A Framework for Enhancing Access to Equitable Home Care for 2SLGBTQ+ Communities


Abstract
:1. Introduction
1.1. 2SLGBTQ+ Health Services Access and Equity
1.2. Organizational Responses to 2SLGBTQ+ Health Services Access and Equity
1.3. The 2SLGBTQ+ Home Care Access Project
2. Methodology
2.1. Recruitment and Data Collection
Surveys, Interviews, and Focus Groups
2.2. Data Analysis
2.2.1. Quantitative Data
2.2.2. Qualitative Data
2.3. Participants
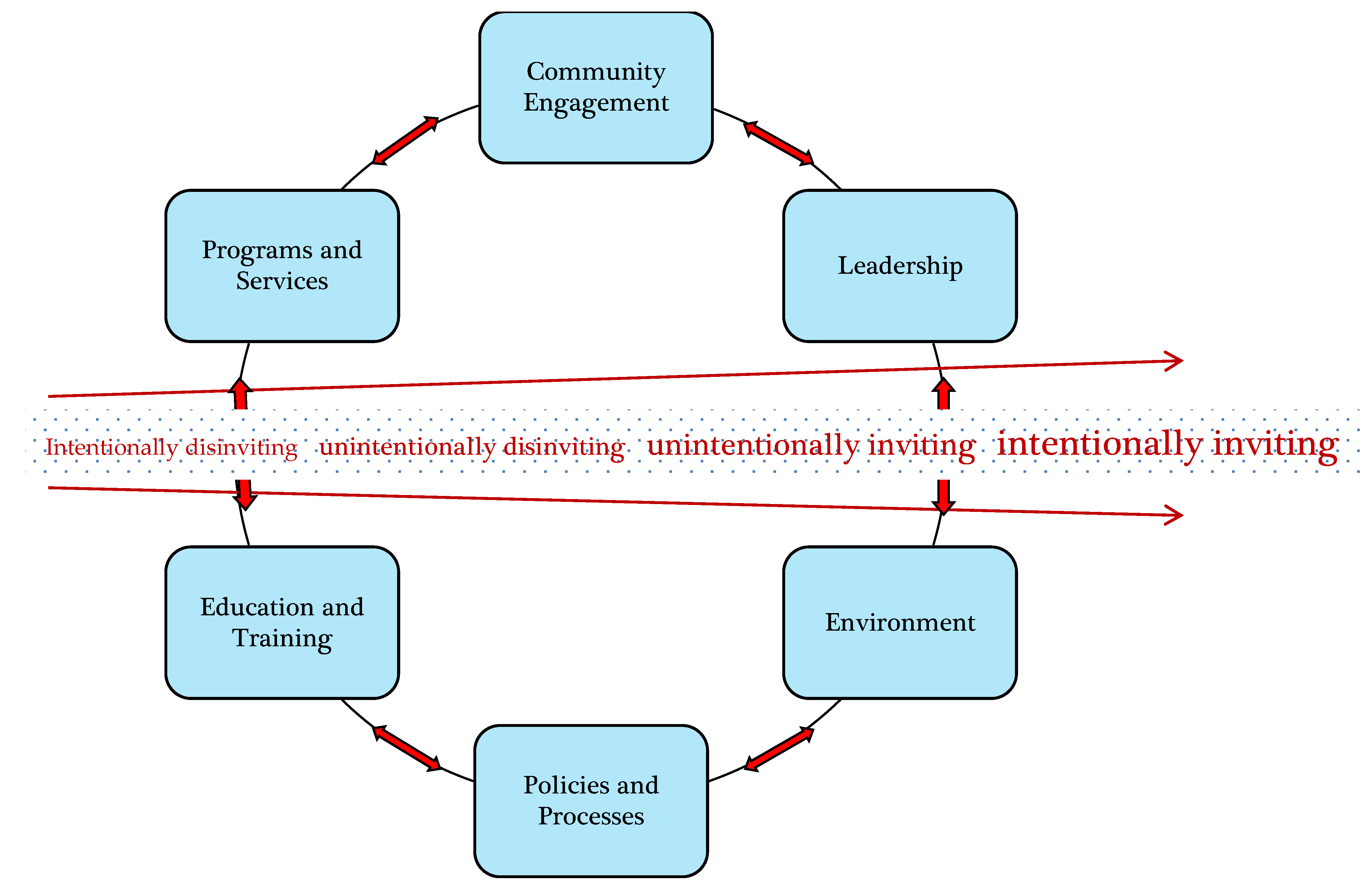
2.3.1. 2SLGBTQ+ Home Care Access and Equity Framework
2.3.2. Implementing the 2SLGBTQ+ Home Care Access and Equity Framework
2.3.3. 2SLGBTQ+ Invisibility in Home Care Organizations
“It takes more than just having a few committed individuals. You really need to formalize [that within] an organizational structure, so you need to have a policy framework ensuring that you’ve got components of recognition of diversity built in, not just a singular policy on anti-discrimination but making sure that it’s woven through all of the policies … and, it really needs to be informed by the communities. (home care administrator)”
2.3.4. Lack of 2SLGBTQ+ Education and Training among Home Care Service Providers
“I had to educate, and they actually appreciated the education because they didn’t really have much experience with transgender people. They didn’t understand what it meant, so I had to explain it. (trans service user)”
“I’m done at this point of teaching people what Black means to me… there’s lots of books and the Internet and I can show you some resources, but I’m not going to be the person who’s always rehashing these parts of myself for your education. (queer service user)”
2.3.5. Trans People Are Less Likely to Use Formal Home Care
“The trans piece would be a knowledge gap for me; supporting the medical side of hormone therapy and all that. (Nurse)”
“My health card still had “M” on it. They came in thinking they were dealing with a male. So that was kind of awkward for me. (trans woman)”
- Secure predictable and sustainable money resources;
- Ensure committed and informed leadership through ongoing training. Attention must be paid to hiring members of equity-seeking groups into leadership positions;
- Establish an equity, diversity, and inclusion (EDI) committee that includes staff across all levels of the organization, including out and diverse 2SLGBTQ+ staff, 2SLGBTQ+ community members that represent diverse experiences, knowledge, and perspectives, and other 2SLGBTQ+-relevant stakeholders (e.g., partner organizations);
- Train all staff, including the EDI committee in order to build EDI capacity and competency and understanding of the A&E Framework;
- Create a communication pathway and feedback loop to ensure that staff is regularly informed of, and can provide input on, A&E implementation goals, processes, and strategies;
- Create a timeline and processes for A&E Framework implementation components including (to be completed by the equity consultant and EDI committee):
- Determine a time period for the 2SLGBTQ+ A&E plan (e.g., 5-year plan with review and renewal every five years);
- Identify organizational EDI goals and measures related to 2SLGBTQ+ access and equity, with realistic consideration of money and people resources (e.g., 15% of Board members identify as S2LGBTQ+ by [date]);
- Prioritize change areas and change strategies (e.g., training for all service providers) based on the 6 key indicators;
- Implement change strategies;
- Determine an assessment and reporting timeline for the change strategies (e.g., quarterly assessment with an annual 2SLGBTQ+ A&E report);
- Determine a timeline for the evaluation of the A&E Framework;
- Determine an evaluation framework (e.g., audit of change strategies, consultation with equity advisors and EDI committee, 2SLGBTQ+ community, and other 2SLGBTQ+-relevant stakeholders);
- Determine performance measures for the A&E Framework;
- Revise A&E Framework where needed;
- At the end of the 2SLGBTQ+ A&E plan period, assess organization change through an organization-wide process and identify EDI goals and measures related to 2SLGBTQ+ access and equity and change strategies for the subsequent plan period.
3. Concluding Thoughts
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Strengthening Equity, Diversity and Inclusion in Research. Available online: https://www.canada.ca/en/research-coordinating-committee/priorities/equity-diversity-inclusionresearch.html (accessed on 31 July 2020).
- GRC News COVID-19 Special Issue Risk, Response, and Resilience in an Aging COVID-19 World. Summer. Available online: https://www.sfu.ca/content/dam/sfu/grc/stories/grc-news/GRC-News-Summer-2020.pdf (accessed on 31 July 2020).
- The Lives and Livelihoods of Many in the LGBTQ Community Are at Risk Amidst COVID-19 Crisis. Available online: https://www.hrc.org/resources/the-lives-and-livelihoods-of-many-in-the-lgbtq-community-are-at-risk-amidst-covid-19-crisis (accessed on 31 July 2020).
- Hulko, W.; Brotman, S.; Stern, L.; Ferrer, I. Gerontological Social Work in Action: Anti-Oppressive Practice with Older Adults, Their Families, and Communities; Routledge: Abingdon, UK, 2020; pp. 1–276. [Google Scholar]
- Gender-Based Analysis Plus. Available online: https://cfc-swc.gc.ca/gba-acs/substainable-perennite-en.html (accessed on 22 August 2020).
- Introduction to GBA+: Module 2—Moving Beyond Sex and Gender. Available online: https://cfc-swc.gc.ca/gba-acs/course-cours/eng/mod02/mod02_01_01.html (accessed on 22 August 2020).
- Hankivsky, O.; Mussell, L. Gender-based analysis plus in Canada: Problems and possibilities of integrating intersectionality. Can. Public Policy 2018, 44, 303–316. [Google Scholar] [CrossRef]
- Findlay, T. Revisiting GBA/GBA+: Innovations and interventions. Can. Public Adm. 2019, 62, 520–525. [Google Scholar] [CrossRef]
- Mulé, N.; Smith, M. Invisible populations: LGBTQ people and federal health policy in Canada. Can. Public Adm. 2014, 57, 234–255. [Google Scholar] [CrossRef]
- Paterson, S.; Scala, F. Gender mainstreaming and the discursive politics of public service values. Adm. Theory Praxis 2017, 39, 1–18. [Google Scholar] [CrossRef]
- Rankin, P.; Wilcox, K. De-gendering engagements? Gender mainstreaming, women’s movements and the Canadian federal state. Atlantis 2004, 29, 52–60. [Google Scholar]
- McNutt, K.; Beland, F. Implementing and integrated government strategy: The quest for gender mainstreaming in Canada. Can. Rev. Am. Stud. 2015, 45, 467–485. [Google Scholar] [CrossRef]
- Mulé, N.J. State involvement in LGBT+ health and social support issues in Canada. Int. J. Environ. Res. Public Health 2020, 17, 7314. [Google Scholar] [CrossRef]
- Paterson, S. What’s the problem with gender-based analysis? Gender mainstreaming policy and practice in Canada. Can. Public Adm./Adm. Publique Can. 2010, 53, 395–416. [Google Scholar] [CrossRef]
- Caceres, B.A.; Travers, J.; Primiano, J.E.; Luscombe, R.; Dorsen, C. Provider and LGBT individuals’ perspectives on LGBT issues in long-term care: A systematic review. Gerontologist 2020, 60, e169–e183. [Google Scholar] [CrossRef]
- Daley, A.; MacDonnell, J.; Brotman, S.; St. Pierre, M.; Aronson, J.; Gillis, L. Providing health and social services to older LGBT adults. Annu. Rev. Gerontol. Geriatr. 2007, 37, 143–160. [Google Scholar] [CrossRef]
- Fredriksen-Goldsen, K.; Jen, S.; Muraco, A. Iridescent life course: LGBTQ aging research and blueprint for the future: A systematic review. Gerontology 2019, 65, 253–274. [Google Scholar] [CrossRef] [PubMed]
- Giblon, R.; Bauer, G.R. Health care availability, quality, and unmet need: A comparison of transgender and cisgender residents of Ontario, Canada. BMC Health Serv. Res. 2017, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Being Safe, Being Me 2019: Results of the Canadian Trans and Non-Binary Youth Health Survey. Available online: https://www.saravyc.ubc.ca/2020/03/18/being-safe-being-me-2019/ (accessed on 22 August 2020).
- Vermeir, E.; Jackson, A.; Gard Marshall, E. Barriers to primary and emergency healthcare for trans adults. Cult. Health Sex 2018, 20, 232–246. [Google Scholar] [CrossRef]
- Kim, H.; Jen, S.; Fredriksen-Goldsen, K.I. Race/ethnicity and health-related quality of life among LGBT older adults. Gerontologist 2017, 57, S30–S39. [Google Scholar] [CrossRef] [Green Version]
- Trinh, M.; Agénor, M.; Austin, S.B.; Jackson, C. Health and healthcare disparities among U.S. women and men at the intersection of sexual orientation and race/ethnicity: A nationally representative cross-sectional study. BMC Public Health 2017, 17, 964. [Google Scholar] [CrossRef]
- Ryan, B.; Brotman, S.; Baradaran, A.; Lee, E. Cultures, Sexualités et Genres; Presses de l’Université du Québec, Coll. Santé et Société: Québec, QC, Canada, 2008; pp. 307–337. [Google Scholar]
- Bird, N.; Robinson, M. The Oxford Handbook of Sexual and Gender Minority Mental Health; Oxford University Press: Oxford, UK, 2020; pp. 209–220. [Google Scholar]
- Kai, H.; MacKay, J.; Ross, L.; Robinson, M. Poverty in lesbian, gay, bisexual, transgender, queer, and two-spirit (LGBTQ2S+) populations in Canada: An intersectional review of the literature. J. Poverty Soc. Justice 2020, 28, 21–54. [Google Scholar] [CrossRef]
- Logie, C.H.; Lacombe-Duncan, A.; Lee-Foon, N.; Ryan, S.; Ramsay, H. It’s for us newcomers, LGBTQ persons, and HIV-positive persons. You feel free to be: A qualitative study exploring social support group participation among African and Caribbean lesbian, gay, bisexual and transgender newcomers and refugees in Toronto, Canada. BMC Int. Health Hum. Rights 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Kamen, C.S.; Alpert, A.; Margolies, L.; Griggs, J.J.; Darbes, L.; Smith-Stoner, M.; Lytle, M.; Poteat, T.; Scout, N.F.N.; Norton, S.A. Treat us with dignity: A qualitative study of the experiences and recommendations of lesbian, gay, bisexual, transgender, and queer (LGBTQ) patients with cancer. Support. Care Cancer 2019, 27, 2525–2532. [Google Scholar] [CrossRef]
- Gahagan, J.; Subirana-Malaret, M. Improving pathways to primary health are among LGBTQ populations and health care providers: Key findings from Nova Scotia, Canada. Int. J. Equity Health 2018, 17. [Google Scholar] [CrossRef] [Green Version]
- Logie, C.H.; Lys, C.L.; Dias, L.; Schott, N.; Zouboules, M.R.; MacNeill, N.; Mackay, K. Automatic assumption of your gender, sexuality and sexual practices is also discrimination: Exploring sexual healthcare experiences and recommendations among sexually and gender diverse persons in Arctic. Health Soc. Care Community 2019, 27, 1204–1213. [Google Scholar] [CrossRef]
- Willis, P.B.; Raithby, M.; Maegusuku-Hewett, T. It’s a nice country but it’s not mine: Exploring the meanings attached to home, rurality and place for older lesbian, gay and bisexual adults. Health Soc. Care Community 2018, 26, 908–916. [Google Scholar] [CrossRef]
- Henderson, N.; Khan, J.F. I will die if I have to go into an old age home: Afrocentric options for care of older LGBT people in South Africa. Agenda 2020. [Google Scholar] [CrossRef]
- Löf, J.; Olaison, A. I don’t want to go back into the closet just because I need care’: Recognition of older LGBTQ adults in relation to future care needs. Eur. J. Soc. Work 2020, 23, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Butler, S. Older lesbians’ experiences with home care: Varying levels of disclosure and discrimination. J. Gay Lesbian Soc. Serv. 2017, 29, 378–398. [Google Scholar] [CrossRef]
- Butler, S. Older lesbians receiving home care: Formal and informal dimensions of caregiving. J. Women Aging 2018, 30, 91–110. [Google Scholar] [CrossRef]
- Grigorovich, A. The meaning of quality of care in home care settings: Older lesbian and bisexual women’s perspectives. Scand. J. Caring Sci. 2016, 30, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Grigorovich, A. Negotiating sexuality in home care settings: Older lesbians and bisexual women’s experiences. Culture Health Sex. 2015, 17, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Pijpers, R. Experiences of LGBT older people aging in pace with care and support: A window on ordinary ageing environments, home-making practices and meeting activities. Sexualities 2020, 9, 1–20. [Google Scholar] [CrossRef]
- Waling, A.; Lyons, A.; Alba, B.; Minichiello, V.; Barrett, C.; Hughes, M.; Fredriksen-Goldsen, K.; Edmonds, S. Experiences and perceptions of residential and home care services among older lesbian women and gay men in Australia. Health Soc. Care Community 2019, 27, 1251–1259. [Google Scholar] [CrossRef]
- Alba, B.; Lyons, A.; Waling, A.; Minichiello, V.; Hughes, M.; Barrett, C.; Fredriksen-Goldsen, K.; Edmonds, S. Health, well-being, and social support in older Australian lesbian and gay care-givers. Health Soc. Care Community 2019, 28, 204–215. [Google Scholar] [CrossRef]
- Daley, A.; MacDonnell, J. ‘That would have been beneficial’: 2SLGBTQ+-specific training for home care service providers. Sexualities 2015, 23, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Furlotte, C.; Gladstone, J.W.; Cosby, R.F.; Fitzgerald, K.A. Could we hold hands? Older lesbian and gay couples’ perceptions of long-term care homes and home care. Can. J. Aging 2016, 35, 432–446. [Google Scholar] [CrossRef] [Green Version]
- Lyons, A.; Alba, B.; Waling, A.; Minichiello, V.; Hughes, M.; Barrett, C.; Fredriksen-Goldsen, K.; Edmonds, S.; Pepping, C. Comfort among older lesbian and gay people in disclosing their sexual orientation to health and aged care services. J. Appl. Gerontol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brotman, S.; Ferrer, I.; Sussman, T.; Ryan, B.; Richard, B. Access and equity in the design and delivery of health and social care to LGBTQ older adults: A Canadian perspective. In The Lives of Lesbian, Gay, Bisexual and transgender Older Adults: Understanding Challenges and Resilience; Orel, N.A., Fruhauf, C.A., Eds.; American Psychological Association: Washington, DC, USA, 2015; pp. 111–140. [Google Scholar]
- LGBT Housing Matters: Results of the Canadian LGBT Older Adults and Housing Project. Available online: http://dc.msvu.ca:8080/xmlui/bitstream/handle/10587/2134/LGBT%20Housing%20Matters.pdf?sequence=1&isAllowed=y (accessed on 31 July 2020).
- Daley, A.; MacDonnell, J.A. Gender, sexuality and the discursive representation of access and equity in health services literature: Implications for LGBT communities. Int. J. Equity Health 2011, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daley, A.; MacDonnell, J.A.; St. Pierre, M. LGBTTQI Communities and Home Care in Ontario: Project Report; York University: Toronto, ON, Canada, 2016; Available online: https://yorkspace.library.yorku.ca/xmlui/bitstream/handle/10315/32817/LGBTTQICommunitiesandHomeCareinOntarioProjectReport.pdf?sequence=1&isAllowed=y (accessed on 31 July 2020).
- Sordi Marti, T.; Mertens, D.M. Mixed methods research with groups at risk: New developments and key debates. J. Mix. Methods Res. 2014, 8, 207–211. [Google Scholar] [CrossRef] [Green Version]
- The Future of Mixed Methods: A Five Year Projection to 2020. Available online: https://mmira.wildapricot.org/resources/Documents/MMIRA%20task%20force%20report%20Jan2016%20final.pdf (accessed on 22 August 2020).
- Mertens, D.M. Philosophy in mixed methods teaching: The transformative paradigm as illustration. Int. J. Mult. Res. Approaches 2010, 4, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Mertens, D. Mixed methods as tools for social change. J. Mix. Methods Res. 2011, 5, 195–197. [Google Scholar] [CrossRef] [Green Version]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs—Principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [Green Version]
- MacDonnell, J.; Daley, A. Examining the development of positive space in health and social service organizations: A Canadian exploratory study. J. Gay Lesbian Soc. Serv. 2015, 27, 263–301. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, I.; Grenier, A.; Brotman, S. Developing a theoretical framework integrating intersectionality and critical life course. J. Aging Stud. 2017, 41, 10–17. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; Sage: London, UK, 2008. [Google Scholar]
- Purkey, W.W.; Novak, J.M. Fundamentals of Invitational Education, 1st ed.; Kennesaw State University: Kennesaw, GA, USA, 2008. [Google Scholar]
- MacDonnell, J.A. LGBT health care access: Considering the contributions of an invitational approach. J. Invit. Theory Pract. 2014, 20, 38–60. [Google Scholar]
- Crenshaw, K.W. On Intersectionality: Essential Writings; The New Press: New York, NY, USA, 2017. [Google Scholar]
- Ahlberg, B.M.; Hamed, S.; Thapar-Björkert, S.; Bradby, H. Invisibility of racism in the global neoliberal era: Implications for researching racism in healthcare. Front. Sociol. 2019, 4. [Google Scholar] [CrossRef] [Green Version]
- Braveman, P. What are health disparities and health equity? We need to be clear. Public Health Rep. 2014, 129, 5–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, M.; Perrin, P.B.; Rybarczyk, B.; Tan, J. Racism, mental health, healthcare provider trust, and medication adherence among black patients in safety-net primary care. J. Clin. Psychol. Med. Settings 2020. [Google Scholar] [CrossRef]
- Powella, W.; Richmond, J.; Mohottigec, D.; Yend, I.; Joslyna, A.; Corbie-Smithe, G. Medical mistrust, racism, and delays in preventive health screening among African-American men. Behavior 2019, 45, 102–117. [Google Scholar] [CrossRef]
- Brotman, S.; Ryan, B.; Jalbert, Y.; Rowe, B. Reclaiming space-regaining health: Health care access and two-spirit people in Canada. J. Gay Lesbian Soc. Serv. 2002, 14, 67–87. [Google Scholar] [CrossRef]
- Diversity and Inclusion: Framework and Implementation Plan. Available online: https://www.edmonton.ca/programs_services/documents/PDF/Final_Diversity__Inclusion_Framework__Implementation_Plan.pdf (accessed on 22 August 2020).


{kind=link}
| Indicator of Access to Care | Assessment Prompts |
|---|---|
| Environment | How does staff use language to convey recognition, acceptance, and affirmation of 2SLGBTQ+ people? Are 2SLGBTQ+ people able to see themselves represented in visual cues within the physical environment of the agency (rainbow/triangle symbols, 2SLGBTQ+ representation of available brochures/posters; 2SLGBTQ+-relevant brochures/posters, promotional materials for agency services and programs that are 2SLGBTQ+-inclusive) and within/amongst agency staff? Do program-specific intake forms include demographic options that convey recognition, acceptance, and affirmation of 2SLGBTQ+ people? (Gender-neutral options such as ‘domestic partner’ or ‘same-sex partner’ along with gender-inclusive options to choose male/female/trans/trans man/trans woman/genderqueer, and gender-neutral questions about relationships and sexual behaviour) What processes are in place to foster the creation of culturally safe space and organizational support of diverse 2SLGBTQ+ employees? How does the agency administratively support 2SLGBTQ+ employee networks/working groups? Does the agency advocate for health equity initiatives to address systemic disparities in access? For example, does the agency advocate for community-based research that will increase their knowledge about the issues in providing 2SLGBTQ+-inclusive services and programs to diversely situated and identified populations? |
| Indicators of Access to Care | Assessment Prompts |
|---|---|
| Community Engagement | Are 2SLGBTQ+ people engaged with the agency? If so, who is represented? Does the community engagement process include diverse 2SLGBTQ+ experiences, knowledge, and perspectives? How are 2SLGBTQ+ people involved in needs assessment processes, identifying program/service directions, and delivering and evaluating them? |
| Leadership | Are openly 2SLGBTQ+ people in positions of leadership including within senior management? Is shared or distributive leadership used across the organization to engage in systems advocacy, for example, in relation to obtaining the resources (e.g., training or research) required to address health disparities and access barriers? |
| Environment | Do program-specific intake forms include demographic options that convey recognition, acceptance, and affirmation of 2SLGBTQ+ people (options such as “domestic partner(s)” or “same-sex partner(s)” and options to indicate used pronouns)? How does the agency administratively support 2SLGBTQ+ employee networks/working groups? |
| Policies & Processes | Are policies that address equity for both 2SLGBTQ+ service users and employees consistent across all programs? Do hiring practices include assessing diversity and 2SLGBTQ+ competence of candidates? Do staff evaluation practices include assessing diversity and 2SLGBTQ+ competency? |
| Indicator of Access to Care | Assessment Prompts |
|---|---|
| Education and training | Do all staff receive education and training? Where does training occur inside/outside the agency? What training opportunities occur (orientation, in-services, continuing education, specialized training to build clinical and human resources capacity)? How are 2SLGBTQ+ people involved in education and the development of material (e.g., train the trainer?)? How are diverse 2SLGBTQ+ experiences, knowledges, and perspectives reflected in education and training? How is education framed in terms of meeting agency goals for quality (mandatory/elective) accreditation? How does the agency culture support the notion of a learning organization, allowing for critical questioning of its practices? |
| Indicator of Access to Care | Assessment Prompts |
|---|---|
| Programs & Services | Are trans service users and staff involved in programming, agency processes (e.g., strategic planning)? How does the agency represent the voice/visibility of trans service users in programs and services? How are all programs inclusive of LGBTTQI health (e.g., intake forms)? Are programs developed, delivered, evaluated with trans communities? What reporting processes for clients/staff are in place to respond to discrimination, quality of care/work environment? How is the agency involved in research and advocacy to meet the needs of trans service users across, e.g., race, age, and condition? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daley, A.; Brotman, S.; MacDonnell, J.A.; St. Pierre, M. A Framework for Enhancing Access to Equitable Home Care for 2SLGBTQ+ Communities. Int. J. Environ. Res. Public Health 2020, 17, 7533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207533
Daley A, Brotman S, MacDonnell JA, St. Pierre M. A Framework for Enhancing Access to Equitable Home Care for 2SLGBTQ+ Communities. International Journal of Environmental Research and Public Health. 2020; 17(20):7533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207533
Chicago/Turabian StyleDaley, Andrea, Shari Brotman, Judith A. MacDonnell, and Melissa St. Pierre. 2020. "A Framework for Enhancing Access to Equitable Home Care for 2SLGBTQ+ Communities" International Journal of Environmental Research and Public Health 17, no. 20: 7533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207533