Study Protocol for the Evaluation of “SuperFIT”, a Multicomponent Nutrition and Physical Activity Intervention Approach for Preschools and Families

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
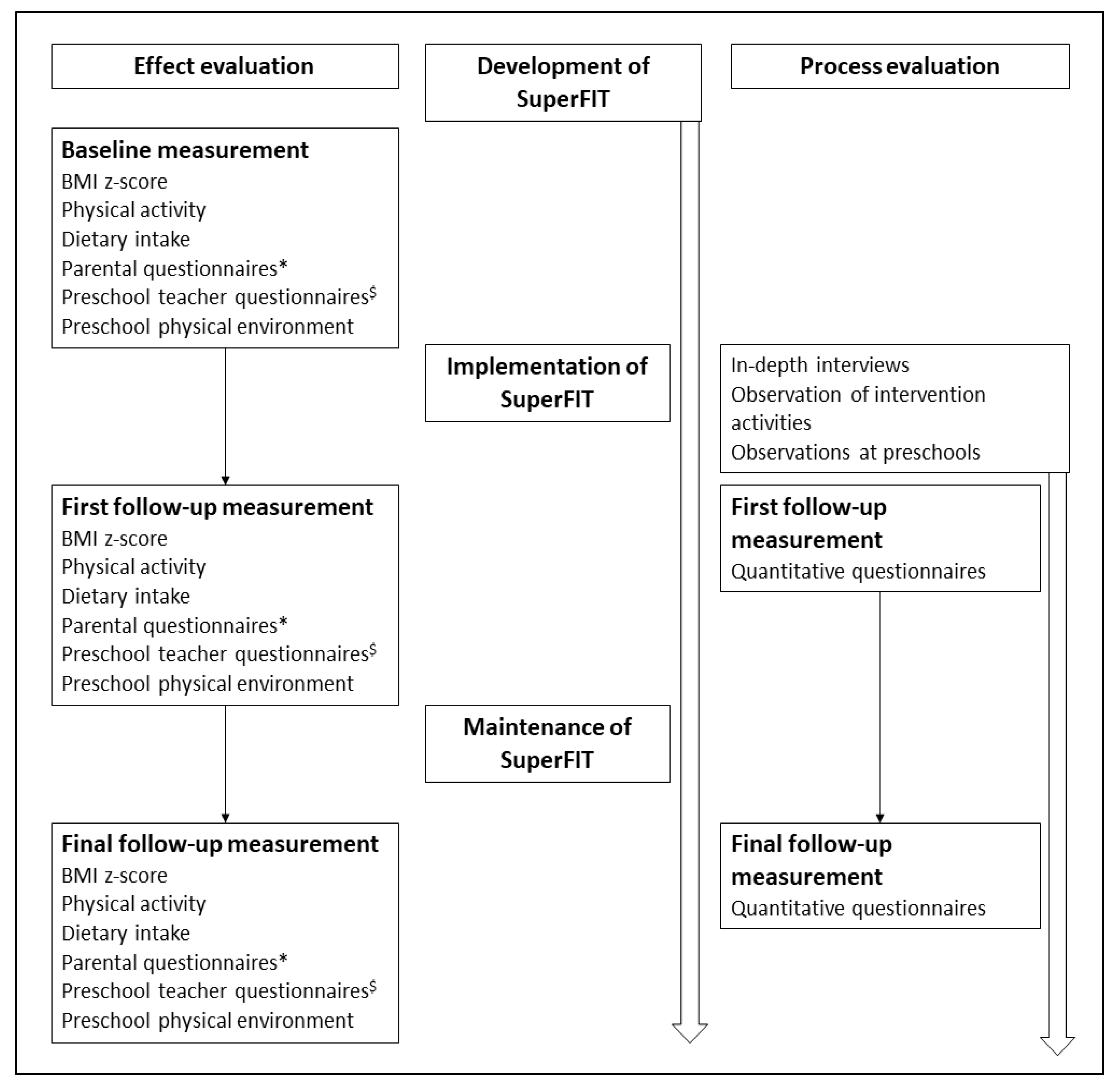
2.1. Study Design
2.2. Study Setting
2.3. The Intervention
2.3.1. Preschool-Based Component
2.3.2. Family-Based Component
2.3.3. Community Component
2.4. Planning
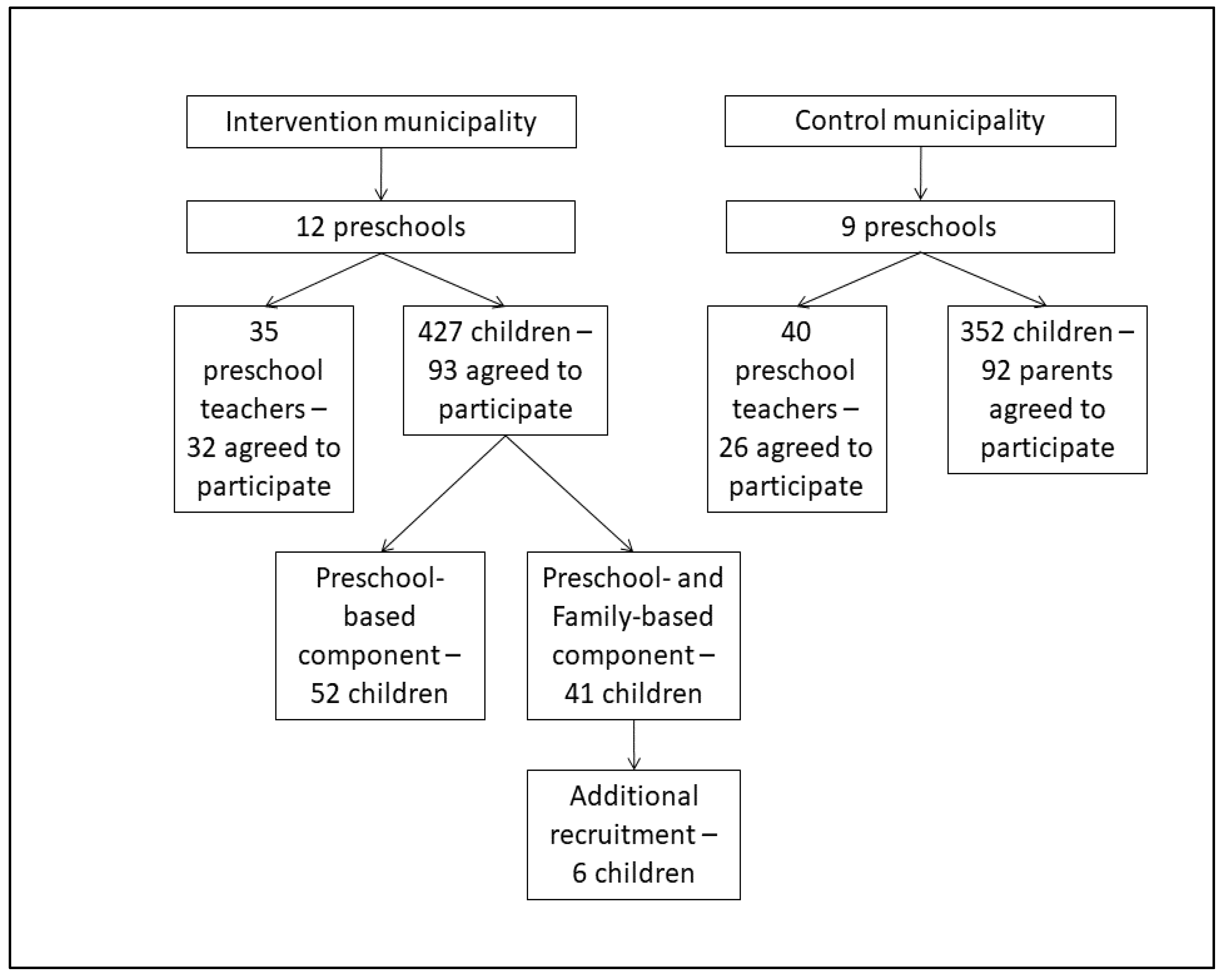
2.5. Participants
3. Data Collection
3.1. Effect Evaluation
3.1.1. BMI z-Score
3.1.2. Dietary Intake
3.1.3. Physical Activity and Sedentary Behaviour
3.1.4. Questionnaires
3.1.5. Preschool Physical Environment
3.2. Process Evaluation
3.3. Data Analysis
3.4. Sample Size
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Organisation for Economic Co-operation and Development. Obesity Update 2017. 2017. Available online: https://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf (accessed on 11 December 2018).
- Schonbeck, Y.; Talma, H.; van Dommelen, P.; Bakker, B.; Buitendijk, S.E.; Hirasing, R.A.; van Buuren, S. Increase in prevalence of overweight in Dutch children and adolescents: A comparison of nationwide growth studies in 1980, 1997 and 2009. PLoS ONE 2011, 6. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef]
- De Kroon, M.L.A.; Renders, C.M.; Van Wouwe, J.P.; Van Buuren, S.; Hirasing, R.A. The Terneuzen Birth Cohort: BMI Changes between 2 and 6 Years Correlate Strongest with Adult Overweight. PLoS ONE 2010, 5, e9155. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.R. Complications of obesity in children and adolescents. Int. J. Obes. 2009, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Rennie, K.L.; Johnson, L.; Jebb, S.A. Behavioural determinants of obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Monasta, L.; Batty, G.D.; Cattaneo, A.; Lutje, V.; Ronfani, L.; Van Lenthe, F.J.; Brug, J. Early-life determinants of overweight and obesity: A review of systematic reviews. Obes. Rev. 2010, 11, 695–708. [Google Scholar] [CrossRef] [PubMed]
- van Lenthe, F.J.; Mackenbach, J.P. Neighbourhood deprivation and overweight: The GLOBE study. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Goldfield, G.S.; Harvey, A.; Grattan, K.; Adamo, K.B. Physical activity promotion in the preschool years: A critical period to intervene. Int. J. Environ. Res. Public Health 2012, 9, 1326–1342. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Essentail Nutrition Actions: Mainstreaming Nutrition Throught the Life-Course; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Gubbels, J.S.; Kremers, S.P.; Goldbohm, R.A.; Stafleu, A.; Thijs, C. Energy balance-related behavioural patterns in 5-year-old children and the longitudinal association with weight status development in early childhood. Public Health Nutr. 2012, 15, 1402–1410. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Dagnelie, P.C.; de Vries, S.I.; de Vries, N.K.; Thijs, C. Clustering of dietary intake and sedentary behavior in 2-year-old children. J. Pediatr. 2009, 155, 194–198. [Google Scholar] [CrossRef]
- Berglind, D.; Tynelius, P. Objectively measured physical activity patterns, sedentary time and parent-reported screen-time across the day in four-year-old Swedish children. BMC Public Health 2017, 18, 69. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Van Kann, D.H.H.; Cardon, G.; Kremers, S.P.J. Activating Childcare Environments for All Children: The Importance of Children’s Individual Needs. Int. J. Environ. Res. Public Health 2018, 15, 1400. [Google Scholar] [CrossRef] [Green Version]
- Hinkley, T.; Salmon, J.; Okely, A.D.; Crawford, D.; Hesketh, K. Preschoolers’ physical activity, screen time, and compliance with recommendations. Med. Sci. Sports Exerc. 2012, 44, 458–465. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Raaijmakers, L.G.; Gerards, S.M.; Kremers, S.P. Dietary intake by Dutch 1- to 3-year-old children at childcare and at home. Nutrients 2014, 6, 304–318. [Google Scholar] [CrossRef] [Green Version]
- Pitt, E.; Cameron, C.M.; Thornton, L.; Gallegos, D.; Filus, A.; Ng, S.K.; Comans, T. Dietary patterns of Australian children at three and five years of age and their changes over time: A latent class and latent transition analysis. Appetite 2018, 129, 207–216. [Google Scholar] [CrossRef]
- Centraal Bureau voor de Statistiek Kinderen Eten te Weinig Fruit, Groente en Vis (Children Eat Too Little Fruit, Vegetables and Fish). Available online: https://www.cbs.nl/nl-nl/nieuws/2017/46/kinderen-eten-te-weinig-fruit-groente-en-vis (accessed on 3 May 2018).
- Sluik, D.; van Lee, L.; Engelen, A.I.; Feskens, E.J. Total, Free, and Added Sugar Consumption and Adherence to Guidelines: The Dutch National Food Consumption Survey 2007–2010. Nutrients 2016, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Banfield, E.C.; Liu, Y.; Davis, J.S.; Chang, S.; Frazier-Wood, A.C. Poor Adherence to US Dietary Guidelines for Children and Adolescents in the National Health and Nutrition Examination Survey Population. J. Acad. Nutr. Diet. 2016, 116, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spence, J.C.; Lee, R.E. Toward a comprehensive model of physical activity. Psychol. Sport Exerc. 2003, 4, 7–24. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development, PF3.2: Enrolment in Childcare and Pre-School. Available online: http://www.oecd.org/els/soc/PF3_2_Enrolment_childcare_preschool.pdf (accessed on 28 June 2018).
- Alberdi, G.; McNamara, A.E.; Lindsay, K.L.; Scully, H.A.; Horan, M.H.; Gibney, E.R.; McAuliffe, F.M. The association between childcare and risk of childhood overweight and obesity in children aged 5 years and under: A systematic review. Eur. J. Pediatr. 2016, 175, 1277–1294. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Dagnelie, P.C.; de Vries, N.K.; Thijs, C. Child-care environment and dietary intake of 2- and 3-year-old children. J. Hum. Nutr. Diet. 2010, 23, 97–101. [Google Scholar] [CrossRef]
- Labarque, V.; Gubbels, J.S.; Cardon, G. Preschooler’s physical activity levels and associations with lesson context, teacher’s behavior, and environment during preschool physical education. Early Child. Res. Q. 2012, 27, 221–230. [Google Scholar]
- van Zandvoort, M.; Tucker, P.; Irwin, J.D.; Burke, S.M. Physical activity at daycare: Issues, challenges and perspectives. J. Early Years 2010, 30, 175–188. [Google Scholar] [CrossRef]
- Bradley, R.H. From Home to Day Care: Chaos in the Family/Child-Care Mesosystem. In Chaos and Its Influence on Children’s Development. An Ecological Perspective; Evans, G.W., Wachs, T.D., Eds.; American Psychological Association: Washington, WA, USA, 2010. [Google Scholar]
- Gubbels, J.S.; Van Kann, D.H.; de Vries, N.K.; Thijs, C.; Kremers, S.P. The next step in health behavior research: The need for ecological moderation analyses–An application to diet and physical activity at childcare. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, J.; Robbins, L.B.; Wen, F. Interventions to prevent and manage overweight or obesity in preschool children: A systematic review. Int. J. Nurs. Stud. 2016, 53, 270–289. [Google Scholar] [CrossRef]
- Sisson, S.B.; Krampe, M.; Anundson, K.; Castle, S. Obesity prevention and obesogenic behavior interventions in child care: A systematic review. Prev. Med. 2016, 87, 57–69. [Google Scholar] [CrossRef]
- Temple, M.; Robinson, J.C. A systematic review of interventions to promote physical activity in the preschool setting. J. Spec. Pediatr. Nurs. 2014, 19, 274–284. [Google Scholar] [CrossRef]
- Ward, D.S.; Welker, E.; Choate, A.; Henderson, K.E.; Lott, M.; Tovar, A.; Wilson, A.; Sallis, J.F. Strength of obesity prevention interventions in early care and education settings: A systematic review. Prev. Med. 2017, 95, S37–S52. [Google Scholar] [CrossRef]
- Black, A.P.; D’Onise, K.; McDermott, R.; Vally, H.; O’Dea, K. How effective are family-based and institutional nutrition interventions in improving children’s diet and health? A systematic review. BMC Public Health 2017, 17, 818. [Google Scholar] [CrossRef] [Green Version]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.; van Sluijs, E.M. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis and realist synthesis. Obes. Rev. 2016, 17, 345–360. [Google Scholar] [CrossRef] [Green Version]
- Hingle, M.D.; O’Connor, T.M.; Dave, J.M.; Baranowski, T. Parental involvement in interventions to improve child dietary intake: A systematic review. Prev. Med. 2010, 51, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Ling, J.; Robbins, L.B.; Wen, F.; Zhang, N. Lifestyle Interventions in Preschool Children: A Meta-analysis of Effectiveness. Am. J. Prev. Med. 2017, 53, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Segal, J.; Wu, Y.; Wilson, R.; Wang, Y. Systematic review of community-based childhood obesity prevention studies. Pediatrics 2013, 132, e201–e210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Ren, H.; Yin, Z.; Wang, L.; Wang, K. A policy-driven multifaceted approach for early childhood physical fitness promotion: Impacts on body composition and physical fitness in young Chinese children. BMC Pediatr. 2014, 14, 118. [Google Scholar] [CrossRef] [Green Version]
- Peterson, K.E.; Fox, M.K. Addressing the Epidemic of Childhood Obesity through School-Based Interventions: What Has Been Done and Where Do We Go from Here? J. Law Med. Ethics 2007, 35, 113–130. [Google Scholar] [CrossRef]
- Kremers, S.P.J.; de Bruijn, G.J.; Visscher, T.L.; van Mechelen, W.; de Vries, N.K.; Brug, J. Environmental influences on energy balance-related behaviors: A dual-process view. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Dagnelie, P.C.; Goldbohm, R.A.; de Vries, N.K.; Thijs, C. Diet-related restrictive parenting practices. Impact on dietary intake of 2-year-old children and interactions with child characteristics. Appetite 2009, 52, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Sleddens, E.F.; Gerards, S.M.; Thijs, C.; de Vries, N.K.; Kremers, S.P. General parenting, childhood overweight and obesity-inducing behaviors: A review. Int. J. Pediatr. Obes. 2011, 6, e12–e27. [Google Scholar] [CrossRef]
- Ward, S.; Belanger, M.; Donovan, D.; Carrier, N. Systematic review of the relationship between childcare educators’ practices and preschoolers’ physical activity and eating behaviours. Obes. Rev. 2015, 16, 1055–1070. [Google Scholar] [CrossRef] [Green Version]
- Anzman-Frasca, S.; Savage, J.S.; Marini, M.E.; Fisher, J.O.; Birch, L.L. Repeated exposure and associative conditioning promote preschool children’s liking of vegetables. Appetite 2012, 58, 543–553. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Van Kann, D.H.; Jansen, M.W. Play equipment, physical activity opportunities, and children’s activity levels at childcare. J. Environ. Public Health 2012, 2012. [Google Scholar] [CrossRef]
- Mazarello Paes, V.; Ong, K.K.; Lakshman, R. Factors influencing obesogenic dietary intake in young children (0–6 years): Systematic review of qualitative evidence. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Kolk, I.; Goossens, A.J.M.; Gerards, S.; Kremers, S.P.J.; Manders, R.M.P.; Gubbels, J.S. Healthy Nutrition and Physical Activity in Childcare: Views from Childcare Managers, Childcare Workers and Parents on Influential Factors. Int. J. Environ. Res. Public Health 2018, 15, 2909. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.; Ward, D.S.; Neelon, S.B.; Story, M. What Role Can Child-Care Settings Play in Obesity Prevention? A Review of the Evidence and Call for Research Efforts. J. Am. Diet. Assoc. 2011, 111, 1343–1362. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Klesges, L.M.; Dzewaltowski, D.A.; Estabrooks, P.A.; Vogt, T.M. Evaluating the impact of health promotion programs: Using the RE-AIM framework to form summary measures for decision making involving complex issues. Health Educ. Res. 2006, 21, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Government of The Netherlands. Welke Soorten kinderopvang zijn er? Available online: https://www.rijksoverheid.nl/onderwerpen/kinderopvang/vraag-en-antwoord/soorten-kinderopvang (accessed on 16 August 2017).
- Tax and Customs administration. Kinderopvangtoeslag (Childcare benefit). Available online: https://www.belastingdienst.nl/wps/wcm/connect/bldcontentnl/belastingdienst/prive/toeslagen/kinderopvangtoeslag/kinderopvangtoeslag-2019/kinderopvangtoeslag-2019 (accessed on 10 December 2018).
- van Kampen, A.; Kloprogge, J.; Rutten, S.; Schonewille, B. Voor-en Vroegschoolse Zorg en Educatie. Available online: https://zoek.officielebekendmakingen.nl/kst-30300-VIII-214-b1.pdf (accessed on 2 November 2016).
- Roeters, A.; Bucx, F. Kijk op Kinderopvang; Sociaal en Cultureel Planbureau: The Hague, The Netherlands, 2018. [Google Scholar]
- Van Stan, S.; Lessard, L.; Dupont Phillips, K. The impact of a statewide training to increase child care providers’ knowledge of nutrition and physical activity rules in Delaware. Child. Obes. 2013, 9, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Reinke, W.M.; Stormont, M.; Herman, K.C.; Newcomer, L. Using Coaching to Support Teacher Implementation of Classroom-based Interventions. J. Behav. Edu. 2014, 23, 150–167. [Google Scholar] [CrossRef]
- Tucker, P.; Vanderloo, L.M.; Johnson, A.M.; Burke, S.M.; Irwin, J.D.; Gaston, A.; Driediger, M.; Timmons, B.W. Impact of the Supporting Physical Activity in the Childcare Environment (SPACE) intervention on preschoolers’ physical activity levels and sedentary time: A single-blind cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 120. [Google Scholar] [CrossRef] [Green Version]
- Caton, S.J.; Ahern, S.M.; Remy, E.; Nicklaus, S.; Blundell, P.; Hetherington, M.M. Repetition counts: Repeated exposure increases intake of a novel vegetable in UK pre-school children compared to flavour-flavour and flavour-nutrient learning. Br. J. Nutr. 2013, 109, 2089–2097. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, J.A. The Lifestyle Triple P Multilevel System of Parenting and Family Support for the Prevention and Treatment of Childhood Obesity; The University of Queensland: Queensland, Australia, 2016. [Google Scholar]
- The Netherlands Institute for Social Research. SCP Statusscores 2014. Available online: http://www.scp.nl/Formulieren/Statusscores_opvragen (accessed on 2 July 2019).
- Van Cauwenberghe, E.; Gubbels, J.; De Bourdeaudhuij, I.; Cardon, G. Feasibility and validity of accelerometer measurements to assess physical activity in toddlers. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gubbels, J.S.; Sleddens, E.F.; Raaijmakers, L.C.; Gies, J.M.; Kremers, S.P. The Child-care Food and Activity Practices Questionnaire (CFAPQ): Development and first validation steps. Public Health Nutr. 2015, 19, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, T.M.; Cerin, E.; Hughes, S.O.; Robles, J.; Thompson, D.I.; Mendoza, J.A.; Baranowski, T.; Lee, R.E. Psychometrics of the preschooler physical activity parenting practices instrument among a Latino sample. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musher-Eizenman, D.; Holub, S. Comprehensive Feeding Practices Questionnaire: Validation of a new measure of parental feeding practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef] [PubMed]
- Niermann, C.; Krapf, F.; Renner, B.; Reiner, M.; Woll, A. Family health climate scale (FHC-scale): Development and validation. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Ward, D.S.; Mazzucca, S.; McWilliams, C.; Hales, D. Use of the Environment and Policy Evaluation and Observation as a Self-Report Instrument (EPAO-SR) to measure nutrition and physical activity environments in child care settings: Validity and reliability evidence. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 124. [Google Scholar] [CrossRef] [Green Version]
- Ball, S.; Benjamin, S.; Hales, D.; Marks, J.; McWilliams, C.; Ward, D. The Environment and Policy Assessment and Observation (EPAO) Child Care Nutrition and Physical Activity Instrument; Center for Health Promotion and Disease Prevention, University of North Carolina at Chapel Hill: Chapel Hill, NC, USA, 2005. [Google Scholar]
- Waters, E.; de Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 7. [Google Scholar] [CrossRef]
- Baranowski, T.; Davis, M.; Resnicow, K.; Baranowski, J.; Doyle, C.; Lin, L.S.; Smith, M.; Wang, D.T. Gimme 5 fruit, juice, and vegetables for fun and health: Outcome evaluation. Health Educ. Behav. 2000, 27, 96–111. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Stessen, K.; van de Kolk, I.; de Vries, N.K.; Thijs, C.; Kremers, S.P.J. Energy balance-related parenting and child-care practices: The importance of meso-system consistency. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [Green Version]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef]
- Hanson, S.; Jones, A. Missed opportunities in the evaluation of public health interventions: A case study of physical activity programmes. BMC Public Health 2017, 17, 674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiltsey Stirman, S.; Kimberly, J.; Cook, N.; Calloway, A.; Castro, F.; Charns, M. The sustainability of new programs and innovations: A review of the empirical literature and recommendations for future research. Implement. Sci. 2012, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawe, P.; Shiell, A.; Riley, T.; Gold, L. Methods for exploring implementation variation and local context within a cluster randomised community intervention trial. J. Epidemiol. Community Health 2004, 58, 788–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremers, S.P.J.; Visscher, T.L.S.; Schuit, A.J. Effect in zijn context. Tijdschrift voor gezondheidswetenschappen 2018, 96, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Evans, R.E.; Hawkins, J.; Littlecott, H.; Melendez-Torres, G.J.; Bonell, C.; Murphy, S. From complex social interventions to interventions in complex social systems: Future directions and unresolved questions for intervention development and evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef] [Green Version]
- Green, L.W. Evaluation and measurement: Some dilemmas for health education. Am. J. Public Health 1977, 67, 155–161. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Kolk, I.; Gerards, S.M.P.L.; Harms, L.S.E.; Kremers, S.P.J.; van Dinther-Erkens, A.M.H.S.; Snellings, M.; Gubbels, J.S. Study Protocol for the Evaluation of “SuperFIT”, a Multicomponent Nutrition and Physical Activity Intervention Approach for Preschools and Families. Int. J. Environ. Res. Public Health 2020, 17, 603. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020603
van de Kolk I, Gerards SMPL, Harms LSE, Kremers SPJ, van Dinther-Erkens AMHS, Snellings M, Gubbels JS. Study Protocol for the Evaluation of “SuperFIT”, a Multicomponent Nutrition and Physical Activity Intervention Approach for Preschools and Families. International Journal of Environmental Research and Public Health. 2020; 17(2):603. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020603
Chicago/Turabian Stylevan de Kolk, Ilona, Sanne M. P. L. Gerards, Lisa S. E. Harms, Stef P. J. Kremers, Angela M. H. S. van Dinther-Erkens, Monique Snellings, and Jessica S. Gubbels. 2020. "Study Protocol for the Evaluation of “SuperFIT”, a Multicomponent Nutrition and Physical Activity Intervention Approach for Preschools and Families" International Journal of Environmental Research and Public Health 17, no. 2: 603. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17020603