1. Introduction
Overweight and obesity in children has been associated to several diseases in adult life, such as cardiovascular diseases, diabetes, hypertension, hypercholesterolemia [
1,
2,
3,
4]. In children, serious psychological and social consequences (e.g., lowered self-esteem and bulling in school) were also reported [
5,
6]. These consequences may be amplified with a serious impact on children when they simultaneously accumulate an immigration background and obesity.
Although the prevalence of overweight and obesity in children appears to be flattening in some European countries, in Portugal, some researchers argue that it is premature to consider that obesity in children is stabilizing [
7,
8]. The National Program for the Promotion of Healthy Eating highlighted a decreasing trend in prevalence of overweight and obesity, in children aged 6–8 years old, from 37.9% in 2008 to 29.6% in 2019 [
9]. However, Portugal is still one of the European countries with the highest prevalence of overweight and obesity in children [
8,
10,
11]. Although there are several local studies about overweight and obesity (e.g., in schools), few have explored overweight and obesity in immigrant children and its sociocultural influences and unhealthy behaviors [
10]. Moreover, data collection in different time moments, their analysis, and interpretation are crucial to understand overweight and obesity trends in immigrant and native children. In 1993, 2009, and 2013, André et al., 2017 found a lower risk of overweight and obesity for Cape Verdean children compared with native children (aged 6–12 years) in a deprived neighborhood in Lisbon area.
The puzzle of immigration in Portugal is different from other European countries. Even though due to the financial crisis from 2008 to 2010 Portugal saw a change in the number and profile of immigrants and foreign residents, the majority of immigrants continues to come from the Community of Portuguese-speaking Countries (CPLP), particularly from Brazil and from the African countries of Portuguese official language [
12].
Migration to Western societies seems to increase the risk of overweight and obesity, especially due to lifestyle alterations. Children that belong to communities with a high percentage of immigrants or with low socioeconomic status have a higher risk to develop obesity [
13,
14]. Studies have shown that obesity is more frequent in successive generations than in the first generation. Over time, immigrant populations assimilate certain attitudes and behaviors of the host country’s population [
15,
16]. Changing in diet patterns, that some immigrant populations are exposed, may in part explain the health status of these populations. Immigrants tend to engage in a more sedentary way of life, having lower access to the practice of sports, and they abandon their traditional food habits and adopt Westernized dietary patterns [
13,
17]. Immigrants tend to be poorer, with low wage jobs and unstable employment and consequently tend to access to low-priced, high-sugar, and high-fat foods [
18,
19,
20].
Further research is needed to understand the role of parental socioeconomic factors in the prevalence of overweight and obesity in children with immigration background, in order to design better community-based interventions at the local level [
21]. The lack of studies in Portugal about children of immigrants, mainly from low-and-middle-income countries and the geographical variations within the country, in terms of overweight and obesity, reinforce the need for regional and local studies [
22,
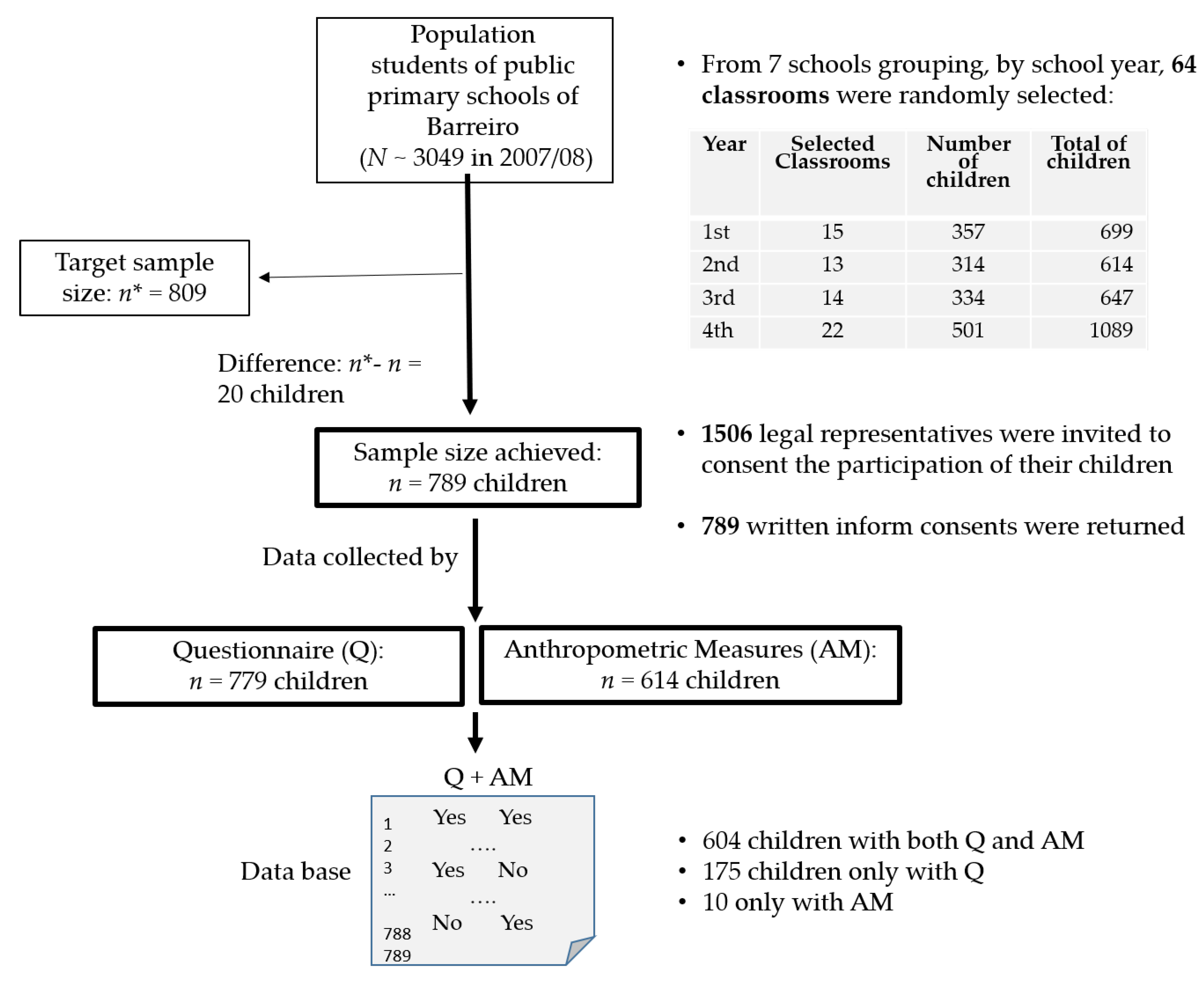
23]. In this work, we present data collected in 2009, in Barreiro—a municipality located south of Lisbon—including native and children with immigration backgrounds. Lisbon, Faro, and Setúbal presented the highest proportion of immigrants in Portugal. According to official data, in 2019, these three districts totalized 405,089 resident citizens (68.6% of the total) and Setúbal (where Barreiro is located) accounts to 51.983% (+29.3% compared with 2018) of immigrants [
24,
25]. School-age children of the public sector in Barreiro were evaluated in order to identify the association between nutritional status and a set of variables, including outdoors physical activity and food intakes, considering the origin of their parents. The last one has a central role in the main null hypotheses: (i) There no differences in terms of overweight and obesity and risk of abdominal obesity among three groups of children: “both mother and father are non-Portuguese,” “only one is Portuguese,” and “both are Portuguese,” (ii) children from immigrant origin and native children present similar anthropometric measures, and (iii) the migratory origin of parents does not influence some potential determinants of overweight and obesity in children of this particular setting.
4. Discussion
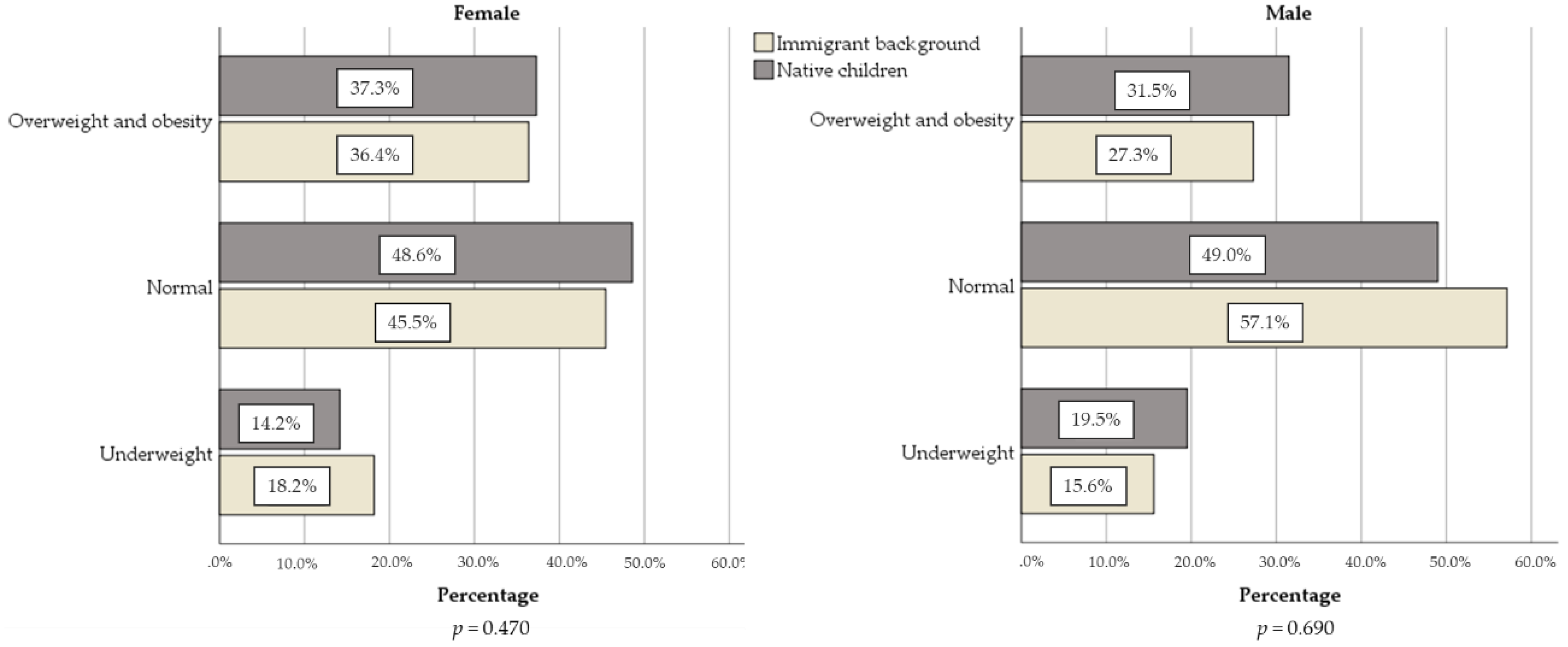
In the municipality of Barreiro, with immigrants mainly from low- and-middle-income countries of CPLP, no differences were found in terms of overweight and obesity and abdominal obesity risk in children of public schools, according to parents’ nationality. However, parents’ nationality seems to play a crucial role in some potential protective and risk factor for obesity. By sex, it seems to be a tendency for the females to have more overweight and obesity than males, however, this difference was not significant. The same occurred for abdominal obesity risk.
Contrary to immigrant children, we found some studies about overweight and obesity and its determinants for Portuguese children of slightly different ages [
28,
33,
34,
35,
36,
37]. For male children (6–10 years old), the prevalence of overweight varied from 14.7% to 30.5% and obesity from 5.3% to 13.2%. In girls, overweight varied from 16.5% to 29.1% and obesity from 6.4% to 12.6% [
28]. In addition to Portuguese children (6–8 years old), overweight prevalence was 32.2–95% CI [29.6; 34.9] and obesity was 14.4–95% CI [11.7; 17.6], following CDC definition [
8,
11]. Among 7–9 years old school children in Aveiro, Pedrosa et al. [
28] reported prevalence of excess weight between 28% and 31% according to International Obesity Task Force (IOTF) and CDC definitions, respectively. Gomes et al. [
33] summarized studies between 2004 and 2013 and a moderate-to-high prevalence values in 9–11 years old were reported in national samples (
n ranging from 405 to 3584).
In Portuguese school-age children, findings about abdominal obesity and detailed anthropometric measures among children with immigrant background (and natives) are rare. In 2013–2014, Rodrigues et al. [
38] found a prevalence of 21.9% and Albuquerque et al. [
39] found 23.6% in central region of Portugal. Both studies presented higher values compared with our study. André et al. [
10] presented height, sitting height, weight, BMI, and skinfolds for children in a deprived neighborhood in 1993, 2009, and 2013, concluding that Cape Verdean children had a lower risk of being overweight or obese than native children. Our children with an immigrant origin, on average, were younger and seem to present higher mean values of the mentioned measures for males and females. This advantageous situation was not found here and almost all anthropometric measures were similar for children with immigrant background and native group. About a one-third of our children (5–11 years old) presented overweight and obesity, without significant differences, according to parents’ nationality. Data also reveal difference between “underweight” and “overweight or obesity” (
Figure 2). The prevalence value for overweight or obesity is almost twice of underweight, even in children with an immigrant background. For Portuguese children (5–13 years old), an even more discrepant pattern has already been described [
40] and also in studies in low and middle-income countries [
41].
Angola was one of the most frequent countries of origin (
Table 1). This may bring a hidden and interesting finding. Angola was devastated by a 40-year period of war until 2002, forcing migration flows and high levels of chronic malnutrition continue to be a serious health problem nowadays. Fathers and mothers of our study (data collected in 2009) probably lived this war period. Angola continues to point out a high proportion of children suffering from stunting (37.6%) and wasting (4.9%), particularly in under-five children [
42]. Our children with parents from African countries seem to move to another extreme in terms of nutritional status, suffering also from overweight and obesity as the native children (aged 5–11 years).
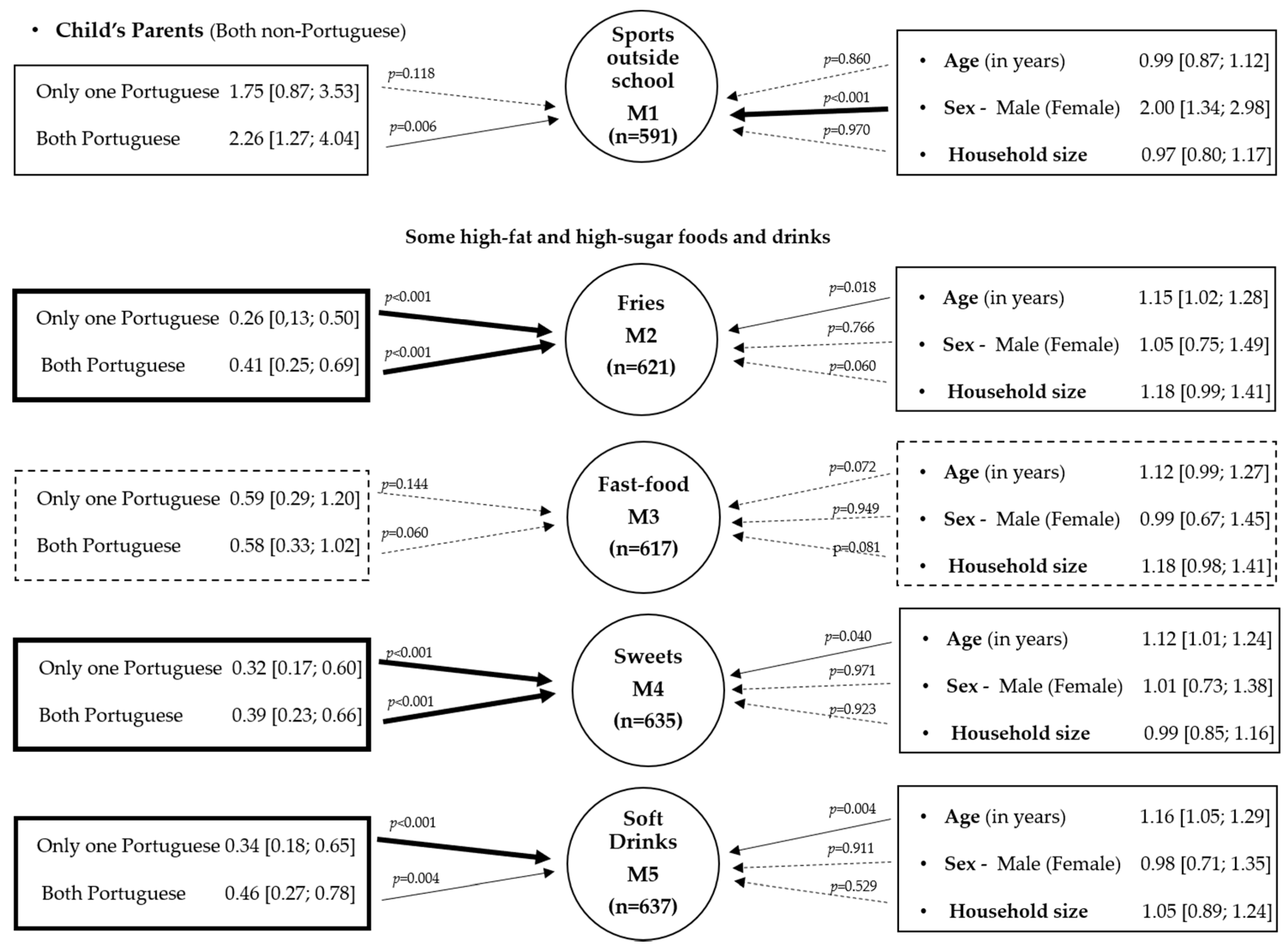
Fitted models highlighted the importance of parents’ nationality direct or indirectly through several variables such as the practice of sports outside school, fries, sweets, and soft drink consumption, which may eventually, in middle and long terms, reflect in the children’s nutritional status. Of course, fitted models were poor, which is likely due to the complexity and multifactorial nature of the food consumption. However, age was associated to an increase in fries, sweets, and soft drink consumption. Our findings need further consideration as high-sugar products consumption and less sports outside school were higher in female children compared with male children. Comparison of childhood obesity among groups brings different complexities regarding genetic, physiological, cultural, socioeconomic, and environmental issues, and the interaction between these variables is not completely understood [
34].
Regarding physical activity, in Europe, immigrants and sons of immigrants have less tendency to be physically active and report a lower health status than nonimmigrants [
15,
43]. Among several possibilities, immigrant parents may face structural challenges (poor neighborhoods, busy schedules, language barriers) that makes difficult to have opportunities for physical activity [
35,
44]. Language is not expected to be a main barrier, because Portuguese is the main language in the Community of Portuguese-speaking countries. However, some local languages continue to be used by immigrants.
Portugal is among one of the countries where the Mediterranean diet-like pattern fits, which is characterized by a protective effect in health. Nevertheless, studies should be undertaken to better understand the adoption of this diet by immigrant communities, where the links with the country of origin through their families and culture may result in different findings.
Associations between childhood obesity and environmental characteristics highlight the importance of environmental determinants in urban areas and its relevance when delineating local and community interventions strategies in order to prevent childhood obesity [
36]. Although the complexity of the determinants of obesity point to several directions, with underlying causes such as social and cultural aspects [
13], in our study, it is highlighted that in the same condition, girls practice less sport outside the school and help slightly more their parents doing housekeeping than boys (in what regards to the parents’ origin). Still, little is known about gender-specific practices among immigrant parents and their children in Portugal. Some studies, in other settings, refer as plausible that immigrant parents may treat sons differently than daughters in leading to differences in the prevalence of overweight and obesity. Daughters may be more restricted than sons because of additional family obligations [
16,
45] and also by religious practices in some communities. Other studies alert for the social valorization of the overweight in African populations [
46]. In particular, for women, this may promote unhealthy eating behaviors.
Regarding eating practices, studies refer that the overall diet in the Portuguese children tends to be low in carbohydrates and high in sugars and fat [
35,
36,
37]. Dietary patterns that included eggs being reported to be consumed 1 or 2 times per week and fast food consumed occasionally or never were described by Rodrigues et al. [
47]. In other study, Rodrigues et al. [
48] found a lifestyle pattern that included sugar-sweetened beverages intakes (>2 times/week) was associated with the increased BMI and waist circumference. A recent work refers that in 7 out of the 24 countries analyzed, immigrant children are more likely to report very high levels of unhealthy eating (e.g., consumption of sweets and sugary drinks), with significant differences ranging from the low of 4.5 percentage points in Spain to the high of 8.7 points in Austria [
30]. Millar et al. [
49] studied immigrants from Sub-Saharan Africa in Australia and pointed out the replacement of traditional foods and an increased consumption of processed food and low ingestion of fiber. The same process is described in south Asians living in Europe [
50]. Migration may, therefore, entail other nutritional habits [
49,
50]. Other studies suggest that even the pattern and speed of change in diet may differ from country to country and that immigrants belonging to the same ethnic group may be at different levels in the acculturation process [
51,
52,
53,
54]. In our study, even though an extensive analysis of the children’s diet was not undertaken, reported data on consumption of eggs, fries, fast food, sweets, and soft drinks is higher form children with immigrant background. Age was also associated to fries, sweets, and soft-drinks intakes. The association between nutritional status and soft drink consumptions was particularly important for female. Silva et al. [
55] studied the effectiveness of the program to increase fruit/vegetable consumption and physical activity only in Portuguese children. Our study has a clear added value because it attempts to identify some aspects of immigrants’ health issues emphasizing the problem of overweight and obesity and abdominal obesity in children of immigrants in this municipality that may have an expression due to social and cultural background of their parents, adding to a growing body of literature that support local interventions focused on sex and culture specificity of immigrants. An open problem is also some variations with age. For example, considering children of immigrant mothers from low- and-middle-income countries, Zulfiqar et al. found sex-specific variations in prevalence with age, increasing more consistently for male than for female children [
56].
Some limitations and strengths should be referred. BMI cutoff points is a central issue requiring careful comparisons and interpretations. In addition, the definition of immigration status varies from study to study [
30]. An advantage of this study is related with measurements that were not self-reported but performed by technicians with ISAK certification, minimizing measurement errors [
27,
57]. However, eating habits, and practicing sports, among other, were self-reported by children primary caregiver and social desirability bias may be present. Data from 2009, may be a historical point to understand trends and processes at local level and contribute to inform researchers, policy makers, and public health practitioners about the evolution of prevalence of overweight and obesity. Additionally, it can be a baseline to future studies with children with immigration background to understand the nutrition transition at the community, household and individual level. Moreover, these children will be mothers and fathers in a near future. The impact of the ongoing introduction of several policies and measures in Portugal since 2010 also benefits from data collected before the implemented measures. For example, additional taxes on sugar drinks, a gradual decrease in the salt in bread, and prohibition on advertisement all food products, including beverages, with high energy values, salt, sugar, fatty acids, and processed fatty acids, to minors of 16 years old, is yet to be documented. Currently, most European countries, including Portugal, do not collect data systematically about the health status of immigrants. Better knowledge of the health of immigrants is essential to a country’s integration and health policies, but it is challenged by the lack of available data. Thus, at a local level, the study of successive generations can be useful to understand the acculturation process and risk factors in this particular setting or similar settings in order to offer guidance to health organizations to address the burden of obesity, its future comorbidities, and also monitoring some modified risk factors.






{kind=link}
{kind=link}
{kind=link}