Longitudinal Association between Sport Participation and Depressive Symptoms after a Two-Year Follow-Up in Mid-Adolescence

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Instruments
2.3. Data Collection Procedure
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics and Gender Differences
3.2. Analysis of Change and Bivariate Correlations
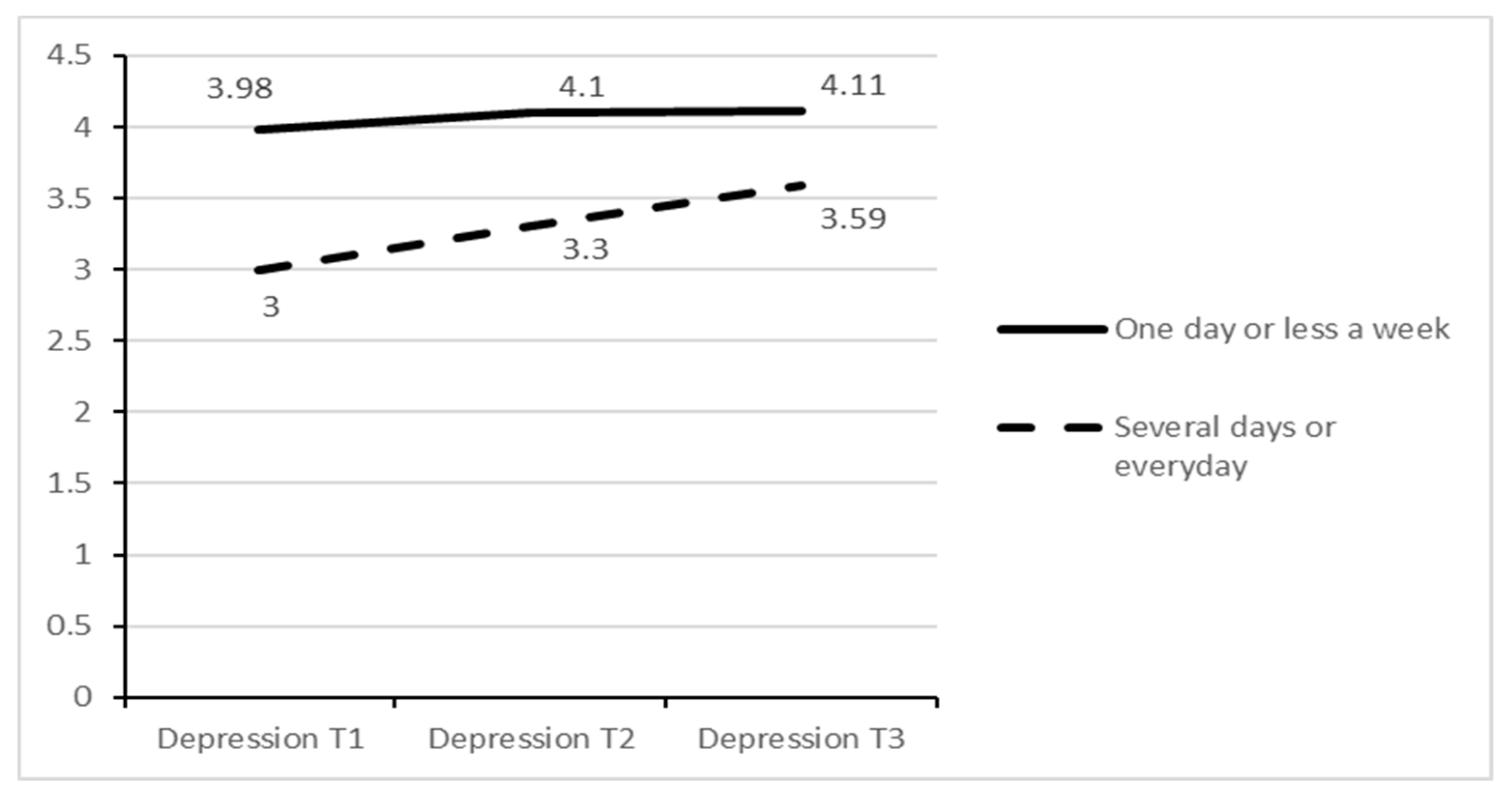
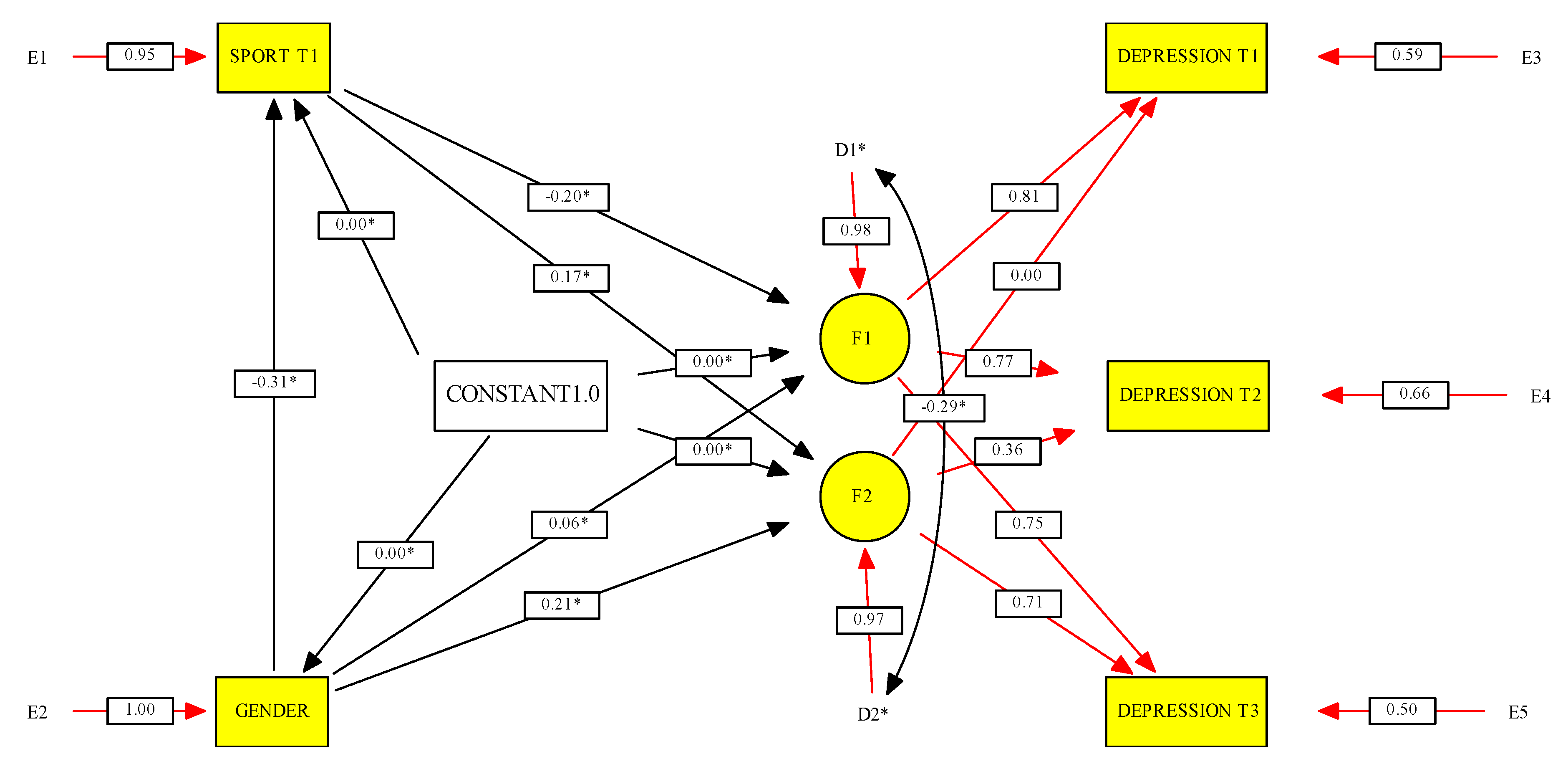
3.3. Change in Depressive Symptoms by Initial Sport Participation and Gender
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Primack, B.A.; Swanier, B.; Georgiopoulos, A.M.; Land, S.R.; Fine, M.J. Association Between Media Use in Adolescence and Depression in Young Adulthood: A longitudinal study. Arch. Gen. Psychiatry 2009, 66, 181–188. [Google Scholar] [CrossRef]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef] [Green Version]
- Galambos, N.L.; Leadbeater, B.J.; Barker, E.T. Gender differences in and risk factors for depression in adolescence: A 4-year longitudinal study. Int. J. Behav. Dev. 2004, 28, 16–25. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calmeiro, L.; Matos, M. Health assets and active lifestyles during pre-adolescence and adolescence: Highlights from the HBSC/WHO health survey and implications to health promotion. In Sport and Exercise Psychology Research: From Theory to Practice; Raab, M., Wylleman, P., Seiler, R., Elbe, A., Hatzigeorgiadis, A., Eds.; Elsevier: London, UK, 2016; pp. 443–460. [Google Scholar]
- White, R.L.; Babic, M.J.; Parker, P.D.; Lubans, D.R.; Astell-Burt, T.; Lonsdale, C. Domain-Specific Physical Activity and Mental Health: A Meta-analysis. Am. J. Prev. Med. 2017, 52, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Chalder, M.; Wiles, N.J.; Campbell, J.; Hollinghurst, S.P.; Haase, A.M.; Taylor, A.H.; Fox, K.R.; Costelloe, C.; Searle, A.; Baxter, H.; et al. Facilitated physical activity as a treatment for depressed adults: Randomised controlled trial. BMJ 2012, 344, e2758. [Google Scholar] [CrossRef] [Green Version]
- Mammen, G.; Faulkner, G. Physical Activity and the Prevention of Depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef]
- Matos, M.G.; Calmeiro, L.; Da Fonseca, D. Effet de l’activité physique sur l’anxiété et la dépression. La Presse Médicale 2009, 38, 734–739. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.H.; Ciaccioni, S.; Thomas, G.; Vergeer, I. Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychol. Sport Exerc. 2019, 42, 146–155. [Google Scholar] [CrossRef]
- Iannotti, R.J.; Janssen, I.; Haug, E.; Kololo, H.; Annaheim, B.; Borraccino, A.; HBSC Physical Activity Focus Group. Interrelationships of adolescent physical activity, screen-based sedentary behaviour, and social and psychological health. Int. J. Public Health 2009, 54, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Marques, A.; Calmeiro, L.; Loureiro, N.; Frasquilho, D.; De Matos, M.G. Health complaints among adolescents: Associations with more screen-based behaviours and less physical activity. J. Adolesc. 2015, 44, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Birkeland, M.S.; Torsheim, T.; Wold, B. A longitudinal study of the relationship between leisure-time physical activity and depressed mood among adolescents. Psychol. Sport Exerc. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Hume, C.; Timperio, A.; Veitch, J.; Salmon, J.; Crawford, D.; Ball, K. Physical Activity, Sedentary Behavior, and Depressive Symptoms Among Adolescents. J. Phys. Act. Health 2011, 8, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Toseeb, U.; Brage, S.; Corder, K.; Dunn, V.J.; Jones, P.B.; Owens, M.; Clair, M.C.S.; Van Sluijs, E.M.F.; Goodyer, I.M. Exercise and Depressive Symptoms in Adolescents. JAMA Pediatr. 2014, 168, 1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olive, L.S.; Telford, R.D.; Byrne, D.; Abhayaratna, W.P.; Telford, R.D. Psychological distress leads to reduced physical activity and fitness in children: The Australian longitudinal LOOK study. J. Behav. Med. 2016, 39, 587–598. [Google Scholar] [CrossRef]
- Raudsepp, L.; Vink, K. Brief report: Longitudinal associations between physical activity, sleep disturbance and depressive symptoms in adolescent girls. J. Adolesc. 2019, 72, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Jerstad, S.J.; Boutelle, K.N.; Ness, K.K.; Stice, E. Prospective reciprocal relations between physical activity and depression in female adolescents. J. Consult. Clin. Psychol. 2010, 78, 268–272. [Google Scholar] [CrossRef] [Green Version]
- Kandola, A.; Lewis, G.; Osborn, D.P.J.; Stubbs, B.; Hayes, J.F. Depressive symptoms and objectively measured physical activity and sedentary behaviour throughout adolescence: A prospective cohort study. Lancet Psychiatry 2020, 7, 262–271. [Google Scholar] [CrossRef] [Green Version]
- Langguth, N.; Schmid, J.; Gawrilow, C.; Stadler, G. Within-Person Link between Depressed Affect and Moderate-to-Vigorous Physical Activity in Adolescence: An Intensive Longitudinal Approach. Appl. Psychol. Health Well-Being 2016, 8, 44–63. [Google Scholar] [CrossRef] [Green Version]
- Straatmann, V.S.; Oliveira, A.J.; Rostila, M.; Lopes, C.S. Changes in physical activity and screen time related to psychological well-being in early adolescence: Findings from longitudinal study ELANA. BMC Public Health 2016, 16, 977. [Google Scholar] [CrossRef] [Green Version]
- Matos, M.G.; Marques, L.C.A.; Nuno, L. Does Physical Activity Promotion Advantages Need the Identification of Associated Health Compromising Features such as Injuries, Alcohol Use and Interpersonal Violence? Highlights from HBSC/WHO Portuguese Survey. J. Child Adolesc. Behav. 2013, 1, 113–118. [Google Scholar] [CrossRef]
- Fredricks, J.A.; Eccles, J.S. Is extracurricular participation associated with beneficial outcomes? Concurrent and longitudinal relations. Dev. Psychol. 2006, 42, 698–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarrett, N.; Fay, K.; Li, Y.; Carrano, J.; Phelps, E.; Lerner, R.M. More than child’s play: Variable-and pattern-centered approaches for examining effects of sports participation on youth development. Dev. Psychol. 2009, 45, 368–382. [Google Scholar] [CrossRef] [PubMed]
- Doré, I.; Sabiston, C.M.; Sylvestre, M.-P.; Brunet, J.; O’Loughlin, J.; Nader, P.A.; Gallant, F.; Bélanger, M. Years Participating in Sports During Childhood Predicts Mental Health in Adolescence: A 5-Year Longitudinal Study. J. Adolesc. Health 2019, 64, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.-T.; Chow, A.; Amemiya, J. Who Wants to Play? Sport Motivation Trajectories, Sport Participation, and the Development of Depressive Symptoms. J. Youth Adolesc. 2017, 52, 317–1998. [Google Scholar] [CrossRef]
- Sabiston, C.M.; Jewett, R.; Ashdown-Franks, G.; Bélanger, M.; Brunet, J.; O’Loughlin, E.; O’Loughlin, J. Number of Years of Team and Individual Sport Participation During Adolescence and Depressive Symptoms in Early Adulthood. J. Sport Exerc. Psychol. 2016, 38, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Del Barrio, V.; Capilla, M.L.R.; Olmedo, M.; Colodrón, F. Primera adaptación del CDI-S a población española. Accion Psicol. 2002, 3, 263–272. [Google Scholar] [CrossRef]
- Kovacs, M. The Children’s Depression Inventory Manual; Multi-Health Systems: New York, NY, USA, 1992. [Google Scholar]
- Mendoza, R.; Sagrera, M.R.; Batista, J.M. Conductas De Los Escolares Espanoles Relacionadas Con La Salud (1986–1990); Consejo Superior de Investigaciones Científicas: Madrid, Spain, 1994. [Google Scholar]
- Wold, B.; Aaro, L.E.; Smith, C. Health Behaviour in School-Aged Children. A WHO Cross-National Survey. Research Protocol for the 1993/94 Study; Research Centerfor Health Promotion, University of Bergen (HE MIL Rapport: 4): Bergen, Norway, 1994. [Google Scholar]
- Duncan, T.E.; Duncan, S.C.; Strycker, L.A. An Introduction to Latent Variable Growth Curve Modeling: Concepts, Issues, and Application; Routledge Academic: New York, NY, USA, 2013. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with EQS: Basic Concepts, Applications, and Programming; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- North, T.C.; Mccullagh, P.; Tran, Z.V. Effect of Exercise on Depression. Exerc. Sport Sci. Rev. 1990, 18, 379–415. [Google Scholar] [CrossRef]
- Craft, L.L.; Landers, D.M. The Effect of Exercise on Clinical Depression and Depression Resulting from Mental Illness: A Meta-Analysis. J. Sport Exerc. Psychol. 1998, 20, 339–357. [Google Scholar] [CrossRef]
- McPHIE, M.L.; Rawana, J.S. The effect of physical activity on depression in adolescence and emerging adulthood: A growth-curve analysis. J. Adolesc. 2015, 40, 83–92. [Google Scholar] [CrossRef] [PubMed]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Sarchiapone, M.; Apter, A.; et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2016, 26, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Matos, M.G.; Aventura Social. A Saúde Dos Adolescentes Portugueses Após a Recessão (e-Book); 2018; Available online: www.aventurasocial.com (accessed on 25 August 2020).
- Zhou, J.; Heim, D.; O’Brien, K.S. Alcohol Consumption, Athlete Identity, and Happiness Among Student Sportspeople as a Function of Sport-Type. Alcohol Alcohol. 2015, 50, 617–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, D.I.; Sabia, J.J. Exercise and adolescent mental health: New evidence from longitudinal data. J. Ment. Health Policy Econ. 2010, 13, 13–25. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Mean (Standard Deviation) | ||||
|---|---|---|---|---|
| Gender Differences | ||||
| Variables | Total | Boys | Girls | t-Tests |
| 1. Depressive symptoms Time 1 | 3.25 (2.57) | 2.92 (2.64) | 3.59 (2.46) | t(519) = −2.97, p = 0.003, d = 0.26 |
| 2. Depressive symptoms Time 2 | 3.57 (2.71) | 3.15 (2.59) | 3.96 (2.77) | t(419) = −3.33, p = 0.001, d = 0.30 |
| 3. Depressive symptoms Time 3 | 3.72 (2.81) | 3.09 (2.71) | 4.32 (2.78) | t(493) = −4.96, p < 0.001, d = 0.45 |
| 4. Frequency of Sport Participation Time 1 | 3.41 (1.28) | 3.80 (1.19) | 3.02 (1.25) | t(523) = 7.34, p < 0.001, d = 0.64 |
| 5. Frequency of Sport Participation Time 2 | 3.38 (1.23) | 3.78 (1.13) | 2.97 (1.19) | t(519) = 7.99, p < 0.001, d = 0.70 |
| 6. Frequency of Sport Participation Time 3 | 3.43 (1.26) | 3.86 (1.09) | 2.99 (1.28) | t(522) = 8.40, p < 0.001, d = 0.73 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Depressive symptoms Time 1 | 1 | |||||
| 2. Depressive symptoms Time 2 | 0.54 *** | 1 | ||||
| 3. Depressive symptoms Time 3 | 0.43 *** | 0.59 *** | 1 | |||
| 4. Sport Participation Time 1 | −0.16 ** | −0.08 | −0.03 | 1 | ||
| 5. Sport Participation Time 2 | −0.14 ** | −0.11 * | −0.05 | 0.65 *** | 1 | |
| 6. Sport Participation Time 3 | −0.10 * | −0.09 | −0.07 | 0.51 *** | 0.59 *** | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Baya, D.; Calmeiro, L.; Gaspar, T.; Marques, A.; Loureiro, N.; Peralta, M.; Mendoza, R.; Gaspar de Matos, M. Longitudinal Association between Sport Participation and Depressive Symptoms after a Two-Year Follow-Up in Mid-Adolescence. Int. J. Environ. Res. Public Health 2020, 17, 7469. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207469
Gómez-Baya D, Calmeiro L, Gaspar T, Marques A, Loureiro N, Peralta M, Mendoza R, Gaspar de Matos M. Longitudinal Association between Sport Participation and Depressive Symptoms after a Two-Year Follow-Up in Mid-Adolescence. International Journal of Environmental Research and Public Health. 2020; 17(20):7469. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207469
Chicago/Turabian StyleGómez-Baya, Diego, Luis Calmeiro, Tânia Gaspar, Adilson Marques, Nuno Loureiro, Miguel Peralta, Ramón Mendoza, and Margarida Gaspar de Matos. 2020. "Longitudinal Association between Sport Participation and Depressive Symptoms after a Two-Year Follow-Up in Mid-Adolescence" International Journal of Environmental Research and Public Health 17, no. 20: 7469. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207469