1. Introduction
In 2016, the Lancet Commission on Adolescent Health and Wellbeing put together several prominent academics to discuss challenges and opportunities of action targeted to this specific population [
1]. Despite the interest on adolescence having increased in the last 30 years on many fronts, the World Health Organization (WHO) has highlighted that much more efforts should be done, globally and nationally, to improve the present and future health and wellbeing of individuals and communities by acting on this period of the life course [
2].
Several studies and actions have been focused on adolescents’ health problems related to sexual health, mental health, reproductive health, HIV, and other infectious diseases. On the contrary, adolescents present many silent and unmet needs related to lifestyle, nutrition, and physical activity, which also have social determinants [
3]. These needs, which are often neglected, occur when growing up in high and medium income countries that are non-communicable disease (NCD)-predominant; these diseases have increased over time [
4] and should have early prevention strategies among their priorities [
1]. Risks linked to the nutritional health of adolescents have become more and more relevant, with an increase of 120% in the prevalence of adolescent overweight or obesity from 1990 to 2016 [
4]. In many NCD-predominant countries, effective and structured health policies are needed to prevent obesity and address their risk factors in adolescence, when health-compromising habits and behaviors could be established [
2]. A lack of knowledge and, therefore, of tailored policy interventions is nowadays an obstacle to health prevention for this population, which has more and more access to unhealthy food products. Moreover, a lacking or insufficient investment in the health and wellbeing of adolescents can contribute to the erosion of the long-term and future quality of life of adolescents, as well as to the healthy start to life of the next generations [
5,
6,
7]. The WHO report “Health for the World’s Adolescents: A Second Chance in the Second Decade (H4WA)” showed that, globally, fewer than one in four adolescents meet recommendations for physical activity, and a great majority (80–90%) do not follow guidelines for nutrition-related behaviors (e.g., fruit and/or vegetable daily consumption); in some countries, as many as one adolescent in every three is obese [
2].
The success of health promotion interventions, intended in general to increase awareness and to improve behaviors related to the object of promotion, strongly depends on the engagement and activation of individuals [
8,
9,
10,
11] since, in the health promotion and prevention fields, the role of individuals (e.g., citizens, patients, and caregivers) in reaching health outcomes is key [
11,
12,
13]. Terms like co-production, shared decision-making, and participation are often used to indicate an evolution of the mutual role of public services’ providers and users who recognize and better use each other’s assets and resources for the success of public services [
14]. This is especially true in the public healthcare sector, where researchers and policy makers have been highlighting the opportunity for a reorientation of the systems towards collaborative processes in designing, organizing, and delivering public services [
12,
14,
15,
16,
17,
18,
19,
20]. Co-production is an approach that allows one to explore needs and habits and to build individual behaviors that can result in good health and wellbeing [
20,
21]. Service users can provide a fundamental contribution in designing, providing, and managing public services and/or in reaching their outcomes. There are several definitions of co-production. A key aspect of co-production regards the respective roles of professionals and users/patients in the co-production process. It was firstly identified as an “equal and reciprocal relationship using their services, their families and their neighbours” [
22]. Nabatchi and colleagues defined co-production as “an umbrella concept that captures a wide variety of activities that can occur in any phase of the public service cycle and in which state and lay actors work together to produce benefits” [
23]. ‘Co-working’ [
22] can be direct or indirect [
24], and it can be explicit or implicit [
20]. In this respect, the definition of co-production has evolved in the literature from co-working to co-design, co-management, co-delivery, and co-assessment as parts of a more comprehensive co-production approach [
25]. From this last perspective, the roles of the participants can assume different configurations rather than ‘an equal and reciprocal relationship’ [
22] between provider and user. The roles of professionals have been also seen as enablers or facilitators of people, who are seen as active agents [
12,
26,
27]. Thus, in this perspective, co-producing is not about transferring responsibility to the health care services’ users but rather about sharing responsibilities [
16] and putting people in the right conditions to produce value for themselves and their community [
9]. Therefore, co-production implies looking at patients, and, more in general, at people as potential partners, as well as looking at their skills, expertise, and abilities as under-used assets in the system—this acknowledgment can open co-production dynamics between former providers and former users [
28].
Co-production is recognized as an effective way to design more successful health promotion and prevention interventions [
29]. Co-production implies sharing resources (including knowledge) and legitimacy (including power) between providers and users. For these reasons, the involvement of service users is needed to enable service innovation [
20,
30]. Scholars from both the public administration and management field and the service management field have argued that an involuntary co-production process is embedded into any kind of public service provision due to the interactions between service providers and service users [
20,
31,
32,
33,
34]. This may be intended as intrinsic or involuntary co-production. In this respect, health is, by definition, a co-produced value: the role and responsibility of people in reaching good health outcomes and, in general, good health conditions are crucial [
9]. The educational services provided within health promotion initiatives are mostly characterized by an overlapping of service production and consumption due to the interaction between knowledge producers and users. Thus, it can be also argued that these services are always co-produced. Nevertheless, this intrinsic co-production typically consists of an interaction where experts teach (provide) and users learn (get/receive) [
35]. Educational services embedded into health promotion interventions are usually based on traditional methods of education not encompassing co-production processes based on collaboration or co-working. For example, traditional educational actions targeted to adolescents are held as lectures by healthcare professionals/experts in educational environments [
36]. When based on these passive mechanisms, educational services often fail in producing behavioral changes [
37].
According to Osborne and colleagues [
20], in addition to the involuntary and embedded co-production as the creation of value-in-use during usage, there is a voluntary co-production, which means collaborative and dialogical interactions between service providers and users during planning processes, service provisions, and service assessments. In this research, the authors refer to the explicit or voluntary nature of co-production that, in the framework of Osborne and colleagues [
20], always implies the active involvement of service users and is defined as co-design at the individual level and co-innovation at the system level. Co-design ‘is about improving the performance of existing public services by actively involving the service user in their design, evaluation, and improvement’ [
20]. Co-innovation encompasses the ‘involvement of the service users not just in the improvement of existing services but rather in the co-innovation’ of the service ‘within the holistic service system and upon novel combinatory means to improve such service delivery’ [
20]. The literature suggests that, on the one hand, explicit co-production processes in the healthcare sector, especially in the health promotion and prevention fields, is key because the role of individuals (e.g., citizens, patients, and caregivers) in reaching the health outcomes is self-evident [
8,
9,
10]; on the other hand, explicit or voluntary co-production mechanisms can also enhance people and patients’ education [
10,
11,
38]. Users can provide various different inputs for service production, e.g., their preferences, ideas, knowledge, and competencies. In addition to the “learned expertise” of educators, the “lived experience” of individuals can be a key asset in the co-production processes of public services [
39,
40,
41,
42,
43]. Co-production can result from ‘more intensive’ interactions [
44] where users can actually act as ‘prosumers’ or ‘consummators’ or, in other words, knowledge/information producers and consumers at the same time [
32,
45,
46,
47]. Participation mechanisms in educational contexts can be enabled by ‘reverse teaching methods’ or ‘flipped classrooms,’ which are user-driven and give participants a central role in the learning process [
48,
49,
50]. In these collaborative methods based on ‘learning-by-doing’ processes, participants can take part in real—and possibly challenging—experiences of learning [
49,
51]. The ‘role sharing’ between provider (teacher) and user (recipient) is a fundamental aspect in these processes, improving the retention of contents and producing better outcomes [
52] such as making what was learnt actionable and changing individual behaviors [
8,
51,
53]. Some authors have argued for a ‘replacing’ or ‘integrative’ role of users in respect to public servants or employees who generally deliver the intervention [
12,
54]. More user-centered education that increasingly engages users can produce better outcomes than traditional methods, including in healthcare contexts [
10,
38,
55]. Keeping adolescents engaged in health promotion initiatives is a key challenge [
56]. In this respect, scholars have argued that, when adolescents co-create health interventions, they are more likely to actively engage with the same intervention in the long-term. According to Raeside and colleagues, the potential effectiveness of co-creation, youth advocacy, and use of digital technologies for health promotion interventions in adolescents should be tested [
57].
1.1. Evaluating Co-Production: The Framework
In order to advance the study and practice of co-production, the available literature suggests several variables to consider in evaluating initiatives [
14,
58,
59,
60,
61,
62]:
Characteristics and determinants (inputs), meaning:
- ○
Characteristics of the co-production process, including: actors/participants involved, recruitment, voluntary participation and/or motivations for engagement, nature and typologies of interactions.
- ○
Determinants for the implementation of the initiative, such as: conditions in the broader system context, drivers for creation and implementation of co-production processes.
Goals and expected intermediate (outputs).
Final (outcomes) results, and their measurement/evaluation: effectiveness, efficacy, and impacts of activities in relation to wider societal outcomes (social/public value).
Despite the claims of the potential impact of co-production as a mechanism for creating more value in the public sector, evaluations of co-production initiatives are rare in the literature [
59,
61,
63]. Most scientific contributions on the co-production of public services do not mention a specific goal of the study because of the a priori assumption that co-production is a normative good [
20,
59]. Few empirical studies have described and discussed the co-production process [
64]. Research on co-production has marginally focused on the role of service professionals [
20]. Given the lack of evaluations of public co-production initiatives, scholars have called for more empirical research [
58] that also considers the costs and challenges of co-production in relation to traditional initiatives [
65]. In fact, on the practical side, research on the direct and indirect costs of co-production is still needed [
66]. The research agenda on public co-production suggests moving the discussion from the co-production process alone to the evaluation of its outcomes in terms of cost-effectiveness, services’ quality improvement, impacts, and value produced to different stakeholders [
58,
59,
62,
63].
1.2. Aims
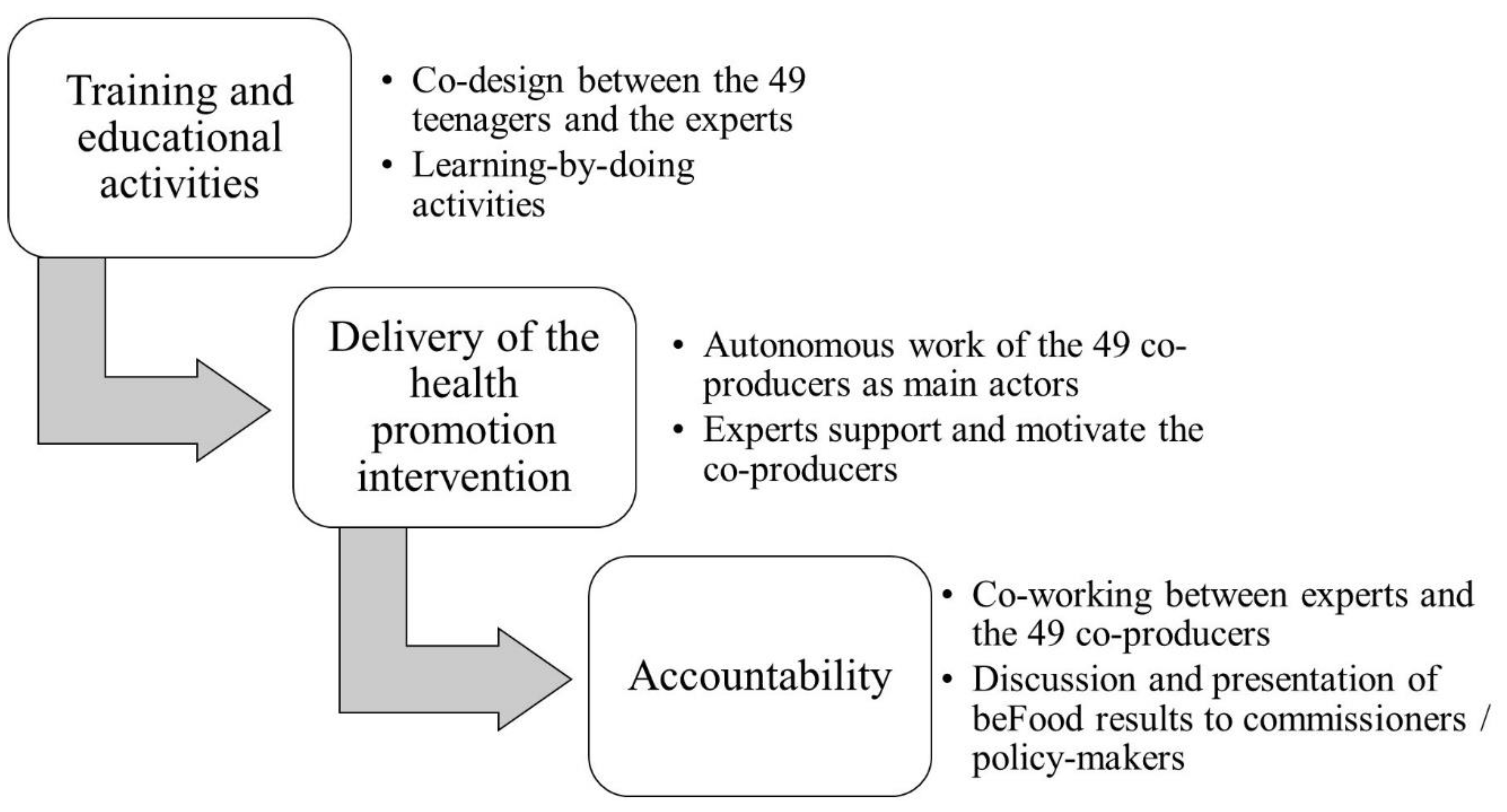
Given these premises, the paper presents the design, dynamics, and results of a co-production experience in Tuscany (Italy) called beFood. This was a public intervention of healthy lifestyle promotion conducted with adolescents for the early prevention of obesity and overweight [
67]. The paper aimed to analyze whether and how applying a co-production approach to an intervention for promoting healthy lifestyle among adolescents could be effective and efficient while considering its impact on both co-producers and the wider society. The authors also describe how public healthcare organizations might enable these value co-production processes by reshaping the role of public servants and giving them different responsibilities. To this end, an evaluation of a public health-promotion initiative co-produced and co-delivered with adolescents (beFood) was conducted regarding:
- (i)
Design and implementation processes, meant as input factors.
- (ii)
Outputs of the co-production approach in terms of intermediate results, such as quality of the process and the development of knowledge and skills of co-producers.
- (iii)
Behavioral and economic outcomes—more precisely, the economic evaluation investigated whether the adoption of beFood as the standard approach for institutional health promotion initiatives was more efficient than traditional approaches.
4. Discussion
Adolescence is one of the best periods to work at redefining actual behaviors or creating new habits that can be present and reinforced during adulthood [
1,
81]. Thus, interventions aimed at improving healthy habits should be adopted in this early period of the life course, a starting point to have a long-term impact on the adolescents’ health and wellbeing [
6,
82].
The authors evaluated the results of beFood, a health promotion intervention co-produced and co-delivered with adolescents. beFood showed that an action of lifestyle promotion based on a co-production approach could be effective and efficient when targeting adolescents. Its effectiveness was related both to outputs, such as empowering adolescents as agents of change, and outcomes, such as reaching a very high number of peers, activating a potential viral effect, and freeing up public resources. Considering that few studies have been published on the impact of co-production [
59,
66], this paper fills in this gap by providing the results of an evaluation performed at different levels (determinants, intermediate results, and final results) and for different stakeholders (the organization/provider, the participant people, and the wider community), with a specific focus on obesity prevention in adolescence by means of lifestyle promotion.
In the presented intervention, both competitive and collaborative dynamics were activated between and within co-producers’ subgroups as an incentive for their participation and engagement [
83]. Autonomy and responsibility were important aspects in co-production [
84] that empowered the 49 adolescents and helped them develop their roles of healthy lifestyle promoters. In this way, a very high number of adolescents was reached with a personalized healthy message, thanks also to the use of digital technologies [
57]. This shows that co-production can multiply size and impact of health promotion initiatives, producing a wider value. The results of beFood also suggest that the co-producers can generate spreading mechanisms of activation towards and above the people they ‘served,’ thus acting as ‘public co-servants’ in producing public value.
In a recent review, co-production interventions for children in primary schools were found to be effective in improving students’ knowledge acquisition [
85]. In a study on the Scottish initiative ‘Thinking Differently,’ involving young people in a research project on how to prevent or address alcohol misuse, the co-working with researchers was reported as a key aspect in the process of empowerment of co-producers into agents of change [
86]. This evidence confirmed that the input variables related to the design, organization, and implementation of the co-production approach can be key determinant factors for the effectiveness of the co-produced initiative.
Consistent with the literature [
12,
20,
87], value was produced in beFood as a mix of private and public forms that were firstly achieved by creating personal value for the individual participant adolescents (e.g., knowledge, skills, personal development, and more healthy behaviors) for whom the process of co-production was intrinsically of value [
62]. They, in turn, both contributed to increases of the impact, efficiency, and effectiveness of the public service intervention, and they were enabled and empowered in producing public and social value (e.g., knowledge and behaviors in the wider community), now and possibly in the future [
20].
Looking at the system or provider side, beFood provides evidence for the effectiveness and efficiency of the co-production approach, confirming other studies [
14] and pushing for a wider use of co-production in addressing obesity-related issues in adolescence. This is an interesting result, considering the absence of strong evidence on comparative evaluation related to co-production in general and in the field of health promotion initiatives targeted to adolescents in particular [
65]. A recent research piece compared the outcomes (hospitalizations and medications’ use) of co-produced mental health services with those of traditional day centers by providing empirical evidence on the preventive effect and the effectiveness of co-produced mental health services [
88].
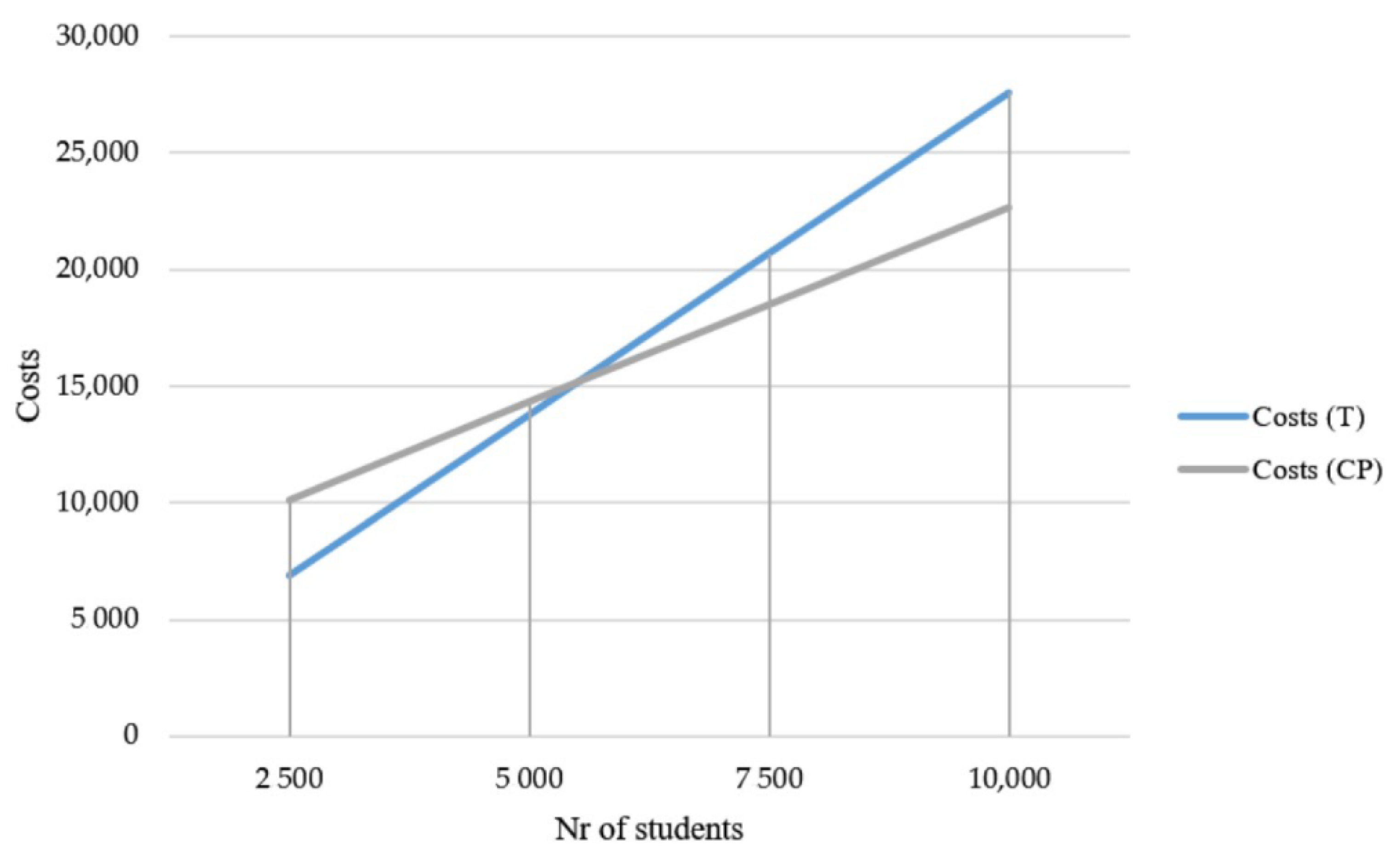
The co-production approach has also been seen as a way to reduce costs, better allocate resources, and, thus, improve efficiency [
89,
90,
91]. In this respect, the efficiency of beFood was made explicit through the opportunity–cost analysis in this study. A scaling-up of the beFood approach at the system level as an institutional health promotion strategy was shown to be more convenient than traditional methods. The savings were increasingly evident for a higher number of targeted individuals and, in particular, adolescents, especially when considering the additional viral effect that the co-production process could produce. Co-production may represent a significant opportunity to reallocate resources within public services or to increase productive capacity when resources are limited. A beFood-like co-production approach may allow for the reallocation of about 3382 h of health professionals’ time onto other public services. This result confirms the little evidence currently available in the literature on this topic. In an older research article, it was reported that the involvement of lay people can increase the cost-efficiency of municipal services delivery by increasing the services’ outputs with the same costs or decreasing the production costs with the same outputs in respect to traditional delivery models [
90]. Similarly, in the above-mentioned initiative, ‘Thinking Differently’ [
86], the engagement of lay people in project activities constituted almost 80% of all unpaid time inputs [
92]. The findings from the opportunity–cost analysis of the beFood initiative confirmed that co-production could produce significant economic benefits and opportunities regarding the reallocation of input resources.
In order to adopt the co-production approach and co-innovate in addressing obesity, several changes and adaptations are needed in regard to how health promotion services are organized and managed [
64,
84]. Though little attention has been payed to the role of service professionals in the co-production literature [
20], it is essential to innovate the role of public servants in order to augment the effectiveness of interventions. As reported in other educational-related initiatives of co-production, investing in the training of educational services providers is key to gain their collaboration and overcome resistance [
85]. In beFood, public servants can be considered ‘inputs’ in the co-production process [
9], and they can also be considered enablers and facilitators for engaging people in the process of value co-creation [
12]. A beFood-like co-production approach implies a voluntary shift of responsibilities and power from providers to users. This role-blurring is based on the mutual trust and acknowledgment of skills, knowledge, and capabilities, as well as on the consequent interdependence in the provision of the public service [
93]. The partnership was a main determinant in achieving better outcomes and higher efficiency [
17,
94]. Healthcare workers involved in health promotion initiatives should be trained and encouraged to work in a people-driven way [
64].
Considering the potential viral-effect of the co-production approach, more research is needed to understand how healthcare services should be organized to support the value chain of the spreading mechanism that such approaches can stimulate.
This study was based on the measurement of short-time outcomes. Further research is needed in order to provide evidence on the longer-term outcomes and costs of applying a beFood-like co-production approach in promoting healthy lifestyle with adolescents [
95]. Moreover, this study was based on a single case study design that did not provide comparative results [
96]. beFood was held in a specific context (Tuscany, Italy). The design and implementation of its co-production approach should be adjusted to be reproduced. However, it was evaluated using a set of key variables and indicators that could be applied to other co-production activities [
58], thus allowing for comparisons.





{kind=link}
{kind=link}