Variable | AOR [95% CI] |
|---|---|
| Endorsement of Avoidance PTSD Symptom Cluster | |
| No | REF |
| Yes | 1.37 [1.24, 1.50] * |
| Endorsement of Re-Experiencing PTSD Symptom Cluster | |
| No | REF |
| Yes | 1.12 [1.03, 1.19] ** |
| Endorsement of Hyperarousal PTSD Symptom Cluster | |
| No | REF |
| Yes | 2.04 [1.88, 2.21] * |
| (N = 26,535) | |
|---|---|
| Variable | AOR [95% CI] |
| Endorsed 0 symptom clusters | REF |
| Endorsed 1 symptom cluster | 1.80 [1.65, 1.95] ** |
| Endorsed 2 symptom clusters | 2.51 [2.28, 2.77] * |
| Endorsed 3 symptom clusters | 2.84 [2.55, 3.17] * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garrey, S.K.; Welch, A.E.; Jacobson, M.H.; Brackbill, R.M.; Gargano, L.M. The Intentional Self-Medication of 9/11-Related PTSD Symptoms with Alcohol: 15 Years after the Disaster. Int. J. Environ. Res. Public Health 2020, 17, 5327. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155327
Garrey SK, Welch AE, Jacobson MH, Brackbill RM, Gargano LM. The Intentional Self-Medication of 9/11-Related PTSD Symptoms with Alcohol: 15 Years after the Disaster. International Journal of Environmental Research and Public Health. 2020; 17(15):5327. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155327
Chicago/Turabian StyleGarrey, Sascha K., Alice E. Welch, Melanie H. Jacobson, Robert M. Brackbill, and Lisa M. Gargano. 2020. "The Intentional Self-Medication of 9/11-Related PTSD Symptoms with Alcohol: 15 Years after the Disaster" International Journal of Environmental Research and Public Health 17, no. 15: 5327. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155327