Improvement of Dietary Diversity and Attitude toward Recommended Feeding through Novel Community Based Nutritional Education Program in Coastal Kenya—An Intervention Study


Abstract
:1. Introduction
2. Materials and Methods
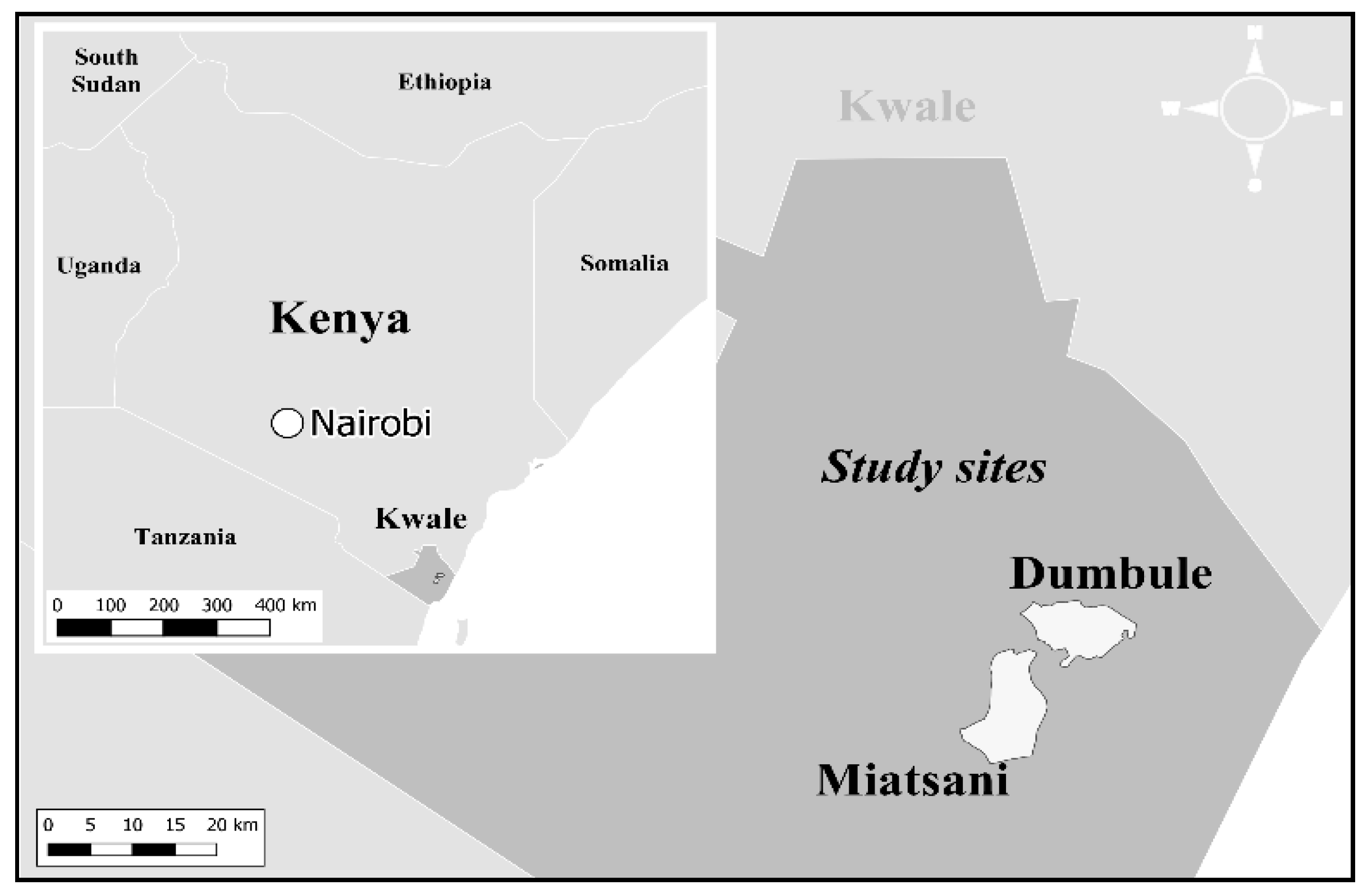
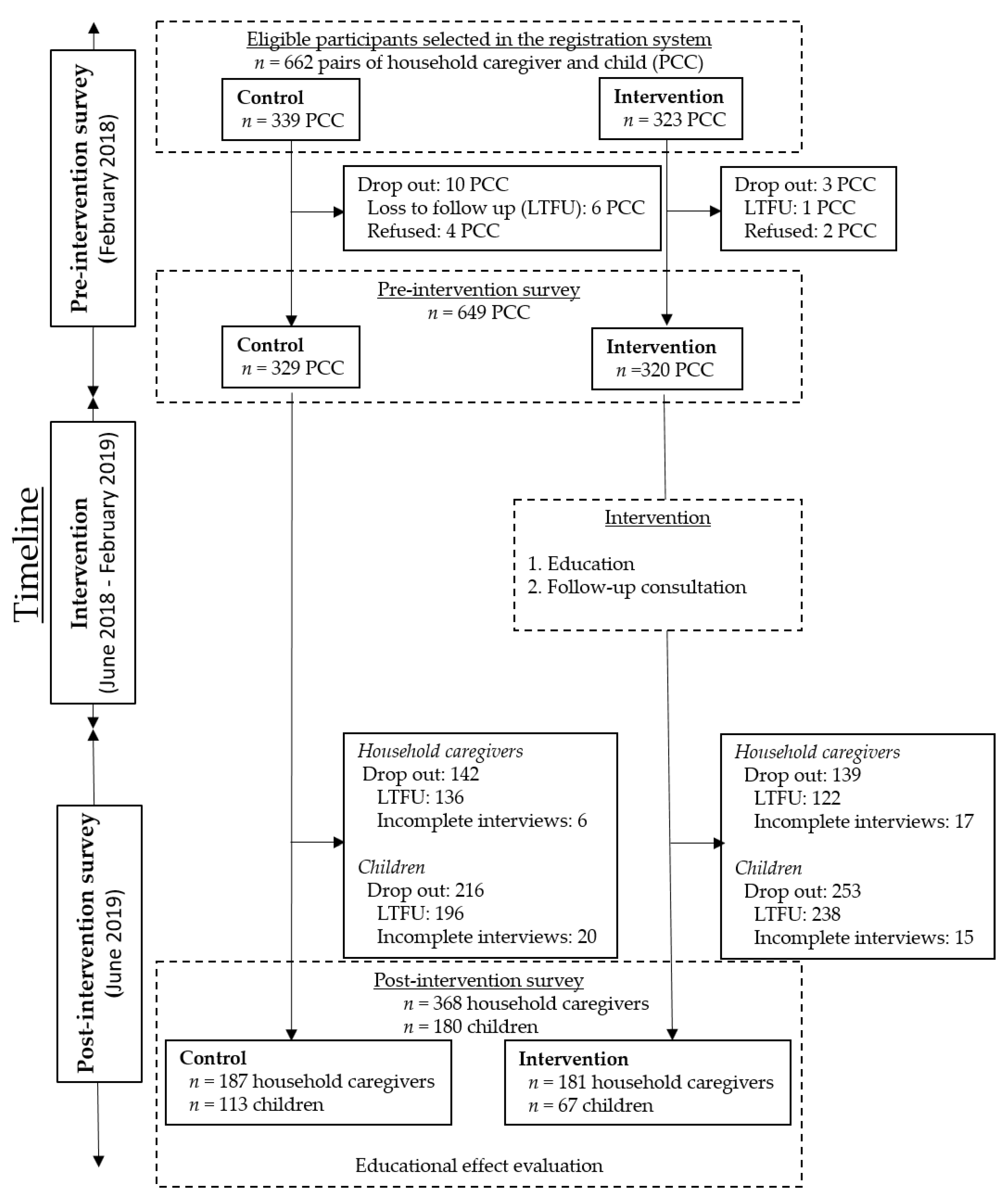
2.1. Pre-Intervention
2.2. Intervention
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Consideration
3. Results
3.1. Participants Characteristics
3.2. Educational Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNICEF. The faces of malnutrition. Available online: https://www.unicef.org/nutrition/index_faces-of-malnutrition.html (accessed on 5 June 2020).
- UNICEF. UNICEF’S APPROACH TO SCALING UP NUTRITION. Available online: https://www.unicef.org/nutrition/files/Unicef_Nutrition_Strategy.pdf (accessed on 25 June 2019).
- World Health Organization. Global Nutrition Targets 2025: Policy brief series. Available online: https://apps.who.int/iris/bitstream/handle/10665/149018/WHO_NMH_NHD_14.2_eng.pdf?ua=1 (accessed on 30 June 2020).
- UNICEF. UNICEF/WHO/World Bank joint child malnutrition estimates regional classifications. Available online: https://data.unicef.org/topic/nutrition/malnutrition/ (accessed on 26 June 2019).
- Ickes, S.B.; Baguma, C.; Brahe, C.A.; Myhre, J.A.; Adair, L.S.; Bentley, M.E.; Ammerman, A.S. Maternal participation in a nutrition education program in Uganda is associated with improved infant and young child feeding practices and feeding knowledge: A post-program comparison study. BMC Nutr. 2017, 3, 427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rah, J.H.; Akhter, N.; Semba, R.D.; De Pee, S.; Bloem, M.W.; Campbell, A.A.; Moench-Pfanner, R.; Sun, K.; Badham, J.; Kraemer, K. Low dietary diversity is a predictor of child stunting in rural Bangladesh. Eur. J. Clin. Nutr. 2010, 64, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
- Darapheak, C.; Takano, T.; Kizuki, M.; Nakamura, K.; Seino, K. Consumption of animal source foods and dietary diversity reduce stunting in children in Cambodia. Int. Arch. Med. 2013, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Hatløy, A.; Torheim, L.E.; Oshaug, A. Food variety—A good indicator of nutritional adequacy of the diet? A case study from an urban area in Mali, West Africa. Eur. J. Clin. Nutr. 1998, 52, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.E.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Kenya National Bureau of Statistics; Ministry of Health/Kenya; National AIDS Control Council/Kenya; Kenya Medical Research Institute; National Council for Population and Development/Kenya. Kenya Demographic and Health Survey 2014; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Tanaka, J.; Yoshizawa, K.; Hirayama, K.; Karama, M.; Wanjihia, V.; Changoma, M.; Kaneko, S. Relationship between dietary patterns and stunting in preschool children: A cohort analysis from Kwale, Kenya. Public Health 2019, 173, 58–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNICEF. Children, Food and Nutrition: Growing Well in a Changing World. Available online: https://www.unicef.org/media/60806/file/SOWC-2019.pdf (accessed on 29 September 2020).
- Matsuyama, A.; Karama, M.; Tanaka, J.; Kaneko, S. Perceptions of caregivers about health and nutritional problems and feeding practices of infants: A qualitative study on exclusive breast-feeding in Kwale, Kenya. BMC Public Heal. 2013, 13, 525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallas, S.W.; Minhas, D.; Pérez-Escamilla, R.; Taylor, L.; Curry, L.; Bradley, E.H. Community health workers in low- and middle-income countries: What do we know about scaling up and sustainability? Am. J. Public Health 2013, 103, e74–e82. [Google Scholar] [CrossRef] [PubMed]
- Kioko, E.M. Conflict Resolution and Crime Surveillance in Kenya: Local Peace Committees and Nyumba Kumi. Afr. Spectr. 2017, 52, 3–32. [Google Scholar] [CrossRef] [Green Version]
- Leting, M. Nyumba Kumi Strategy of Community Policing And Its Impact on Curbing Crime; Empirical Assessment From Kenya. IOSR J. Humanit. Soc. Sci. 2017, 22, 32–36. [Google Scholar] [CrossRef]
- Kaneko, S.; K’Opiyo, J.; Kiche, I.; Wanyua, S.; Goto, K.; Tanaka, J.; Changoma, M.; Ndemwa, M.; Komazawa, O.; Karama, M.; et al. Health and Demographic Surveillance System in the Western and Coastal Areas of Kenya: An Infrastructure for Epidemiologic Studies in Africa. J. Epidemiology 2012, 22, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices, Part I: Definition; WHO Press: Geneva, Switzerland, 2008. [Google Scholar]
- Kenya National Bureau of Statistics. 2019 Kenya Population and Housing Census: Volume I: POPULATION BY County and Sub-County; Kenya National Bureau of Statistics: Nairobi, Kenya, 2019. [Google Scholar]
- Kennedy, G.; Ballard, T.; Dop, M.C. Guidelines for Measuring Household and Individual Dietary Diversity; Food and Agricultural Organization of the United Nations: Rome, Italy, 2011; Volume 2020. [Google Scholar]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO Press: Geneva, Switzerland, 2006. [Google Scholar]
- Shi, L.; Zhang, J. Recent Evidence of the Effectiveness of Educational Interventions for Improving Complementary Feeding Practices in Developing Countries. J. Trop. Pediatr. 2010, 57, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hitachi, M.; Honda, S.; Kaneko, S.; Kamiya, Y. Correlates of exclusive breastfeeding practices in rural and urban Niger: A community-based cross-sectional study. Int. Breastfeed. J. 2019, 14, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Kenya. Kenya Report 167 New Cases of COVID-19 Nairobi, Sunday, June 7, 2020. Available online: https://www.health.go.ke/kenya-report-167-new-cases-of-covid-19-nairobi-sunday-june-7-2020 (accessed on 10 July 2020).
- Roba, K.T.; O’Connor, T.P.; Belachew, T.; O’Brien, N.M. Variations between post- and pre-harvest seasons in stunting, wasting, and Infant and Young Child Feeding (IYCF) practices among children 6–23 months of age in lowland and midland agro-ecological zones of rural Ethiopia. Pan Afr. Med. J. 2016, 24, 163. [Google Scholar] [CrossRef] [PubMed]
- Abizari, A.-R.; Azupogo, F.; Nagasu, M.; Creemers, N.; Brouwer, I.D. Seasonality affects dietary diversity of school-age children in northern Ghana. PLoS ONE 2017, 12, e0183206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, V.; Tefft, J.F.; Kelly, V.A.; Staatz, J.M. Knowledge, Attitudes and Practices on Child Feeding and Care: Preliminary Insights from the Project on Linkages between Child Nutrition and Agricultural Growth. Food Security International Development Policy Syntheses; Michigan State University, Department of Agricultural, Food, and Resource Economics: East Lansing, MI, USA, 2002; pp. 1–8. [Google Scholar] [CrossRef]
- Marquis, G.S.; Colecraft, E.K.; Sakyi-Dawson, O.; Lartey, A.; Ahunu, B.K.; Birks, K.A.; Butler, L.M.; Reddy, M.B.; Jensen, H.H.; Huff-Lonergan, E. An Integrated Microcredit, Entrepreneurial Training, and Nutrition Education Intervention Is Associated with Better Growth Among Preschool-Aged Children in Rural Ghana. J. Nutr. 2014, 145, 335–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penny, M.E.; Creed-Kanashiro, H.M.; Robert, R.C.; Narro, M.R.; Caulfield, L.E.; Black, R.E. Effectiveness of an educational intervention delivered through the health services to improve nutrition in young children: A cluster-randomised controlled trial. Lancet 2005, 365, 1863–1872. [Google Scholar] [CrossRef]
- Amugsi, D.A.; Dimbuene, Z.T.; Kimani-Murage, E.W.; Mberu, B.; Ezeh, A.C. Differential effects of dietary diversity and maternal characteristics on linear growth of children aged 6–59 months in sub-Saharan Africa: A multi-country analysis. Public Heal. Nutr. 2017, 20, 1029–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Control | (%) | Intervention | (%) | p-Value |
|---|---|---|---|---|---|
| Household | n = 187 | n = 181 | |||
| Household population | 0.09 | ||||
| <5 members | 34 | (18.2) | 46 | (25.4) | |
| ≥5 members | 153 | (81.8) | 135 | (74.6) | |
| Socioeconomic status | 0.43 | ||||
| Lower | 105 | (56.2) | 109 | (60.2) | |
| Higher | 82 | (43.8) | 72 | (39.8) | |
| Religion | 0.40 | ||||
| Islam | 162 | (86.6) | 162 | (89.5) | |
| Other | 25 | (13.4) | 19 | (10.5) | |
| Place of delivery | 0.66 | ||||
| Home | 60 | (32.1) | 62 | (34.3) | |
| Facility | 127 | (67.9) | 119 | (65.8) | |
| Child | n = 113 | n = 67 | |||
| Sex | 0.72 | ||||
| Male | 55 | (48.7) | 35 | (51.5) | |
| Female | 58 | (51.3) | 33 | (48.5) | |
| Age | 0.18 | ||||
| Mean age a (month) | 26.41 ± 9.98 | 24.46 ± 11.30 | |||
| Variable | Control | Intervention | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre- | Post- | Δ a | p-Value b | Pre- | Post- | Δ a | p-Value b | |
| Household | n = 187 | n = 181 | ||||||
| DDS c | 4.18 ± 1.81 | 6.15 ± 1.36 | 1.97 ± 0.45 | <0.01 | 4.97 ± 1.95 | 6.91 ± 1.42 | 1.94 ± 0.53 | <0.01 |
| Attitude score | 7.86 ± 1.25 | 8.32 ± 1.10 | 0.46 ± 0.15 | <0.01 | 8.15 ± 1.09 | 8.64 ± 0.68 | 0.49 ± 0.41 | <0.01 |
| Child | n = 113 | n = 67 | ||||||
| HAZ | −1.56 ± 1.25 | −1.55 ± 0.89 | 0.01 ± 0.36 | 0.06 | −1.30 ± 1.62 | −1.51 ± 1.16 | 0.21 ± 0.46 | 0.79 |
| WAZ | −1.14 ± 1.10 | −1.04 ± 0.81 | 0.10 ± 0.29 | 0.36 | −0.89 ± 1.13 | −0.97 ± 0.88 | 0.08 ± 0.25 | 0.36 |
| WHZ | −0.44 ± 1.18 | −0.22 ± 0.94 | 0.22 ± 0.24 | 0.22 | −0.24 ± 1.26 | −0.16 ± 1.20 | 0.08 ± 0.06 | 0.66 |
| Variable | DDS b (n = 368) | Attitude Score (n = 368) | HAZ c (n = 180) | WAZ d (n = 180) | WHZ e (n = 180) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |||||||||||
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| Group | ||||||||||||||||||||
| Control (reference) | ||||||||||||||||||||
| Intervention | −0.04 | 0.86 | 0.54 | <0.01 | 0.02 | 0.89 | 0.29 | <0.01 | −0.22 | 0.24 | −0.04 | 0.79 | −0.19 | 0.11 | −0.08 | 0.38 | −0.14 | 0.46 | −0.05 | 0.72 |
| Adjusted variable Pre-intervention score of outcome | ||||||||||||||||||||
| −0.8 | <0.01 | −0.79 | <0.01 | −0.89 | <0.01 | −0.90 | <0.01 | −0.65 | <0.01 | −0.62 | <0.01 | −0.46 | <0.01 | −0.46 | <0.01 | −0.62 | <0.01 | −0.61 | <0.01 | |
| Household population | ||||||||||||||||||||
| <5 members (reference) | ||||||||||||||||||||
| ≥5 members | −0.81 | <0.01 | −0.46 | <0.01 | 0.03 | 0.85 | −0.02 | 0.86 | 0.2 | 0.37 | 0.04 | 0.79 | 0.09 | 0.53 | −0.03 | 0.8 | −0.14 | 0.47 | −0.05 | 0.76 |
| Child mean age (month) | −0.05 | <0.01 | −0.02 | <0.01 | −0.00 | 0.69 | −0.00 | 0.25 | 0.04 | <0.01 | 0.01 | 0.04 | 0.01 | 0.21 | −0.00 | 0.30 | −0.02 | 0.04 | −0.02 | 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hitachi, M.; Wanjihia, V.; Nyandieka, L.; Francesca, C.; Wekesa, N.; Changoma, J.; Muniu, E.; Ndemwa, P.; Honda, S.; Hirayama, K.; et al. Improvement of Dietary Diversity and Attitude toward Recommended Feeding through Novel Community Based Nutritional Education Program in Coastal Kenya—An Intervention Study. Int. J. Environ. Res. Public Health 2020, 17, 7269. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197269
Hitachi M, Wanjihia V, Nyandieka L, Francesca C, Wekesa N, Changoma J, Muniu E, Ndemwa P, Honda S, Hirayama K, et al. Improvement of Dietary Diversity and Attitude toward Recommended Feeding through Novel Community Based Nutritional Education Program in Coastal Kenya—An Intervention Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7269. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197269
Chicago/Turabian StyleHitachi, Mami, Violet Wanjihia, Lilian Nyandieka, Chepkirui Francesca, Norah Wekesa, Juma Changoma, Erastus Muniu, Phillip Ndemwa, Sumihisa Honda, Kenji Hirayama, and et al. 2020. "Improvement of Dietary Diversity and Attitude toward Recommended Feeding through Novel Community Based Nutritional Education Program in Coastal Kenya—An Intervention Study" International Journal of Environmental Research and Public Health 17, no. 19: 7269. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197269