Impact of Ambient Temperature and Relative Humidity on the Incidence of Hand-Foot-Mouth Disease in Wuhan, China

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Area
2.2. Data Collection
2.3. Statistical Analysis
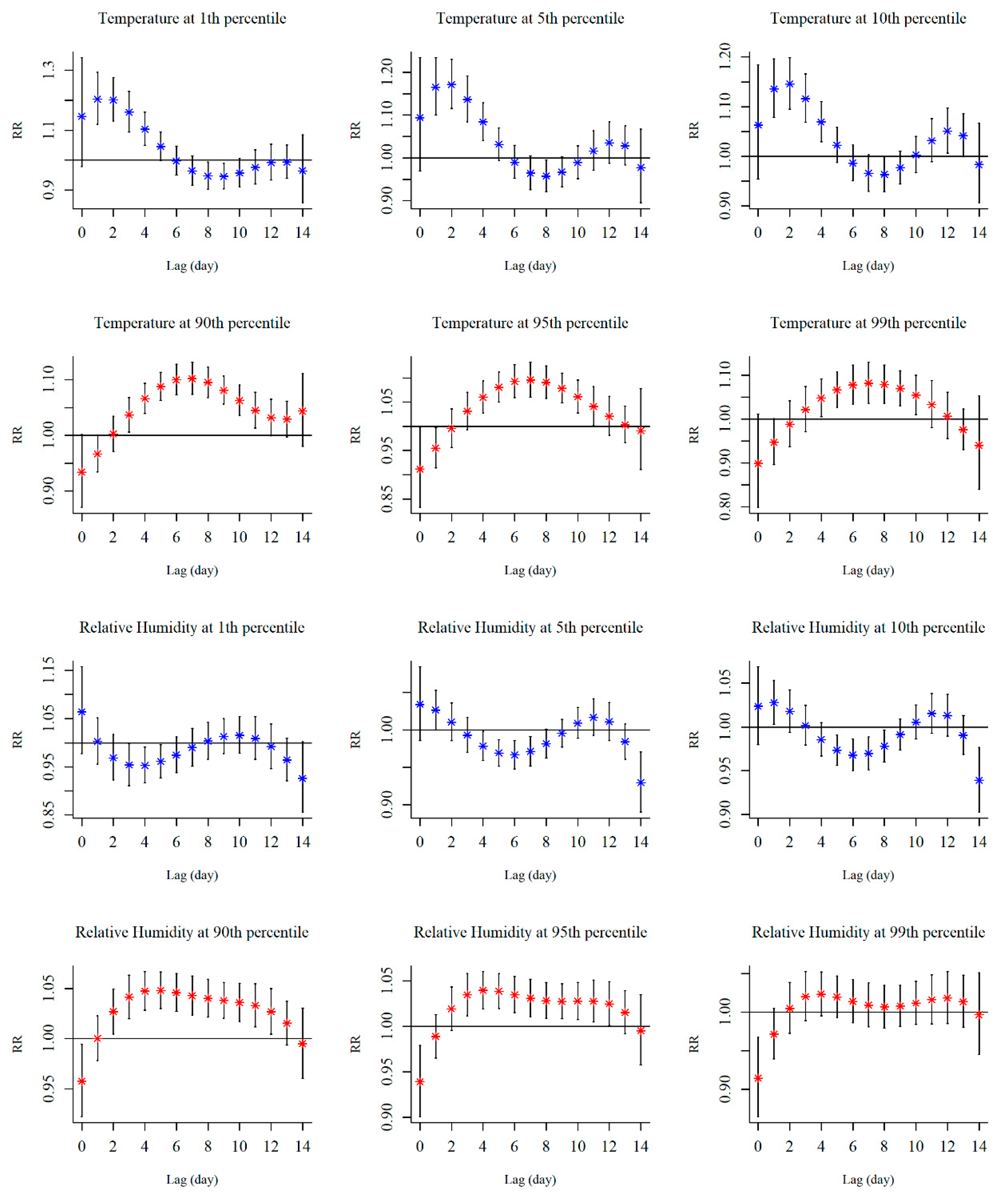
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD). Available online: https://www.who.int/westernpacific/emergencies/surveillance/archives/hand-foot-and-mouth-disease (accessed on 25 May 2019).
- Park, S.K.; Park, B.; Ki, M.; Kim, H.; Lee, K.; Jung, C.; Sohn, Y.M.; Choi, S.-M.; Kim, D.-K.; Lee, D.S.; et al. Transmission of seasonal outbreak of childhood enteroviral aseptic meningitis and hand-foot-mouth disease. J. Korean Med. Sci. 2010, 25, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Ooi, M.H.; Wong, S.C.; Lewthwaite, P.; Cardosa, M.J.; Solomon, T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010, 9, 1097–1105. [Google Scholar] [CrossRef]
- Huang, C.C.; Liu, C.C.; Chang, Y.C.; Chen, C.Y.; Wang, S.T.; Yeh, T.F. Neurologic complications in children with enterovirus 71 infection. N. Engl. J. Med. 1999, 341, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Chen, E.-R.; Hsu, K.-H.; Twu, S.-J.; Chen, K.-T.; Tsai, S.-F.; Wang, J.-R.; Shih, S.-R. An epidemic of enterovirus 71 infection in Taiwan. N. Engl. J. Med. 1999, 341, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tan, X.-J.; Wang, H.-Y.; Yan, D.-M.; Zhu, S.-L.; Wang, D.-Y.; Ji, F.; Wang, X.-J.; Gao, Y.-J.; Chen, L.; et al. An outbreak of hand, foot, and mouth disease associated with subgenotype C4 of human enterovirus 71 in Shandong, China. J. Clin. Virol. 2009, 44, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.-Z.; Wang, X.-M.; Sun, S.-W.; Song, Q.; Li, S.-N.; He, C.-Q. Appearance of mosaic enterovirus 71 in the 2008 outbreak of China. Virus Res. 2009, 145, 157–161. [Google Scholar] [CrossRef]
- NHFPC. The National Statutory Epidemic Situation of Infectious Diseases in 2012. Available online: http://www.moh.gov.cn/wsb/pyqxx/201303/f02d91321f524a66a9df357a53bd0cf0.shtml (accessed on 23 April 2019).
- Wu, X.; Lu, Y.; Zhou, S.; Chen, L.; Xu, B. Impact of climate change on human infectious diseases: Empirical evidence and human adaptation. Environ. Int. 2016, 86, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Zhang, J.; Zhang, Y.; Lao, J.; Liu, Y.; Wang, H.; Jiang, B. Effects and interaction of meteorological factors on influenza: Based on the surveillance data in Shaoyang, China. Environ. Res. 2019, 172, 326–332. [Google Scholar] [CrossRef]
- Xiao, Y.; He, L.; Chen, Y.; Wang, Q.; Meng, Q.; Chang, W.; Xiong, L.; Yu, Z. The influence of meteorological factors on tuberculosis incidence in Southwest China from 2006 to 2015. Sci. Rep. 2018, 8, 10053. [Google Scholar] [CrossRef]
- Yu, G.; Yang, R.; Yu, D.; Cai, J.; Tang, J.; Zhai, W.; Wei, Y.; Chen, S.; Chen, Q.; Zhong, G.; et al. Impact of meteorological factors on mumps and potential effect modifiers: An analysis of 10 cities in Guangxi, Southern China. Environ. Res. 2018, 166, 577–587. [Google Scholar] [CrossRef]
- Onozuka, D.; Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci. Total Environ. 2011, 410–411, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wang, H.; Wang, Q.; Xin, Q.; Lin, H. The effect of meteorological factors on adolescent hand, foot, and mouth disease and associated effect modifiers. Glob. Health Action 2014, 7, 24664. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; You, E.; Wu, J.; Zhang, W.; Jin, J.; Zhou, M.; Jiang, C.; Huang, F. Effects of relative humidity on childhood hand, foot, and mouth disease reinfection in Hefei, China. Sci. Total Environ. 2018, 630, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Lam, T.; Wong, C.; Chuang, S.K. Is hand, foot and mouth disease associated with meteorological parameters? Epidemiol. Infect. 2010, 138, 1779–1788. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Lin, H.; Li, X.; Lang, L.; Xiao, X.; Ding, P.; He, P.; Zhang, Y.; Wang, M.; Liu, Q. Short-term effects of meteorological factors on children hand, foot and mouth disease in Guangzhou, China. Int. J. Biometeorol. 2014, 58, 1605–1614. [Google Scholar] [CrossRef]
- Huang, R.; Bian, G.; He, T.; Chen, L.; Xu, G. Effects of meteorological parameters and PM10 on the Incidence of hand, foot, and mouth disease in children in China. Int. J. Environ. Res. Public Health 2016, 13, 481. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Wang, L.; Cheng, J.; Xu, J.; Xu, Z.; Xie, M.; Yang, H.; Li, K.; Wen, L.; Wang, X.; et al. Impact of weather factors on hand, foot and mouth disease, and its role in short-term incidence trend forecast in Huainan City, Anhui Province. Int. J. Biometeorol. 2017, 61, 453–461. [Google Scholar] [CrossRef]
- Zhang, Z.; Xie, X.; Chen, X.; Li, Y.; Lu, Y.; Mei, S.; Liao, Y.; Lin, H. Short-term effects of meteorological factors on hand, foot and mouth disease among children in Shenzhen, China: Non-linearity, threshold and interaction. Sci. Total Environ. 2016, 539, 576–582. [Google Scholar] [CrossRef]
- Du, Z.; Zhang, W.; Zhang, D.; Yu, S.; Hao, Y. The threshold effects of meteorological factors on Hand, foot, and mouth disease (HFMD) in China, 2011. Sci. Rep. 2016, 6, 36351. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-C.; Juan, H.-C.; Cheng, Y.-C. Ozone exposure in the culture medium inhibits enterovirus 71 virus replication and modulates cytokine production in rhabdomyosarcoma cells. Antivir. Res. 2007, 76, 241–251. [Google Scholar] [CrossRef]
- Yu, G.; Li, Y.; Cai, J.; Yu, D.; Tang, J.; Zhai, W.; Wei, Y.; Chen, S.; Chen, Q.; Qin, J. Short-term effects of meteorological factors and air pollution on childhood hand-foot-mouth disease in Guilin, China. Sci. Total Environ. 2019, 646, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Jiao, K.; Hu, W.; Ren, C.; Xu, Z.; Ma, W. Impacts of tropical cyclones and accompanying precipitation and wind velocity on childhood hand, foot and mouth disease in Guangdong Province, China. Environ. Res. 2019, 173, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhou, M.; Yang, Y.; You, E.; Wu, J.; Zhang, W.; Jin, J.; Huang, F. Short-term effects of extreme meteorological factors on childhood hand, foot, and mouth disease reinfection in Hefei, China: A distributed lag non-linear analysis. Sci. Total Environ. 2019, 653, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Lawrence, W.R.; Zhang, W.; Zhang, D.; Yu, S.; Hao, Y. Interactions between climate factors and air pollution on daily HFMD cases: A time series study in Guangdong, China. Sci. Total Environ. 2019, 656, 1358–1364. [Google Scholar] [CrossRef]
- Zhong, P.; Huang, S.; Zhang, X.; Wu, S.; Zhu, Y.; Li, Y.; Ma, L. Individual-level modifiers of the acute effects of air pollution on mortality in Wuhan, China. Glob. Health Res. Policy 2018, 3, 27. [Google Scholar] [CrossRef]
- Health, C.M.o. Diagnostic Criteria and Principle of Management for Hand Foot Mouth Disease. Available online: http://www.nhc.gov.cn/yzygj/s3593g/201306/6d935c0f43cd4a1fb46f8f71acf8e245.shtml (accessed on 21 April 2019).
- Wei, Q.; Wu, J.; Zhang, Y.; Cheng, Q.; Bai, L.; Duan, J.; Gao, J.; Xu, Z.; Yi, W.; Pan, R.; et al. Short-term exposure to sulfur dioxide and the risk of childhood hand, foot, and mouth disease during different seasons in Hefei, China. Sci. Total Environ. 2019, 658, 116–121. [Google Scholar] [CrossRef]
- Yin, F.; Zhang, T.; Liu, L.; Lv, Q.; Li, X. The association between ambient temperature and childhood hand, foot, and mouth disease in Chengdu, China: A distributed lag non-linear analysis. Sci. Rep. 2016, 6, 27305. [Google Scholar] [CrossRef]
- Steadman, R.G. A universal scale of apparent temperature. J. Clim. Appl. Meteorol. 1984, 23, 1674–1687. [Google Scholar] [CrossRef]
- Smith, G.S.; Van Den Eeden, S.K.; Garcia, C.; Shan, J.; Baxter, R.; Herring, A.H.; Richardson, D.B.; Van Rie, A.; Emch, M.; Gammon, M.D. Air pollution and pulmonary tuberculosis: A nested case-control study among members of a northern California health plan. Environ. Health Perspect. 2016, 124, 761–768. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Chen, S.; Wu, Y.; Tong, Y.; Wang, L.; Zhu, M.; Hu, S.; Guan, X.; Wei, S. Quantifying the influence of temperature on hand, foot and mouth disease incidence in Wuhan, Central China. Sci. Rep. 2018, 8, 1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, J.; Yu, S.; Yang, F.; Yang, M.; Hu, Y.; Zhang, J. Short-Term Effects of Climatic Variables on Hand, Foot, and Mouth Disease in Mainland China, 2008–2013: A Multilevel Spatial Poisson Regression Model Accounting for Overdispersion. PLoS ONE 2016, 11, e0147054. [Google Scholar] [CrossRef] [PubMed]
- Altizer, S.; Dobson, A.; Hosseini, P.; Hudson, P.; Pascual, M.; Rohani, P. Seasonality and the dynamics of infectious diseases. Ecol. Lett. 2010, 9, 467–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, X.; Gasparrini, A.; Huang, J.; Liao, Q.; Liu, F.; Yin, F.; Yu, H.; Li, X. The exposure-response relationship between temperature and childhood hand, foot and mouth disease: A multicity study from mainland China. Environ. Int. 2017, 100, 102–109. [Google Scholar] [CrossRef]
- Bertrand, I.; Schijven, J.F.; Sánchez, G.; Wyn-Jones, P.; Ottoson, J.; Morin, T.; Muscillo, M.; Verani, M.; Nasser, A.; Husman, A.M. The impact of temperature on the inactivation of enteric viruses in food and water: A review. J. Appl. Microbiol. 2012, 112, 1059–1074. [Google Scholar] [CrossRef]
- Fletcher, J. The importance of correctly choosing a bandage and bandaging technique. Nurs. Times 2004, 100, 52. [Google Scholar]
- Wong, S.S.Y.; Yip, C.C.Y.; Lau, S.K.P.; Yuen, K.Y. Human enterovirus 71 and hand, foot and mouth disease. Epidemiol. Infect. 2010, 138, 1071–1089. [Google Scholar] [CrossRef] [Green Version]
- Abad, F.X.; Pintó, R.M.; Bosch, A. Survival of enteric viruses on environmental fomites. Appl. Environ. Microbiol. 1994, 60, 3704–3710. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Zhang, C.; Wang, H.-q.; Sheng, X.; Xiao, L.; Sun, Y.-h.; Yang, B. Application of a laser-guided docking system in robot-assisted urologic surgery. Int. J. Med Robot. Comput. Assist. Surg. 2016, 12, 524–527. [Google Scholar] [CrossRef]
- Yang, H.; Wu, J.; Cheng, J.; Wang, X.; Wen, L.; Li, K.; Su, H. Is high relative humidity associated with childhood hand, foot, and mouth disease in rural and urban areas? Public Health 2017, 142, 201–207. [Google Scholar] [CrossRef]
- Royé, D.; Zarrabeitia, M.T.; Riancho, J.; Santurtún, A. A time series analysis of the relationship between apparent temperature, air pollutants and ischemic stroke in Madrid, Spain. Environ. Res. 2019, 173, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Vanos, J.K.; Kosaka, E.; Iida, A.; Yokohari, M.; Middel, A.; Scott-Fleming, I.; Brown, R.D. Planning for spectator thermal comfort and health in the face of extreme heat: The Tokyo 2020 Olympic marathons. Sci. Total Environ. 2019, 657, 904–917. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD | Min | 25th | 50th | 75th | Max |
|---|---|---|---|---|---|---|
| Ambient Temperature (°C) | 17.29 ± 8.97 | −4.32 | 9.55 | 18.40 | 24.80 | 33.45 |
| Apparent Temperature (°C) | 14.62 ± 9.54 | −8.55 | 6.32 | 15.64 | 22.77 | 31.76 |
| Relative Humidity (%) | 77.90 ± 10.99 | 40.66 | 70.54 | 78.65 | 86.09 | 100.00 |
| Wind Velocity (m/s) | 1.73 ± 0.95 | 0.90 | 1.04 | 1.54 | 2.21 | 7.16 |
| Atmospheric Pressure (hPa) | 1012.93 ± 9.39 | 994.22 | 1004.76 | 1012.59 | 1020.48 | 1041.62 |
| Vapor Pressure (hPa) | 17.07 ± 8.86 | 2.25 | 8.66 | 16.05 | 24.66 | 36.73 |
| PM10 (μg/m3) | 109.98 ± 57.43 | 12.23 | 67.90 | 100.13 | 140.36 | 405.97 |
| PM2.5 (μg/m3) | 72.28 ± 48.53 | 8.24 | 38.59 | 60.22 | 90.86 | 299.50 |
| SO2 (μg/m3) | 25.31 ± 17.67 | 3.70 | 12.90 | 20.69 | 32.14 | 107.58 |
| HFMD (counts/day) | 44.80 ± 38.11 | 0 | 17 | 31 | 64 | 239 |
| Variables | Ambient Temperature | Apparent Temperature | Relative Humidity | Wind Velocity | Atmospheric Pressure | Vapor Pressure | PM10 | PM2.5 | SO2 |
|---|---|---|---|---|---|---|---|---|---|
| Ambient Temperature | 1 | ||||||||
| Apparent Temperature | 0.998 * | 1 | |||||||
| Relative Humidity | −0.085 * | −0.075 * | 1 | ||||||
| Wind Velocity | 0.092 * | 0.037 | −0.124 * | 1 | |||||
| Atmospheric Pressure | −0.908 * | −0.904 * | −0.074 * | −0.135 * | 1 | ||||
| Vapor Pressure | 0.963 * | 0.965 * | 0.166 * | 0.061 * | −0.917 * | 1 | |||
| PM10 | −0.273 * | −0.263 * | −0.378 * | −0.274 * | 0.329 * | −0.376 * | 1 | ||
| PM2.5 | −0.496 * | −0.487 * | −0.141 * | −0.233 * | 0.488 * | −0.531 * | 0.869 * | 1 | |
| SO2 | −0.272 * | −0.268 * | −0.350 * | −0.109 * | 0.263 * | −0.361 * | 0.533 * | 0.551 * | 1 |
| Percentile | Ambient Temperature | Relative Humidity | ||
|---|---|---|---|---|
| Value (°C) | RR (95% CI) | Value (%) | RR (95% CI) | |
| 1th | −0.1 | 1.697 (1.113–2.588) | 49.2 | 0.805 (0.597–1.086) |
| 5th | 2.9 | 1.756 (1.224–2.518) | 59.0 | 0.878 (0.746–1.033) |
| 10th | 5.0 | 1.681 (1.202–2.351) | 63.5 | 0.900 (0.769–1.053) |
| 90th | 28.7 | 1.919 (1.530–2.407) | 92.2 | 1.474 (1.261–1.722) |
| 95th | 31.0 | 1.616 (1.221–2.138) | 94.7 | 1.304 (1.113–1.528) |
| 99th | 32.5 | 1.297 (0.916–1.839) | 97.5 | 1.044 (0.841–1.297) |
| Lag | Ambient Temperature | Relative Humidity | ||
|---|---|---|---|---|
| Value (°C) | RR (95% CI) | Value (%) | RR (95% CI) | |
| 0–1 | −4.3 | 1.543 (1.047–2.275) | 51.3 | 1.067 (0.966–1.178) |
| 0–2 | −4.3 | 1.893 (1.249–2.869) | 60.5 | 1.073 (0.994–1.157) |
| 0–3 | −4.3 | 2.238 (1.460–3.431) | 62.9 | 1.072 (0.986–1.165) |
| 0–4 | −4.3 | 2.521 (1.623–3.914) | 88.1 | 1.109 (1.020–1.207) |
| 0–5 | −4.3 | 2.691 (1.704–4.249) | 88.5 | 1.165 (1.061–1.278) |
| 0–6 | −4.3 | 2.725 (1.686–4.405) | 88.7 | 1.222 (1.105–1.352) |
| 0–7 | −4.3 | 2.631 (1.576–4.393) | 88.8 | 1.281 (1.149–1.428) |
| 0–8 | −4.3 | 2.444 (1.412–4.230) | 88.8 | 1.339 (1.192–1.504) |
| 0–9 | −4.3 | 2.208 (1.237–3.942) | 88.9 | 1.396 (1.234–1.579) |
| 0–10 | −4.3 | 1.965 (1.076–3.589) | 89.0 | 1.450 (1.273–1.651) |
| 0–11 | −1.4 | 1.795 (1.169–2.757) | 89.1 | 1.498 (1.306–1.719) |
| 0–12 | 28.3 | 1.791 (1.467–2.186) | 89.2 | 1.537 (1.329–1.779) |
| 0–13 | 28.2 | 1.847 (1.502–2.273) | 89.2 | 1.559 (1.337–1.818) |
| 0–14 | 27.9 | 1.945 (1.570–2.408) | 89.2 | 1.553 (1.322–1.824) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hao, J.; Yang, Z.; Yang, W.; Huang, S.; Tian, L.; Zhu, Z.; Lu, Y.; Xiang, H.; Liu, S. Impact of Ambient Temperature and Relative Humidity on the Incidence of Hand-Foot-Mouth Disease in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 428. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020428
Hao J, Yang Z, Yang W, Huang S, Tian L, Zhu Z, Lu Y, Xiang H, Liu S. Impact of Ambient Temperature and Relative Humidity on the Incidence of Hand-Foot-Mouth Disease in Wuhan, China. International Journal of Environmental Research and Public Health. 2020; 17(2):428. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020428
Chicago/Turabian StyleHao, Jiayuan, Zhiyi Yang, Wenwen Yang, Shuqiong Huang, Liqiao Tian, Zhongmin Zhu, Yuanan Lu, Hao Xiang, and Suyang Liu. 2020. "Impact of Ambient Temperature and Relative Humidity on the Incidence of Hand-Foot-Mouth Disease in Wuhan, China" International Journal of Environmental Research and Public Health 17, no. 2: 428. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020428