The Need for Universal Screening for Postnatal Depression in South Africa: Confirmation from a Sub-District in Pretoria, South Africa


Abstract
:1. Introduction
1.1. The Use of the Edinburg Postnatal Depression Scale to Screen for Postnatal Depression
1.2. Objectives
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Sample
2.3. Study Setting
2.4. Sampling and Sample Size
2.5. Inclusion and Exclusion Criteria
2.6. Data Collection
2.7. Data Analysis
2.8. Reliability and Validity
2.9. Ethical Considerations
3. Results
3.1. Sociodemographic Characteristics of the Participants
3.2. Characteristics of the Babies
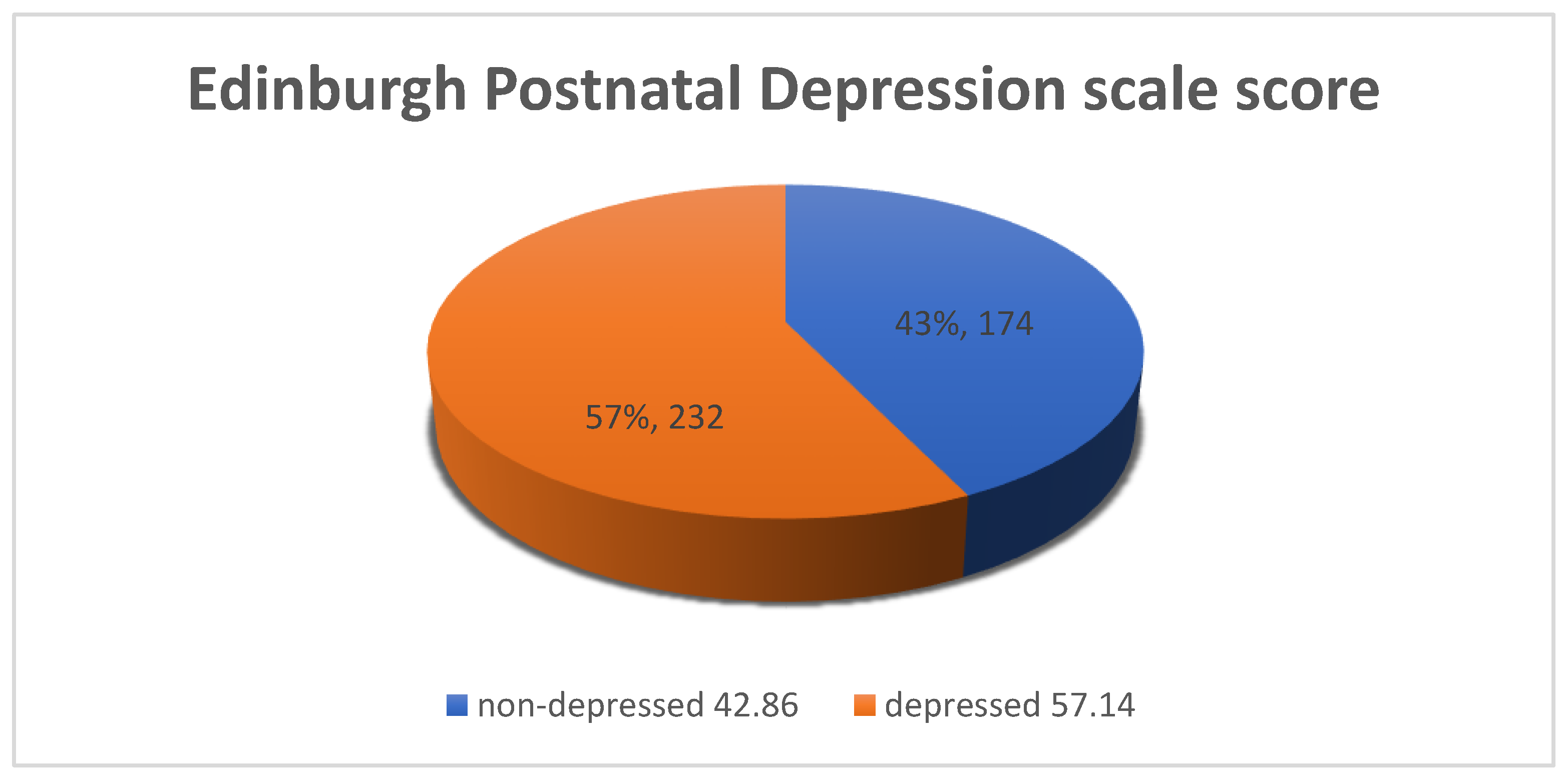
3.3. The Prevalence of Postnatal Depression
3.4. Factors Associated with Postnatal Depression
4. Discussion
5. Conclusions
5.1. Recommendation
5.2. Limitations of the Study
Author Contributions
Funding
Conflicts of Interest
References
- Kathree, T.; Selohilwe, O.; Bhana, A.; Petersen, I. Perceptions of postnatal depression and health care needs in a South African sample: The “mental” in maternal health care. BMC Women’s Health 2014, 14, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, D.E.; Vigod, S.N. Postpartum depression: Pathophysiology, treatment, and emerging therapeutics. Annu. Rev. Med. 2019, 70, 183–196. [Google Scholar] [CrossRef]
- Norhayati, N.M.; Hazlina, N.N.; Asrenee, A.; Emilin, W.M.A.W. Magnitude and risk factors for postpartum symptoms: A literature review. J. Affect. Disord. 2015, 175, 34–52. [Google Scholar] [CrossRef] [Green Version]
- Abajobir, A.A.; Maravilla, J.C.; Alati, R.; Najman, J.M. A systematic review and meta-analysis of the association between unintended pregnancy and perinatal depression. J. Affect. Disord. 2016, 192, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Parsons, C.E.; Young, K.S.; Rochat, T.J.; Kringelbach, M.L.; Stein, A. Postnatal depression and its effects on child development: A review of evidence from low- and middle-income countries. Br. Med. Bull. 2012, 101, 57–79. [Google Scholar] [CrossRef]
- January, J.; Chimbari, M.J. Prevalence and factors associated with postnatal depression among women in two rural districts of Manicaland, Zimbabwe. S. Afr. J. Psychiatry 2018, 24. [Google Scholar] [CrossRef]
- Vythilingum, B.; Field, S.; Kafaar, Z.; Baron, E.; Stein, D.J.; Sanders, L.; Honikman, S. Screening and pathways to maternal mental health care in a South African antenatal setting. Arch. Women’s Ment. Health 2013, 16, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Yeger, B.E.; Muzio, C.; Rinosi, G.; Solano, P.; Geoffroy, P.; Pompili, M.; Amore, M.; Serafini, G. Extreme sensory processing patterns and their relation with clinical conditions among individuals with major affective disorders. Psychiatry Res. Neuroimaging 2016, 236, 112–118. [Google Scholar] [CrossRef]
- Serafini, G.; Gonda, X.; Canepa, G.; Pompili, M.; Rihmer, Z.; Amore, M.; Yeger, B.E. Extreme sensory processing patterns show a complex association with depression, and impulsivity, alexithymia, and hopelessness. J. Affect. Disord. 2017, 210, 249–257. [Google Scholar] [CrossRef]
- Serafini, G.; Canepa, G.; Adavastro, G.; Nebbia, J.; Murri, M.B.; Erbuto, D.; Pocai, B.; Fiorillo, A.; Pompili, M.; Flouri, E.; et al. The relationship between childhood maltreatment and non-suicidal self-injury: A systematic review. Front. Psychiatry 2017, 8, 149. [Google Scholar] [CrossRef]
- Liu, J.; Fang, Y.; Gong, J.; Cui, X.; Meng, T.; Xiao, B.; He, Y.; Shen, Y.; Luo, X. Associations between suicidal behavior and childhood abuse and neglect: A meta-analysis. J. Affect. Disord. 2017, 220, 147–155. [Google Scholar] [CrossRef]
- Myers, S.; Johns, S. Postnatal depression is associated with detrimental life-long and multi-generational impacts on relationship quality. PeerJ 2018, 6, e4305. [Google Scholar] [CrossRef]
- Underwood, L.; Waldie, K.E.; D’Souza, S.; Peterson, E.R.; Morton, S.M.B. A review of longitudinal studies on antenatal and postnatal depression. Arch. Women’s Ment. Health 2016, 19, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, S.D.; Pradhan, R.; Tran, T.D.; Gualano, R.C.; Fisher, J. Reliability and validity of the Edinburgh Postnatal Depression Scale (EPDS) for detecting perinatal common mental disorders (PCMDs) among women in low-and lower-middle-income countries: A systematic review. BMC Pregnancy Childbirth 2016, 16, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Ding, Y.; Ma, Y.; Xin, X.; Zhang, D. Cesarean section and risk of postpartum depression: A meta-analysis. J. Psychosom. Res. 2017, 97, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Tamakoshi, K. Factors Associated with early postpartum maternity blues and depression tendency among japanese mothers with full-term healthy infants. Nagoya J. Med. Sci. 2014, 76, 129–138. [Google Scholar]
- Giri, R.K.; Khatri, R.B.; Mishra, S.R.; Khanal, V.; Sharma, V.D.; Gartoula, R.P. Prevalence and factors associated with depressive symptoms among post-partum mothers in Nepal. BMC Res. Notes 2015, 8, 111. [Google Scholar] [CrossRef] [Green Version]
- Andersson, E.; Hildingsson, I. Mother’s postnatal stress: An investigation of links to various factors during pregnancy and post-partum. Scand. J. Caring Sci. 2016, 30, 782–789. [Google Scholar] [CrossRef]
- Wittkowski, A.; Garrett, C.; Cooper, A.; Wieck, A. The relationship between postpartum depression and beliefs about motherhood and perfectionism during pregnancy. J. Woman’s Reprod. Health 2017, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Hahn-Holbrook, J.; Cornwell-Hinrichs, T.; Anaya, I. Economic and health predictors of national postpartum depression prevalence: A systematic review, meta-analysis, and meta-regression of 291 studies from 56 countries. Front. Psychiatry 2018, 8, 248. [Google Scholar] [CrossRef] [Green Version]
- Mokwena, K.; Shiba, D. Prevalence of postnatal depression symptoms in a primary health care clinic in Pretoria, South Africa: Management of health care services. Afr. J. Phys. Health Educ. Recreat. Dance 2014, 20 (Suppl. 1), 116–127. [Google Scholar]
- Stellenberg, E.L.; Abrahams, J.M. Prevalence of and factors influencing postnatal depression in a rural community in South Africa. Afr. J. Prim. Health Care Fam. Med. 2015, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kozinszky, Z.; Dudas, R.B. Validation studies of the Edinburgh Postnatal Depression Scale for the antenatal period. J. Affect. Disord. 2015, 176, 95–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahi, F.; Lye, M.-S.; Zain, A.M.; Ghazali, S.S.; Zarghami, M. Postnatal depression and its associated factors in women from different cultures. Iran. J. Psychiatry Behav. Sci. 2011, 5, 5–11. [Google Scholar]
- Peltzer, K.; Shikwane, M.E. Prevalence of postnatal depression and associated factors among HIV-positive women in primary care in Nkangala district, South Africa. S. Afr. J. HIV Med. 2011, 12, 24. [Google Scholar] [CrossRef] [Green Version]
- Statistics South Africa. Unemployment Rate. South Africa, Pretoria. 2019. Available online: www.statssa.goc.za (accessed on 18 September 2019).
- Wesselhoeft, R.; Madsen, F.K.; Lichtenstein, M.B.; Sibbersen, C.; Manongi, R.; Mushi, D.L.; Nguyen, H.T.T.; Van, T.N.; Kyhl, H.; Bilenberg, N.; et al. Postnatal depressive symptoms display marked similarities across continents. J. Affect. Disord. 2020, 261, 58–66. [Google Scholar] [CrossRef]
- Rollè, L.; Giordano, M.; Santoniccolo, F.; Trombetta, T. Prenatal attachment and perinatal depression: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2644. [Google Scholar] [CrossRef] [Green Version]
- Tsai, A.C.; Tomlinson, M.; Comulada, W.S.; Rotheram-Borus, M.J. Intimate partner violence and depression symptom severity among South African women during pregnancy and postpartum: Population-based prospective cohort study. PLoS Med. 2016, 13, e1001943. [Google Scholar] [CrossRef] [Green Version]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Evagorou, O.; Arvaniti, A.; Samakouri, M. Cross-cultural approach of postpartum depression: Manifestation, practices applied, risk factors and therapeutic interventions. Psychiatry Q. 2016, 87, 129–154. [Google Scholar] [CrossRef]
- Adjaye-Gbewonyo, K.; Avendaño, M.; Subramanian, S.V.; Kawachi, I. Income inequality and depressive symptoms in South Africa: A longitudinal analysis of the National Income Dynamics Study. Health Place 2016, 42, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Camps Meschino, D.; Philipp, D.; Israel, A.; Vigod, S.N. Maternal-infant mental health: Postpartum group intervention. Arch. Women’s Ment. Health 2016, 19, 243–251. [Google Scholar] [CrossRef]
- Hegde, S.; Latha, K.S.; Bhat, S.M.; Sharma, P.S.; Kamath, A. Postpartum depression: Prevalence and associated factors among women in India. J. Women’s Health Issues Care 2012, 1, 1–7. [Google Scholar]
- Bener, A.; Burgut, F.T.; Ghuloum, S.; Sheikh, J.I. A study of postpartum depression in a fast developing country: Prevalence and related factors. Int. J. Psychiatry Med. 2012, 43, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Taherifard, P.; Delpisheh, A.; Shiraly, R.; Afkhamzadeh, A.; Veisani, Y. Socioeconomic, psychiatric and materiality determinants and risk of postpartum depression in border city of ilam, Western Iran. Depress. Res. Treat. 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Peltzer, K.; Rodriguez, V.J.; Jones, D. Prevalence of prenatal depression and associated factors among HIV-positive women in primary care in Mpumalanga province, South Africa. SAHARA-J J. Soc. Asp. HIV/AIDS 2016, 13, 60–67. [Google Scholar] [CrossRef]
- Kendall-Tackett, K.A. Depression in New Mothers: Causes, Consequences and Treatment Alternatives; Taylor & Francis: Abingdon, UK, 2016. [Google Scholar]
- González, G.; Moraes, M.; Sosa, C.; Umpierrez, E.; Duarte, M.; Cal, J.; Ghione, A. Maternal postnatal depression and its impact on child neurodevelopment: A cohort study. Rev. Chil. Pediatr. 2017, 88, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, C. Maternal depression and child development in sub-Saharan Africa. In Child and Adolescent Development: An Expanded Focus on Public Health in Africa; UCT Press: Cape Town, South Africa, 2018. [Google Scholar]
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of persistent and severe postnatal depression with child outcomes. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef] [Green Version]
- Soboka, M.; Feyissa, G.T. The impact of maternal postnatal depression on infant growth in sub-Saharan African countries: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 58–67. [Google Scholar] [CrossRef]
- Judd, F.; Lorimer, S.; Thomson, R.H.; Hay, A. Screening for depression with the Edinburgh Postnatal Depression Scale and finding borderline personality disorder. Aust. N. Z. J. Psychiatry 2019, 53, 424–432. [Google Scholar] [CrossRef]
- Howard, L.; Ryan, E.G.; Trevillion, K.; Anderson, F.; Bick, D.; Bye, A.; Byford, S.; O’Connor, S.; Sands, P.; Demilew, J.; et al. Accuracy of the Whooley questions and the Edinburgh Postnatal Depression Scale in identifying depression and other mental disorders in early pregnancy. Br. J. Psychiatry 2018, 212, 50–56. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Frequency (n) | Percentage (%) |
|---|---|---|
| Mother’s Age | ||
| <30 | 250 | 61.58% |
| ≥30 | 156 | 38.42% |
| 406 | 100% | |
| Home Language | ||
| Afrikaans | 5 | 1.23% |
| English | 46 | 11.36% |
| South African local languages | 223 | 55.06% |
| Other African languages | 132 | 32.35% |
| 406 | 100% | |
| Level of Education Completed | ||
| No formal education | 4 | 0.99% |
| Primary | 53 | 13.05% |
| Secondary | 307 | 75.62% |
| Tertiary | 42 | 10.34% |
| 406 | 100% | |
| Marital Status | ||
| Ever married | 293 | 72.17% |
| Never married | 113 | 27.83% |
| 406 | 100% | |
| Employment Status | ||
| Unemployed | 309 | 76.11% |
| Employed | 97 | 23.89% |
| 406 | 100% | |
| Who Does the Participant Live With? | ||
| Alone | 37 | 9.11% |
| Partner/husband | 289 | 71.18% |
| Family | 79 | 19.46% |
| Friend | 1 | 0.25% |
| 406 | 100% | |
| Household Income | ||
| R 0–499 | 85 | 20.94% |
| R 500–1000 | 114 | 28.08% |
| R 1001–2000 | 111 | 27.34% |
| R 2001–5000 | 61 | 15.02% |
| R 5000–8000 | 19 | 4.68% |
| R > 8000 | 16 | 3.94% |
| 406 | 100 |
| Variable | Frequency (n) | Percentage (%) |
|---|---|---|
| Parity | ||
| 1–2 babies | 297 | 73.15% |
| 3–4 babies | 104 | 25.62% |
| 5–6 babies | 5 | 1.23% |
| 406 | 100% | |
| Baby’s Age in Weeks | ||
| 1–10 weeks | 177 | 43.6% |
| 11–24 weeks | 124 | 30.54% |
| 25–48 weeks | 105 | 25.86% |
| 406 | 100% | |
| Delivery Method | ||
| Normal vaginal delivery | 315 | 77.59% |
| Caesarean section | 91 | 22.41% |
| 406 | 100% | |
| Baby Planned | ||
| No | 126 | 31.03% |
| Yes | 280 | 68.97% |
| 406 | 100% | |
| Mother Breastfeeding | ||
| No | 76 | 18.72% |
| Yes | 330 | 81.28% |
| 406 | 100% | |
| Baby’s Health | ||
| Good | 369 | 90.89% |
| Sometimes not well | 29 | 7.14% |
| Mostly not well | 8 | 1.97% |
| 406 | 100% | |
| Baby’s Sex | ||
| Girl | 206 | 50.74% |
| Boy | 200 | 49.26% |
| 406 | 100% | |
| Preferred Sex | ||
| Girl | 163 | 40.15 |
| Boy | 192 | 47.29 |
| No preference | 49 | 12.07 |
| I didn’t want a baby | 2 | 0.49% |
| 406 | 100% |
| Variable | No PND n (%) | PND n (%) | Chi2 | p-Value |
|---|---|---|---|---|
| Age of Mother | 134.79 | 0.00 | ||
| <30 years | 174 (100%) | 76 (32.76%) | ||
| ≥30 years | 0 (0) | 156 (67.24%) | ||
| Total | 174 | 232 | ||
| Home Language | 103.22 | 0.00 | ||
| Afrikaans | 5 (2.87%) | 0 | ||
| English | 46 (26.44%) | 0 | ||
| Local South African languages | 100 (57.47%) | 123 (53.02%) | ||
| Other African languages | 23 (13.22%) | 110 (41.51%) | ||
| Total | 174 | 232 | ||
| Level of Education | 110.32 | 0.00 | ||
| No formal education | 4 (2.30%) | 0 (0) | ||
| Primary | 53 (30.46%) | 0 (0) | ||
| Secondary | 117 (67.24%) | 190 (81.90%) | ||
| Tertiary | 0 (0) | 42 (18.10%) | ||
| Total | 174 | 232 | ||
| Marital Status | 117.44 | 0.00 | ||
| Never married | 0 (0) | 113 (48.71%) | ||
| Ever married | 174 (100%) | 119 (51.29%) | ||
| Total | 174 | 232 | ||
| Employment Status | 169.9 | 0.00 | ||
| Unemployed | 77 (44.25%) | 232 (100%) | ||
| Employed | 97 (55.75%) | 0 (0) | ||
| Total | 174 | 232 | ||
| Live With | 59.31 | 0.00 | ||
| Alone | 37 (21.26%) | 0 (0) | ||
| Family | 22 (12.64% | 57 (24.57%) | ||
| Husband/partner | 114 (65.52%) | 175 (75.43%) | ||
| Friend | 1 (0.57%) | 0 (0) | ||
| Total | 174 | 232 | ||
| Occupants: Adults | 72.41 | 0.00 | ||
| <3 | 141 (100%) | 187 (70.57%) | ||
| ≥3 | 0 (0) | 78 (29.43%) | ||
| Total | 174 | 232 | ||
| Variable | No PND n (%) | PND n (%) | Chi2 | p-Value |
| Occupants: Children | 95.59 | 0.00 | ||
| <3 | 174 (100%) | 135 (58.19%) | ||
| ≥3 | 0 (0) | 97 (41.81%) | ||
| Total | 174 | 232 | ||
| Household Income | 35.22 | 0.00 | ||
| R < 2000 | 158 (90.80%) | 152 (65.52%) | ||
| R ≥ 2000 | 16 (9.20%) | 80 (34.48%) | ||
| Total | 174 | 232 | ||
| Father’s Financial Support | 128.7 | 0.00 | ||
| No | 78 (44.83%) | 0 (0) | ||
| Yes | 96 (55.17%) | 232 (100%) | ||
| Total | 174 | 232 | ||
| Parity | 111.75 | 0.00 | ||
| <3 | 174 (100%) | 123 (53.02%) | ||
| ≥3 | 0 (0) | 109 (46.98%) | ||
| Total | 174 | 232 | ||
| Baby’s Age in Weeks | 113.40 | 0.00 | ||
| 1–10 weeks | 91 (52.30%) | 86 (37.07%) | ||
| 11–24 weeks | 83 (47.70%) | 71 (26.80%) | ||
| 25–48 weeks | 0 (0) | 105 (45.26%) | ||
| Total | 174 | 232 | ||
| Method of Delivery | 156.39 | 0.00 | ||
| Normal vaginal delivery | 83 (47.70%) | 265 (100%) | ||
| Caesarean section | 91 (52.30%) | 0 (0) | ||
| Total | 174 | 232 | ||
| Planned Baby | 243.60 | 0.00 | ||
| Unplanned baby | 126 (72.41%) | 0 (0) | ||
| Planned baby | 48 (27.59% | 232 (100%) | ||
| Total | 174 | 232 | ||
| Baby’s Health | 30.53 | 0.00 | ||
| Healthy | 174 (100%) | 195 (84.05%) | ||
| Sickly | 0 (0) | 37 (15.95%) | ||
| Total | 174 | 232 | ||
| Baby’s Preferred Sex | 227.89 | 0.00 | ||
| Girl | 0 (0) | 163 (70.26%) | ||
| Boy | 125 (71.84%) | 67 (28.88%) | ||
| No preferred sex | 49 (28.16%) | 0 (0) | ||
| I didn’t want a baby | 0 (0) | 2 (0.86%) | ||
| Total | 174 | 232 | ||
| Baby Breastfed | 124.67 | 0.00 | ||
| No | 76 (43.68%) | 0 (0) | ||
| Yes | 98 (56.32%) | 232 (100%) | ||
| Total | 174 | 232 | ||
| Currently Have Partner | 95.71 | 0.00 | ||
| No | 61(35.06%) | 0 (0) | ||
| Yes | 113 (64.94%) | 265 (100%) | ||
| Total | 174 | 232 | ||
| Support From Partner | 216.53 | 0.00 | ||
| No | 116 (66.67%) | 0 (0) | ||
| Yes | 58 (33.33%) | 232(100%) | ||
| Total | 174 | 232 | ||
| Partner has Other Sexual Partners | 190.01 | 0.00 | ||
| No | 174 (100%) | 76 (32.76%) | ||
| Yes | 0 (0) | 156 (67.24%) | ||
| Total | 174 | 232 | ||
| Has Support in Difficult Times | 47.89 | 0.00 | ||
| No | 33 (81.03%) | 0 (0) | ||
| Yes | 141(81.03 | 232 (100%) | ||
| Total | 174 | 232 | ||
| Who Supports | 224.40 | 0.00 | ||
| No one | 0 (0) | 31 (10.0%) | ||
| Family | 15 (8.62%) | 159 (68.53%) | ||
| Husband/partner | 115 (66.09%) | 42 (18.10%) | ||
| Friend | 44 (25.29%) | 0 (0) | ||
| Total | 174 | 232 | ||
| Threatened to Hit | 0.26 | 0.61 | ||
| No | 154 (88.51%) | 209 (90.09%) | ||
| Yes | 20 (11.49%) | 23 (9.31%) | ||
| Total | 174 | 232 | ||
| Partner Drinking Alcohol | 26.72 | 0.00 | ||
| No | 73 (41.95%) | 43 (18.53% | ||
| Yes | 101 (58.05%) | 189 (81.47%) | ||
| Total | 174 | 232 | ||
| Has Experienced Severe Stress | 378.25 | 0.00 | ||
| No | 167 (95.98%) | 0 (0) | ||
| Yes | 7 (4.02) | 232 (100%) | ||
| Total | 174 | 232 | ||
| Reason for Stress | 41.94 | 0.00 | ||
| Severe financial crisis | 91 (52.30%) | 63 (96.92%) | ||
| Death of a close person | 26 (14.94%) | 0 (0) | ||
| Illness | 22 (12.64%) | 1(1.54%) | ||
| Cheating and not supportive | 22 (12.64%) | 0 (0) | ||
| Changed jobs and place | 8 (4.60%) | 0 (0) | ||
| Regret, unhappiness, and life-threatening crime | 5 (2.87%) | 1 (1.54%) | ||
| Total | 174 | 232 |
| Variable | Odds Ratio | Std. Error | Z | P > |Z| | 95% Confidence Interval |
|---|---|---|---|---|---|
| Household income | 1.44 | 0.11 | 4.57 | 0.00 | 1.23–1.67 |
| Baby’s age in weeks | 1.34 | 0.07 | 5.41 | 0.00 | 1.09–1.24 |
| Currently have partner | 0.45 | 0.11 | −3.4 | 0.00 | 0.28–0.71 |
| Support difficult times | 76 | 76.5 | 4.30 | 0.00 | 10.57–546.51 |
| Preferred sex | 0.47 | 0.05 | −6.82 | 0.00 | 0.37–0.58 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mokwena, K.; Masike, I. The Need for Universal Screening for Postnatal Depression in South Africa: Confirmation from a Sub-District in Pretoria, South Africa. Int. J. Environ. Res. Public Health 2020, 17, 6980. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17196980
Mokwena K, Masike I. The Need for Universal Screening for Postnatal Depression in South Africa: Confirmation from a Sub-District in Pretoria, South Africa. International Journal of Environmental Research and Public Health. 2020; 17(19):6980. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17196980
Chicago/Turabian StyleMokwena, Kebogile, and Itumeleng Masike. 2020. "The Need for Universal Screening for Postnatal Depression in South Africa: Confirmation from a Sub-District in Pretoria, South Africa" International Journal of Environmental Research and Public Health 17, no. 19: 6980. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17196980