Health Literacy among People in Cardiac Rehabilitation: Associations with Participation and Health-Related Quality of Life in the Heart Skills Study in Denmark


Abstract
:1. Introduction
- Examine the associations between nine aspects of health literacy and participation in cardiac rehabilitation.
- Examine the associations between nine aspects of health literacy and physical and mental HRQoL.
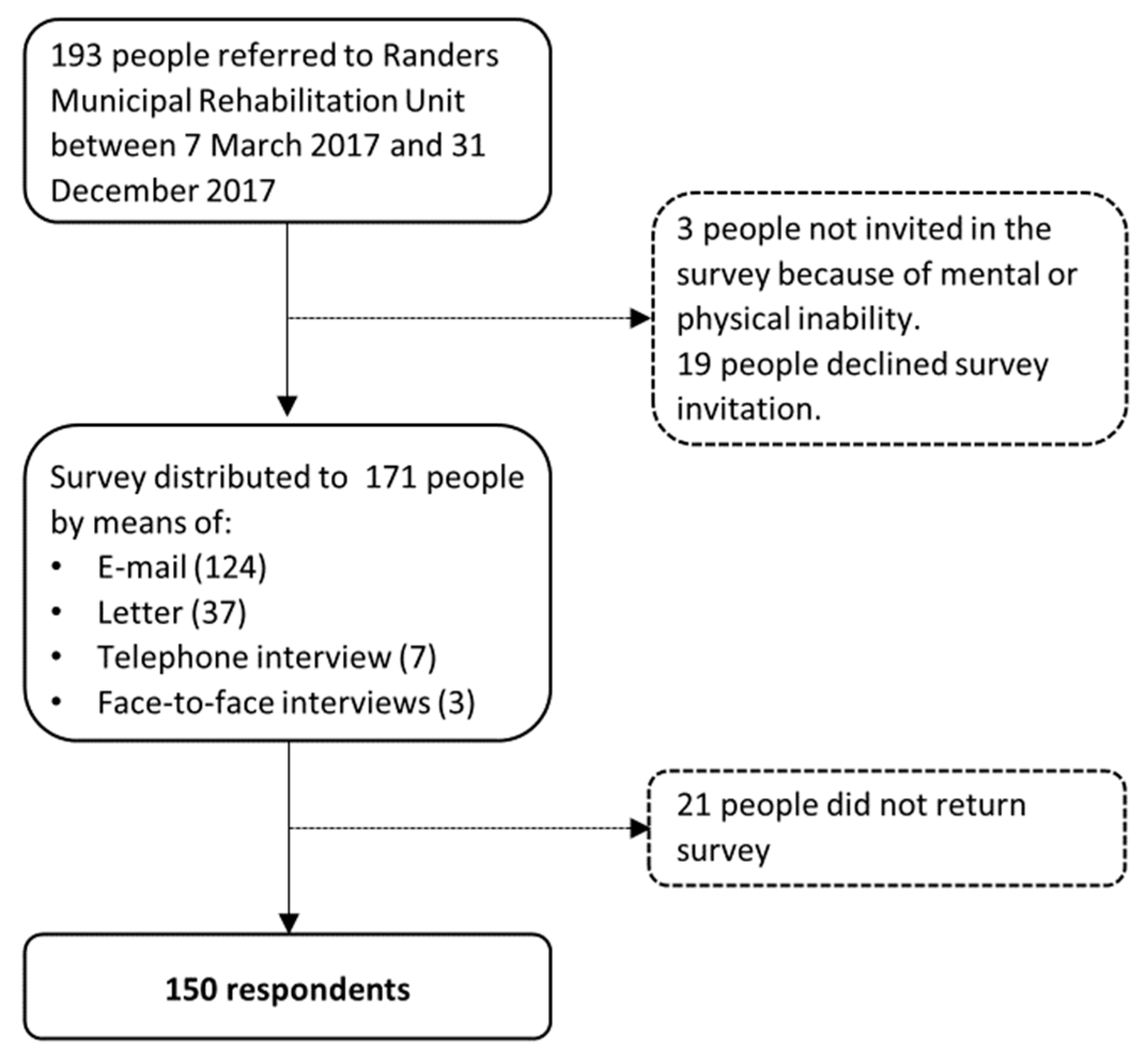
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Anderson, L.; Taylor, R.S. Cardiac Rehabilitation for People with Heart Disease: An Overview of Cochrane Systematic Reviews. Cochrane Database Syst. Rev. 2014, 1–74. [Google Scholar] [CrossRef]
- Kotseva, K.; Wood, D.; De Bacquer, D.; Jennings, C.; De Backer, G.; Ryde, L.; Gyberg, V.; Amouyel, P.; Bruthans, J.; Conde, A.C.; et al. EUROASPIRE IV: A European Society of Cardiology Survey on the Lifestyle, Risk Factor and Therapeutic Management of Coronary Patients from 24 European Countries. Eur. J. Prev. Cardiol. 2016, 23, 636–648. [Google Scholar] [CrossRef]
- Ruano-Ravina, A.; Pena-Gil, C.; Abu-Assi, E.; Raposeiras, S.; van’t Hof, A.; Meindersma, E.; Bossano Prescott, E.I.; González-Juanatey, J.R. Participation and Adherence to Cardiac Rehabilitation Programs. A Systematic Review. Int. J. Cardiol. 2016, 223, 436–443. [Google Scholar] [CrossRef]
- Karmali, K.N.; Davies, P.; Taylor, F.; Beswick, A.; Martin, N.; Ebrahim, S. Promoting Patient Uptake and Adherence in Cardiac Rehabilitation. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- International Union for Health Promotion and Education. IUHPE Position Statement on Health Literacy: A Practical Vision for a Health Literate World; IUHPE Global Working Group on Health Literacy: Paris, France, 2018. [Google Scholar]
- Nutbeam, D. Health Literacy as a Public Health Goal: A Challenge for Contemporary Health Education and Communication Strategies into the 21st Century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Kickbusch, I.; Pelikan, J.; Apfel, F.; Tsouros, A. Health Literacy: The Solid Facts; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Friis, K.; Lasgaard, M.; Rowlands, G.; Osborne, R.H.; Maindal, H.T. Health Literacy Mediates the Relationship Between Educational Attainment and Health Behavior: A Danish Population-Based Study Health Literacy Mediates the Relationship Between Educational Attainment and Health Behavior: A Danish Population-Based Study. J. Health Commun. 2016, 21, 54–60. [Google Scholar] [CrossRef]
- van der Heide, I.; Wang, J.; Droomers, M.; Spreeuwenberg, P.; Rademakers, J.; Uiters, E. The Relationship between Health, Education, and Health Literacy: Results from the Dutch Adult Literacy and Life Skills Survey. J. Health Commun. 2013, 18, 172–184. [Google Scholar] [CrossRef] [Green Version]
- Stormacq, C.; Van Den Broucke, S.; Wosinski, J. Does Health Literacy Mediate the Relationship between Socioeconomic Status and Health Disparities? Integr. Rev. 2018, 34, 1–17. [Google Scholar] [CrossRef]
- Jansen, T.; Rademakers, J.; Waverijn, G.; Verheij, R.; Osborne, R.; Heijmans, M. The Role of Health Literacy in Explaining the Association between Educational Attainment and the Use of Out-of-Hours Primary Care Services in Chronically Ill People: A Survey Study. BMC Health Serv. Res. 2018, 18, 394. [Google Scholar] [CrossRef]
- Friis, K.; Lasgaard, M.; Osborne, R.H.; Maindal, H.T. Gaps in Understanding Health and Engagement with Healthcare Providers across Common Long-Term Conditions: A Population Survey of Health Literacy in 29 473 Danish Citizens. BMJ Open 2016, 6, e009627. [Google Scholar] [CrossRef] [Green Version]
- Aaby, A.; Friis, K.; Christensen, B.; Rowlands, G.; Maindal, H.T. Health Literacy Is Associated with Health Behaviour and Self-Reported Health: A Large Population-Based Study in Individuals with Cardiovascular Disease. Eur. J. Prev. Cardiol. 2017, 24, 1880–1888. [Google Scholar] [CrossRef] [Green Version]
- Osborn, C.Y.; Paasche-Orlow, M.K.; Bailey, S.C.; Wolf, M.S. The Mechanisms Linking Health Literacy to Behavior and Health Status. Am. J. Health Behav. 2011, 35, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Cajita, M.I.; Cajita, T.R.; Han, H.-R. Health Literacy and Heart Failure: A Systematic Review. J Cardiovasc Nurs. 2016, 31, 121–130. [Google Scholar] [CrossRef] [Green Version]
- de Ghisi, G.L.M.; da Chaves, G.S.S.; Britto, R.R.; Oh, P. Health Literacy and Coronary Artery Disease: A Systematic Review. Patient Educ. Couns. 2017, 101, 177–184. [Google Scholar] [CrossRef]
- Moser, D.K.; Biddle, M.J.; Robinson, S.; Dracup, K.; Pelter, M.M.; Nesbitt, T.S.; Southard, J.; Cooper, L. Health Literacy Predicts Morbidity and Mortality in Rural Patients with Heart Failure. J. Card. Fail. 2015, 21, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Westlake, C.; Sethares, K.; Davidson, P. How Can Health Literacy Influence Outcomes in Heart Failure Patients? Mechanisms and Interventions. Curr. Heart Fail. Rep. 2013, 10, 232–243. [Google Scholar] [CrossRef]
- González-Chica, D.A.; Mnisi, Z.; Avery, J.; Duszynski, K.; Doust, J.; Tideman, P.; Murphy, A.; Burgess, J.; Beilby, J.; Stocks, N. Effect of Health Literacy on Quality of Life amongst Patients with Ischaemic Heart Disease in Australian General Practice. PLoS ONE 2016, 11, e0151079. [Google Scholar] [CrossRef]
- Tung, H.-H.; Cheng, Y.; Shih, C.-C.; Chen, L.-K.; Lee, J.-Y.; Wang, T.-J. Quality of Life among Patients with Abdominal Aortic Aneurysm Undergoing Endografting in Taiwan. Eur. J. Cardiovasc. Nurs. 2014, 13, 369–377. [Google Scholar] [CrossRef]
- Jovanić, M.; Zdravković, M.; Stanisavljević, D.; Jović Vraneš, A. Exploring the Importance of Health Literacy for the Quality of Life in Patients with Heart Failure. Int. J. Environ. Res. Public Health 2018, 15, 1761. [Google Scholar] [CrossRef] [Green Version]
- Dankner, R.; Drory, Y.; Geulayov, G.; Ziv, A.; Novikov, I.; Zlotnick, A.Y.; Moshkovitz, Y.; Elami, A.; Schwammenthal, E.; Goldbourt, U. A Controlled Intervention to Increase Participation in Cardiac Rehabilitation. Eur. J. Prev. Cardiol. 2015, 22, 1121–1128. [Google Scholar] [CrossRef]
- Mattson, C.C.; Rawson, K.; Hughes, J.W.; Waechter, D.; Rosneck, J. Health Literacy Predicts Cardiac Knowledge Gains in Cardiac Rehabilitation Participants. Health Educ. J. 2015, 74, 96–102. [Google Scholar] [CrossRef]
- Lynggaard, V.; Nielsen, C.V.; Zwisler, A.D.; Taylor, R.S.; May, O. The Patient Education—Learning and Coping Strategies—Improves Adherence in Cardiac Rehabilitation (LC-REHAB): A Randomised Controlled Trial. Int. J. Cardiol. 2017, 236, 65–70. [Google Scholar] [CrossRef]
- Knudsen, M.V.; Petersen, A.K.; Angel, S.; Hjortdal, V.E.; Maindal, H.T.; Laustsen, S. Tele-Rehabilitation and Hospital-Based Cardiac Rehabilitation Are Comparable in Increasing Patient Activation and Health Literacy: A Pilot Study. Eur. J. Cardiovasc. Nurs. 2019. [Google Scholar] [CrossRef]
- Ibrahim, S.Y.; Reid, F.; Shaw, A.; Rowlands, G.; Gomez, G.B.; Chesnokov, M.; Ussher, M. Validation of a Health Literacy Screening Tool (REALM) in a UK Population with Coronary Heart Disease. J. Public Health Bangk. 2008, 30, 449–455. [Google Scholar] [CrossRef] [Green Version]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief Questions to Identify Patients with Inadequate Health Literacy. Fam. Med. 2004, 11, 12. [Google Scholar]
- Baker, D.W.; Williams, M.V.; Parker, R.M.; Gazmararian, J.A.; Nurss, J. Development of a Brief Test to Measure Functional Health Literacy. Patient Educ. Couns. 1999, 38, 33–42. [Google Scholar] [CrossRef]
- Rowlands, G.; Khazaezadeh, N.; Oteng-Ntim, E.; Seed, P.; Barr, S.; Weiss, B.D.; Kickbusch, I.; Nutbeam, D.; Baker, D.; Parker, R.; et al. Development and Validation of a Measure of Health Literacy in the UK: The Newest Vital Sign. BMC Public Health 2013, 13, 116. [Google Scholar] [CrossRef] [Green Version]
- Region Midtjylland; de midtjydske kommuner. Forløbsprogram for Hjertesygdom [Program on Heart Disease]; Region Midtjylland & de midtjydske kommuner: Viborg, Frederiksberg C, Denmark, 2015. [Google Scholar]
- Osborne, R.H.; Batterham, R.W.; Elsworth, G.R.; Hawkins, M.; Buchbinder, R. The Grounded Psychometric Development and Initial Validation of the Health Literacy Questionnaire (HLQ). BMC Public Health 2013, 13, 658. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, A.; Buchbinder, R.; Dodson, S.; Batterham, R.W.; Elsworth, G.R.; Mcphee, C.; Sparkes, L.; Hawkins, M.; Osborne, R.H. Distribution of Health Literacy Strengths and Weaknesses across Socio-Demographic Groups: A Cross-Sectional Survey Using the Health Literacy Questionnaire (HLQ). BMC Public Health 2015, 15, 678. [Google Scholar] [CrossRef] [Green Version]
- Elsworth, G.R.; Beauchamp, A.; Osborne, R.H. Measuring Health Literacy in Community Agencies: A Bayesian Study of the Factor Structure and Measurement Invariance of the Health Literacy Questionnaire (HLQ). BMC Health Serv. Res. 2016, 16, 508. [Google Scholar] [CrossRef] [Green Version]
- Maindal, H.T.; Kayser, L.; Norgaard, O.; Bo, A.; Ellsworth, G.; Osborne, R. Cultural Adaptation and Validation of the Health Literacy Questionnaire (HLQ): Robust Nine-Dimension Danish Language Confirmatory Factor Model. Springerplus 2016, 5, 1232. [Google Scholar] [CrossRef] [Green Version]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.M.; et al. Health Literacy in Childhood and Youth: A Systematic Review of Definitions and Models. BMC Public Health 2017, 17, 361. [Google Scholar] [CrossRef]
- Rademakers, J.; Heijmans, M. Beyond Reading and Understanding: Health Literacy as the Capacity to Act. Int. J. Environ. Res. Public Health 2018, 15, 1676. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Kosinski, M.; Keller, S.D. How to Score the SF12 Physical and Mental Health Summary Scales, 2nd ed.; The Health Institute, New England Medical Center: Boston, MA, USA, 1995; Available online: https://www.researchgate.net/publication/291994160_How_to_score_SF-12_items (accessed on 1 December 2019).
- Schmidt, M.; Schmidt, S.A.J.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sørensen, H.T. The Danish National Patient Registry: A Review of Content, Data Quality, and Research Potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef] [Green Version]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a Clinical Comorbidity Index for Use with ICD-9-CM Administrative Databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities In. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Aaby, A.; Beauchamp, A.; O’Hara, J.; Maindal, H.T. Large Diversity in Danish Health Literacy Profiles: Perspectives for Care of Long-Term Illness and Multimorbidity. Eur. J. Public Health 2019. [Google Scholar] [CrossRef]
- MacAbasco-O’Connell, A.; Dewalt, D.A.; Broucksou, K.A.; Hawk, V.; Baker, D.W.; Schillinger, D.; Ruo, B.; Bibbins-Domingo, K.; Holmes, G.M.; Erman, B.; et al. Relationship between Literacy, Knowledge, Self-Care Behaviors, and Heart Failure-Related Quality of Life among Patients with Heart Failure. J. Gen. Intern. Med. 2011, 26, 979–986. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M.S.; Gazmararian, J.A.; Baker, D.W. Health Literacy and Functional Health Status among Older Adults. Arch. Intern. Med. 2005, 165, 1946–1952. [Google Scholar] [CrossRef] [Green Version]
- Tough, H.; Siegrist, J.; Fekete, C. Social Relationships, Mental Health and Wellbeing in Physical Disability: A Systematic Review. BMC Public Health 2017, 17, 414. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. “Distributed Health Literacy”: Longitudinal Qualitative Analysis of the Roles of Health Literacy Mediators and Social Networks of People Living with a Long-Term Health Condition. Health Expect. 2013, 18, 1180–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, L.; Nunes, J.A.; Taylor, P.; Silva, S. Distributed Health Literacy among People Living with Type 2 Diabetes in Portugal: Defining Levels of Awareness and Support. Heal. Soc. Care Community 2018, 26, 90–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldridge, N. Exercise-Based Cardiac Rehabilitation in Patients with Coronary Heart Disease: Meta-Analysis Outcomes Revisited. Future Cardiol. 2012, 8, 729–751. [Google Scholar] [CrossRef]
- Bakker, M.M.; Putrik, P.; Aaby, A.S.E.; Debussche, X.; Morrissey, J.; Borge, C.R.; Do, D.N.; Kolarčik, P.; Batterham, R.; Osborne, R.H.; et al. Acting Together—WHO National Health Literacy Demonstration Projects (NHLDPs) Address Health Literacy Needs in the European Region. Public Heal. Panor. 2019, 5, 233–243. [Google Scholar]
- Jessup, R.L.; Osborne, R.H.; Buchbinder, R.; Beauchamp, A. Using Co-Design to Develop Interventions to Address Health Literacy Needs in a Hospitalised Population. BMC Health Serv. Res. 2018, 18, 989. [Google Scholar] [CrossRef] [Green Version]
- Beauchamp, A.; Batterham, R.W.; Dodson, S.; Astbury, B.; Elsworth, G.R.; Mcphee, C.; Jacobson, J.; Buchbinder, R.; Osborne, R.H. Systematic Development and Implementation of Interventions to OPtimise Health Literacy and Access. BMC Public Health 2017, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Leiter, A.; Diefenbach, M.A.; Doucette, J.; Oh, W.K.; Galsky, M.D. Clinical Trial Awareness: Changes over Time and Sociodemographic Disparities. Clin Trials. 2015, 12, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Sirico, F.; Miressi, S.; Castaldo, C.; Spera, R.; Montagnani, S.; Di Meglio, F.; Nurzynska, D. Habits and Beliefs Related to Food Supplements: Results of a Survey among Italian Students of Different Education Fields and Levels. PLoS ONE 2018, 13, e0191424. [Google Scholar] [CrossRef]


{kind=link}
| HLQ Scale | Category |
|---|---|
| 2. Having sufficient information to manage my health (four questions) | Cognitive capacities |
| 5. Appraisal of health information (five questions) | |
| 9. Understand health information enough to know what to do (five questions) | |
| 8. Ability to find good health information (five questions) | Executive capacities |
| 3. Actively managing my health (five questions) | |
| 6. Ability to actively engage with healthcare providers (five questions) | |
| 7. Navigating the healthcare system (six questions) | |
| 1. Feeling understood and supported by healthcare providers (four questions) | Social capacities |
| 4. Social support for health (five questions) |
| Total Population (n = 193) | Survey Respondents (n = 150) | Survey Non-Respondents (n = 43) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Socio-Demographic Characteristics | ||||||||
| Mean age (SD) | 67.0 | (12.1) | 67.0 | (11.8) | 66.8 | (13.4) | 0.92 | |
| Gender | Male (%) | 133 | (68.9) | 107 | (71.3) | 26 | (60.5) | |
| Female (%) | 60 | (31.1) | 43 | (28.7) | 17 | (39.5) | 0.17 | |
| Country of origin | Danish origin | 273 | (96.1) | N/A | N/A | |||
| Non-Danish origin | 7 | (3.9) | N/A | N/A | ||||
| Cohabitation | Lives with someone (%) | 128 | (70.7) | 108 | (74.0) | 20 | (57.1) | |
| Lives alone (%) | 53 | (29.3) | 38 | (26.0) | 15 | (42.9) | 0.05 | |
| Educational attainment | Above 11 years (%) | 117 | (65.4) | 101 | (70.1) | 16 | (45.7) | |
| 11 years or below (%) | 62 | (34.6) | 43 | (29.9) | 29 | (54.3) | <0.05 | |
| Health-Related Characteristics | ||||||||
| Participation in rehabilitation | Participate (%) | N/A | 118 | (80.8) | N/A | |||
| Does not participate (%) | N/A | 28 | (19.2) | N/A | ||||
| Mean physical HRQoL (PCS) (SD) | N/A | 40.0 | (10.7) | N/A | ||||
| Mean mental HRQoL (MCS) (SD) | N/A | 46.2 | (11.1) | N/A | ||||
| Mean weighted Charlson Index (SD) | 1.58 | (1.4) | 1.61 | (1.4) | 1.49 | (1.2) | 0.64 | |
| Health Literacy Characteristics | ||||||||
| 2. Having sufficient information to manage my health | ||||||||
| Mean (SD) | N/A | 3.00 | (0.52) | N/A | ||||
| 5. Appraisal of health information | ||||||||
| Mean (SD) | N/A | 2.67 | (0.50) | N/A | ||||
| 9. Understand health information enough to know what to do | ||||||||
| Mean (SD) | N/A | 3.61 | (0.65) | N/A | ||||
| 8. Ability to find good health information | ||||||||
| Mean (SD) | N/A | 3.56 | (0.70) | N/A | ||||
| 3. Actively managing my health | ||||||||
| Mean (SD) | N/A | 2.92 | (0.48) | N/A | ||||
| 6. Ability to actively engage with healthcare providers | ||||||||
| Mean (SD) | N/A | 3.70 | (0.66) | N/A | ||||
| 7. Navigating the healthcare system | ||||||||
| Mean (SD) | N/A | 3.38 | (0.72) | N/A | ||||
| 1. Feeling understood and supported by healthcare providers | ||||||||
| Mean (SD) | N/A | 2.99 | (0.57) | N/A | ||||
| 4. Social support for health | ||||||||
| Mean (SD) | N/A | 3.10 | (0.52) | N/A | ||||
| Participation in Rehabilitation | ||||
|---|---|---|---|---|
| Socio-demographic characteristics | Crude | Adjusted * | ||
| OR | (95% CI) | OR | (95% CI) | |
| Age (per year) | 0.99 | (0.95;1.02) | 1.00 | (0.96;1.04) |
| Gender (ref. women) | 1.74 | (0.74;4.11) | 1.48 | (0.57;3.82) |
| Cohabitation (ref. lives alone) | 2.35 | (0.97;5.69) | 2.32 | (0.90;6.01) |
| Educational attainment (ref. ≤ 11 years) | 0.78 | (0.30;2.01) | 0.62 | (0.23;1.69) |
| Health literacy characteristics | Crude | Adjusted ** | ||
| OR | (95% CI) | OR | (95% CI) | |
| 2. Having sufficient information to manage my health | 1.23 | (0.53;2.83) | 1.39 | (0.55;3.53) |
| 5. Appraisal of health information | 1.50 | (0.61;3.71) | 1.49 | (0.56;4.01) |
| 9. Understand health information enough to know what to do | 1.19 | (0.61;2.33) | 1.47 | (0.69;3.12) |
| 8. Ability to find good health information | 1.29 | (0.70;2.38) | 1.57 | (0.77;3.21) |
| 3. Actively managing my health | 1.67 | (0.68;4.14) | 1.72 | (0.64;4.58) |
| 6. Ability to actively engage with healthcare providers | 1.33 | (0.71;2.51) | 1.36 | (0.69;2.66) |
| 7. Navigating the healthcare system | 1.24 | (0.66;2.33) | 1.51 | (0.74;3.08) |
| 1. Feeling understood and supported by healthcare providers | 1.89 | (0.85;4.18) | 1.74 | (0.74;4.07) |
| 4. Social support for health | 0.90 | (0.40;2.06) | 0.97 | (0.41;2.31) |
| Physical Health Status (PCS) | Mental Health Status (MCS) | |||||||
|---|---|---|---|---|---|---|---|---|
| Socio-Demographic Characteristics | Crude | Adjusted * | Crude | Adjusted * | ||||
| β | (95% CI) | β | (95% CI) | β | (95% CI) | β | (95% CI) | |
| Age (years) | −0.13 | (−0.29;0.03) | −0.02 | (−0.18;0.14) | 0.10 | (−0.06;0.27) | 0.13 | (−0.05;0.31) |
| Gender (ref women) | 2.54 | (−1.45;6.54) | 2.78 | (−1.34;6.90) | 1.50 | (−2.65;5.65) | 1.23 | (−3.31;5.78) |
| Cohabitation (ref single living) | 3.99 | (−0.09;8.08) | 2.68 | (−1.53;6.89) | 1.93 | (−2.38;6.24) | 1.24 | (−3.41;5.89) |
| Educational Attainment (ref ≤ 11 years) | 2.47 | (−0.48;6.43) | 1.61 | (−2.26;5.48) | −0.63 | (−4.77;3.51) | −0.50 | (−4.77;3.77) |
| Health Literacy Characteristics | Crude | Adjusted ** | Crude | Adjusted ** | ||||
| β | (95% CI) | β | (95% CI) | β | (95% CI) | β | (95% CI) | |
| 2. Having sufficient information to manage my health | 3.12 | (−0.36;6.59) | 2.56 | (−0.93;6.05) | 3.05 | (−0.55;6.66) | 2.87 | (−0.96;6.71) |
| 5. Appraisal of health information | 1.93 | (−1.63;5.49) | 1.59 | (−1.93;5.10) | 1.82 | (−1.91;5.54) | 1.23 | (−2.65;5.11) |
| 9. Understand health information enough to know what to do | 3.17 | (0.34;6.00) | 2.81 | (−0.14;5.76) | 6.06 | (3.25;8.86) | 6.61 | (3.53;9.68) |
| 8. Ability to find good health information | 2.51 | (−0.07;5.10) | 1.59 | (−1.22;4.41) | 4.38 | (1.76;6.99) | 4.63 | (1.63;7.64) |
| 3. Actively managing my health | 2.79 | (−0.98;6.55) | 3.04 | (−0.63;6.71) | 3.36 | (−0.54;7.25) | 2.72 | (−0.33;6.77) |
| 6. Ability to actively engage with healthcare providers | 3.90 | (1.25;6.55) | 3.53 | (0.88;6.18) | 7.29 | (4.75;9.84) | 7.10 | (4.36;9.83) |
| 7. Navigating the healthcare system | 3.34 | (0.88;5.80) | 2.79 | (0.12;5.46) | 4.93 | (2.45;7.40) | 4.83 | (2.00;7.66) |
| 1. Feeling understood and supported by healthcare providers | 0.70 | (−2.40;3.81) | 0.42 | (−2.66;3.50) | 1.70 | (−1.51;4.91) | 0.96 | (−2.42;4.35) |
| 4. Social support for health | 1.92 | (−1.59;5.42) | 1.13 | (−2.43;4.70) | 9.31 | (6.00;12.62) | 9.64 | (6.09;13.18) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aaby, A.; Friis, K.; Christensen, B.; Maindal, H.T. Health Literacy among People in Cardiac Rehabilitation: Associations with Participation and Health-Related Quality of Life in the Heart Skills Study in Denmark. Int. J. Environ. Res. Public Health 2020, 17, 443. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020443
Aaby A, Friis K, Christensen B, Maindal HT. Health Literacy among People in Cardiac Rehabilitation: Associations with Participation and Health-Related Quality of Life in the Heart Skills Study in Denmark. International Journal of Environmental Research and Public Health. 2020; 17(2):443. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020443
Chicago/Turabian StyleAaby, Anna, Karina Friis, Bo Christensen, and Helle Terkildsen Maindal. 2020. "Health Literacy among People in Cardiac Rehabilitation: Associations with Participation and Health-Related Quality of Life in the Heart Skills Study in Denmark" International Journal of Environmental Research and Public Health 17, no. 2: 443. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020443