Can Health Disparity Be Eliminated? The Role of Family Doctor Played in Shanghai, China


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Approval
2.2. Data and Measurements
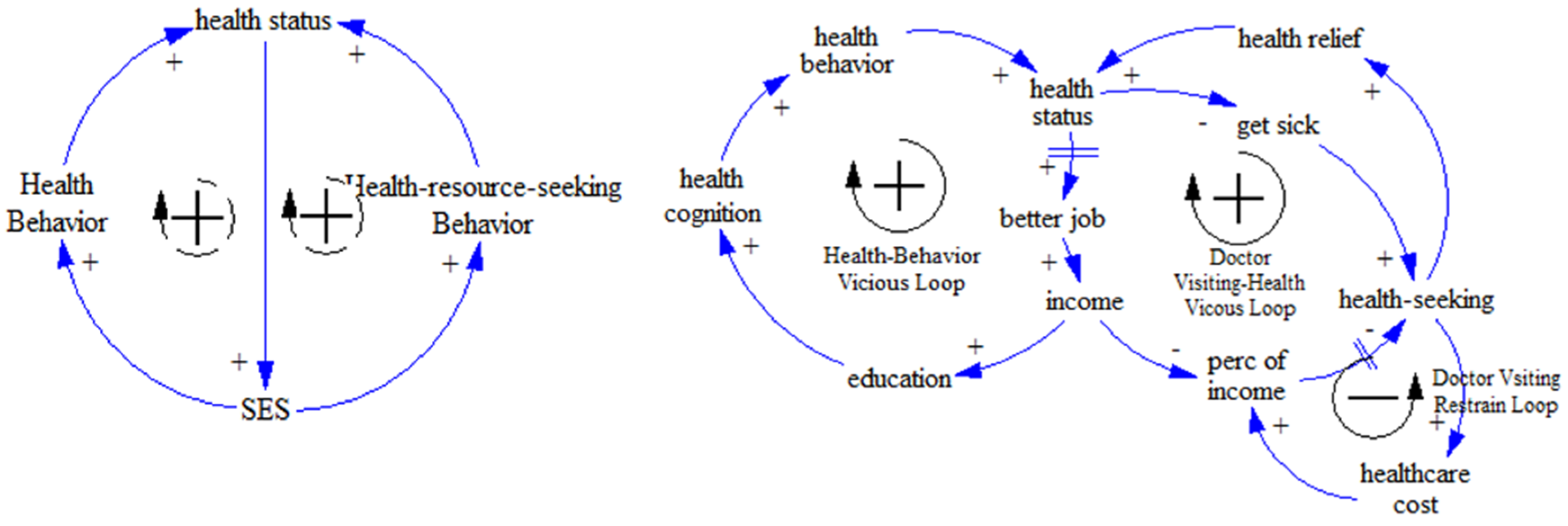
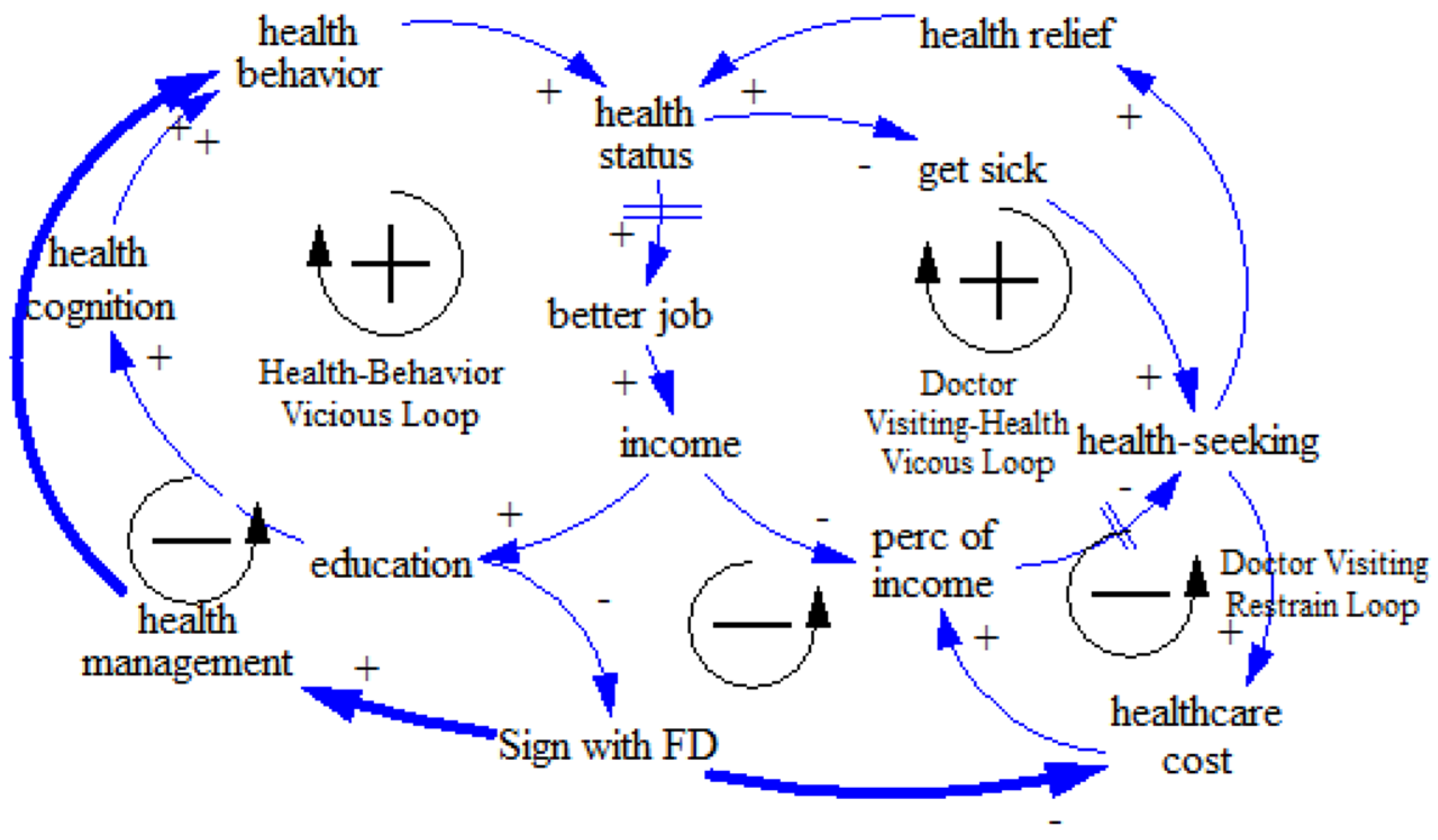
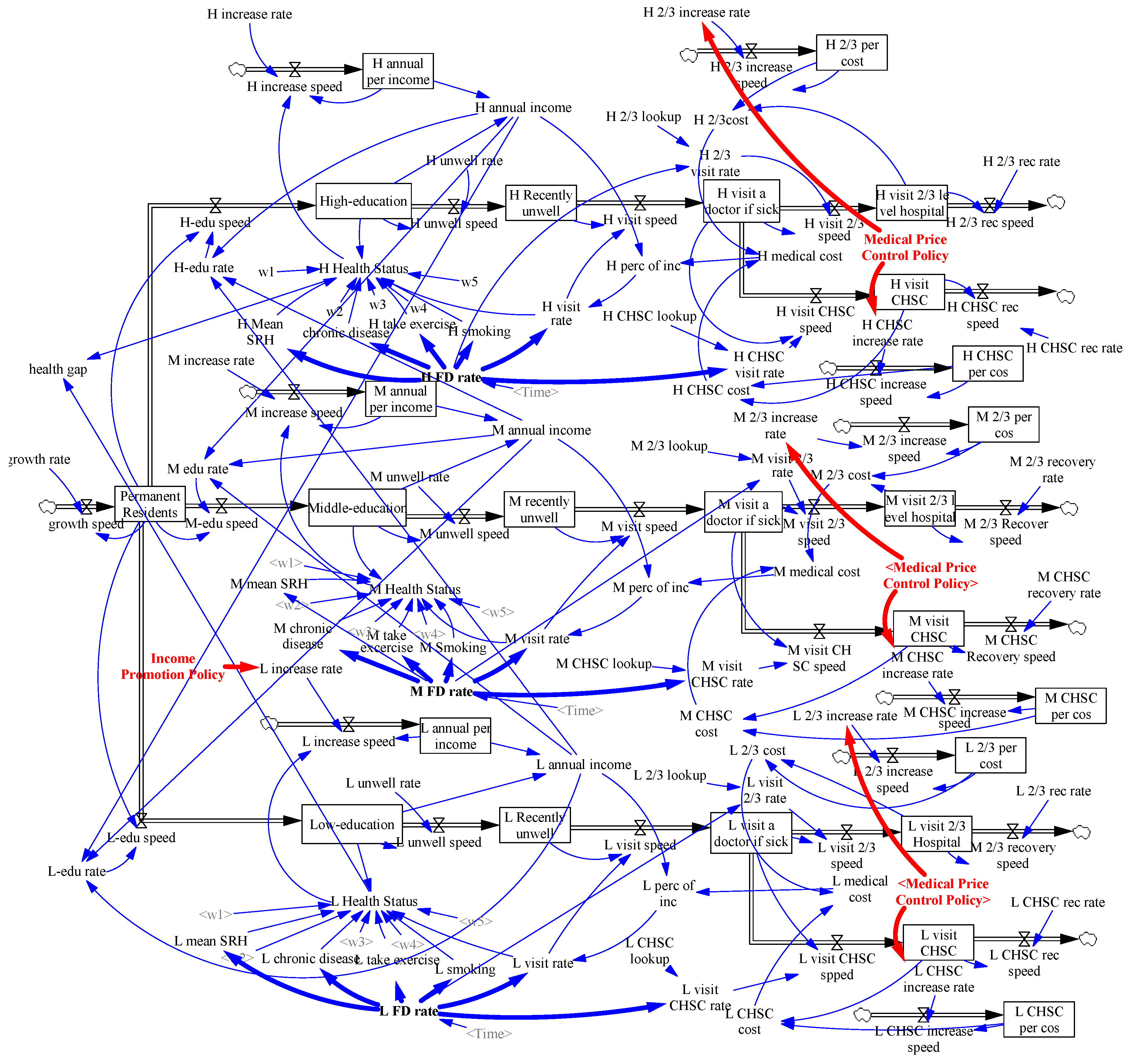
2.3. Model Construction
3. Results
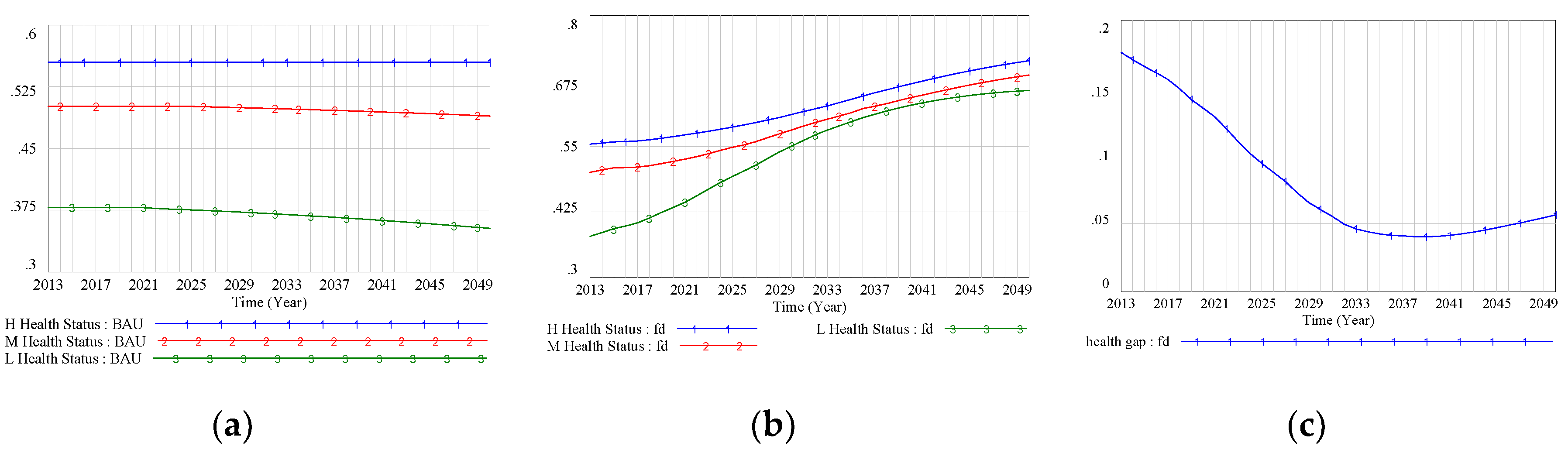
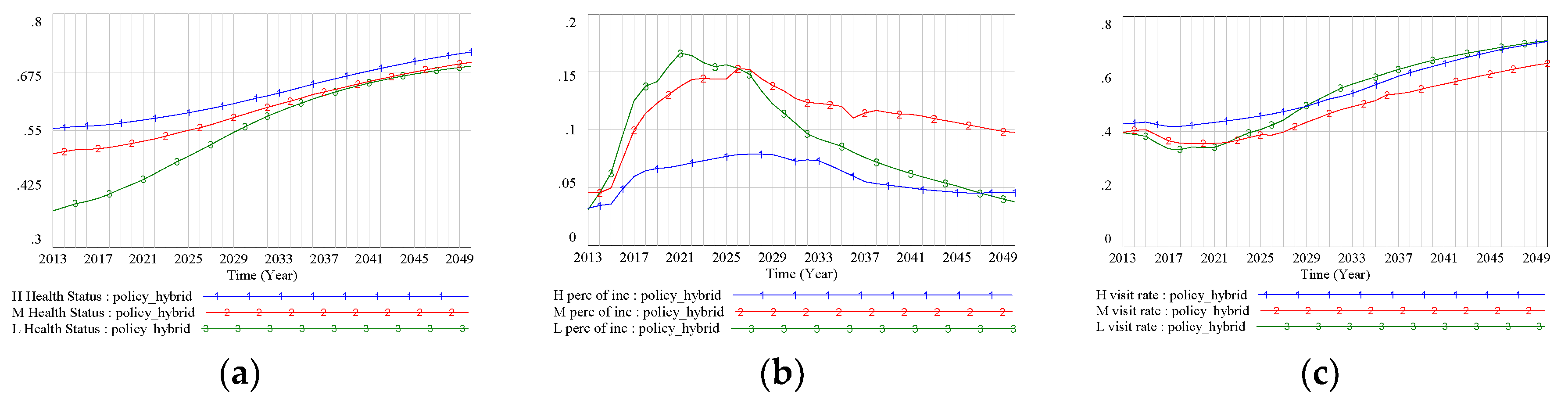
3.1. Analysis of Health Status under the Family Doctor Policy Intervention
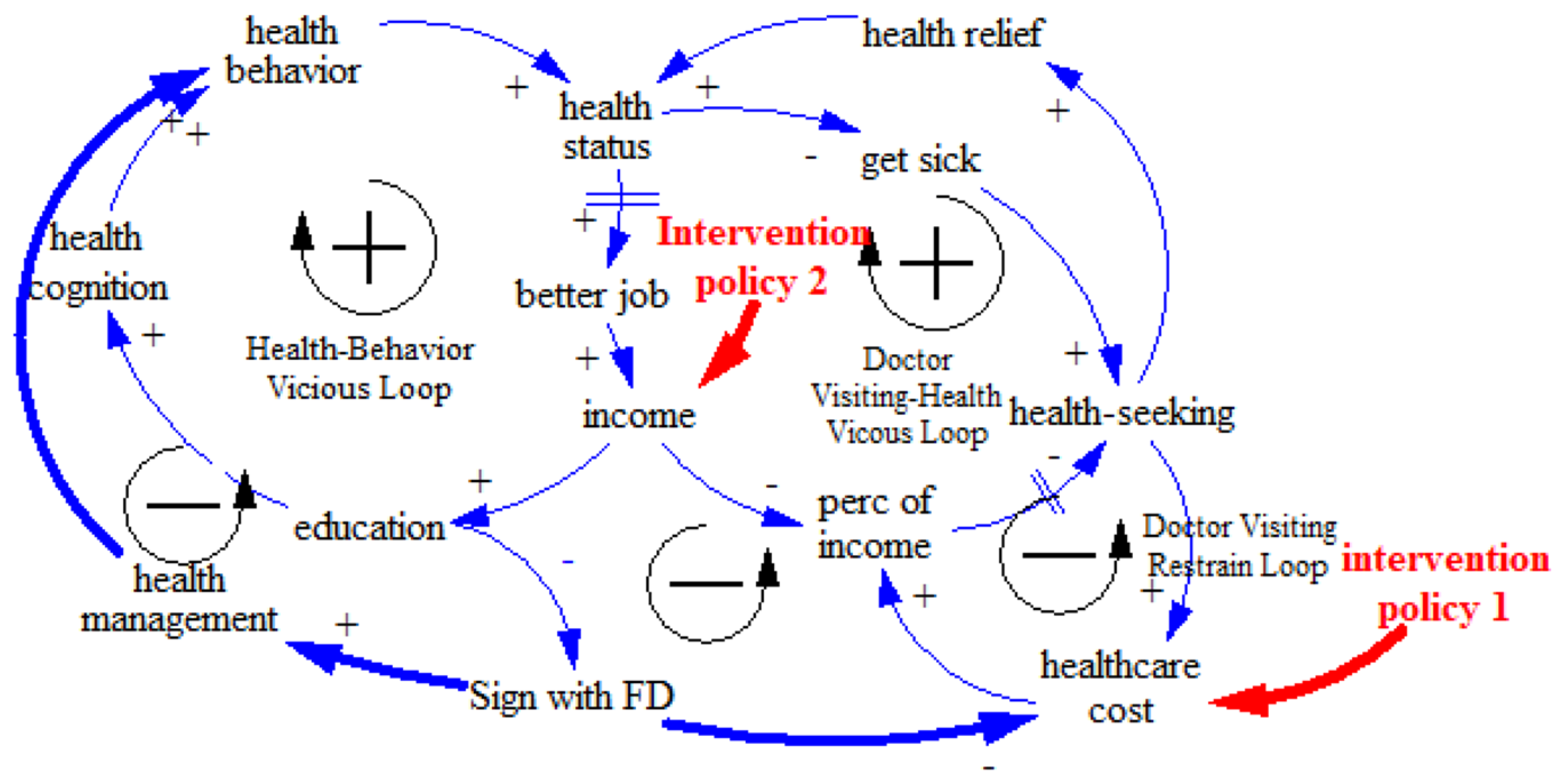
3.2. Supporting Policy Intervention Simulation
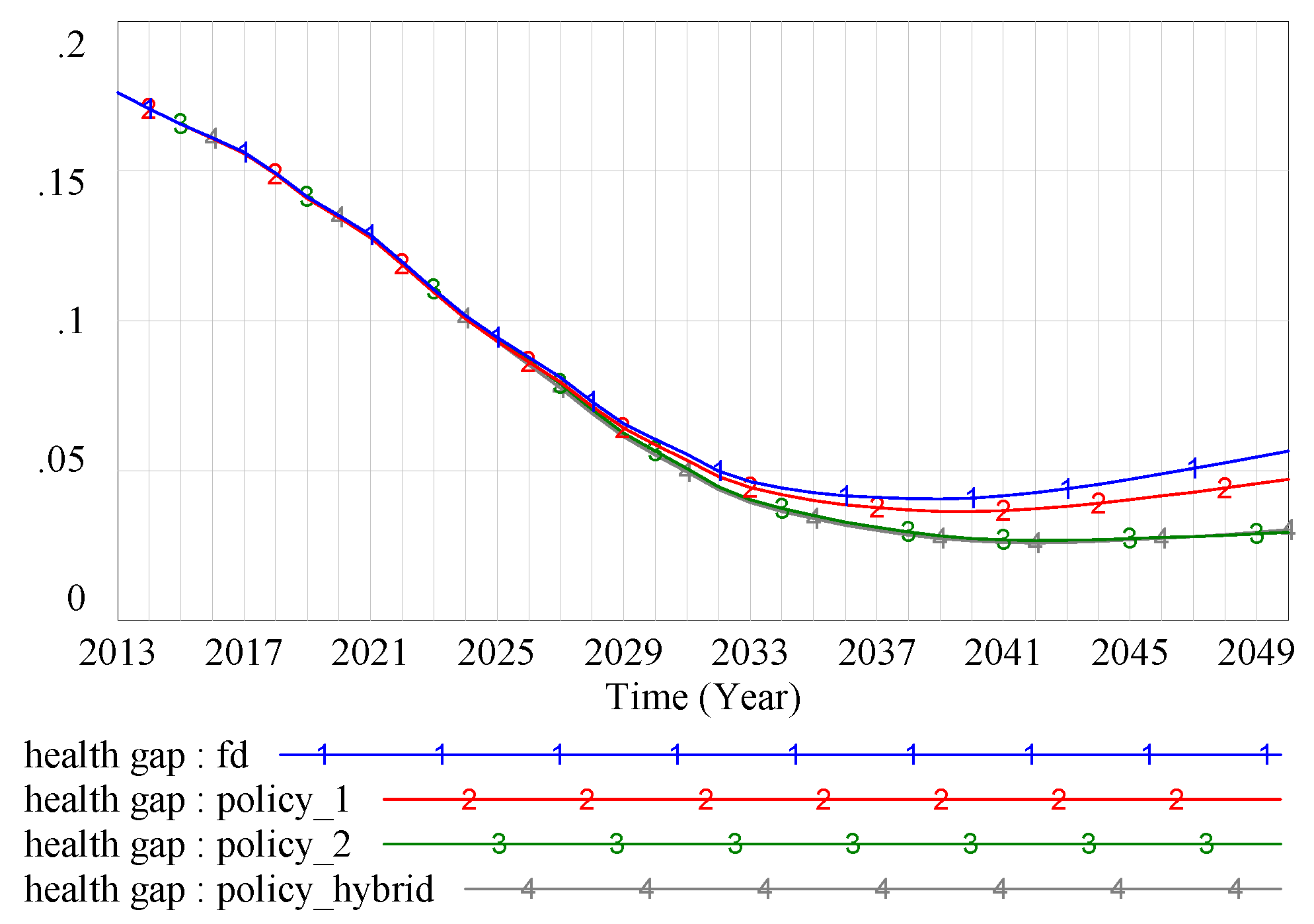
3.3. Policy Conparison
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Marmot, M.G.; Shipley, M.J.; Rose, G. Inequalities in death—Specific explanations of a general pattern? Lancet 1984, 1, 1003–1006. [Google Scholar] [CrossRef]
- Department of Health and Social Security. Inequalities in Health: Report of A Research Working Group; DHSS: London, UK, 1980.
- Humphries, K.H.; van Doorslaer, E. Income-related health inequality in Canada. Soc. Sci. Med. 2000, 50, 663–671. [Google Scholar] [CrossRef]
- Wagstaff, A.; Van Doorslaer, E.; Watanabe, N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J. Econom. 2003, 112, 207–223. [Google Scholar] [CrossRef] [Green Version]
- Robert, S.A.; House, J.S. Socioeconomic inequalities in health: An enduring sociological problem. Handb. Med. Sociol. 2000, 5, 79–97. [Google Scholar]
- Wilkinson, R.G.; Pickett, K.E. Income inequality and socioeconomic gradients in mortality. Am. J. Public Health 2008, 98, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J.M.; Vaccarino, V.; Zhang, H.; Kasl, S.V. Socioeconomic status and type 2 diabetes in African American and non-Hispanic white women and men: Evidence from the Third National Health and Nutrition Examination Survey. Am. J. Public Health 2001, 91, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Crimmins, E.M.; Saito, Y. Trends in healthy life expectancy in the United States, 1970–1990: Gender, racial, and educational differences. Soc. Sci. Med. 2001, 52, 1629–1641. [Google Scholar] [CrossRef]
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social conditions as fundamental causes of health inequalities: Theory, evidence, and policy implications. J. Health Soc. Behav. 2010, 51 (Suppl. 1), S28–S40. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M. Achieving health equity: From root causes to fair outcomes. Lancet 2007, 370, 1153–1163. [Google Scholar] [CrossRef]
- Hurt, L.S.; Ronsmans, C.; Saha, S. Effects of education and other socioeconomic factors on middle age mortality in rural Bangladesh. J. Epidemiol. Community Health 2004, 58, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Vega, J.; Hollstein, R.D.; Delgardo, I.; Perez, J.; Carrasco, M.S.; Marshall, G.; Derek, Y. Socioeconomic health inequities in an intermediate-development nation: Chile, 1985–1996. In Challenging Health Inequities: From Ethics to Action; Evans, T., Whitehead, M., Diderichsen, F., Bhuiya, A., Wirth, M., Eds.; Oxford University Press: New York, NY, USA, 2002. [Google Scholar]
- Murphy, M.; Bobak, M.; Nicholson, A.; Rose, R.; Marmot, M. The widening gap in mortality by educational level in the Russian Federation, 1980–2001. Am. J. Public Health 2006, 96, 1293–1299. [Google Scholar] [CrossRef]
- Li, H.; Zhu, Y. Income, income inequality, and health: Evidence from China. J. Comp. Econ. 2008, 34, 137–172. [Google Scholar]
- Sanders, D.; Baum, F.E.; Benos, A.; Davide, L. Revitalising primary healthcare requires an equitable global economic system–now more than ever. J. Epidemiol. Community Health 2011, 65, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Rasanathan, K.; Montesinos, E.V.; Matheson, D.; Etienne, C.; Evans, T. Primary health care and the social determinants of health: Essential and complementary approaches for reducing inequities in health. J. Epidemiol. Community Health 2011, 65, 656–660. [Google Scholar] [CrossRef] [Green Version]
- Starfield, B. Politics, primary healthcare and health: Was Virchow right? J. Epidemiol. Community Health 2011, 65, 653–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of primary care to health systems and health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef]
- Gorey, K.M. Breast cancer survival in Canada and the USA: Meta-analytic evidence of a Canadian advantage in low-income areas. Int. J. Epidemiol. 2009, 38, 1543–1551. [Google Scholar] [CrossRef]
- Vapattanawong, P.; Hogan, M.C.; Hanvoravongchai, P.; Gakidou, E.; Vos, T.; Lopez, A.D. Reductions in child mortality levels and inequalities in Thailand: Analysis of two censuses. Lancet 2007, 369, 850–855. [Google Scholar] [CrossRef]
- Guttmann, A.; Shipman, S.A.; Lam, K.; Lam, K.; Goodman, D.C.; Stukel, T.A. Primary care physician supply and children’s health care use, access, and outcomes: Findings from Canada. Pediatrics 2010, 125, 1119–1126. [Google Scholar] [CrossRef]
- Cueto, M. The Promise of Primary Health Care. Bull. World Health Organ. 2005, 83, 322. [Google Scholar]
- World Health Organization. The World Health Report 2008: Primary Health Care—Now More Than Ever; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Zhang, Z.Y. China’s village doctors take great strides. Bull. World Health Organ. 2008, 86, 914–915. [Google Scholar] [CrossRef] [Green Version]
- Cueto, M. The origins of primary health care and selective primary health care. Am. J. Public Health 2004, 94, 1864–1874. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Unschuld, P.U. China’s barefoot doctor: Past, present, and future. Lancet 2008, 372, 1865–1867. [Google Scholar] [CrossRef]
- Liu, X.; Hsiao, W.C.L. The cost escalation of social health insurance plans in China: Its implication for public policy. Soc. Sci. Med. 1995, 41, 1095–1101. [Google Scholar] [CrossRef]
- Chen, Z. Launch of the health-care reform plan in China. Lancet 2009, 373, 1322–1324. [Google Scholar] [CrossRef]
- Huang, J.L.; Liu, S.S.; He, R.R.; Fang, S.; Lu, W.; Wu, J.; Liang, H.; Zhang, Y. Factors associated with residents’ contract behavior with family doctors in community health service centers: A longitudinal survey from China. PLoS ONE 2018, 13, 1–16. [Google Scholar] [CrossRef]
- Franks, P.; Clancy, C.M.; Nutting, P.A. Gatekeeping revisited--protecting patients from overtreatment. N. Engl. J. Med. 1992, 327, 424–429. [Google Scholar] [CrossRef]
- Vogt, F.; Hall, S.; Marteau, T.M. General practitioners’ and family physicians’ negative beliefs and attitudes towards discussing smoking cessation with patients: A systematic review. Addiction 2005, 100, 1423–1431. [Google Scholar] [CrossRef]
- Beich, A.; Gannik, D.; Malterud, K. Screening and brief intervention for excessive alcohol use: Qualitative interview study of the experiences of general practitioners. BMJ 2002, 325, 870. [Google Scholar] [CrossRef] [Green Version]
- Regan, J.; Schempf, A.H.; Yoon, J.; Politzer, R.M. The role of federally funded health centers in serving the rural population. J. Rural Health 2003, 19, 117–124. [Google Scholar] [CrossRef]
- O’Malley, A.S.; Forrest, C.B.; Politzer, R.M.; Wulu, J.T.; Shi, L. Health center trends, 1994–2001: What do they portend for the federal growth initiative? Health Aff. 2005, 24, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, M. Economy and Society: An Outline of Interpretive Sociology; Univ of California Press: Berkeley, CA, USA; Los Angeles, CA, USA, 1978. [Google Scholar]
- Adler, N.E.; Rehkopf, D.H. U.S. disparities in health: Descriptions, causes, and mechanisms. Annu. Rev. Public Health 2008, 29, 235–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, N.B.; Armstead, C.A. Toward understanding the association of socioeconomic status and health: A new challenge for the biopsychosocial approach. Psychosom. Med. 1995, 57, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Macinko, J.; Starfield, B.; Xu, J.; Regan, J.; Politzer, R.; Wulu, R.P. Primary care, infant mortality, and low birth weight in the states of the USA. J. Epidemiol. Community Health 2004, 58, 374–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, A.W.; Bury, G.; Plunkett, P.K.; Gibney, D.; Smith, M.; Mullan, E.; Johnson, Z. Randomised controlled trial of general practitioner versus usual medical care in an urban accident and emergency department: Process, outcome, and comparative cost. BMJ 1996, 312, 1135–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, C.H.; Evans, R.G. Heterogeities in health status and the determinants of population health. In Why are Some People Healthy and Others Not? The Determinants of Health of Populations; Evans, R.G., Barer, M.L., Marmor, T.R., Eds.; Aldine de Gruyter: New York, NY, USA, 1994; pp. 35–43. [Google Scholar]
- Sun, Z.X.; Long, J.R.; Duan, G.F.; Tian, W.H. Analysis on the hierarchical system of regional longitudinal medical consortium based on system dynamics. Chin. J. Health Policy 2018, 11, 21–28. [Google Scholar]
- Kennedy, B.M.; Paeratakul, S.; Ryan, D.H.; Bray, G.A. Socioeconomic status and health disparity in the United States. J. Hum. Behav. Soc. Environ. 2007, 15, 13–23. [Google Scholar] [CrossRef]
- Chen, F.; Yang, Y.; Liu, G. Social Change and Socioeconomic Disparities in Health over the Life Course in China: A Cohort Analysis. Am. Sociol. Rev. 2010, 75, 126–150. [Google Scholar] [CrossRef]
- Macinko, J.; Starfield, B.; Shi, L. Quantifying the health benefits of primary care physician supply in the United States. Int. J. Health Serv. 2007, 37, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Macinko, J.; Starfield, B.; Politzer, R.; Wulu, J.; Xu, J. Primary care, social inequalities, and all-cause, heart disease, and cancer mortality in US counties, 1990. Am. J. Public Health 2005, 95, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Yin, T.; Yin, D.; Qin, K.; She, R.; Jing, L.; Huang, J.; Jin, C.; Mao, C.; Zhang, X.; Chen, B. Survey on the service contract signature of primary medical and health institutions in China. Chin. J. Hosp. Adm. 2016, 32, 213–216. [Google Scholar]
- Link, B.G.; Phelan, J. Social conditions as fundamental causes of disease. J. Health Soc. Behav. 1995, Spec No. extra issue, 80–94. [Google Scholar] [CrossRef] [Green Version]










© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.; Zhu, Q.; Guo, J. Can Health Disparity Be Eliminated? The Role of Family Doctor Played in Shanghai, China. Int. J. Environ. Res. Public Health 2020, 17, 5548. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155548
Huang J, Zhu Q, Guo J. Can Health Disparity Be Eliminated? The Role of Family Doctor Played in Shanghai, China. International Journal of Environmental Research and Public Health. 2020; 17(15):5548. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155548
Chicago/Turabian StyleHuang, Jiaoling, Qin Zhu, and Jing Guo. 2020. "Can Health Disparity Be Eliminated? The Role of Family Doctor Played in Shanghai, China" International Journal of Environmental Research and Public Health 17, no. 15: 5548. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155548