Adolescent Tobacco Exposure in 31 Latin American Cities before and after the Framework Convention for Tobacco Control

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Policy Indicators: The MPOWER Framework
2.2. Policy Data
2.3. Youth Tobacco Survey
2.3.1. Transformation of Youth Survey Data into MPOWER
2.3.2. Survey Data Analysis
3. Results
3.1. Changes in Tobacco Control Policies at the Country Level
3.2. Youth Tobacco Surveys at the City-Level (GYTS)
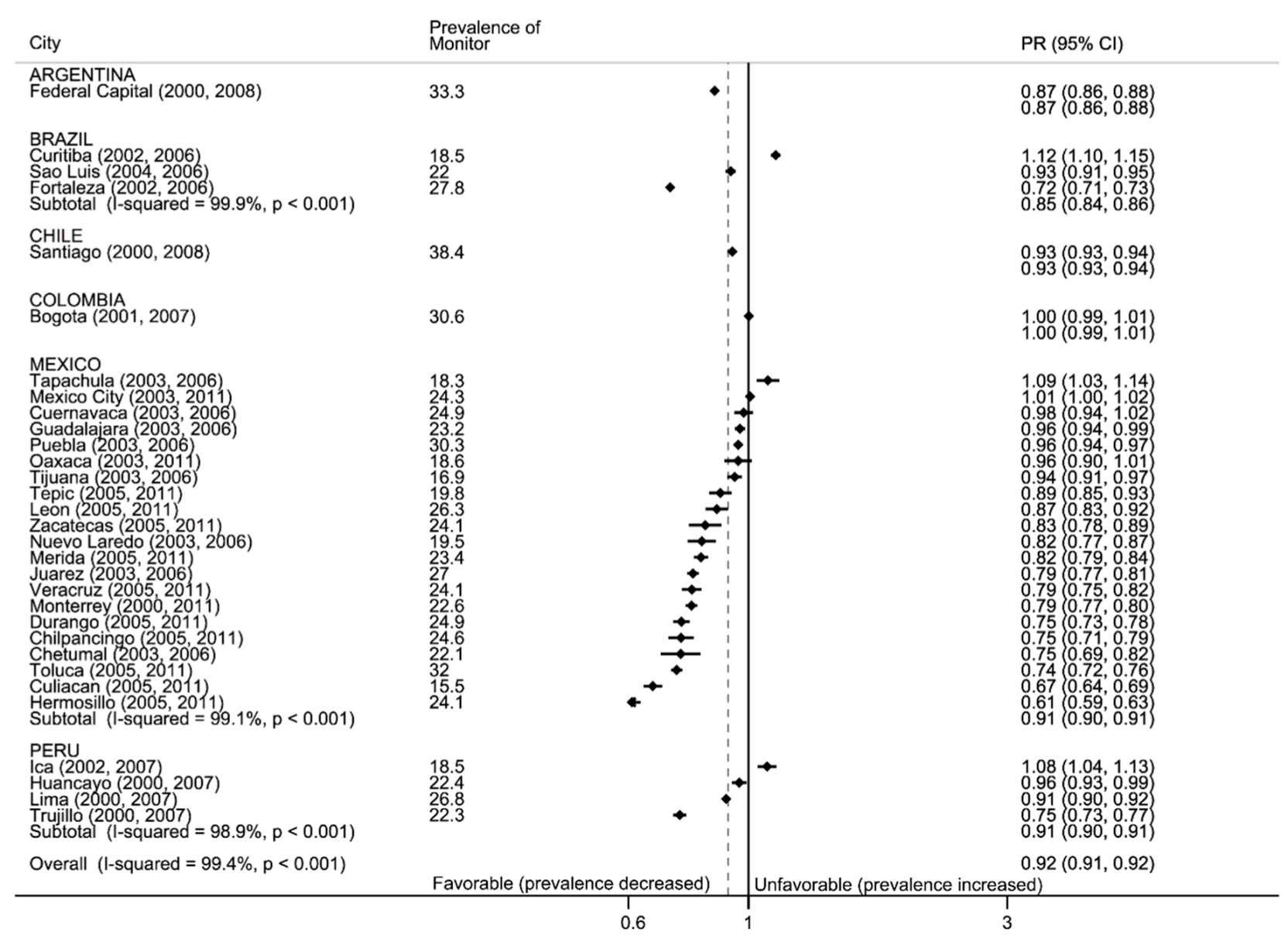
3.2.1. Monitor: Tobacco Use
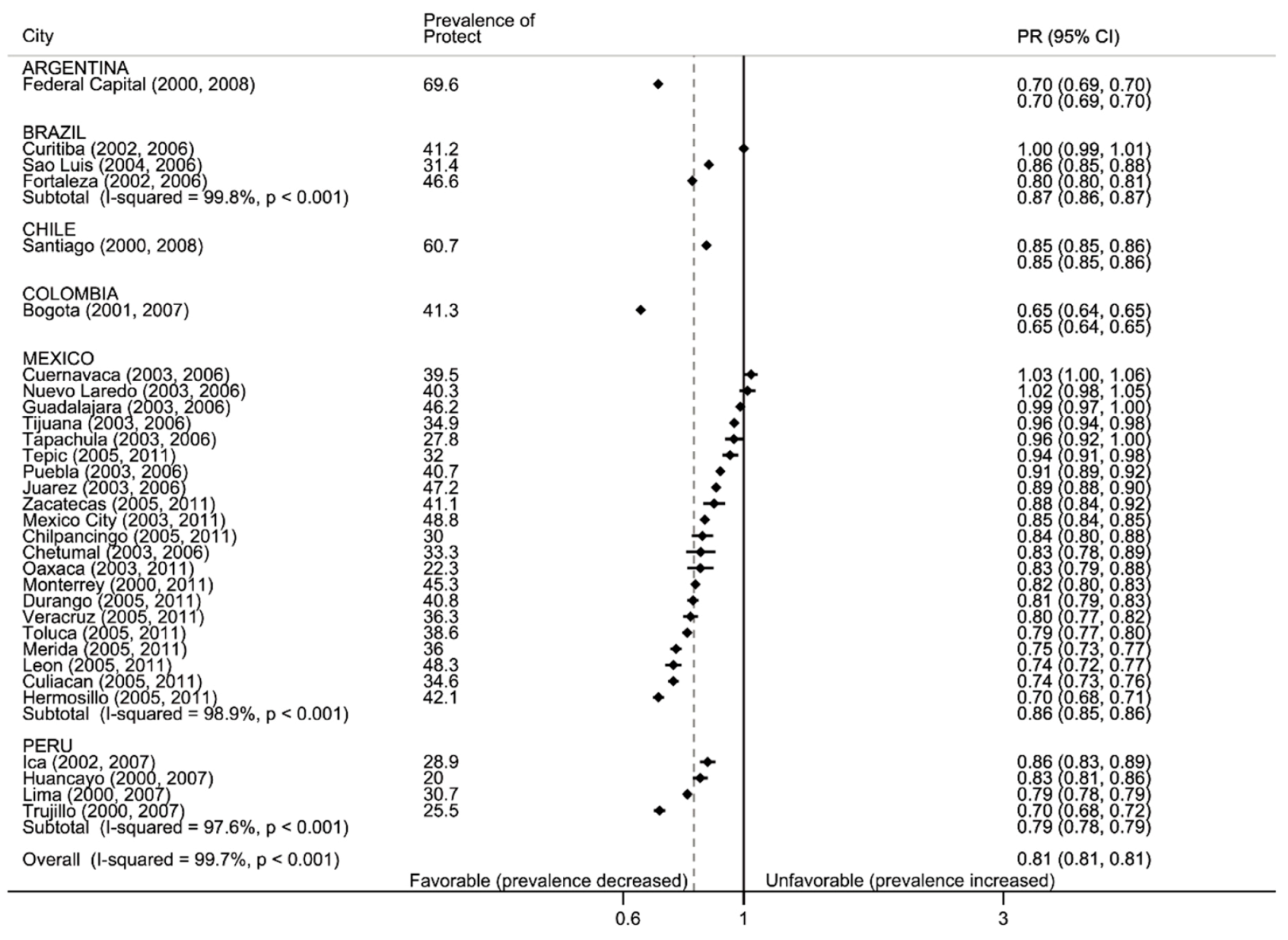
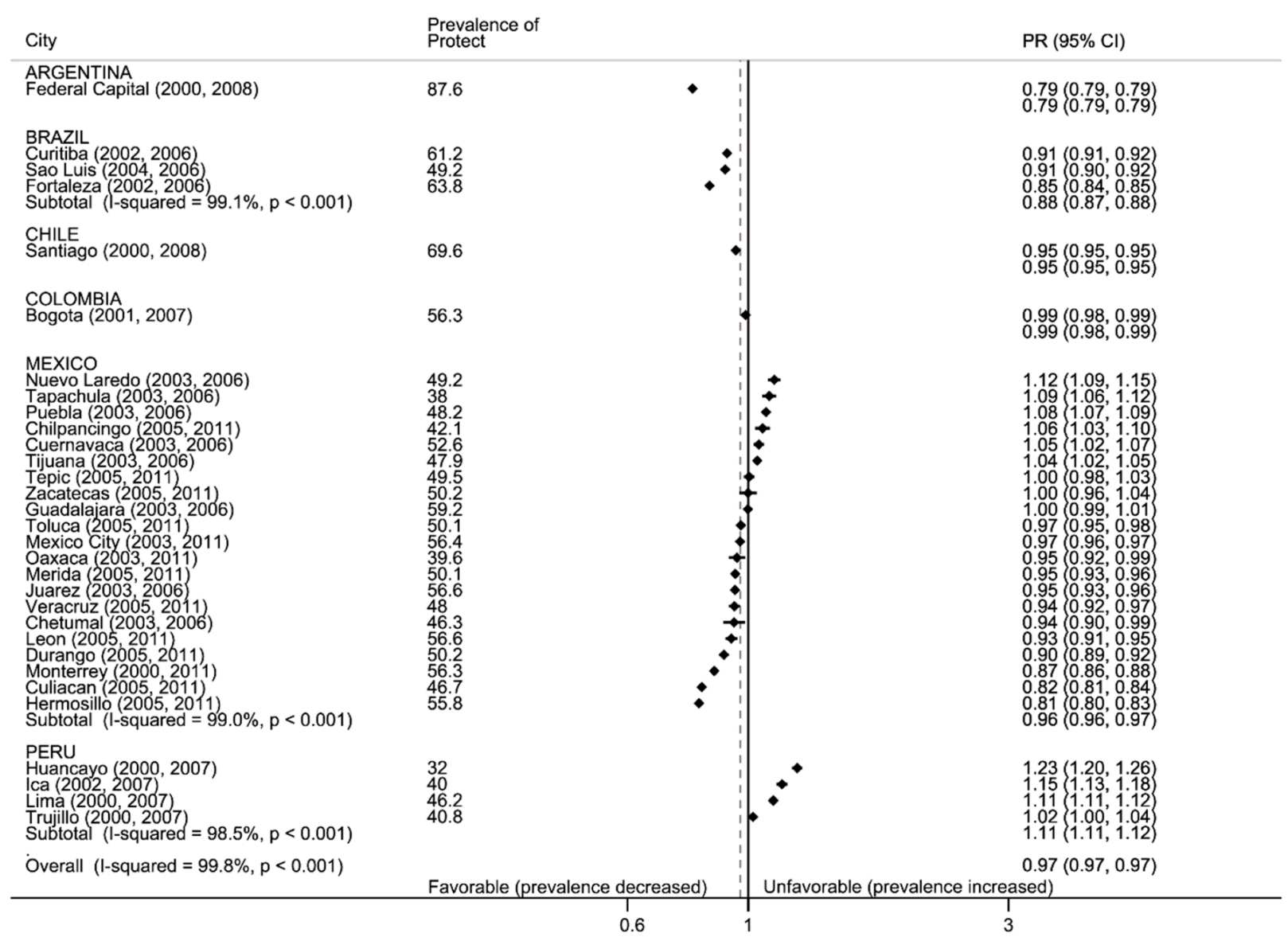
3.2.2. Protect: Secondhand Smoke
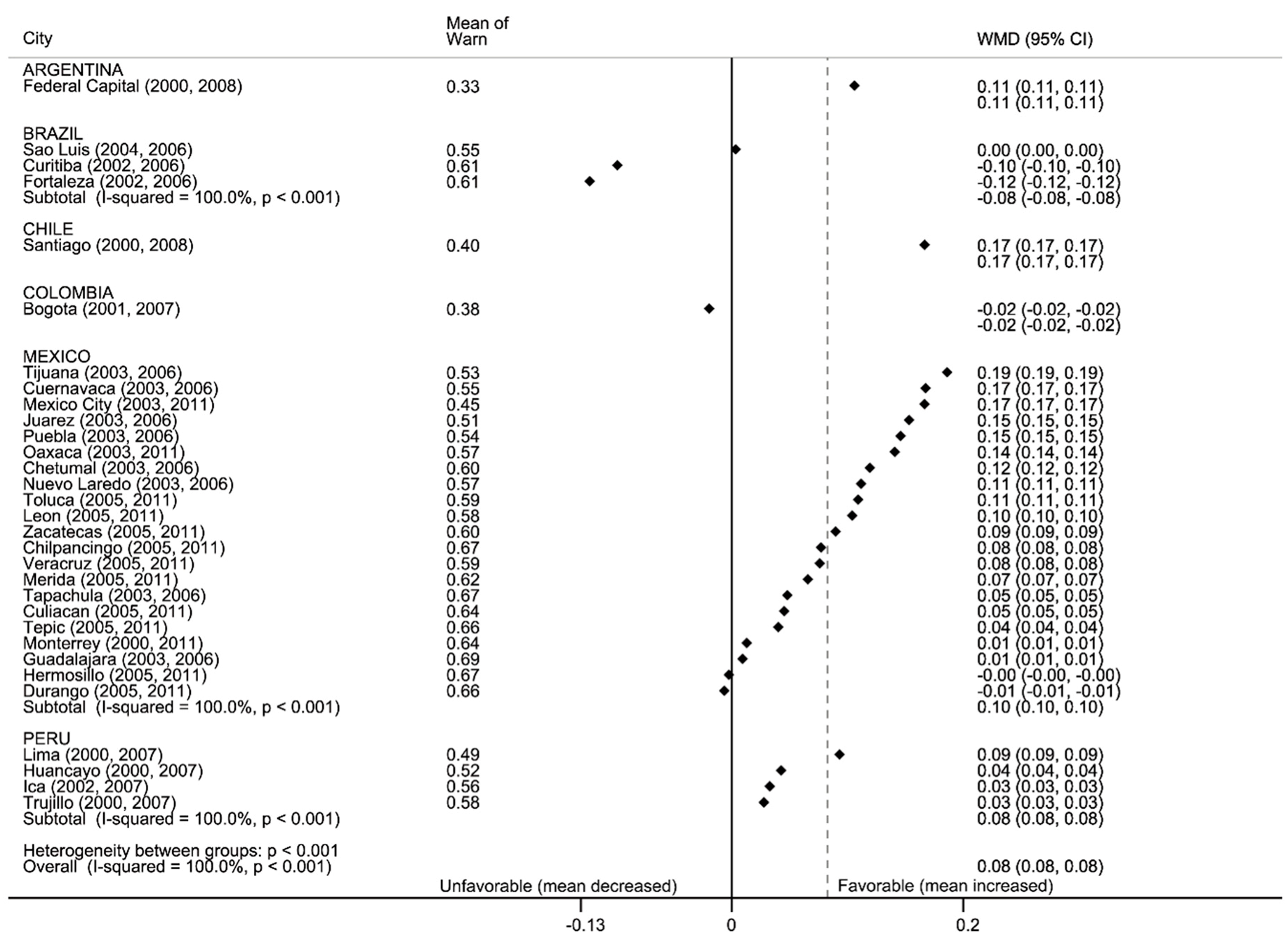
3.2.3. Warn: Education against Tobacco
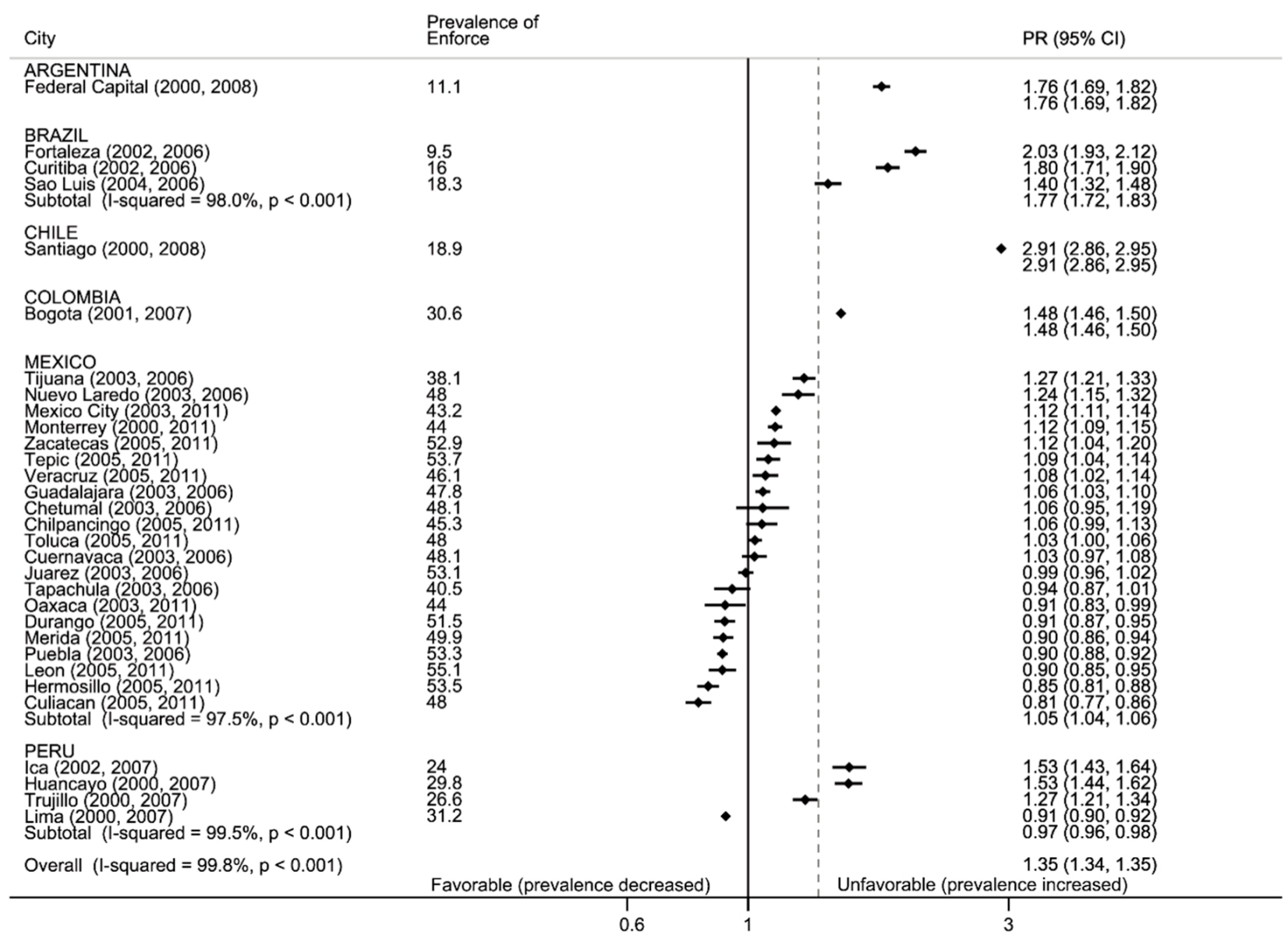
3.2.4. Enforce: Media and Advertising, Refusal to Sell and Free Cigarettes and Offering Free Cigarettes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2003; Available online: http://www.who.int/fctc/text_download/en/ (accessed on 19 July 2020).
- WHO. World Health Statistics: Monitoring Health for the SDGs; World Health Organization: Villars-sous-Yens/Geneva, Switzerland, 2017; Available online: https://www.who.int/gho/publications/world_health_statistics/2017/en/ (accessed on 19 July 2020).
- Cummings, K.M.; Sebrie, E.M. Latin America: A laboratory for tobacco control research. Salud Publica Mex. 2010, 52 (Suppl. 2), S91–S93. [Google Scholar] [CrossRef] [Green Version]
- Valente, T.W.; Dyal, S.R.; Chu, K.H.; Wipfli, H.; Fujimoto, K. Diffusion of innovations theory applied to global tobacco control treaty ratification. Soc. Sci. Med. 2015, 145, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, E.; Sonneland, H.K. Weekly Chart: Tobacco Use in Latin America. Report Americas Society Council of the Americas May 29 2015; Americas Society (AS) & Council of the Americas (COA): New York, NY, USA, 2015; Available online: https://www.as-coa.org/articles/weekly-chart-tobacco-use-latin-america (accessed on 4 July 2020).
- De Maio, F.G.; Konfino, J.; Ondarsuhu, D.; Goldberg, L.; Linetzky, B.; Ferrante, D. Sex-stratified and age-adjusted social gradients in tobacco in Argentina and Uruguay: Evidence from the Global Adult Tobacco Survey (GATS). Tob. Control 2015, 24, 562–567. [Google Scholar] [CrossRef] [Green Version]
- Champagne, B.M.; Sebrie, E.M.; Schargrodsky, H.; Pramparo, P.; Boissonnet, C.; Wilson, E. Tobacco smoking in seven Latin American cities: The CARMELA study. Tob. Control 2010, 19, 457–462. [Google Scholar] [CrossRef] [Green Version]
- IOM; Bonnie, R.J.; Stratton, K.; Kwan, L.Y. Public Health Implications of Raising the Minimum Age of Legal Access to Tobacco Products; National Academies Press: Washington, DC, USA, 23 July 2015. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK310407/#_ncbi_dlg_citbx_NBK310407 (accessed on 10 June 2020).
- Sebrie, E.M.; Schoj, V.; Travers, M.J.; McGaw, B.; Glantz, S.A. Smokefree policies in Latin America and the Caribbean: Making progress. Int. J. Environ. Res. Public Health 2012, 9, 1954–1970. [Google Scholar] [CrossRef] [Green Version]
- WHO; CDC. Global Youth Tobacco Survey (GYTS); World Health Organization: Geneva, Switzerland, 2008; Available online: https://www.who.int/tobacco/surveillance/gyts/en/ (accessed on 10 May 2020).
- Valdes Salgado, R.; Shigematsu, L.M.; Hernandez Avila, M.; Peruga, A.; Hallal, A.L.; Warren, C.W.; Jones, N.R.; Asma, S.; Lee, J. Linking Global Youth Tobacco Survey (GYTS) data to the WHO Framework Convention on Tobacco Control (FCTC): The case for Mexico. Prev. Med. 2008, 47 (Suppl. 1), S20–S26. [Google Scholar] [CrossRef]
- de Almeida, L.M.; Cavalcante, T.M.; Casado, L.; Fernandes, E.M.; Warren, C.W.; Peruga, A.; Jones, N.R.; Curi Hallal, A.L.; Asma, S.; Lee, J. Linking Global Youth Tobacco Survey (GYTS) data to the WHO Framework Convention on Tobacco Control (FCTC): The case for Brazil. Prev. Med. 2008, 47 (Suppl. 1), S4–S10. [Google Scholar] [CrossRef]
- Konfino, J.; Ferrante, D.; Goldberg, L.; Caixeta, R.; Palipudi, K.M. Prevention. Tobacco use among youths--Argentina, 2007 and 2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 588–590. [Google Scholar]
- Zavaleta, A.; Salas, M.; Peruga, A.; Hallal, A.L.; Warren, C.W.; Jones, N.R.; Asma, S. Prevalence of smoking and other smoking related behaviors reported by the Global Youth Tobacco Survey (GYTS) in four Peruvian cities. BMC Public Health 2008, 8 (Suppl. 1), S2. [Google Scholar] [CrossRef] [Green Version]
- Warren, C.W.; Riley, L.; Asma, S.; Eriksen, M.P.; Green, L.; Blanton, C.; Loo, C.; Batchelor, S.; Yach, D. Tobacco use by youth: A surveillance report from the Global Youth Tobacco Survey project. Bull. World Health Organ. 2000, 78, 868–876. [Google Scholar]
- Arrazola, R.A.; Seidenberg, A.B.; Ahluwalia, I.B. Percentage of current tobacco smoking students receiving help or advice to quit: Evidence from the Global Youth Tobacco Survey, 56 countries, 2012–2015. Tob. Prev. Cessat. 2019, 5, 5. [Google Scholar] [CrossRef]
- WHO-TFI. WHO Report on the Global Tobacco Epidemic, 2008: The MPOWER Package; Tobacco Free Initiative (TFI); World Health Organization: Geneva, Switzerland, 2008; Available online: https://www.who.int/tobacco/mpower/2008/en/ (accessed on 19 August 2020).
- Quistberg, D.A.; Diez Roux, A.V.; Bilal, U.; Moore, K.; Ortigoza, A.; Rodriguez, D.A.; Sarmiento, O.L.; Frenz, P.; Friche, A.A.; Caiaffa, W.T.; et al. Building a Data Platform for Cross-Country Urban Health Studies: The SALURBAL Study. J. Urban Health Bull. N. Y. Acad. Med. 2019, 96, 311–337. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. GYTS: Sample Design and Weights; World Health Organization: Atlanta, GA, USA, 2014. [Google Scholar]
- Siegel, M.; Albers, A.B.; Cheng, D.M.; Hamilton, W.L.; Biener, L. Local restaurant smoking regulations and the adolescent smoking initiation process: Results of a multilevel contextual analysis among Massachusetts youth. Arch. Pediatr. Adolesc. Med. 2008, 162, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Cheng, K.-W.; Glantz, S.A.; Lightwood, J.M. Association between smokefree laws and voluntary smokefree-home rules. Am. J. Prev. Med. 2011, 41, 566–572. [Google Scholar] [CrossRef] [Green Version]
- Barrientos-Gutiérrez, T. Scientific and technical evaluation of Mexico’s General Law for Tobacco Control. Salud Publica Mex. 2010, 52 (Suppl. 2), S277–S282. [Google Scholar] [CrossRef] [Green Version]
- Backinger, C.L.; Fagan, P.; Matthews, E.; Grana, R. Adolescent and young adult tobacco prevention and cessation: Current status and future directions. Tob. Control 2003, 12, iv46–iv53. [Google Scholar] [CrossRef]
- Portes, L.H.; Machado, C.V.; Turci, S.R.B.; Figueiredo, V.C.; Cavalcante, T.M.; Silva, V.L.d.C.e. A Política de Controle do Tabaco no Brasil: Um balanço de 30 anos. Ciência Saúde Coletiva 2018, 23, 1837–1848. [Google Scholar] [CrossRef]
- Ministerio de Salud y Protección Social (Colombia). Estrategia de Entorno Educativo Saludable Dirección de Promoción y Prevención Subdirección de Salud Ambiental; Ministerio de Saud y Protección Social: Bogotá, Colombia, 2018. Avilable online:https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/SA/estrategia-entorno-educativo-2019.pdf (accessed on 28 July 2020).
- Gilpin, E.A.; White, M.M.; Messer, K.; Pierce, J.P. Receptivity to tobacco advertising and promotions among young adolescents as a predictor of established smoking in young adulthood. Am. J. Public Health 2007, 97, 1489–1495. [Google Scholar] [CrossRef]
- Audrain-McGovern, J.; Rodriguez, D.; Patel, V.; Faith, M.S.; Rodgers, K.; Cuevas, J. How do psychological factors influence adolescent smoking progression? The evidence for indirect effects through tobacco advertising receptivity. Pediatrics 2006, 117, 1216–1225. [Google Scholar] [CrossRef]
- Henriksen, L.; Schleicher, N.C.; Feighery, E.C.; Fortmann, S.P. A longitudinal study of exposure to retail cigarette advertising and smoking initiation. Pediatrics 2010, 126, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Congreso de la Republica (Peru). Ley 28705. Ley General Para La Prevención Y Control De Los Riesgos Del Consumo De Tabaco. and Modified 2010; Congreso de la República Peru: Lima, Peru, 2006; Available online: http://www.digesa.minsa.gob.pe/norma_consulta/Ley_29517.pdf (accessed on 23 July 2020).
- Stillman, F.A. Capacity building and human resource development for tobacco control in Latin America. Salud Pública de México 2010, 52, S340–S346. Available online: https://scielosp.org/pdf/spm/2010.v52suppl2/S340-S346/en (accessed on 26 June 2020). [CrossRef] [Green Version]
- Ramchand, R.; Ialongo, N.S.; Chilcoat, H.D. The effect of working for pay on adolescent tobacco use. Am. J. Public Health 2007, 97, 2056–2062. [Google Scholar] [CrossRef]
- World Health Organization. WHO Report on the Globla Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Estimator Used in Analysis | Direction | |
|---|---|---|
| Tobacco use | ||
| During the past 30 days (one month), on how many days did you smoke cigarettes? | Percentage of students who smoke cigarettes or used other tobacco products (answered ‘Yes’ to any of the 3 questions within this domain) | Lower is more favorable |
| During the past 30 days (one month), on the days you smoked, how many cigarettes did you usually smoke? | ||
| During the past 30 days (one month), have you ever used any form of tobacco products other than cigarettes (e.g., chewing tobacco, snuff, dip, cigars, cigarillos, little cigars, pipe)? | ||
| Smoke at home | ||
| During the past 7 days, on how many days have people smoked in your home, in your presence? | Percentage of students exposed to smokers in the home | Lower is more favorable |
| Smoke in other places | ||
| During the past 7 days, on how many days have people smoked in your presence, in places other than in your home? | Percentage of students who are exposed to smoke outside the home | Lower is more favorable |
| Anti-tobacco education in school | ||
| During this school year, were you taught in any of your classes about the dangers of smoking? | Average of the sum of the three items at city level (respondents were included if they answered at least 2 out of 3 items) | Higher is more favorable (more exposure to anti-tobacco information at school) |
| During this school year, did you discuss in any of your classes the reasons why people your age smoke? | ||
| During this school year, were you taught in any of your classes about the effects of smoking, like it makes your teeth yellow, causes wrinkles, or makes you smell bad? | ||
| Retailer refuses to sell cigarette | ||
| During the past 30 days (one month), did anyone ever refuse to sell you cigarettes because of your age? | Percentage of students who were unable to purchase a cigarette, among those who reported trying to buy a cigarette | Higher is more favorable (unable to purchase tobacco) |
| Media and advertising | ||
| Do you have something (t-shirt, pen, backpack, etc.) with a cigarette brand logo on it? | Average of the sum of the three items at city level (respondents were included if they answered at least 2 out of 3 items) | Lower is more favorable (less exposure to tobacco media and advertising) |
| During the past 30 days, did you see or hear any anti-tobacco media messages on television, radio, internet, billboards, posters, newspapers, magazines, or movies?/During the past 30 days (one month), how many anti-smoking media messages (e.g., television, radio, billboards, posters, newspapers, magazines, movies) have you seen? | ||
| When you watch TV, videos, or movies, how often do you see actors smoking? | ||
| Offered free cigarette | ||
| Has a cigarette+H20 representative ever offered you a free cigarette? | Percentage of students offered a free cigarette. | Lower is more favorable |
| Domains * and Summary Scores ** (Possible Range 1 = Worst Policy to 5 = Best Policy) | |||||||
|---|---|---|---|---|---|---|---|
| Average Score, All Domains | PROTECT | OFFER | WARN | ENFORCE | RAISE | ||
| Bans on Smoking | Cessation Services | Warnings on Packages | Bans on Advertising | Price of Tobacco | |||
| All countries below, average | |||||||
| Earliest year of monitoring | 2007 | 3.1 | 2.3 | 3.7 | 3.0 | 2.7 | 3.8 |
| Mid-period | 2010 | 3.6 | 3.0 | 3.7 | 4.3 | 3.2 | 3.8 |
| Later-period | 2014 | 4.1 | 4.3 | 4.0 | 4.8 | 3.7 | 3.8 |
| % Change 2007 to 2014 | 33% | 86% | 9% | 61% | 38% | 0% | |
| Argentina | |||||||
| Earliest year of monitoring | 2007 | 2.8 | 2 | 4 | 2 | 2 | 4 |
| Mid-period | 2010 | 2.8 | 2 | 4 | 2 | 2 | 4 |
| Later-period | 2014 | 4.4 | 5 | 4 | 5 | 4 | 4 |
| % Change 2007 to 2014 | 57% | 150% | 0% | 150% | 100% | 0% | |
| Brazil | |||||||
| Earliest year of monitoring | 2007 | 4.0 | 2 | 5 | 5 | 4 | 4 |
| Mid-period | 2010 | 4.0 | 2 | 5 | 5 | 4 | 4 |
| Later-period | 2014 | 4.8 | 5 | 5 | 5 | 5 | 4 |
| % Change 2007 to 2014 | 20% | 150% | 0% | 0% | 25% | 0% | |
| Chile | |||||||
| Earliest year of monitoring | 2007 | 4.0 | 3 | 3 | 5 | 4 | 5 |
| Mid-period | 2010 | 4.0 | 3 | 3 | 5 | 4 | 5 |
| Later-period | 2014 | 4.4 | 5 | 3 | 5 | 4 | 5 |
| % Change 2007 to 2014 | 10% | 67% | 0% | 0% | 0% | 0% | |
| Colombia | |||||||
| Earliest year of monitoring | 2007 | 2.4 | 2 | 3 | 2 | 2 | 3 |
| Mid-period | 2010 | 4.0 | 5 | 3 | 4 | 5 | 3 |
| Later-period | 2014 | 4.0 | 5 | 3 | 4 | 5 | 3 |
| % Change 2007 to 2014 | 67% | 150% | 0% | 100% | 150% | 0% | |
| Mexico | |||||||
| Earliest year of monitoring | 2007 | 2.8 | 2 | 4 | 2 | 2 | 4 |
| Mid-period | 2010 | 3.2 | 1 | 4 | 5 | 2 | 4 |
| Later-period | 2014 | 3.4 | 1 | 5 | 5 | 2 | 4 |
| % Change 2007 to 2014 | 21% | −50% | 25% | 150% | 0% | 0% | |
| Peru | |||||||
| Earliest year of monitoring | 2007 | 2.6 | 3 | 3 | 2 | 2 | 3 |
| Mid-period | 2010 | 3.6 | 5 | 3 | 5 | 2 | 3 |
| Later-period | 2014 | 3.8 | 5 | 4 | 5 | 2 | 3 |
| % Change 2007 to 2014 | 46% | 67% | 33% | 150% | 0% | 0% | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prado-Galbarro, F.-J.; Auchincloss, A.H.; Pérez-Ferrer, C.; Sanchez-Franco, S.; Barrientos-Gutierrez, T. Adolescent Tobacco Exposure in 31 Latin American Cities before and after the Framework Convention for Tobacco Control. Int. J. Environ. Res. Public Health 2020, 17, 7423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207423
Prado-Galbarro F-J, Auchincloss AH, Pérez-Ferrer C, Sanchez-Franco S, Barrientos-Gutierrez T. Adolescent Tobacco Exposure in 31 Latin American Cities before and after the Framework Convention for Tobacco Control. International Journal of Environmental Research and Public Health. 2020; 17(20):7423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207423
Chicago/Turabian StylePrado-Galbarro, Francisco-Javier, Amy H. Auchincloss, Carolina Pérez-Ferrer, Sharon Sanchez-Franco, and Tonatiuh Barrientos-Gutierrez. 2020. "Adolescent Tobacco Exposure in 31 Latin American Cities before and after the Framework Convention for Tobacco Control" International Journal of Environmental Research and Public Health 17, no. 20: 7423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207423