Vitamin D and Calcium Milk Fortification in Pregnant Women with Periodontitis: A Feasibility Trial

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Randomisation Procedures, and Ethics
2.2. Setting
2.3. Eligibility
2.4. Study Intervention Groups and Blinding
- Group 1—consumption of one sachet with powdered milk fortified with calcium and vitamin D twice a day and PT throughout gestation (early therapy).
- Group 2—consumption of a placebo sachet with powdered milk (plain milk) twice a day and PT throughout gestation.
- Group 3—consumption of one sachet with powdered milk fortified with calcium and vitamin D twice a day and PT after childbirth (late therapy).
- Group 4—consumption of a placebo sachet with powdered milk twice a day and PT after childbirth.
2.5. Outcomes and Data Sources
3. Parallel Process Evaluation
4. Analysis
5. Results
Qualitative Findings
6. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
The Trial Registration Number and Trial Register
References
- Offenbacher, S.; Barros, S.P.; Beck, J.D. Rethinking Periodontal Inflammation. J. Periodontol. 2008, 79, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-de-Albornoz, A.; Figuero, E.; Herrera, D.; Bascones-Martínez, A. Gingival changes during pregnancy: II. Influence of hormonal variations on the subgingival biofilm. J. Clin. Periodontol. 2010, 37, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Carrillo-de-Albornoz, A.; Martín, C.; Tobías, A.; Herrera, D. Effect of pregnancy on gingival inflammation in systemically healthy women: A systematic review. J. Clin. Periodontol. 2013, 40, 457–473. [Google Scholar] [CrossRef] [PubMed]
- González-Jaranay, M.; Téllez, L.; Roa-López, A.; Gómez-Moreno, G.; Moreu, G. Periodontal status during pregnancy and postpartum. PLoS ONE 2017, 12, e0178234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Grath, C.; Bedi, R. Public dental health: Can dental attendance improve quality of life? Br. Dent. J. 2001, 190, 262–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambrone, L.; Guglielmetti, M.R.; Pannuti, C.M.; Chambrone, L.A. Evidence grade associating periodontitis to preterm birth and/or low birth weight: I. A systematic review of prospective cohort studies. J. Clin. Periodontol. 2011, 38, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Pannuti, C.M.; Guglielmetti, M.R.; Chambrone, L.A. Evidence grade associating periodontitis with preterm birth and/or low birth weight: II. A systematic review of randomized trials evaluating the effects of periodontal treatment. J. Clin. Periodontol. 2011, 38, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Gatto, R.; Monaco, A. Relationship between Periodontitis and Pre-Eclampsia: A Meta-Analysis. PLoS ONE 2013, 8, e71387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteves Lima, R.P.; Cyrino, R.M.; de Carvalho Dutra, B.; Oliveira da Silveira, J.; Martins, C.C.; Miranda Cota, L.O.; Costa, F.O. Association Between Periodontitis and Gestational Diabetes Mellitus: Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 48–57. [Google Scholar] [CrossRef]
- da Silva, H.E.C.; Stefani, C.M.; de Santos Melo, N.; de Almeida de Lima, A.; Rösing, C.K.; Porporatti, A.L.; Canto, G.D.L. Effect of intra-pregnancy nonsurgical periodontal therapy on inflammatory biomarkers and adverse pregnancy outcomes: A systematic review with meta-analysis. Syst. Rev. 2017, 6, 197. [Google Scholar] [CrossRef] [Green Version]
- Xiong, X.; Buekens, P.; Goldenberg, R.L.; Offenbacher, S.; Qian, X. Optimal timing of periodontal disease treatment for prevention of adverse pregnancy outcomes: Before or during pregnancy? Am. J. Obstet. Gynecol. 2011, 205, 111.e1–111.e6. [Google Scholar] [CrossRef]
- Adegboye, A.R.; Boucher, B.J.; Kongstad, J.; Fiehn, N.E.; Christensen, L.B.; Heitmann, B.L. Calcium, vitamin D, casein and whey protein intakes and periodontitis among Danish adults. Public Health Nutr. 2016, 19, 503–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bothwell, L.E.; Podolsky, S.H. The Emergence of the Randomized, Controlled Trial. N. Engl. J. Med. 2016, 375, 501–504. [Google Scholar] [CrossRef] [Green Version]
- Adegboye, A.R.A.; Cocate, P.G.; Benaim, C.; da Veiga Soares Carvalho, M.C.; Schlüssel, M.M.; de Castro, M.B.T.; Kac, G.; Heitmann, B.L. Recruitment of low-income pregnant women into a dietary and dental care intervention: Lessons from a feasibility trial. Trials 2020, 21, 244. [Google Scholar] [CrossRef] [Green Version]
- Cocate, P.G.; Kac, G.; Heitmann, B.L.; Nadanovsky, P.; da Veiga Soares Carvalho, M.C.; Benaim, C.; Schlüssel, M.M.; de Castro, M.B.T.; Alves-Santos, N.H.; Baptista, A.F.; et al. Calcium and vitamin D supplementation and/or periodontal therapy in the treatment of periodontitis among Brazilian pregnant women: Protocol of a feasibility randomised controlled trial (the IMPROVE trial). Pilot Feasibility Stud. 2019, 5, 38. [Google Scholar] [CrossRef] [Green Version]
- Thabane, L.; Hopewell, S.; Lancaster, G.A.; Bond, C.M.; Coleman, C.L.; Campbell, M.J.; Eldridge, S.M. Methods and processes for development of a CONSORT extension for reporting pilot randomized controlled trials. Pilot Feasibility Stud. 2016, 2, 25. [Google Scholar] [CrossRef] [Green Version]
- McCormick, S.A.; Vatter, S.; Carter, L.-A.; Smith, S.J.; Orgeta, V.; Poliakoff, E.; Silverdale, M.A.; Raw, J.; Ahearn, D.J.; Taylor, C.; et al. Parkinson’s-adapted cognitive stimulation therapy: Feasibility and acceptability in Lewy body spectrum disorders. J. Neurol. 2019, 266, 1756–1770. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Costalonga, M.; Herzberg, M.C. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol. Lett. 2014, 162, 22–38. [Google Scholar] [CrossRef] [Green Version]
- Merchant, A.T. Periodontitis and Dental Caries Occur Together. J. Evid. Based Dent. Pract. 2012, 12, 18–19. [Google Scholar] [CrossRef]
- Mattila, P.T.; Niskanen, M.C.; Vehkalahti, M.M.; Nordblad, A.; Knuuttila, M.L.E. Prevalence and simultaneous occurrence of periodontitis and dental caries. J. Clin. Periodontol. 2010, 37, 962–967. [Google Scholar] [CrossRef]
- Vettore, M.V.; de Amorim Marques, R.A.; Peres, M.A. Desigualdades sociais e doença periodontal no estudo SBBrasil 2010: Abordagem multinível. Rev. Saude Publica 2013, 47 (Suppl. 3), 29–39. [Google Scholar] [CrossRef] [Green Version]
- Kamp Dush, C.M.; Yavorsky, J.E.; Schoppe-Sullivan, S.J. What Are Men Doing while Women Perform Extra Unpaid Labor? Leisure and Specialization at the Transitions to Parenthood. Sex Roles 2018, 78, 715–730. [Google Scholar] [CrossRef]
- Olshansky, E.F. Women’s Health and Wellness Across the Lifespan. Choice Review Online. 2015. Available online: http://choicereviews.org/review/10.5860/CHOICE.190644 (accessed on 20 August 2020).
- White, J.H. Vitamin D signaling, infectious diseases, and regulation of innate immunity. Infect. Immun. 2008, 76, 3837–3843. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.N.; Hildebolt, C.F.; Miley, D.D.; Dixon, D.A.; Couture, R.A.; Anderson Spearie, C.L.; Langenwalter, E.M.; Shannon, W.D.; Deych, E.; Mueller, C.; et al. One-Year Effects of Vitamin D and Calcium Supplementation on Chronic Periodontitis. J. Periodontol. 2011, 82, 25–32. [Google Scholar] [CrossRef]
- Asemi, Z.; Samimi, M.; Siavashani, M.A.; Mazloomi, M.; Tabassi, Z.; Karamali, M.; Jamilian, M.; Esmaillzadeh, A. Calcium-Vitamin D Co-supplementation Affects Metabolic Profiles, but not Pregnancy Outcomes, in Healthy Pregnant Women. Int. J. Prev. Med. 2016, 7, 49. [Google Scholar]
- Adegboye, A.R.; Twetman, S.; Christensen, L.B.; Heitmann, B.L. Intake of dairy calcium and tooth loss among adult Danish men and women. Nutrition 2012, 28, 779–784. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Indicators | Threshold | Data Source | Descriptive Outcome | Decision |
|---|---|---|---|---|
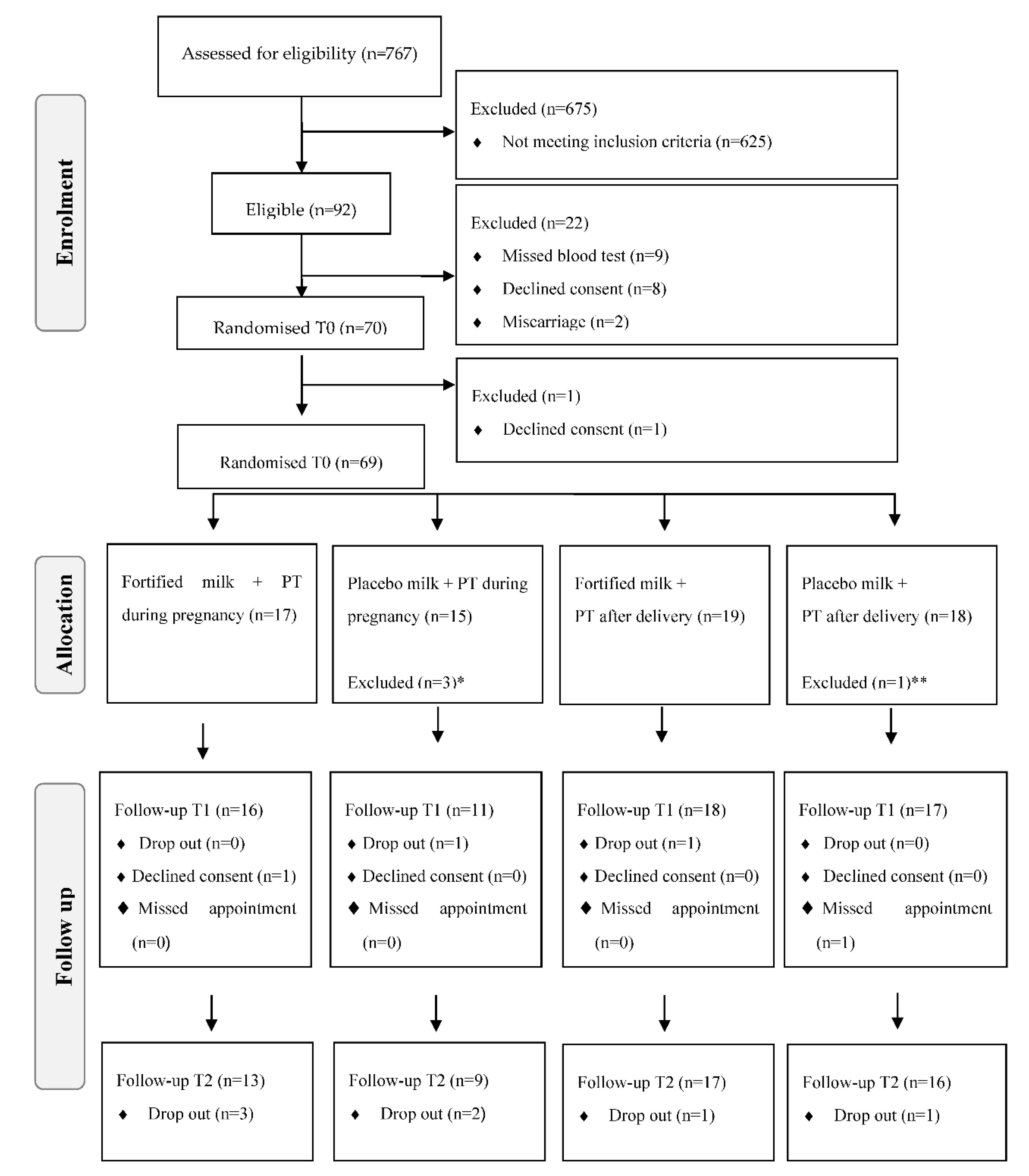
| Eligibility rate a N of eligible participants/total n of participants referred to the study | A: ≥15% M: 15–10% R: <10% | Recruitment screening log | 767 women were referred and 92 were considered eligible after dental screening. Eligibility rate was 12% | Modify |
| Participation rate a N of randomised participants/n of eligible participants after dental screening | A: ≥75% M: 74–70% R: <70% | Recruitment screening log | 92 women were eligible after dental screening and 70 were randomised. Participation rate was 76.1% | Accept |
| Recruitment rate a N of randomised participants/total n of recruitment weeks | A: ≥1.7 women/week M: 1–1.6 women/week R: <1 women/week | Recruitment screening and participant flow logs | Actual recruitment of 2 women/week (70 randomised women in 32 weeks) | Accept |
| Retention rate N of randomised participants remaining in the study/total n of randomised participants | A: ≥80% M: 79–70% R: <70% | Participant flow log | In total, 70 women were randomised. 69 women remained at the baseline, 62 in the 2nd follow-up and 55 in the 3rd follow-up Retention rate: 78.6% | Modify |
| Adherence to milk consumption N sachets consumed/total n of sachets provided to participants | A: ≥80% M: 79–60% R: <60% | Participant flow log | Fortification group: 82.4% Placebo group: 88.1% Overall:85.2% | Accept |
| Adherence to periodontal therapy N of therapy sessions completed per PT group/total n of therapy sessions offered per PT group | A: ≥70% M: 69–60% R: <60% | Participant flow log | Early PT group: 98.8% | Accept |
| Tolerability of intervention N of serious adverse events related to the intervention | A: no events M: tolerable for the majority of participants R: any serious adverse event related to the intervention | Routine phone calls Field notes Blood test results | No adverse event reported | Accept |
| Acceptability of random allocation N of randomised participants accepting recruitment allocation | A: ≥95% M: 94–90% R: < 90% | Participant flow log Field notes | All randomised participants accepted their allocated group (100% acceptability) | Accept |
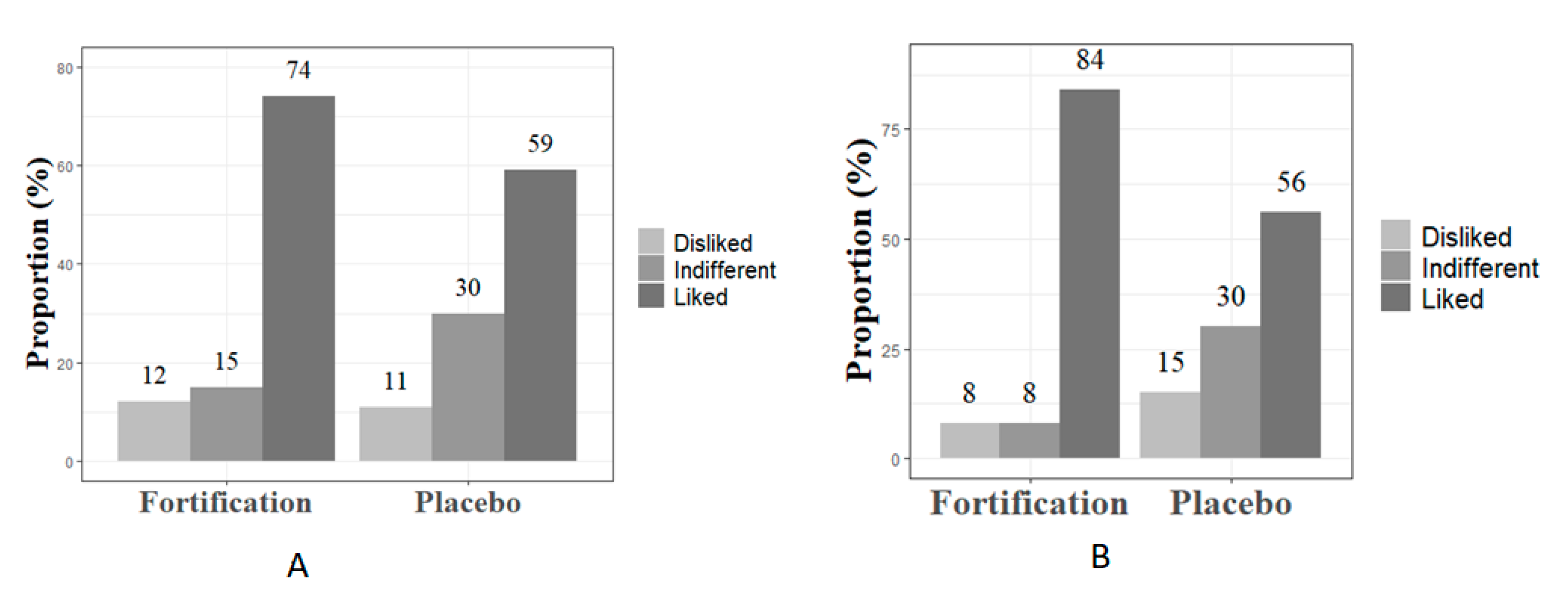
| Acceptability of milk consumption b N of participants who liked the milk in T0 and T1/total n of participants who answered the questionnaire in T0 and T1 | A: ≥90% M: 89–70% R: <70% | Study questionnaire | T0 74% in the fortification group liked the milk 59% in the placebo group liked the milk T1 84% in the fortification group liked the milk 56% in the placebo group liked the milk | Modify for the fortified group Reject for the placebo group |
| Balanced groups at baseline The ability of random sequence generation to produce comparable groups | A: no sig differences M: 1–2 sig differences R: >2 sig differences | Descriptive statistics | No significant differences in the main socio-demographic characteristics | Accept |
| Blinding N of un-blinding cases reported by the trial coordinator/total n of randomised participants | A: <10% M: 10%–15% R: ≥15% | Field notes | No un-blinding cases reported | Accept |
| Feasibility of data collection Reported ability of researchers of applying questionnaires and complete activities on the study protocol | A: no major reported difficulty M: few minor reported difficulties R: any major reported difficulty | Field notes End-of-study evaluation survey | No reports of difficulties | Accept |
| Tolerability of data collection and study participation N of complaints related to taking part in the study (visits to the centre, filling up questionnaires, blood tests, etc.) | A: no major complaint M: few minor complaints R: any major complaint | Field notes | No participant reported any major complaints on feeling burdened or frustrated with data collection or taking part in the study | Accept |
| Variables a | Total | Early PT (during Pregnancy) | Late PT (After Delivery) | p -Value d | ||
|---|---|---|---|---|---|---|
| Plain Milk | Fortified Milk | Plain Milk | Fortified Milk | |||
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | ||
| Age (year) | 28.0 (7.0) | 29.5 (6.0) | 28.0 (9.0) | 25 (10.0) | 29.0 (7.0) | 0.51 |
| Gestational age (week) | 15.0 (5.0) | 14.5 (5.0) | 16.0 (2.0) | 13.0 (4.0) | 16.0 (5.0) | 0.17 |
| Education (year) | 12.0 (3.0) | 12.0 (2.0) | 12.0 (3.0) | 11.0 (4.0) | 11.0 (2.0) | 0.96 |
| Monthly per-capita b income (USD) | 126.7 (94.9) | 147.8 (93.3) | 100.0 (69.1) | 126.7 (207.5) | 151.6 (131.6) | 0.19 |
| Pre-pregnancy BMI (kg/m2) | 26.3 (9.5) | 25.9 (8.3) | 23.9 (8.5) | 22.4 (12.8) | 28.6 (7.7) | 0.77 |
| Pocket depth (mm) c | 4.2 (0.3) | 4.2 (0.4) | 4.3 (0.3) | 4.2 (0.3) | 4.2 (0.4) | 0.50 |
| Clinical attachment loss (mm) c | 4.2 (0.3) | 4.3 (0.4) | 4.3 (0.3) | 4.2 (0.2) | 4.2 (0.3) | 0.81 |
| Sites with bleeding on probing (%) c | 16.0 (21.0) | 23.0 (31.0) | 19.0 (11.0) | 16.0 (17.0) | 12.0 (14.0) | 0.36 |
| N (%) | p-Value e | |||||
| Marital status | ||||||
| Living with partner | 60 (87.0) | 16 (88.9) | 13 (76.5) | 13 (86.7) | 18 (94.7) | 0.43 |
| Other f | 9 (13.0) | 2 (11.1) | 4 (23.5) | 2 (13.3) | 1 (5.3) | |
| Self-reported skin colour | 0.38 | |||||
| White | 10 (14.5) | 3 (16.7) | 3 (17.6) | - | 2 (10.5) | |
| Other | 59 (85.5) | 15 (83.3) | 14 (82.3) | 15 (100.0) | 17 (89.5) | |
| Parity g | 0.86 | |||||
| 0 | 24 (34.8) | 5 (33.3) | 7 (41.2) | 5 (27.7) | 7 (36.8) | |
| ≥1 | 45 (65.2) | 10 (66.6) | 10 (58.8) | 13 (72.2) | 12 (63.1) | |
| Current smoker | 0.82 | |||||
| No | 61 (88.4) | 16 (88.9) | 16 (94.1) | 13 (86.7) | 16 (84.2) | |
| Yes | 8 (11.6) | 2 (11.1) | 1 (5.9) | 2 (13.3) | 3 (15.8) | |
| Alcohol consumption | 0.89 | |||||
| No | 57 (82.6) | 15 (83.3) | 15 (88.2) | 12 (80.0) | 15 (78.9) | |
| Yes | 12 (17.4) | 3 (16.7) | 2 (11.7) | 3 (20.0) | 4 (21.0) | |
| Variables | Pregnant Women | p-Value a | |
| Complete (Three Measures) N = 55 | One or Two Measures N = 15 | ||
| Median (IQR) | Median (IQR) | ||
| Age (years) | 29.0 (8.0) | 25.0 (8.0) | 0.115 |
| Gestational age (weeks) | 16.3 (4.7) | 16.4 (3.1) | 0.517 |
| Schooling (years) | 12.0 (2.0) | 11.0 (4.0) | 0.270 |
| Monthly per-capita income (USD) b | 130.0 (104.9) | 124.75 (140.0) | 0.621 |
| Prepregnancy BMI (kg/m2) | 27.6 (9.5) | 22.7 (8.4) | 0.161 |
| Variables | n (%) | n (%) | p-Value c |
| Marital status | 0.077 | ||
| Living with partner | 49 (90.7) | 11 (73.3) | |
| Other d | 5 (9.3) | 4 (26.7) | |
| Self-reported skin colour | 0.500 | ||
| White | 7 (13.0) | 1 (6.7) | |
| Black or mixed | 47 (87.0) | 14 (93.3) | |
| Parity | 0.894 | ||
| 0 | 19 (35.2) | 5 (33.3) | |
| ≥1 | 35 (64.8) | 10 (66.7) | |
| Alcohol | |||
| No | 47 (87.0) | 10 (66.7) | 0.066 |
| Yes | 7 (13.0) | 5 (33.3) | |
| Current smoker | |||
| No | 50 (91.0) | 11 (78.6) | 0.34 |
| Yes | 5 (9.0) | 3 (21.4) | |
| Category | Sub-Categories | Factors | Quotes |
|---|---|---|---|
| Dietetics and culinary skills |
| Favourable: Preparation was considered easy. Women reported consumption of smoothies (milk blended with fruits). Women had basic utensils at home for simple recipes (porridges and smoothies), but the provision of a shaker bottle helped with the preparation. Unfavourable: dislike of the test of pure milk; consumption of milk daily was considered monotonous. | “In the beginning, it was very difficult to adapt to taking it twice and at the end of the pregnancy, I was already sick. Sometimes I took it pure but I got tired of it. Mixing with fruits, yogurt or in the porridge is much better.” “I add the milk powder, sachet and powdered cereal in the saker and carry it with me. I always have a bottle of water and the shaker is very handy.” |
| Favourable: milk was considered a healthy food. Unfavourable: Some women reported nausea when consuming milk and sachet. | “In the beginning, it was very good because I was not eating, I was’ losing weight. So for me, milk was my only food. Milk is good for our health. Vitamins and milk are good for the baby.” “I was vomiting in the beginning. I could not take it. Now it is okay.” | |
| Sharing of food with other family members |
| Favourable: Provision of whole milk to the children prevented the sharing of the milk provided to women with their family. Unfavourable: Some women shared milk and sachets with their children. Sharing was sporadic and related to children’s curiosity. | “I gave it to my son. He just wanted to taste it.” “The children like milk but I did not share my mine with them. They had their milk.” |
| Health care needs |
| Favourable: Women reported a positive outcome after PT. Women considered dentists competent. Women trusted health care professionals. Unfavourable: Women complained about discomfort and pain during the PT. | “It hurts but it very good (…) my teeth are now sparkling clean.” “I felt discomfort but it was bearable.” “I see amazing results.” “The dentist was excellent.” “Everybody there is nice. She explained how to use dental floss. I have never used it properly.” |
| Favourable: refund of transportation cost and home delivery of milk was appreciated by the women. Unfavourable: Lack of money; lack of safety and fear of violence; competing priorities prevented women to attend the visits. | “I avoid going there too often because of the lack of security in the area.” “There are times when I do have money at home to go to the health centre.” “Home delivery was convenient. It is difficult to go out when you are busy and have kids at home.” | |
| Social support network |
| Favourable: Some women had support from their mothers, the father of the baby or wider family. Unfavourable: Some women lacked support from their mothers, the father of the baby, or wider family | “(…) I count on my mum to stay with my daughter when I go to the health centre.” “I have my mum. She helps me a lot. (…) She reminds me to take the milk.” “I do not have anybody to help with my kids. I leave them at school. I manage things on my own.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues Amorim Adegboye, A.; Dias Santana, D.; Guedes Cocate, P.; Benaim, C.; Teixeira dos Santos, P.P.; Heitmann, B.L.; da Veiga Soares Carvalho, M.C.; Maia Schlüssel, M.; Trindade de Castro, M.B.; Kac, G. Vitamin D and Calcium Milk Fortification in Pregnant Women with Periodontitis: A Feasibility Trial. Int. J. Environ. Res. Public Health 2020, 17, 8023. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218023
Rodrigues Amorim Adegboye A, Dias Santana D, Guedes Cocate P, Benaim C, Teixeira dos Santos PP, Heitmann BL, da Veiga Soares Carvalho MC, Maia Schlüssel M, Trindade de Castro MB, Kac G. Vitamin D and Calcium Milk Fortification in Pregnant Women with Periodontitis: A Feasibility Trial. International Journal of Environmental Research and Public Health. 2020; 17(21):8023. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218023
Chicago/Turabian StyleRodrigues Amorim Adegboye, Amanda, Danilo Dias Santana, Paula Guedes Cocate, Camila Benaim, Pedro Paulo Teixeira dos Santos, Berit Lilienthal Heitmann, Maria Cláudia da Veiga Soares Carvalho, Michael Maia Schlüssel, Maria Beatriz Trindade de Castro, and Gilberto Kac. 2020. "Vitamin D and Calcium Milk Fortification in Pregnant Women with Periodontitis: A Feasibility Trial" International Journal of Environmental Research and Public Health 17, no. 21: 8023. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218023