A Systematic Review of Job Demands and Resources Associated with Compassion Fatigue in Mental Health Professionals

Abstract
:1. Introduction
2. Materials and Methods
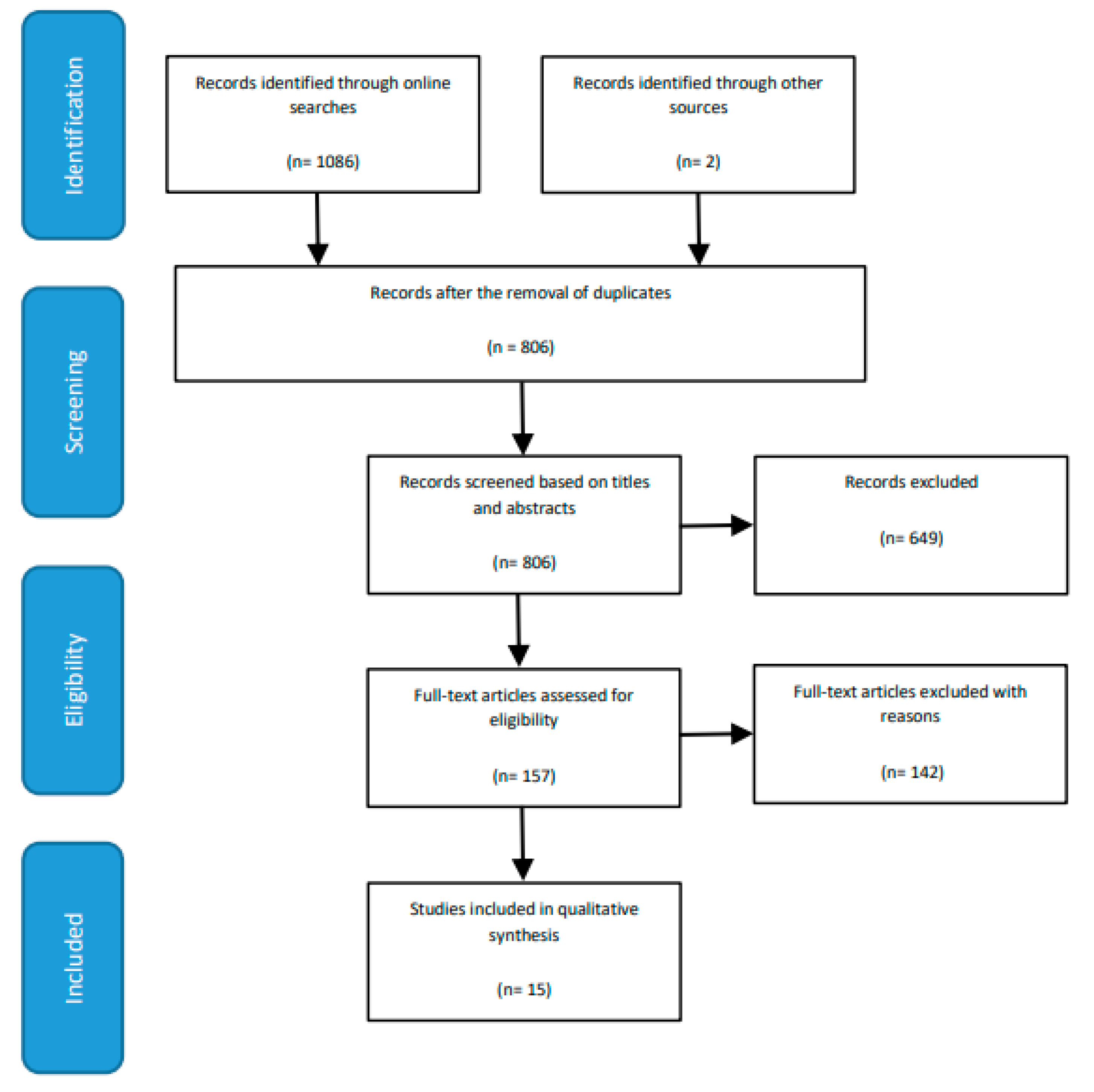
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection, Data Extraction and Risk of Bias (Quality) Assessment
2.4. Strategy for Data Synthesis
3. Results
3.1. Characteristics of Included Studies
3.2. Quality Assessment of Studies
3.3. Characteristics of Compassion Fatigue Measures
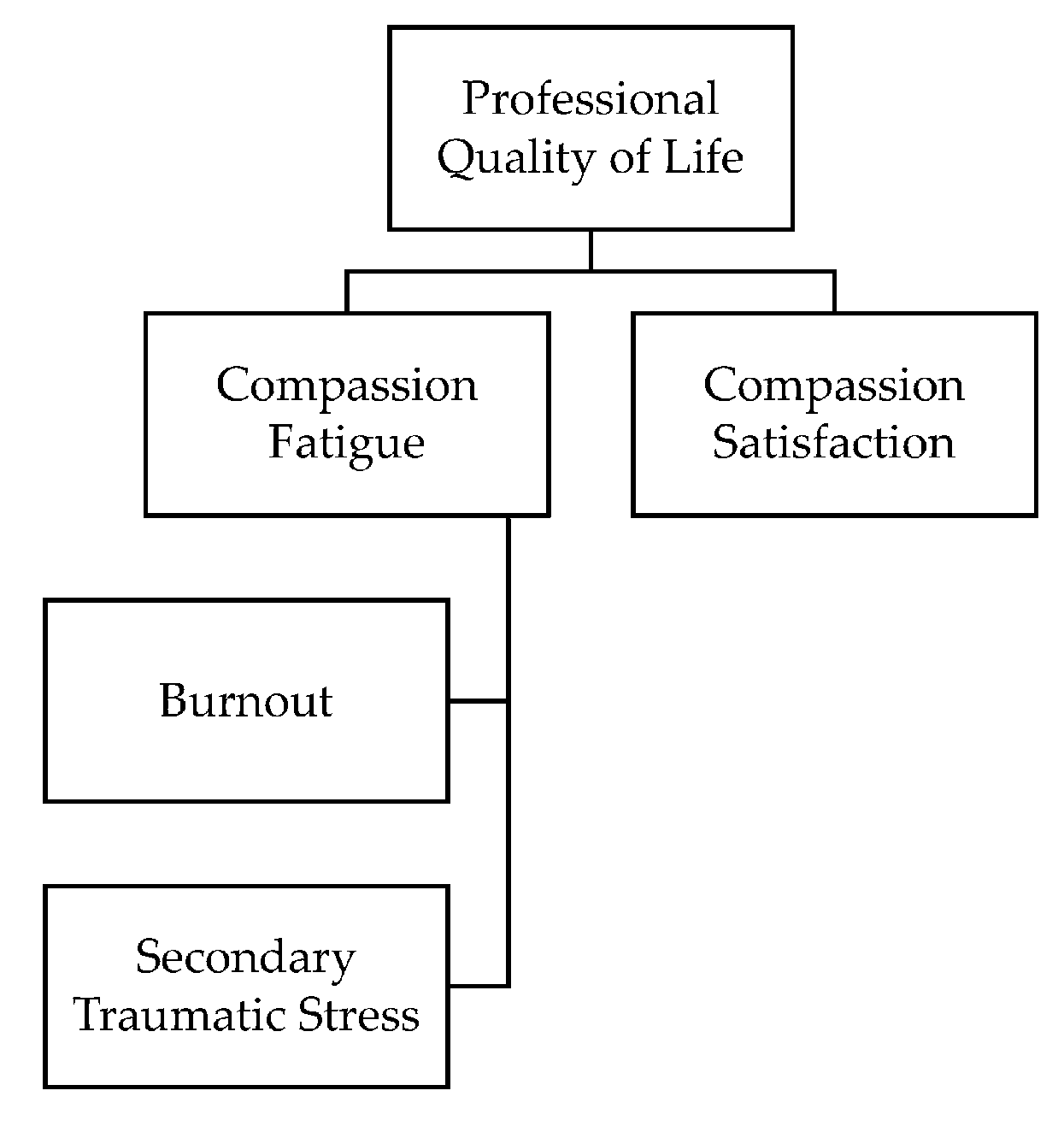
3.4. Theoretical Framework
3.5. Qualitative Synthesis of Themes
3.5.1. Job Demands Associated with Compassion Fatigue
Workplace Trauma
Workload
Therapeutic Settings
3.5.2. Job Resources Associated with Compassion Fatigue
Support from Co-Workers
Support from Supervisors
Organisational Resources and Support
3.6. Additional Findings
3.6.1. Association between Secondary Traumatic Stress and Burnout
3.6.2. Compassion Satisfaction
4. Discussion
4.1. Implications and Directions for Further Research
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gladding, S.T. Counseling: A Comprehensive Profession; Pearson: New York, NY, USA, 2013. [Google Scholar]
- Rogers, C.R. On Becoming a Person: A Therapist’s View of Psychotherapy; Constable: London, UK, 1967. [Google Scholar]
- Kohut, H. On Empathy. Int. J. Psychoanal. Self Psychol. 2010, 5, 122–131. [Google Scholar]
- Beck, A.T. Cognitive Therapy of Depression; Guilford Press: New York, NY, USA, 1979. [Google Scholar]
- Freud, S. 1856–1939 The Standard Edition of the Complete Psychological Works of Sigmund Freud: Early Psycho-Analytic Publications. Moses and Monotheism, An Outline of Psycho-Analysis Other Works; Vintage: London, UK, 2001; Volume 23, pp. 1937–1939. [Google Scholar]
- Flückiger, C.; Del Re, A.C.; Wampold, B.E.; Symonds, D.; Horvath, A.O. How central is the alliance in psychotherapy? A multilevel longitudinal meta-analysis. J. Couns. Psychol. 2012, 59, 10. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.; Bohart, A.C.; Watson, J.C.; Greenberg, L.S. Empathy; Oxford University Press: New York, NY, USA, 2011; pp. 132–152. [Google Scholar]
- Morrissette, P.J. The Pain of Helping: Psychological Injury of Helping Professionals; Brunner-Routledge: New York, NY, USA, 2004; p. xxiv, 149. [Google Scholar]
- Rothschild, B.; Rand, M. Help for the Helper: The Psychophysiology of Compassion Fatigue and Vicarious Trauma; W.W. Norton: New York, NY, USA, 2006. [Google Scholar]
- Newell, J.M.; MacNeil, G.A. Professional burnout, vicarious trauma, secondary traumatic stress, and compassion fatigue: A review of theoretical terms, risk factors, and preventive methods for clinicians and researchers. Best Pract. Ment. Health Int. J. 2010, 6, 57–68. [Google Scholar]
- Canfield, J. Secondary Traumatization, Burnout, and Vicarious Traumatization: A Review of the Literature as It Relates to Therapists Who Treat Trauma. Smith Coll. Stud. Soc. Work 2005, 75, 81–101. [Google Scholar] [CrossRef]
- Jachens, L.; Houdmont, J.; Thomas, R. Work-related stress in a humanitarian context: A qualitative investigation. Disasters 2018, 42, 619–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figley, C.R. Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized; Brunner/Mazel psychological stress series, No. 23; Brunner/Mazel: Philadelphia, PA, USA, 1995. [Google Scholar]
- Stamm, B. Secondary Traumatic Stress: Self-Care Issues for Clinicians, Researchers, and Educators; Sidran Press: Baltimore, MD, USA, 1999. [Google Scholar]
- Maslach, C.; Jackson, S. The measurement of experienced burnout. J. Occup. Behav. 1981, 2, 99. [Google Scholar] [CrossRef]
- Diehm, R.M.; Mankowitz, N.N.; King, R.M. Secondary traumatic stress in Australian psychologists: Individual risk and protective factors. Traumatology 2019, 25, 196–202. [Google Scholar] [CrossRef]
- Makadia, R.; Sabin-Farrell, R.; Turpin, G. Indirect exposure to client trauma and the impact on trainee clinical psychologists: Secondary traumatic stress or vicarious traumatization? Clin. Psychol. Psychother. 2017, 24, 1059. [Google Scholar] [CrossRef] [Green Version]
- Ivicic, R.; Motta, R. Variables associated with secondary traumatic stress among mental health professionals. Traumatology 2017, 23, 196–204. [Google Scholar] [CrossRef]
- Mccormack, H.M.; Macintyre, T.E.; O’Shea, D.; Herring, M.P.; Campbell, M.J. The Prevalence and Cause(s) of Burnout among Applied Psychologists: A Systematic Review. Front. Psychol. 2018, 9, 1897. [Google Scholar] [CrossRef] [Green Version]
- Berjot, S.; Altintas, E.; Grebot, E.; Lesage, F. Burnout risk profiles among French psychologists. Burn. Res. 2017, 7, 10–20. [Google Scholar] [CrossRef]
- O’connor, K.; Neff, D.M.; Pitman, S. Burnout in mental health professionals: A systematic review and meta-analysis of prevalence and determinants. Eur. Psychiatry 2018, 53, 74–99. [Google Scholar] [CrossRef]
- Rauvola, R.S.; Vega, D.M.; Lavigne, K.N. Compassion Fatigue, Secondary Traumatic Stress, and Vicarious Traumatization: A Qualitative Review and Research Agenda. Occup. Health Sci. 2019, 3, 297–336. [Google Scholar] [CrossRef]
- Bride, B.; Radey, M.; Figley, C. Measuring Compassion Fatigue. Clin. Soc. Work J. 2007, 35, 155–163. [Google Scholar] [CrossRef]
- McCann, I.L.; Pearlman, L.A. Vicarious traumatization: A framework for understanding the psychological effects of working with victims. J. Trauma. Stress 1990, 3, 131–149. [Google Scholar] [CrossRef]
- Shoji, K.; Lesnierowska, M.; Smoktunowicz, E.; Bock, J.; Luszczynska, A.; Charles, C.B.; Cieslak, R. What Comes First, Job Burnout or Secondary Traumatic Stress? Findings from Two Longitudinal Studies from the U.S. and Poland. PLoS ONE 2015, 10, e0136730. [Google Scholar] [CrossRef] [PubMed]
- Cocker, F.; Joss, N. Compassion Fatigue among Healthcare, Emergency and Community Service Workers: A Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 618. [Google Scholar] [CrossRef] [Green Version]
- Negash, S.; Sahin, S. Compassion fatigue in marriage and family therapy: Implications for therapists and clients. J. Marital Fam. 2011, 37, 1–13. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.; Nachreiner, F.; Schaufeli, W. A model of burnout and life satisfaction among nurses. J. Adv. Nurs. 2000, 32, 454–464. [Google Scholar] [CrossRef]
- Mathieu, F. Running on empty: Compassion fatigue in health professionals. Rehab Community Care Med. 2007, 4, 1–7. [Google Scholar]
- Sodeke-Gregson, E.; Holttum, S.; Billings, J. Compassion satisfaction, burnout, and secondary traumatic stress in UK therapists who work with adult trauma clients. Eur. J. Psychotraumatology 2013, 4, 21869. [Google Scholar] [CrossRef] [PubMed]
- MAILONLINE REPORTER Almost HALF of NHS Psychotherapists Feel Depressed as a Result of Service Cuts That Are Fueling the Ongoing Crisis. Available online: https://www.dailymail.co.uk/health/article-4316648/Depression-reported-half-NHS-psychotherapists.html (accessed on 15 August 2020).
- Barr, P. Compassion fatigue and compassion satisfaction in neonatal intensive care unit nurses: Relationships with work stress and perceived social support. Traumatology 2017, 23, 214–222. [Google Scholar] [CrossRef]
- Connally, D. The Relationship between Clinician Sex, Ethnicity, Sexual Identity and Secondary Traumatic Stress. J. Gay Lesbian Ment. Health 2012, 16, 306–321. [Google Scholar]
- Rossi, A.; Cetrano, G.; Pertile, R.; Rabbi, L.; Donisi, V.; Grigoletti, L.; Curtolo, C.; Tansella, M.; Thornicroft, G.; Amaddeo, F. Burnout, compassion fatigue, and compassion satisfaction among staff in community-based mental health services. Psychiatry Res. 2012, 200, 933–938. [Google Scholar] [CrossRef] [Green Version]
- Rochell, S.; Buonanno, L. Charting the attitudes of county child protection staff in a post-crisis environment. Child. Youth Serv. Rev. 2018, 86, 166. [Google Scholar] [CrossRef]
- Gleichgerrcht, E.; Decety, J. Empathy in Clinical Practice: How Individual Dispositions, Gender, and Experience Moderate Empathic Concern, Burnout, and Emotional Distress in Physicians. PLoS ONE 2013, 8, e61526. [Google Scholar]
- Salloum, A.; Kondrat, D.C.; Johnco, C.; Olson, K.R. The role of self-care on compassion satisfaction, burnout and secondary trauma among child welfare workers. Child. Youth Serv. Rev. 2015, 49, 54–61. [Google Scholar]
- Jacobson, J.M. Risk of Compassion Fatigue and Burnout and Potential for Compassion Satisfaction Among Employee Assistance Professionals: Protecting the Workforce. Traumatology 2012, 18, 64–72. [Google Scholar] [CrossRef]
- Hamid, A.A.R.M.; Musa, S.A. The mediating effects of coping strategies on the relationship between secondary traumatic stress and burnout in professional caregivers in the UAE. J. Ment. Health 2017, 26, 28–35. [Google Scholar]
- Thomas, J. Association of Personal Distress with Burnout, Compassion Fatigue, and Compassion Satisfaction among Clinical Social Workers. J. Soc. Serv. Res. 2013, 39, 365–379. [Google Scholar]
- Valavanis, S. The Relationships between Nurses’ Emotional Intelligence, Attachment Style, Burnout, Compassion and Stigma. Ph.D. Thesis, Lancaster University, Lancaster, UK, 2019. [Google Scholar] [CrossRef]
- Roden-Foreman, J.W.; Bennett, M.M.; Rainey, E.E.; Garrett, J.S.; Powers, M.B.; Warren, A.M. Secondary traumatic stress in emergency medicine clinicians. Cogn. Behav. Ther. 2017, 46, 522–532. [Google Scholar] [CrossRef]
- Borges, E.M.d.N.; Fonseca, C.I.N.d.; Baptista, P.C.P.; Queirós, C.M.L.; Baldonedo-Mosteiro, M.; Mosteiro-Diaz, M.P. Compassion fatigue among nurses working on an adult emergency and urgent care unit. Rev. Lat. Am. Enferm. 2019, 27, e3175. [Google Scholar] [CrossRef]
- Creamer, T.L.; Liddle, B.J. Secondary traumatic stress among disaster mental health workers responding to the September 11 attacks. J. Trauma. Stress 2005, 18, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Sprang, G.; Clark, J.J.; Whitt-Woosley, A. Compassion Fatigue, Compassion Satisfaction, and Burnout: Factors Impacting a Professional’s Quality of Life. J. Loss Trauma 2007, 12, 259–280. [Google Scholar] [CrossRef]
- Singh, J.; Hassard, J. Emotional Labour, Emotional Regulation, and Secondary Traumatic Stress among Allied Mental Health Professionals in the UK: A Pilot Study, Proceedings of the 14th European Academy of Occupational Health Psychology Conference: ‘Promoting Healthy and Sustainable Work’, Cyprus, Cyprus, 2–4 September 2020; European Academy of Occupational Health Psychology: Nottingham, UK, 2020; p. 188. [Google Scholar]
- Finzi-Dottan, R.; Kormosh, M.B. The spillover of compassion fatigue into marital quality: A mediation model. Traumatology 2018, 24, 113. [Google Scholar] [CrossRef]
- Phelps, A.; Lloyd, D.; Creamer, M.; Forbes, D. Caring for Carers in the Aftermath of Trauma. J. Aggress. Maltreat. Trauma 2009, 18, 313–330. [Google Scholar] [CrossRef]
- Badger, K.; Royse, D.; Craig, C.D. Hospital social workers and indirect trauma exposure: An exploratory study of contributing factors. Health Soc. Work 2008, 33, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Turgoose, D.; Maddox, L. Predictors of compassion fatigue in mental health professionals: A narrative review. Traumatology 2017, 23, 172–185. [Google Scholar] [CrossRef]
- McManus, S.; Bebbington, P.; Jenkins, R.; Brugha, T. Mental Health and Wellbeing in England. Adult Psychiatric Morbidity Survey 2014; Key Non Parliam. Pap. Health; 2016; pp. 1–405. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/556596/apms-2014-full-rpt.pdf (accessed on 30 July 2020).
- Community and Mental Health Team. Health and Social Care Information Centre Monthly MHMDS Report: August 2014 final data. Health Soc. Care Inf. Cent. 2014, 1–10. Available online: https://files.digital.nhs.uk/publicationimport/pub15xxx/pub15733/mhmds-monthly-exec-jul-2014.pdf (accessed on 30 July 2020).
- Community and Mental Health Team Mental Health Act Statistics. Annual Figures 2016/17: Experimental Statistics. Health Soc. Care Inf. Cent. 2017, 1–27. [Google Scholar]
- Community and Mental Health Analysis Team Mental Health Act Statistics. Annual Figures England, 2017–2018. Health Soc. Care Inf. Cent. 2018, 1–23. [Google Scholar]
- Mental Health Analysis Team Mental Health Act Statistics. Annual Figures England, 2018–2019. Health Soc. Care Inf. Cent. 2019, 1–23. [Google Scholar]
- Belur, J.; Tompson, L.; Thornton, A.; Simon, M. Interrater Reliability in Systematic Review Methodology: Exploring Variation in Coder Decision-Making. Sociol. Methods Res. 2018. [Google Scholar] [CrossRef] [Green Version]
- Gough, D.; Oliver, S.; Thomas, J. An Introduction to Systematic Reviews; SAGE: Los Angeles, CA, USA; London, UK, 2017. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Lamontagne, A.D.; Keegel, T.; Louie, A.M.; Ostry, A.; Landsbergis, P.A. A Systematic Review of the Job-stress Intervention Evaluation Literature, 1990–2005. Int. J. Occup. Environ. Health 2007, 13, 268–280. [Google Scholar] [CrossRef]
- Montano, D.; Hoven, H.; Siegrist, J. Effects of organisational-level interventions at work on employees’ health: A systematic review. BMC Public Health 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Corbière, M.; Shen, J.; Rouleau, M.; Dewa, C.S. A systematic review of preventive interventions regarding mental health issues in organizations. Work 2009, 33, 81–116. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009. [Google Scholar] [CrossRef] [Green Version]
- Leahey, T.H. A History of Psychology: Main Currents in Psychological Thought; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2004. [Google Scholar]
- Crowe, M. Crowe Critical Appraisal Tool (CCAT) User Guide; Conchra House: Scotland, UK, 2013. [Google Scholar]
- Crowe, M.; Sheppard, L.; Campbell, A. Comparison of the effects of using the Crowe Critical Appraisal Tool versus informal appraisal in assessing health research: A randomised trial. Int. J. Evid. Based Healthc. 2011, 9, 444. [Google Scholar] [CrossRef]
- Crowe, M.; Sheppard, L.; Campbell, A. Reliability analysis for a proposed critical appraisal tool demonstrated value for diverse research designs. J. Clin. Epidemiol. 2012, 65, 375–383. [Google Scholar] [CrossRef]
- Crowe, M.; Sheppard, L. A general critical appraisal tool: An evaluation of construct validity. Int. J. Nurs. Stud. 2011, 48, 1505–1516. [Google Scholar] [PubMed]
- Caceres, B.A.; Brody, A.; Luscombe, R.; Primiano, J.; Marusca, P.; Sitts, E.; Chyun, D. A Systematic Review of Cardiovascular Disease in Sexual Minorities. Am. J. Public Health 2017, 107, E13–E21. [Google Scholar] [PubMed]
- Corrigan, F.M.; Broome, H.; Dorris, L. A systematic review of psychosocial interventions for children and young people with epilepsy. Epilepsy Behav. 2016, 56, 99–112. [Google Scholar] [PubMed]
- Donnelly, N.; Hickey, A.; Burns, A.; Murphy, P.; Doyle, F. Systematic Review and Meta-Analysis of the Impact of Carer Stress on Subsequent Institutionalisation of Community-Dwelling Older People. PLoS ONE 2015, 10, e0128213. [Google Scholar]
- Feinstein, A.R.; Cicchetti, D.V. High agreement but low Kappa: I. the problems of two paradoxes. J. Clin. Epidemiol. 1990, 43, 543–549. [Google Scholar]
- Spitzer, R.L.; Fleiss, J.L. A re-analysis of the Reliability of Psychiatric Diagnosis. Br. J. Psychiatry 1974, 125, 341–347. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows. 23.0; IBM Corp.: Armonk, New York, NY, USA, 2015. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar]
- Adams, R.; Boscarino, J.; Figley, C. Compassion fatigue and psychological distress among social workers: A validation study. Am. J. Orthopsychiatry 2006, 76, 103–108. [Google Scholar]
- Jacobson, J.M. Compassion Fatigue, Compassion Satisfaction, and Burnout: Reactions among Employee Assistance Professionals Providing Workplace Crisis Intervention and Disaster Management Services. J. Workplace Behav. Health 2006, 21, 133–152. [Google Scholar]
- Boscarino, J.A.; Figley, C.R.; Adams, R.E. Compassion fatigue following the September 11 terrorist attacks: A study of secondary trauma among New York City social workers. Int. J. Emerg. Ment. Health 2004, 6, 57–66. [Google Scholar] [PubMed]
- Tosone, C.; Bettmann, J.E.; Minami, T.; Jasperson, R.A. New York City social workers after 9/11: Their attachment, resiliency, and compassion fatigue. Int. J. Emerg. Ment. Health 2010, 12, 103. [Google Scholar] [PubMed]
- Craig, C.D.; Sprang, G. Compassion satisfaction, compassion fatigue, and burnout in a national sample of trauma treatment therapists. Anxiety Stress Coping 2010, 23, 319–339. [Google Scholar] [CrossRef]
- Butler, L.; Carello, J.; Maguin, E. Trauma, Stress, and Self-Care in Clinical Training: Predictors of Burnout, Decline in Health Status, Secondary Traumatic Stress Symptoms, and Compassion Satisfaction. Psychol. Trauma Theory Res. Pract. Policy 2017, 9, 406. [Google Scholar] [CrossRef] [PubMed]
- Deighton, R.M.; Gurris, N.; Traue, H. Factors affecting burnout and compassion fatigue in psychotherapists treating torture survivors: Is the therapist’s attitude to working through trauma relevant? J. Trauma. Stress 2007, 20, 63. [Google Scholar] [CrossRef]
- Somoray, K.; Shakespeare-Finch, J.; Armstrong, D. The Impact of Personality and Workplace Belongingness on Mental Health Workers’ Professional Quality of Life. Aust. Psychol. 2017, 52, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Mangoulia, P.; Koukia, E.; Alevizopoulos, G.; Fildissis, G.; Katostaras, T. Prevalence of Secondary Traumatic Stress among Psychiatric Nurses in Greece. Arch. Psychiatr. Nurs. 2015, 29, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Hopkin, G.; Forrester, A. Exposure to Traumatic Events and the Experience of Burnout, Compassion Fatigue and Compassion Satisfaction among Prison Mental Health Staff: An Exploratory Survey. Issues Ment. Health Nurs. 2019, 40, 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetrano, G.; Tedeschi, F.; Rabbi, L.; Gosetti, G.; Lora, A.; Lamonaca, D.; Manthorpe, J.; Amaddeo, F. How are compassion fatigue, burnout, and compassion satisfaction affected by quality of working life? Findings from a survey of mental health staff in Italy. BMC Health Serv. Res. 2017, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Verhaeghe, S.; Duprez, V.; Beeckman, D.; Leys, J.; Van Meijel, B.; Van Hecke, A. Mental Health Nurses’ Attitudes and Perceived Self-Efficacy Toward Inpatient Aggression: A Cross-Sectional Study of Associations with Nurse-Related Characteristics. Perspect. Psychiatr. Care 2016, 52, 12–24. [Google Scholar]
- Itzhaki, M.; Bluvstein, I.; Peles Bortz, A.; Kostistky, H.; Bar Noy, D.; Filshtinsky, V.; Theilla, M. Mental Health Nurse’s Exposure to Workplace Violence Leads to Job Stress, Which Leads to Reduced Professional Quality of Life. Front. Psychiatry 2018, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linley, P.; Joseph, S. Therapy work and therapists’ positive and negative well-being. J. Soc. Clin. Psychol. 2007, 26, 385–403. [Google Scholar] [CrossRef]
- Ray, S.L.; Wong, C.; White, D.; Heaslip, K. Compassion Satisfaction, Compassion Fatigue, Work Life Conditions, and Burnout among Frontline Mental Health Care Professionals. Traumatology 2013, 19, 255–267. [Google Scholar] [CrossRef]
- Stamm, B.H. The Concise ProQOL Manual. Available online: https://proqol.org/uploads/ProQOLManual.pdf (accessed on 15 August 2020).
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Hakanen, J.J.; Demerouti, E.; Xanthopoulou, D. Job Resources Boost Work Engagement, Particularly when Job Demands Are High. J. Educ. Psychol. 2007, 99, 274. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Van Emmerik, H.; Van Riet, P. How job demands, resources, and burnout predict objective performance: A constructive replication. Anxiety Stress Coping 2008, 21, 309–324. [Google Scholar] [CrossRef]
- Crawford, E.R.; Lepine, J.A.; Rich, B.L. Linking job demands and resources to employee engagement and burnout: A theoretical extension and meta-analytic test. J. Appl. Psychol. 2010, 95, 834. [Google Scholar] [CrossRef]
- Lesener, T.; Gusy, B.; Wolter, C. The job demands-resources model: A meta-analytic review of longitudinal studies. Work Stress 2018, 33, 76–103. [Google Scholar] [CrossRef]
- Aarons, G.; Glisson, C.; Green, P.; Hoagwood, K.; Kelleher, K.; Landsverk, J. The organizational social context of mental health services and clinician attitudes toward evidence-based practice: A United States national study. Implement. Sci. 2012, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- Bennett, S.; Allen, S.; Caldwell, E.; Whitehead, M.; Turpin, M.; Fleming, J.; Cox, R. Organisational support for evidence-based practice: Occupational therapists perceptions. Aust. Occup. J. 2016, 63, 9–18. [Google Scholar] [CrossRef]
- Bride, B.E.; Robinson, M.M.; Yegidis, B.; Figley, C.R. Development and Validation of the Secondary Traumatic Stress Scale. Res. Soc. Work Pract. 2004, 14, 27–35. [Google Scholar]
- Bria, M.; Spânu, F.; Băban, A.; Dumitraşcu, D.L. Maslach Burnout Inventory—General Survey: Factorial validity and invariance among Romanian healthcare professionals. Burn. Res. 2014, 1, 103–111. [Google Scholar]
- Ployhart, R.E.; Vandenberg, R.J. Longitudinal research: The theory, design, and analysis of change. J. Manag. 2010, 36, 94–120. [Google Scholar]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Kelloway, E.K.; Francis, L. Longitudinal Research and Data Analysis; Routledge/Taylor & Francis Group: New York, NY, USA, 2013; pp. 374–394. [Google Scholar]
- De La Rosa, G.M.; Webb-Murphy, J.; Fesperman, S.F.; Johnston, S.L. Professional quality of life normative benchmarks. Psychol. Trauma Theory Res. Pract. Policy 2018, 10, 225–228. [Google Scholar]
- McCann, I.L.; Pearlman, L.A. Constructivist self-development theory: A theoretical framework for assessing and treating traumatized college students. J. Am. Coll. Health 1992, 40, 189–196. [Google Scholar]
- Pearlman, L.A.; Saakvitne, K.W. Trauma and the Therapist: Countertransference and Vicarious Traumatization in Psychotherapy with Incest Survivors; W W Norton & Co.: New York, NY, USA, 1995; p. xix, 451. [Google Scholar]
- MacRitchie, V.; Leibowitz, S. Secondary traumatic stress, level of exposure, empathy and social support in trauma workers. S. Afr. J. Psychol. 2010, 40, 149–158. [Google Scholar]
- Jovanović, N.; Podlesek, A.; Volpe, U.; Barrett, E.; Ferrari, S.; Rojnic Kuzman, M.; Wuyts, P.; Papp, S.; Nawka, A.; Vaida, A.; et al. Burnout syndrome among psychiatric trainees in 22 countries: Risk increased by long working hours, lack of supervision, and psychiatry not being first career choice. Eur. Psychiatry 2016, 32, 34–41. [Google Scholar]
- Hamaideh, S.H. Burnout, social support, and job satisfaction among Jordanian mental health nurses. Issues Ment. Health Nurs. 2011, 32, 234–242. [Google Scholar]
- Kumar, S.; Hatcher, S.; Dutu, G.; Fischer, J.; Ma’U, E. Stresses Experienced by Psychiatrists and Their Role in Burnout: A National Follow-Up Study. Int. J. Soc. Psychiatry 2011, 57, 166–179. [Google Scholar]
- Lasalvia, A.; Bonetto, C.; Bertani, M.; Bissoli, S.; Cristofalo, D.; Marrella, G.; Ceccato, E.; Cremonese, C.; De Rossi, M.; Lazzarotto, L.; et al. Influence of perceived organisational factors on job burnout: Survey of community mental health staff. Br. J. Psychiatry J. Ment. Sci. 2009, 195, 537. [Google Scholar]
- Peter, R.; Sorgaard Knut, W.; Ian, D. Qualified and Unqualified (N-R C) mental health nursing staff - minor differences in sources of stress and burnout. A European multi-centre study. BMC Health Serv. Res. 2010, 10, 163. [Google Scholar]
- Nelson, T.; Johnson, S.; Bebbington, P. Satisfaction and burnout among staff of crisis resolution, assertive outreach and community mental health teams. Soc. Psychiat. Epidemiol. 2009, 44, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Finzi-Dottan, R.; Kormosh, M.B. Social Workers in Israel: Compassion, Fatigue, and Spillover into Married Life. J. Soc. Serv. Res. 2016, 42, 703–717. [Google Scholar] [CrossRef]
- Olashore, A.A.; Akanni, O.O.; Molebatsi, K.; Ogunjumo, J.A. Post-traumatic stress disorder among the staff of a mental health hospital: Prevalence and risk factors. South Afr. J. Psychiatry 2018, 24, 1222. [Google Scholar] [CrossRef]
- Rodrigues, N.C.; Ham, E.; Hilton, N.Z.; Seto, M.C. Workplace characteristics of forensic and nonforensic psychiatric units associated with posttraumatic stress disorder (PTSD) symptoms. Psychol. Serv. 2020. [Google Scholar] [CrossRef]
- Hilton, N.Z.; Ham, E.; Rodrigues, N.C.; Kirsh, B.; Chapovalov, O.; Seto, M.C. Contribution of Critical Events and Chronic Stressors to PTSD Symptoms Among Psychiatric Workers. PS 2020, 71, 221–227. [Google Scholar] [CrossRef]
- Weathers, F.W.; Huska, J.A.; Keane, T.M. PCL-C for DSM-IV. 1991. Available online: http://library.niwap.org/wp-content/uploads/2015/PTSDChecklist.pdf (accessed on 16 August 2020).
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5\Textregistered); American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Ben-Zur, H.; Michael, K. Burnout, Social Support, and Coping at Work among Social Workers, Psychologists, and Nurses: The Role of Challenge/Control Appraisals. Soc. Work Health Care 2007, 45, 63–82. [Google Scholar] [CrossRef]
- Mccormack, H.M.; Macintyre, T.E.; O’Shea, D.; Campbell, M.J.; Igou, E.R. Practicing What We Preach: Investigating the Role of Social Support in Sport Psychologists’ Well-Being. Front. Psychol. 2015, 6, 1854. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.; Araya, R.; Wearn, E.; Moli, P.; Stafford, M.; Wellman, N.; Nolan, F.; Lloyd-Evans, B.; Anderson, E.; Wood, S. Morale in the English mental health workforce: Questionnaire survey. Br. J. Psychiatry 2012, 201, 239–246. [Google Scholar] [CrossRef]
- Hensel, J.M.; Ruiz, C.; Finney, C.; Dewa, C.S. Meta-analysis of risk factors for secondary traumatic stress in therapeutic work with trauma victims. J. Trauma. Stress 2015, 28, 83. [Google Scholar] [CrossRef] [PubMed]
- Sprang, G.; Craig, C.; Clark, J. Secondary Traumatic Stress and Burnout in Child Welfare Workers: A Comparative Analysis of Occupational Distress Across Professional Groups. Child Welf. 2011, 90, 149–168. [Google Scholar]
- Cohen, M.; Gagin, R.; Peled-Avram, M. Multiple terrorist attacks: Compassion fatigue in Israeli social workers. Traumatology 2006, 12, 293–301. [Google Scholar] [CrossRef]
- Nelson-Gardell, D.; Harris, D. Childhood abuse history, secondary traumatic stress, and child welfare workers. Child Welf. 2003, 82, 5–26. [Google Scholar]
- Thomas, J.T.; Otis, M.D. Intrapsychic Correlates of Professional Quality of Life: Mindfulness, Empathy, and Emotional Separation. J. Soc. Soc. Work Res. 2010, 1, 83–98. [Google Scholar] [CrossRef]
- Udipi, S.; Veach, P.; Kao, J.; LeRoy, B. The Psychic Costs of Empathic Engagement: Personal and Demographic Predictors of Genetic Counselor Compassion Fatigue. J. Genet. Couns. 2008, 17, 459–471. [Google Scholar] [CrossRef]
- Potter, P.; Deshields, T.; Divanbeigi, J.; Berger, J.; Cipriano, D.; Norris, L.; Olsen, S. Compassion Fatigue and Burnout: Prevalence among Oncology Nurses. Clin. J. Oncol. Nurs. 2010, 14, 56. [Google Scholar] [CrossRef]
- Quinn, A.; Ji, P.; Nackerud, L. Predictors of secondary traumatic stress among social workers: Supervision, income, and caseload size. J. Soc. Work 2019, 19, 504–528. [Google Scholar] [CrossRef]
- D’Oria, L. The SAGE Encyclopedia of Industrial and Organizational Psychology, 2nd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2020; pp. 1371–1372. [Google Scholar]
- Joseph, S.; Linley, A.P. Positive Adjustment to Threatening Events: An Organismic Valuing Theory of Growth through Adversity. Rev. Gen. Psychol. 2005, 9, 262–280. [Google Scholar] [CrossRef]
- Sidani, S.; Sechrest, L. Putting Program Theory into Operation. Am. J. Eval. 1999, 20, 227–238. [Google Scholar]
- Vanderplasschen, W.; De Maeyer, J. Theory-Driven Interventions; Encyclopedia of Quality of Life and Well-being Research; Michalos, A.C., Ed.; Springer: The Netherlands, 2014; pp. 6629–6632. Available online: https://0-www-springer-com.brum.beds.ac.uk/gp/book/9789400707528 (accessed on 18 August 2020).
- Broekaert, E.; Autrique, M.; Vanderplasschen, W.; Colpaert, K. ‘The Human Prerogative’: A Critical Analysis of Evidence-Based and Other Paradigms of Care in Substance Abuse Treatment. Psychiatr. Q. 2010, 81, 227–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corley, K.G.; Gioia, D.A. Building Theory about Theory Building: What Constitutes a Theoretical Contribution? Acad. Manag. Rev. 2011, 36, 12–32. [Google Scholar] [CrossRef] [Green Version]
- Neuman, W.L. Social Research Methods; Pearson: Boston, MA, USA, 2014; pp. 1–640. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- British Psychological Society BPS Practice Guidelines, 3rd ed.; British Psychological Society: Leicester, UK, 2017; pp. 1–89.
- Health and Safety Executive. The Health and Safety Executive Annual Report and Accounts 2018/2019; UK Parliam. House Commons Pap.; 2019; pp. 1–120. Available online: https://www.hse.gov.uk/aboutus/reports/ara-2018-19.pdf (accessed on 18 August 2020).
- Taris, T.W.; Kompier, M.A.J. Cause and effect: Optimizing the designs of longitudinal studies in occupational health psychology. Work Stress 2014, 28, 1–8. [Google Scholar] [CrossRef]
- Houdmont, J.; Jachens, L.; Randall, R.; Hopson, S.; Nuttall, S.; Pamia, S. What Does a Single-Item Measure of Job Stressfulness Assess? Int. J. Environ. Res. Public Health 2019, 16, 1480. [Google Scholar] [CrossRef] [Green Version]
- Fisher, G.G.; Matthews, R.A.; Gibbons, A.M. Developing and investigating the use of single-item measures in organizational research. J. Occup. Health Psychol. 2016, 21, 3–23. [Google Scholar] [CrossRef]
- Elo, A.-L.; Leppänen, A. Antti Jahkola Validity of a single-item Measure of Stress Symptoms. Scand. J. Work Environ. Health 2003, 29, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Littman, A.J.; White, E.; Satia, J.A.; Bowen, D.J.; Kristal, A.R. Reliability and Validity of 2 Single-Item Measures of Psychosocial Stress. Epidemiology 2006, 17, 398–403. [Google Scholar] [CrossRef]
- Hoeppner, B.B.; Kelly, J.F.; Urbanoski, K.A.; Slaymaker, V. Comparative utility of a single-item versus multiple-item measure of self-efficacy in predicting relapse among young adults. J. Subst. Abus. Treat. 2011, 41, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Loo, R. A caveat on using single-item versus multiple-item scales. J. Manag. Psychol. 2002, 17, 68–75. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Population | Sample | Aim(s) | Measure | Theoretical Framework | Results | CCAT Score |
|---|---|---|---|---|---|---|---|---|
| Adams et al. [76] | USA | New-York based members of the National Association of Social Workers (NASW) | n = 236 Males = 20.5% Females = 79.5% | To determine the psychometric properties of the CF (CF) Scale-Revised | CF (CF) Scale-Revised | Stress-Process Framework | Information to work effectively and sense of mastery were negatively associated with BO and STS. | 65% |
| Jacobson [77] | USA | Members of Employee Assistance Professional Association (EAPA) | n = 325 Mean Age = 50.06 (8.67) Males = 44.0% Females = 55.7% Involved in clinical work = 47.7% Involved in administrative work = 23.7% Number of clinical hours per week = 21.67 (14.35) Number of EAP sessions = 4.8 (2.96) | To explore the prevalence and predictors of CF, BO and compassion satisfaction in a sample of employee assistance professionals. | ProQOL | Constructivist Self-Development Theory | Work-related stress due to engagement with traumatised clients was positively associated with CF and BO. Services offered by employee assistance professionals to cope with work-related stress was associated with BO. | 65% |
| Boscarino et al. [78] | USA | New-York based members of the National Association of Social Workers (NASW) | n = 236 Males = 20.5% Females = 79.5% | To assess the prevalence of CF among social workers who cared for victims of the September 11 attack in New York City. | CF Scale-Revised | NR | World Trade Centre Recovery Involvement was positively associated with STS. Work Environment Support was negatively associated with STS and BO. | 70% |
| Tosone et al. [79] | USA | Manhattan-based members of the National Association of Social Work (NASW) | n = 481 Mean Age = 59.83 (9.3) Males = 19.5% Females = 79.6% Length of service = 26.35 (9.77) Psychoanalytic = 61.3% Integrative/Eclectic = 23.7% Cognitive-Behavioural = 6.2% Family Systems = 2.9% General Systems = 2.3% | To explore the relationships among attachment style, resilience and CF. | ProQOL-IV | NR | Percentage of clients experiencing trauma predicted CF. | 68% |
| Craig & Sprang [80] | USA | Clinical psychologists and clinical social workers | n = 532 Clinical Psychology = 225 Clinical Social Work = 235 Mean Age = 53.2 Males = 34% Females = 65% | To examine the association between the use of evidence-based practices and CF, BO and compassion satisfaction. | ProQOL-III | ProQOL Framework | Utilisation of evidence-based practices reduced CF and BO. | 88% |
| Butler et al. [81] | USA | Students in the graduate social work training programme at the University of Buffalo | n = 195 Males = 11.8% Females = 87.7% Mental health or substance abuse = 31.1% School social work = 20.4% Child welfare = 19.9% Organisations/Community = 12.2% Healthcare = 9.2% Trauma programme/Domestic violence = 8.2% Crisis intervention = 5.1% Residential treatment = 3.1% | To examine trauma-related exposures in graduate training and to investigate whether training-related risk and protective factors predict BO, decline in health status, STS and compassion satisfaction. | ProQOL 5 | NR | Training retraumatisation, high field stress and decreased self-care effort were predictors of BO and STS. | 83% |
| Deighton et al. [82] | Germany, Austria and Switzerland | German speaking trauma therapists based | n = 100 Males = 34% Females = 65% Clinical Psychology = 35% Other branches of Psychology = 13% Psychiatry = 10% Other clinical professionals = 9% Social workers = 18% Physiotherapy = 6% Art Therapy = 7% Child Therapy = 1% Psychoanalysis/Psychodynamic therapy = 15% Systemic Family Therapy = 12% Cognitive-Behaviour Therapy = 11% Client-Oriented Therapy = 9% Creative Therapies = 9% Gestalt Therapy = 8% Integrative therapy = 5% EMDR = 3% Psychodrama = 2% Other therapies = 8% Number of colleagues = 5.9 (3.5) Weekly working hours = 24.7 (11.2) Weekly caseload = 10.4 (5.4) Length of service with traumatised clients = 7.7 (5.5) | To explore the nature of relationship between trauma therapists’ advocacy and use of working through and work-related outcomes. | ProQOL-III | NR | The degree of working through was negatively associated with BO. The advocacy of working through was positively was positively associated with CF. The participants who advocated working through but did not practice it experienced higher levels of CF than those who advocated as well as practiced it. | 53% |
| Somoray et al. [83] | Australia | Mental health workers working in an NGO providing counselling services | n = 156 Mean Age = 44.60 (12.42) Males = 17.9% Females = 79.5% | To investigate the role of personality traits and workplace belongingness in predicting the ProQOL. | ProQOL 5 | Five Factor Model of Personality | Workplace belongingness was positively associated with BO. | 70% |
| Mangoulia et al. [84] | Greece | Registered and assistant psychiatric nurses in 12 public hospitals | n = 174 Registered nurses = 51.2% Assistant nurses = 48.8% Mean Age = 36.87 (7.37) Males = 29.9% Females = 70.1% Length of service in psychiatric unit = 6.71 (6.65) | To investigate the prevalence of CF, BO and compassion satisfaction and examine the personal and work-related factors associated with them. | ProQOL-IV | NR | Participants who considered their working environment as very good and that the staff always worked as a team reported lower levels of BO. Nurses who worked fewer weekends per month had 1.2 to 2.6 times higher levels of CF. | 88% |
| Bell et al. [85] | UK | Mental health nurses and correctional officers employed at a prison in London | n = 36 Mental health nurses = 21 Correctional officers = 15 Mean Age = 40.31 (1.57) Males = 58.3% Females = 41.7% | To determine the levels of CF, BO and compassion satisfaction; and, to explore the relationship between risk and protective factors and ProQOL. | ProQOL 5 | NR | Low CF was associated with support and consultation from line managers, emotional support from colleagues and perceived level of skills. Low BO was associated with supervision and emotional support from colleagues. | 75% |
| Cetrano et al. [86] | Italy | Mental health professionals based in three mental health institutions | n = 400 Males = 24.1% Females = 75.9% Psychiatry/Training = 19.9% Psychiatric Nursing = 30.5% Psychology = 6.8% Education/Social Work = 16.4% Rehabilitation Therapy = 5.5% Support Work = 20.9% | To examine the predictive association of quality of working life and ProQOL. | ProQOL -III | ProQOL Framework | Ergonomic problems and impact of work on life were associated with CF and BO. Impact of life on work was associated with CF. Trust and perceived risks for future were associated with BO. | 80% |
| Verhaeghe et al. [87] | Belgium | Nursing staff employed at 17 wards in psychiatric hospital | n = 219 Mean Age = 41.23 (11.43) Males = 23.7% Females = 72.6% | To explore the associations between attitudes and perceived self-efficacy toward aggression and nurse-related characteristics. | ProQOL 5 | Theory of Planned Behaviour (Fishbein and Ajzen, 2010) Bandura’s theory of self-efficacy (Bandura, 1991) | STS was negatively correlated with staff confidence. BO was negatively correlated with prediction and staff anxiety and fear of assault. | 78% |
| Itzhaki et al. [88] | Israel | Nurses working at a mental health centre | n = 177 Males = 11.86% Females = 87.01% | To explore the relationships among workplace violence, job stress and ProQOL (ProQOL). | ProQOL 5 | ProQOL Framework | Work stress was positively associated with BO. | 70% |
| Linley & Joseph [89] | UK | Psychotherapists | n = 156 Mean Age = 53.67 (10.90) Males = 21.79% Females = 78.21% Weekly caseload = 12.64 (6.60) | To examine the impact of organisational level factors and psychological level factors on the positive and negative well-being of psychotherapists. | ProQOL | NR | Therapists who had either received or were receiving personal therapy reported less BO. Therapists with cognitive-behavioural and existential therapeutic orientation were more likely to experience BO. | 55% |
| Ray et al. [90] | Canada | Frontline mental health professionals (FMHPs) in South-western Ontario | n = 169 Mean Age = 43.8 (11.61) Males = 18.3% Females = 81.7% Length of service in the profession = 17.23 (11.45) Length of service in mental health = 13.98 (9.86) Length of service in current setting = 6.67 (7.02) Caseload = 14.30 (16.10) Nursing = 40.8% Allied Healthcare = 17.2% Case Management = 17.8% Mental Health = 24.3% | To explore relationships among compassion satisfactions, CF, work-life conditions and BO. | ProQOL-IV-R | ProQOL Framework and Compassion Stress/Fatigue Model | CF was negatively correlated with workload, control, reward, community and fairness. | 68% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, J.; Karanika-Murray, M.; Baguley, T.; Hudson, J. A Systematic Review of Job Demands and Resources Associated with Compassion Fatigue in Mental Health Professionals. Int. J. Environ. Res. Public Health 2020, 17, 6987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17196987
Singh J, Karanika-Murray M, Baguley T, Hudson J. A Systematic Review of Job Demands and Resources Associated with Compassion Fatigue in Mental Health Professionals. International Journal of Environmental Research and Public Health. 2020; 17(19):6987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17196987
Chicago/Turabian StyleSingh, Jasmeet, Maria Karanika-Murray, Thom Baguley, and John Hudson. 2020. "A Systematic Review of Job Demands and Resources Associated with Compassion Fatigue in Mental Health Professionals" International Journal of Environmental Research and Public Health 17, no. 19: 6987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17196987