Risk Management in the New Frontier of Professional Liability for Nosocomial Infection: Review of the Literature on Mycobacterium Chimaera



Abstract
:1. Introduction
2. Materials and Methods
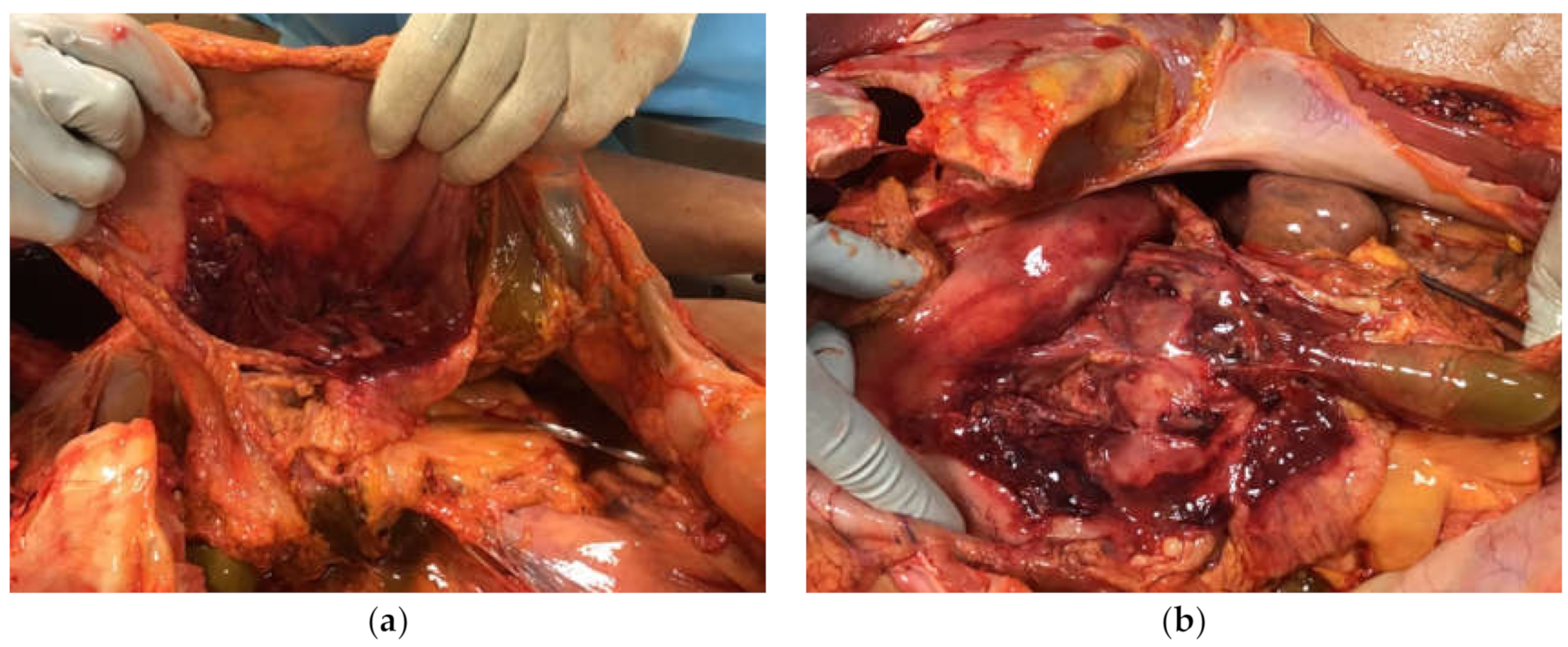
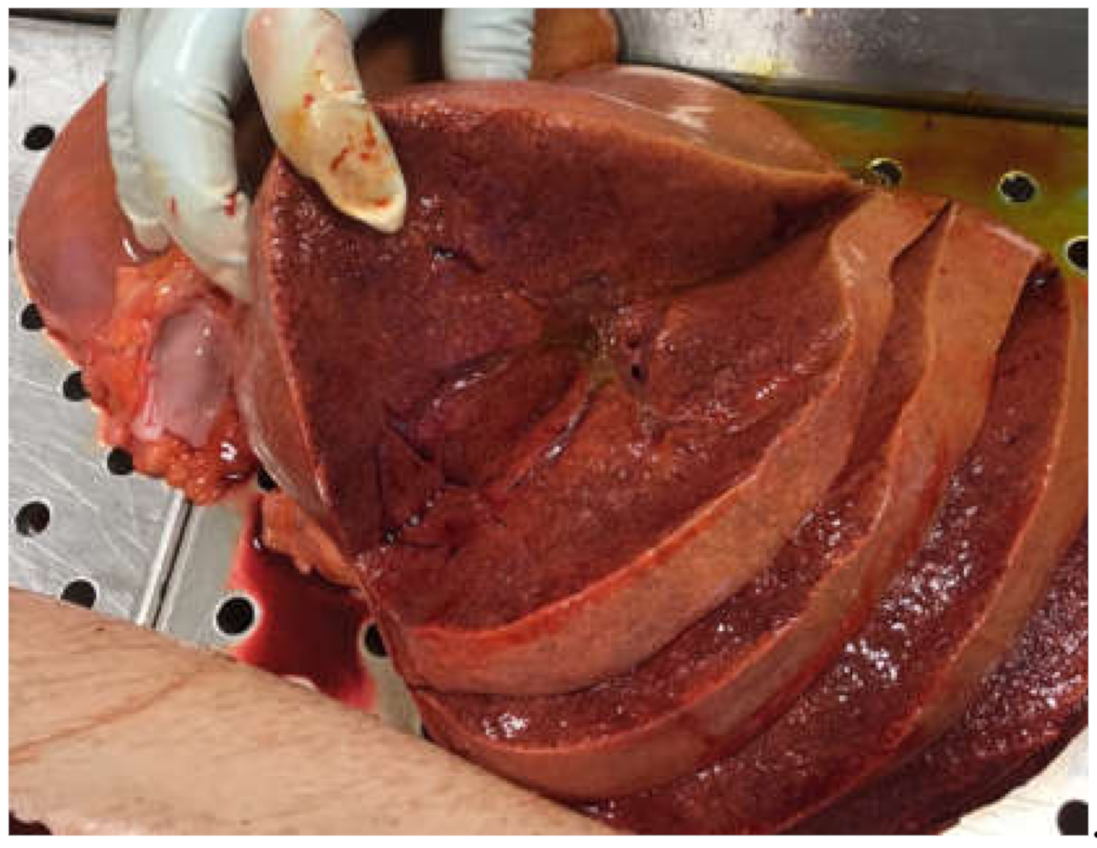
2.1. Case Report
2.2. Official Recommendation Documents
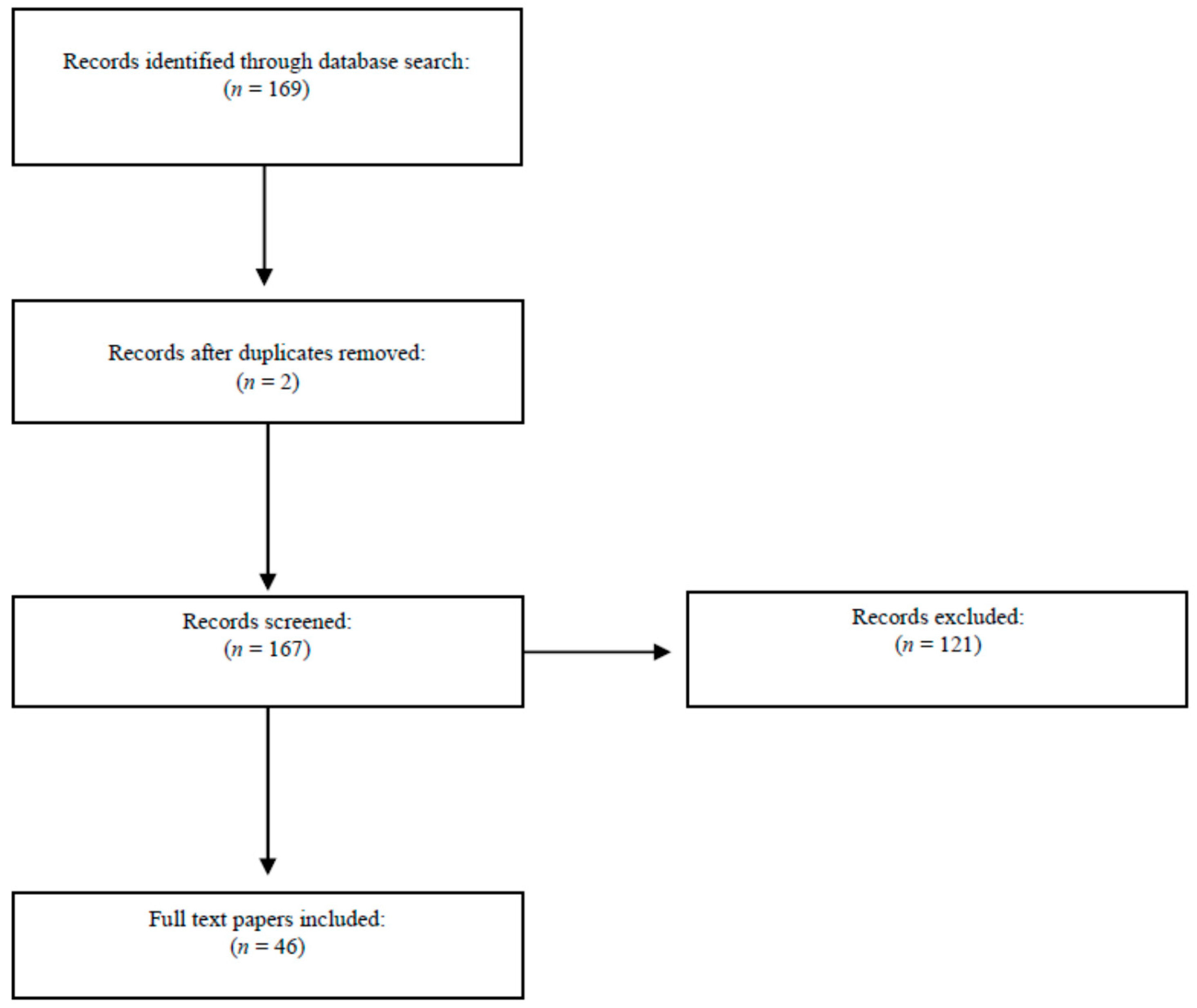
2.3. Literature Review
3. Results
3.1. Case Report
3.2. Review of Official Recommendation Documents
- (a)
- HCU devices, where contamination by MC is suspected or certain, must be removed from the operating room or from use as soon as possible.
- (b)
- Facilities equipped with devices where no MC contamination has been confirmed must:
- Observe the instructions for use for heater–cooler devices, particularly as regards cleaning and disinfection.
- If the operating room available permits, direct or channel the heater–cooler’s exhaust vent away from the patient, e.g. towards the operating room exhaust vent in line with the safety notice on the “Risks of Mycobacteria Infection in Cardiac Surgery”.
- Monitor the water quality in accord with the safety notice on the “Risks of Mycobacteria Infection in Cardiac Surgery”.
- Use new accessories, tubing, and connectors to prevent recontamination if using a different heater–cooler device.
3.3. Literature Review
3.3.1. Physical Containment Measures
3.3.2. Operator Training and Monitoring Patients at Risk
3.3.3. Information to Provide to Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tortoli, E.; Rindi, L.; Garcia, M.J.; Chiaradonna, P.; Dei, R.; Garzelli, C.; Kroppenstedt, R.M.; Lari, N.; Mattei, R.; Mariottini, A.; et al. Proposal to elevate the genetic variant MAC-A, included in the Mycobacterium avium complex, to species rank as Mycobacterium chimaera sp. nov. Int. J. Syst. Evol. Microbiol. 2004, 54, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Boyle, D.P.; Zembower, T.R.; Reddy, S.; Qi, C. Comparison of clinical features, virulence, and relapse among Mycobacterium avium complex species. Am. J. Respir. Crit. Care Med. 2015, 191, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Schweickert, B.; Goldenberg, O.; Richter, E.; Göbel, U.B.; Petrich, A.; Buchholz, P.; Moter, A. Occurrence and clinical relevance of Mycobacterium chimaera sp. nov., Germany. Emerg. Infect. Dis. 2008, 14, 1443–1446. [Google Scholar] [CrossRef] [PubMed]
- Van Ingen, J.; Hoefsloot, W.; Buijtels, P.C.A.M.; Tortoli, E.; Supply, P.; Dekhuijzen, P.N.R.; Boeree, M.J.; Van Soolingen, D. Characterization of a novel variant of Mycobacterium chimaera. J. Med. Microbiol. 2012, 61, 1234–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, R.J.; Iakhiaeva, E.; Williams, M.D.; Brown-Elliott, B.A.; Vasireddy, S.; Vasireddy, R.; Lande, L.; Peterson, D.D.; Sawicki, J.; Kwait, R.; et al. Absence of Mycobacterium intracellulare and presence of Mycobacterium chimaera in household water and biofilm samples of patients in the United States with Mycobacterium avium complex respiratory disease. J. Clin. Microbiol. 2013, 51, 1747–1752. [Google Scholar] [CrossRef] [Green Version]
- Durnez, L.; Eddyani, M.; Mgode, G.F.; Katakweba, A.; Katholi, C.R.; Machang’U, R.R.; Kazwala, R.R.; Portaels, F.; Leirs, H. First detection of mycobacteria in African rodents and insectivores, using stratified pool screening. Appl. Environ. Microbiol. 2007, 74, 768–773. [Google Scholar] [CrossRef] [Green Version]
- Bills, N.D.; Hinrichs, S.H.; Aden, T.A.; Wickert, R.S.; Iwen, P.C. Molecular identification of Mycobacterium chimaera as a cause of infection in a patient with chronic obstructive pulmonary disease. Diagn. Microbiol. Infect. Dis. 2009, 63, 292–295. [Google Scholar] [CrossRef]
- Cohen-Bacrie, S.; David, M.; Le Bel, N.S.; Dubus, J.-C.; Rolain, J.-M.; Drancourt, M. Mycobacterium chimaera pulmonary infection complicating cystic fibrosis: A case report. J. Med. Case Rep. 2011, 5, 473. [Google Scholar] [CrossRef] [Green Version]
- Larcher, R.; Lounnas, M.; Dumont, Y.; Michon, A.-L.; Bonzon, L.; Chiron, R.; Carriere, C.; Klouche, K.; Godreuil, S. Mycobacterium chimaera pulmonary disease in cystic fibrosis patients, France, 2010–2017. Emerg. Infect. Dis. 2019, 25, 611–613. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Chen, S.-T.; Yu, X.; Li, Y.-X.; Ling, Y.; Dong, L.-L.; Zheng, S.-H.; Huang, H.-R. Bacteriological and virulence study of a Mycobacterium chimaera isolate from a patient in China. Antonie Leeuwenhoek 2015, 107, 901–909. [Google Scholar] [CrossRef]
- Honda, J.R.; Hasan, N.A.; Davidson, R.M.; Williams, M.D.; Epperson, L.E.; Reynolds, P.R.; Smith, T.; Iakhiaeva, E.; Bankowski, M.J.; Wallace, R.J.; et al. Environmental nontuberculous mycobacteria in the Hawaiian Islands. PLoS Neglected Trop. Dis. 2016, 10, e0005068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soetaert, K.; Vluggen, C.; André, E.; Vanhoof, R.; Vanfleteren, B.; Mathys, V. Frequency of Mycobacterium chimaera among Belgian patients, 2015. J. Med. Microbiol. 2016, 65, 1307–1310. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.; Cooper, R.; Chen, J.; Sim, V.L.; McCombe, J.A.; Tyrrell, G.J.; Bhargava, R.; Adam, B.; Chapman, E.; Croxen, M.A.; et al. Mycobacterium chimaera encephalitis post-cardiac surgery: A new syndrome. Clin. Infect. Dis. 2019, 70, 692–695. [Google Scholar] [CrossRef]
- Zweifel, S.A.; Mihic-Probst, D.; Curcio, C.A.; Barthelmes, D.; Thielken, A.; Keller, P.M.; Hasse, B.; Böni, C. Clinical and histopathologic ocular findings in disseminated Mycobacterium chimaera infection after cardiothoracic surgery. Ophthalmology 2017, 124, 178–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lecorche, E.; De Ponfilly, G.P.; Mougari, F.; Benmansour, H.; Poisnel, E.; Janvier, F.; Cambau, E. disseminated Mycobacterium chimaera following open-heart surgery, the heater-cooler unit worldwide outbreak: Case report and minireview. Front. Med. 2020, 7. [Google Scholar] [CrossRef]
- Chand, M.; Lamagni, T.; Kranzer, K.; Hedge, J.; Moore, G.; Parks, S.; Collins, S.; Elias, C.D.O.; Ahmed, N.; Brown, T.; et al. Insidious risk of severe Mycobacterium chimaera infection in cardiac surgery patients. Clin. Infect. Dis. 2016, 64, 335–342. [Google Scholar] [CrossRef] [Green Version]
- Maurer, F.P.; Pohle, P.; Kernbach, M.; Sievert, D.; Hillemann, R.; Rupp, J.; Hombach, M.; Kranzer, K. Differential drug susceptibility patterns of Mycobacterium chimaera and other members of the Mycobacterium avium-intracellulare complex. Clin. Microbiol. Infect. 2019, 25, 379. [Google Scholar] [CrossRef] [Green Version]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef]
- Overton, K.; Mennon, V.; Mothobi, N.; Neild, B.; Martinez, E.; Masters, J.; Grant, P.; Akhunji, Z.; Su, W.-Y.; Torda, A.; et al. Cluster of invasive Mycobacteria chimaera infections following cardiac surgery demonstrating novel clinical features and risks of aortic valve replacement. Intern. Med. J. 2018, 48, 1514–1520. [Google Scholar] [CrossRef]
- Kasperbauer, S.H.; Daley, C.L. Mycobacterium chimaera infections related to the heater-cooler unit outbreak: A guide to diagnosis and management. Clin. Infect. Dis. 2018, 68, 1244–1250. [Google Scholar] [CrossRef]
- Schreiber, P.W.; Sax, H. Mycobacterium chimaera infections associated with heater-cooler units in cardiac surgery. Curr. Opin. Infect. Dis. 2017, 30, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Scriven, J.E.; Scobie, A.; Verlander, N.Q.; Houston, A.; Collyns, T.; Čajić, V.; Kon, O.M.; Mitchell, T.; Rahama, O.; Robinson, A.; et al. Mycobacterium chimaera infection following cardiac surgery in the United Kingdom: Clinical features and outcome of the first 30 cases. Clin. Microbiol. Infect. 2018, 24, 1164–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falkinham, J.O.; Norton, C.D.; Lechevallier, M.W. Factors influencing numbers of Mycobacterium avium, Mycobacterium intracellulare, and other mycobacteria in drinking water distribution systems. Appl. Environ. Microbiol. 2001, 67, 1225–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohler, P.; Kuster, S.P.; Bloemberg, G.; Schulthess, B.; Frank, M.; Tanner, F.C.; Rössle, M.; Böni, C.; Falk, V.; Wilhelm, M.J.; et al. Healthcare-associated prosthetic heart valve, aortic vascular graft, and disseminated Mycobacterium chimaera infections subsequent to open heart surgery. Eur. Hear. J. 2015, 36, 2745–2753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sax, H.; Bloemberg, G.; Hasse, B.; Sommerstein, R.; Kohler, P.; Achermann, Y.; Rössle, M.; Falk, V.; Kuster, S.P.; Böttger, E.C.; et al. Prolonged outbreak of Mycobacterium chimaera infection after open-chest heart surgery. Clin. Infect. Dis. 2015, 61, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Achermann, Y.; Rössle, M.; Hoffmann, M.; Deggim, V.; Kuster, S.; Zimmermann, D.R.; Bloemberg, G.; Hombach, M.; Hasse, B. Prosthetic valve endocarditis and bloodstream infection due to Mycobacterium chimaera. J. Clin. Microbiol. 2013, 51, 1769–1773. [Google Scholar] [CrossRef] [Green Version]
- Acosta, F.; Pérez-Lago, L.; Serrano, M.R.; Marín, M.; Kohl, T.A.; Lozano, N.; Niemann, S.; Valerio, M.; Olmedo, M.; Pérez-Granda, M.J.; et al. Fast update of undetected Mycobacterium chimaera infections to reveal unsuspected cases. J. Hosp. Infect. 2018, 100, 451–455. [Google Scholar] [CrossRef]
- Williamson, D.A.; Howden, B.; Stinear, T. Mycobacterium chimaera spread from heating and cooling units in heart surgery. New Engl. J. Med. 2017, 376, 600–602. [Google Scholar] [CrossRef]
- Bursle, E.; Playford, E.G.; Coulter, C.; Griffin, P. First Australian case of disseminated Mycobacterium chimaera infection post-cardiothoracic surgery. Infect. Dis. Heal. 2017, 22, 1–5. [Google Scholar] [CrossRef]
- Sommerstein, R.; Schreiber, P.W.; Diekema, D.J.; Edmond, M.B.; Hasse, B.; Marschall, J.; Sax, H. Mycobacterium chimaera outbreak associated with heater-cooler devices: Piecing the puzzle together. Infect. Control. Hosp. Epidemiol. 2016, 38, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Haller, S.; Höller, C.; Jacobshagen, A.; Hamouda, O.; Abu Sin, M.; Monnet, D.L.; Plachouras, D.; Eckmanns, T. Contamination during production of heater-cooler units by Mycobacterium chimaera potential cause for invasive cardiovascular infections: Results of an outbreak investigation in Germany, April 2015 to February 2016. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [Green Version]
- Perkins, K.M.; Lawsin, A.; Hasan, N.A.; Strong, M.; Halpin, A.L.; Rodger, R.R.; Moulton-Meissner, H.; Crist, M.B.; Schwartz, S.; Marders, J.; et al. Notes from the field: Mycobacterium chimaera contamination of heater-cooler devices used in cardiac surgery-United States. MMWR. Morb. Mortal. Wkly. Rep. 2016, 65, 1117–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trudzinski, F.C.; Schlotthauer, U.; Kamp, A.; Hennemann, K.; Muellenbach, R.M.; Reischl, U.; Gärtner, B.; Wilkens, H.; Bals, R.; Herrmann, M.; et al. Clinical implications of Mycobacterium chimaera detection in thermoregulatory devices used for extracorporeal membrane oxygenation (ECMO), Germany, 2015 to 2016. Eurosurveillance 2016, 21, 30398. [Google Scholar] [CrossRef] [PubMed]
- Götting, T.; Klassen, S.; Jonas, D.; Benk, C.; Serr, A.; Wagner, D.; Ebner, W. Heater-cooler units: Contamination of crucial devices in cardiothoracic surgery. J. Hosp. Infect. 2016, 93, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Lyman, M.M.; Grigg, C.; Kinsey, C.B.; Keckler, M.S.; Moulton-Meissner, H.; Cooper, E.; Soe, M.M.; Noble-Wang, J.; Longenberger, A.; Walker, S.R.; et al. Invasive nontuberculous mycobacterial infections among cardiothoracic surgical patients exposed to heater-cooler devices1. Emerg. Infect. Dis. 2017, 23, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Sommerstein, R.; Rüegg, C.; Kohler, P.; Bloemberg, G.; Kuster, S.P.; Sax, H. Transmission of Mycobacterium chimaera from heater-cooler units during cardiac surgery despite an ultraclean air ventilation system. Emerg. Infect. Dis. 2016, 22, 1008–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control (ECDC). EU Protocol for Case Detection, Laboratori Diagnosis and Environmental Testing of Mycobacterium Chimaera Infections Potentially Associated with Heater-Cooler Units: Case Definition and Environmental Testing Methodology; ECDC: Stockholm, Sweden, 2015; Available online: https://www.ecdc.europa.eu/en/publications-data/eu-protocol-case-detection-laboratory-diagnosis-and-environmental-testing (accessed on 30 July 2020).
- European Centre for Disease Prevention and Control (ECDC). Invasive Cardiovascular Infection by Mycobacterium Chimaera Associated with 3T Heater-Cooler System Used during Open-Heart Surgery-18 November 2016; ECDC: Stockholm, Sweden, 2016; Available online: https://www.ecdc.europa.eu/en/publications-data/rra-invasive-cardiovascular-infection-mycobacterium-chimaera-associated-3t-heater (accessed on 30 July 2020).
- Centers for Disease Control and Prevention (CDC). Non-Tuberculous Mycobacterium (NTM) Infections and Heater-Cooler Devices Interim Practical Guidance: Updated October 27, 2015. CDC: Atlanta. Available online: http://www.cdc.gov/hai/pdfs/outbreaks/cdc-notice-heater-cooler-units-final-clean.pdf (accessed on 30 July 2020).
- National Infection Control Guidance for Non-Tuberculous Mycobacterium Associated with Heater-Cooler Devices; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2017. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/national-infection-control-guidance-non-tuberculous-mycobacterium-associated-heater-cooler-devices (accessed on 30 July 2020).
- Sorin Group Deutschland GMBH. Potential Cardiac Surgery Infection Risk Reduction Measure: Hydrogen Peroxide Concentration Monitoring. Available online: http://www.salute.gov.it/imgs/C_17_AvvisiSicurezza_8434_azione_itemAzione0_files_itemFiles0_fileAzione.pdf (accessed on 30 July 2020).
- Sorin Group Deutschland GMBH. Risks of Mycobacterial Contamination in Cardiac Surgery. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=5645 (accessed on 30 July 2020).
- Maquet Cardiopulmonary GmbH. Review of Washing and Decontamination Procedures. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=6247 (accessed on 30 July 2020).
- Sorin Group Italia, S.R.L. Security Notice. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=6690 (accessed on 30 July 2020).
- Sorin Group Deutschland GmbH. Security Notice. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=6744 (accessed on 30 July 2020).
- Sorin Group Deutschland GmbH. Security Notice. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=6745 (accessed on 30 July 2020).
- Sorin Group Deutschland GMBH. Sistema Generatore Termico. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=6770 (accessed on 30 July 2020).
- Sorin Group Deutschland GMBH. Security Notice. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=7050 (accessed on 30 July 2020).
- Maquet Cardiopulmonary, A.G. Security Istructions. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=7074 (accessed on 30 July 2020).
- Maquet Cardiopulmonary, A.G. Security Istructions. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=7077 (accessed on 30 July 2020).
- Livanova Deutschland GMBH. Heater-Cooler 3T. Available online: http://www.salute.gov.it/portale/news/p3_2_1_3_1_1.jsp?lingua=italiano&menu=notizie&p=avvisi&tipo=dispo&id=8434 (accessed on 30 July 2020).
- Ortiz-Martínez, Y.; Galindo-Regino, C.; González-Hurtado, M.R.; Vanegas-Pastrana, J.J.; Valdes-Villegas, F. State of the art on Mycobacterium chimaera research: A bibliometric analysis. J. Hosp. Infect. 2018, 100, e159–e160. [Google Scholar] [CrossRef]
- Matteo, S.; Anna, A.; Matteo, B. Mycobacterium chimaera: Clinical and medico-legal considerations starting from a case of sudden acoustic damage. Leg. Med. 2020, 47, 101747. [Google Scholar] [CrossRef]
- Struelens, M.J.; Plachouras, D. Mycobacterium chimaera infections associated with heater-cooler units (HCU): Closing another loophole in patient safety. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [Green Version]
- Ogunremi, T.; Taylor, G.; Johnston, L.; Amaratunga, K.; Muller, M.; Coady, A.; DeFalco, K.; Dunn, K.; Johnstone, J.; Smith, S.; et al. Mycobacterium chimaera infections in post-operative patients exposed to heater-cooler devices: An overview. Can. Commun. Dis. Rep. 2017, 43, 107–113. [Google Scholar] [CrossRef]
- Marra, A.R.; Diekema, D.J.; Edmond, M.B. Mycobacterium chimaera infections associated with contaminated heater-cooler devices for cardiac surgery: Outbreak management. Clin. Infect. Dis. 2017, 65, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.A.; Dandekar, U.; Fraser, N.; Dawkin, L.; Sweeney, P.; Heron, F.; Simmons, J.; Parmar, J. Minimising the risk of Mycobacterium chimaera infection during cardiopulmonary bypass by the removal of heater-cooler units from the operating room. Perfusion 2017, 33, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Public Health England, Medicines and Healthcare Products Regulatory Agency, Health and Safety Executive, NHS England. Infections Associated with Heater Cooler Units Used in Cardiopulmonary Bypass and ECMO: Guidance for Healthcare Providers in the UK. 2017. Available online: https://www.gov.uk/government/publications/infections-associated-with-heater-cooler-units-used-in-cardiopulmonary-bypass-and-ecmo (accessed on 30 July 2020).
- Kanamori, H.; Weber, D.J.; Rutala, W.A. Healthcare outbreaks associated with a water reservoir and infection prevention strategies. Clin. Infect. Dis. 2016, 62, 1423–1435. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.H.; Falkinham, J.O.; Norton, C.D.; Lechevallier, M.W. Chlorine, chloramine, chlorine dioxide, and ozone susceptibility of Mycobacterium avium. Appl. Environ. Microbiol. 2000, 66, 1702–1705. [Google Scholar] [CrossRef] [Green Version]
- Norton, G.J.; Williams, M.; Falkinham, J.O.I.; Honda, J.R. Physical measures to reduce exposure to tap water-associated nontuberculous mycobacteria. Front. Public Heal. 2020, 8. [Google Scholar] [CrossRef]
- Schreiber, P.W.; Kuster, S.P.; Hasse, B.; Bayard, C.; Rüegg, C.P.; Kohler, P.; Keller, P.M.; Bloemberg, G.V.; Maisano, F.; Bettex, D.; et al. Reemergence of Mycobacterium chimaera in heater-cooler units despite intensified cleaning and disinfection protocol. Emerg. Infect. Dis. 2016, 22, 1830–1833. [Google Scholar] [CrossRef] [Green Version]
- Canadian Public Health Laboratory Network (CPHLN) Testing Working Group. Device Testing Recommendations Regarding Non-Tuberculous Mycobacteria (NTM) Contamination in Heater-Cooler Units. Available online: www.canada.ca/en/public-health/services/publications/diseases-conditions/device-testing-non-tuberculous-mycobacteria-contamination-heater-cooler.html (accessed on 30 July 2020).
- Bolcato, M.; De Salvia, A.; Rodriguez, D.; Aprile, A. Is the Italian consent to transfusion really informed? A medico-legal analysis between old ghosts and new evidence. Transfus. Apher. Sci. 2020, 102823, 102823. [Google Scholar] [CrossRef]
- D’Errico, S.; Pennelli, S.; Colasurdo, A.P.; Frati, P.; Sicuro, L.; Fineschi, V. The right to be informed and fear of disclosure: Sustainability of a full error disclosure policy at an Italian cancer centre/clinic. BMC Health Serv. Res. 2015, 15, 130. [Google Scholar] [CrossRef] [Green Version]
- Ben Appenheimer, A.; Diekema, D.J.; Berriel-Cass, D.; Crook, T.; Daley, C.L.; Dobbie, D.; Edmond, M.; Hellinger, W.; Ince, D.; Julian, K.G.; et al. Mycobacterium chimaera outbreak response: Experience from four United States healthcare systems. Open Forum Infect. Dis. 2016, 3, 2637746. [Google Scholar] [CrossRef]
- Gatto, V.; Scopetti, M.; La Russa, R.; Santurro, A.; Cipolloni, L.; Viola, R.V.; Di Sanzo, M.; Frati, P.; Fineschi, V. Advanced loss eventuality assessment and technical estimates: An integrated approach for management of healthcare-associated infections. Curr. Pharm. Biotechnol. 2019, 20, 625–634. [Google Scholar] [CrossRef]
- Giraldi, G.; Montesano, M.; Napoli, C.; Frati, P.; La Russa, R.; Santurro, A.; Scopetti, M.; Orsi, G.B. Healthcare-associated infections due to multidrug-resistant organisms: A surveillance study on extra hospital stay and direct costs. Curr. Pharm. Biotechnol. 2019, 20, 643–652. [Google Scholar] [CrossRef] [PubMed]
- La Russa, R.; Finesch, V.; Di Sanzo, M.; Gatto, V.; Santurro, A.; Martini, G.; Scopetti, M.; Frati, P. Personalized medicine and adverse drug reactions: The experience of an italian teaching hospital. Curr. Pharm. Biotechnol. 2017, 18, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Bellandi, T.; Tartaglia, R.; Sheikh, A.; Donaldson, L. Italy recognises patient safety as a fundamental right. BMJ 2017, 357, j2277. [Google Scholar] [CrossRef] [PubMed]
- Bolcato, M.; Russo, M.; Rodriguez, D.; Aprile, A. Patient blood management implementation in light of new Italian laws on patient’s safety. Transfus. Apher. Sci. 2020, 59, 102811. [Google Scholar] [CrossRef] [PubMed]
- Bolcato, M.; Russo, M.; Trentino, K.; Isbister, J.; Rodriguez, D.; Aprile, A. Patient blood management: The best approach to transfusion medicine risk management. Transfus. Apher. Sci. 2020, 59, 102779. [Google Scholar] [CrossRef] [PubMed]
- Bolcato, M.; Fassina, G.; Rodriguez, D.; Russo, M.; Aprile, A. The contribution of legal medicine in clinical risk management. BMC Health Serv. Res. 2019, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Safety Notice: 6 February 2015. Disinfection and cleaning of Sorin heat generators [42] |
| Safety Notice: 9 December 2015. Revised washing and decontamination procedures [43] |
| Safety Notice: 15 June 2016. Recall on disinfection and cleaning of oxygenator mounting brackets [44] |
| Safety Notice: 1 July 2016. Recall on disinfection and cleaning of oxygenator mounting brackets [45] |
| Safety Notice: 1 July 2016 (2nd) Disinfection and cleaning of pediatric oxygenator mounting brackets [46] |
| Safety Notice: 8 July 2016. Safety information on heat generator system [47] |
| Safety Notice: 11 November 2016. Updated instructions to monitor and adjust the concentration of hydrogen peroxide in the water circuit to limit microbial growth [41] |
| Safety Notice: 1 December 2016. Risks related to extracorporeal circulation instrumentation [48] |
| Safety Notice: 14 December 2016. Revised Heating Unit HU35 disinfection procedure [49] |
| Safety Notice: 16 December 2016. Safety Instructions HCU 40 [50] |
| Safety Notice: 29 October 2018. Updated instructions to monitor and adjust the concentration of hydrogen peroxide in the water circuit to limit microbial growth [51] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolcato, M.; Rodriguez, D.; Aprile, A. Risk Management in the New Frontier of Professional Liability for Nosocomial Infection: Review of the Literature on Mycobacterium Chimaera. Int. J. Environ. Res. Public Health 2020, 17, 7328. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197328
Bolcato M, Rodriguez D, Aprile A. Risk Management in the New Frontier of Professional Liability for Nosocomial Infection: Review of the Literature on Mycobacterium Chimaera. International Journal of Environmental Research and Public Health. 2020; 17(19):7328. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197328
Chicago/Turabian StyleBolcato, Matteo, Daniele Rodriguez, and Anna Aprile. 2020. "Risk Management in the New Frontier of Professional Liability for Nosocomial Infection: Review of the Literature on Mycobacterium Chimaera" International Journal of Environmental Research and Public Health 17, no. 19: 7328. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197328