Comorbidity in Older Patients Hospitalized with Cancer in Northeast China based on Hospital Discharge Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Source
2.2. Statistical Analysis
3. Results
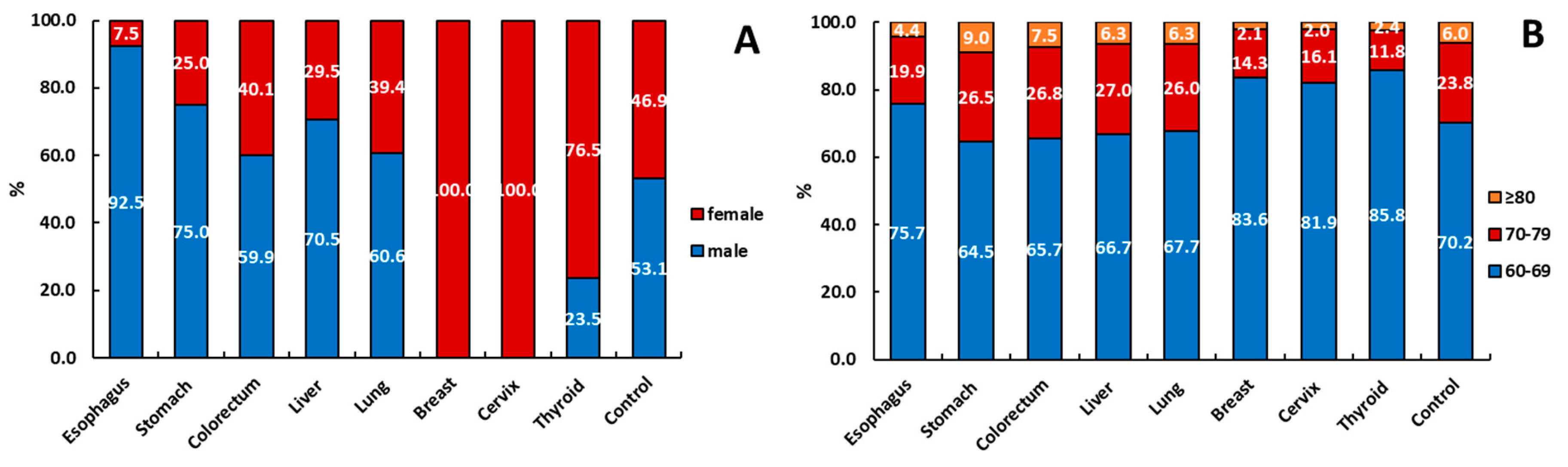
3.1. Patient Statistics
3.2. Comorbidity Prevalence and Prevalence Ratios
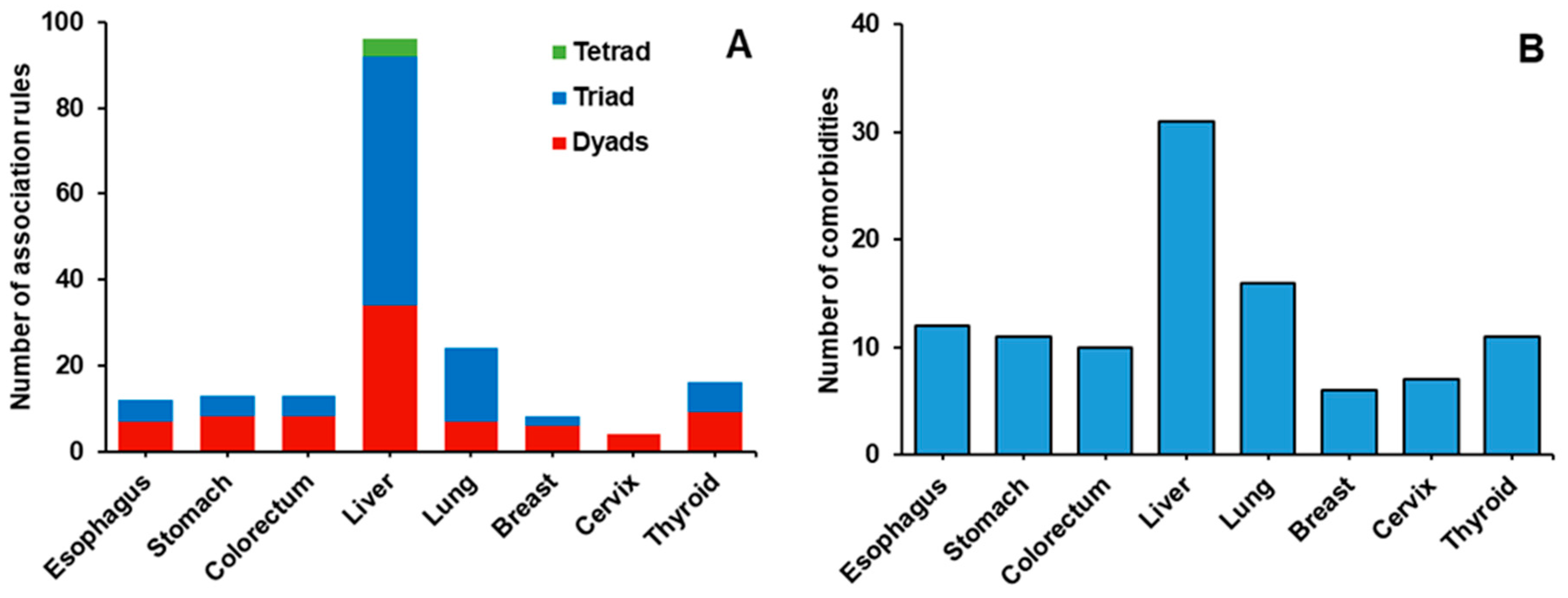
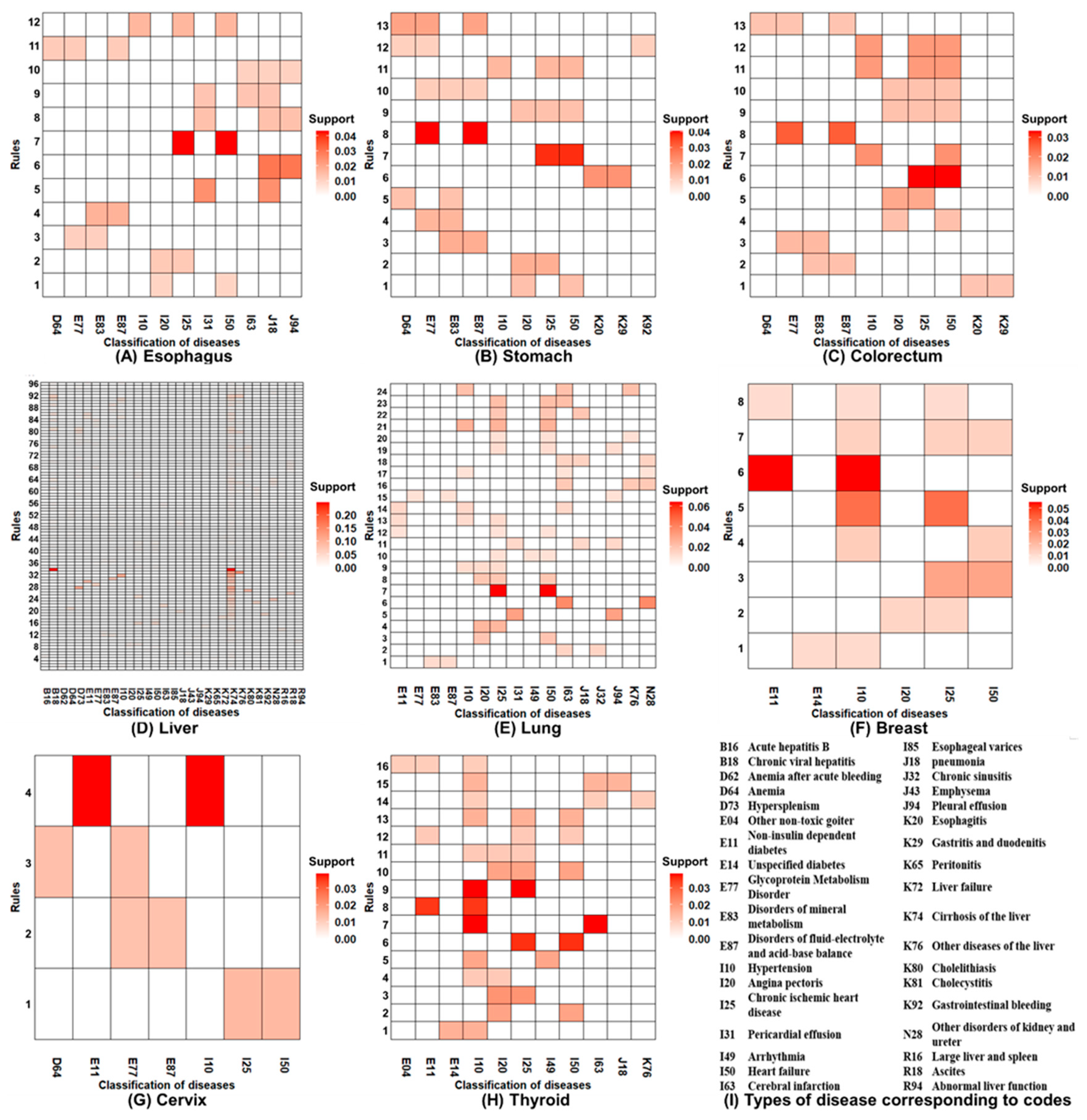
3.3. Association Rule Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Sun, K.; Zheng, R.; Zheng, R.; Zeng, H.; Zhang, S.; Xia, C.; Yang, L.; Li, H.; Zou, X.; et al. Cancer incidence and mortality in China. Chin. J. Cancer Res. 2018, 30, 1–12. [Google Scholar] [CrossRef]
- Søgaard, M.; Thomsen, R.W.; Bossen, K.S.; Sorensen, H.T.; Norgaard, M. The impact of comorbidity on cancer survival: A review. J. Clin. Epidemiol. 2013, 5, 3–29. [Google Scholar] [CrossRef] [Green Version]
- Edwards, B.K.; Noone, A.M.; Mariotto, A.B.; Simard, E.P.; Boscoe, F.P.; Henley, S.J.; Jemal, A.; Cho, H.; Anderson, R.N.; Kohler, B.A.; et al. Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 2014, 120, 1290–1314. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Sarfati, D.; Koczwara, B.; Jackson, C. The impact of comorbidity on cancer and its treatment. CA Cancer J. Clin. 2016, 66, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Antol, D.D.; Casebeer, A.W.; Khoury, R.; Todd, M.; Andrew, R.; Sari, H.; Aparna, P.; Alisha, S.; Mary, C.; Stephen, S.; et al. The relationship between comorbidity medication adherence and health related quality of life among patients with cancer. J. Patient Rep. Outcomes 2018, 2, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.H.; Lee, T.Y.; Hui, K.C.; Chung, M.H. Mental disorders and medical comorbidities: Association rule mining approach. Perspect. Psychiatr. Care 2019, 55, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Fried, E.I.; Van Borkulo, C.D.; Cramer Angélique, O.J.; Boschloo, L.; Schoevers, R.A.; Borsboom, D. Mental disorders as networks of problems: A review of recent insights. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Held, F.P.; Fiona, B.; Danijela, G.; Vasant, H.; Vasikaran, N.; Waite, L.M.; Seibel, M.J.; Rollo, J.; Handelsman, D.J.; Cumming, R.G.; et al. Association rules analysis of comorbidity and multimorbidity: The concord health and aging in men project. J. Gerontol. 2016, 71, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Hossain, M.E.; Khan, A.; Uddin, S. Understanding the Comorbidity of Multiple Chronic Diseases Using a Network Approach. In Proceedings of the Australasian Computer Science Week Multiconference (ACSW), Sydney, Australia, 29 January 2019. [Google Scholar]
- Cho, H.; Mariotto, A.B.; Mann, B.S.; Klabunde, C.N.; Feuer, E.J. Assessing non-cancer-related health status of US cancer patients: Other-cause survival and comorbidity prevalence. Am. J. Epidemiol. 2013, 178, 339–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, G.; Azevedo, P.; Martins, J.; Arantes, C.; Quina-Rodrigues, C.; Fonseca, S.; Braga, C.; Vieira, C.; Marques, J. Prevalence of cancer and its impact on prognosis of acute coronary syndrome population. In Proceedings of the Congress of the European-Society-of-Cardiology (ESC), Rome, Italy, 27–31 August 2016. [Google Scholar]
- Seong, J.M.; Shin, D.; Sung, J.W.; Cho, S.; Yang, J.; Kang, S.; Moon, H.W.; Lee, K.W.; Ha, U.S. Gonadotropin-releasing hormone agonists, anti-androgens and the risk of cardio-cerebrovascular disease in prostate cancer patients: An asian population-based observational study. J. Cancer 2020, 11, 4015–4022. [Google Scholar] [CrossRef]
- Ballout, F.; Manshad, A.S.; Okwuosa, T.M. Pulmonary Hypertension and Cancer: Etiology, Diagnosis, and Management. Curr. Treat. Opt. Cardiovasc. Med. 2017, 19, 44. [Google Scholar] [CrossRef]
- Kozlowska, K.; Malyszko, J.; Kozlowski, L. Colorectal Cancer and Hypertension. In Proceedings of the 27th Scientific Meeting of the International-Society-of-Hypertension, Beijing, China, 20–23 September 2018. [Google Scholar]
- Jorgensen, T.L.; Hallas, J.; Friis, S.; Herrstedt, J. Comorbidity in elderly cancer patients in relation to overall and cancer-specific mortality. Br. J. Cancer 2012, 106, 1353–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancik, R.; Havlik, R.J.; Wesley, M.N.; Ries, L.; Long, S.; Rossi, W.K.; Edwards, B.K. Cancer and comorbidity in older patients: A descriptive profile. Ann. Epidemiol. 1996, 6, 399–412. [Google Scholar] [CrossRef]
- Sarkar, I.N.; Chen, E.S. Determining compound comorbidities for heart failure from hospital discharge data. AMIA Ann. Symp. Proc. 2012, 2012, 809–818. [Google Scholar]
- Chen, H.; Zhang, Y.Y.; Wu, D.; Gong, C.X.; Pan, Q.; Dong, X.; Wu, Y.H.; Zhang, K.; Wang, S.P.; Lei, J.B.; et al. Comorbidity in adult patients hospitalized with type 2 diabetes in northeast china: An analysis of hospital discharge data from 2002 to 2013. BioMed Res. Int. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Sarfati, D.; Gurney, J.; Lim, B.T.; Bagheri, N.; Simpson, A.; Koea, J.; Dennett, E. Identifying important comorbidity among cancer populations using administrative data: Prevalence and impact on survival. Asia Pac. J. Clin. Oncol. 2016, 12, e47–e56. [Google Scholar] [CrossRef]
- Sarfati, D.; Gurney, J.; Stanley, J.; Koea, J. A retrospective cohort study of patients with stomach and liver cancers: The impact of comorbidity and ethnicity on cancer care and outcomes. BMC Cancer 2014, 14. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.T.; Gersing, K.R.; Swartz, M.S.; Burchett, B.; Li, T.K.; Blazer, D.G. Using electronic health records data to assess comorbidities of substance use and psychiatric diagnoses and treatment settings among adults. J. Psychiatr. Res. 2013, 47, 555–563. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.T.; Gersing, K.; Burchett, B.; Woody, G.E.; Blazer, D.G. Substance use disorders and comorbid Axis I and II psychiatric disorders among young psychiatric patients: Findings from a large electronic health records database. J. Psychiatr. Res. 2011, 45, 1453–1462. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Xu, R. Mining cancer-specific disease comorbidities from a large observational health database. Cancer Inform. 2014, 2014, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, R.; Srikant, R. Fast algorithms for mining association rules. In Proc. of the 20th International Conference on Very Large Data Bases; IEEE: Piscataway, NJ, USA, 1994. [Google Scholar]
- Borgelt, C. Simple Algorithms for Frequent Item Set Mining Advances in Machine Learning II; Springer: Berlin/Heidelberg, Germany, 2010; pp. 351–369. [Google Scholar]
- WHO Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems 10th Rev. World Health Organ. 1992, 56, 65. [Google Scholar]
- Zheng, R.S.; Sun, K.X.; Zhang, S.W.; Zeng, H.M.; He, J. Report of cancer epidemiology in China, 2015. Chin. J. Oncol. 2019, 41, 19–28. [Google Scholar]
- Gaspar, B.L.; Sharma, P.; Das, R. Anemia in malignancies: Pathogenetic and diagnostic considerations. Hematology 2015, 20, 18–25. [Google Scholar] [CrossRef]
- Ludwig, H. Epoetin in cancer-related anaemia. 2nd European Epoetin Symposium on Optimizing Anaemia Therapy in CRF. Nephrol. Dial. Transplant. 1998, 14. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Jung, C.W.; Kim, K.; Kim, S.J.; Kim, W.S.; Jang, J.H. Iron deficient erythropoiesis might play key role in development of anemia in cancer patients. Oncotarget 2015, 6, 42803–42812. [Google Scholar] [CrossRef] [Green Version]
- Sundriyal, D.; Nayak, P.P.; Arya, L.; Walia, M.; Saha, R. Evaluation of Iron Status in Patients of Solid Organ Malignancies: Study from a Cancer Research Centre. Indian J. Surg. Oncol. 2020, 11, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Baby, D.; Rajguru, J.P.; Patil, P.B.; Thakkannavar, S.S.; Pujari, V.B. Inflammation and Cancer. Ann. Afr. Med. 2019, 18, 121–126. [Google Scholar] [CrossRef]
- Chen, J.; Pitmon, E.; Wang, K. Microbiome, inflammation and colorectal cancer. Semin. Immunol. 2017, 32, 43–53. [Google Scholar] [CrossRef]
- Zeber, J.E.; Copeland, L.A.; Hosek, B.J.; Karnad, A.B.; Lawrence, V.A.; Sanchez-Reilly, S.E. Cancer rates, medical comorbidities, and treatment modalities in the oldest patients. Crit. Rev. Oncol. Hematol. 2008, 67, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, J.F.; Vlahiotis, A.; Barrett, L.B.; Flood, K.L.; Spitznagel, E.L.; Steyerberg, E.W. The changing prevalence of comorbidity across the age spectrum. Crit. Rev. Oncol. Hematol. 2008, 67, 124–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Yan, Z.R.; Liang, Y.J.; Tan, E.C.K.; Cai, C.Z.; Jiang, H.; Song, A.Q.; Qiu, C.X. Prevalence and Patterns of Chronic Disease Pairs and Multimorbidity among Older Chinese Adults Living in a Rural Area. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Artaman, A.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar]
- MuX, M.; Wang, W.; Jiang, Y.Y.; Feng, J. Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective. Int. J. Environ. Res. Public Health 2020, 17, 3108. [Google Scholar] [CrossRef]
- Siegel, A.B.; Zhu, A.X. Metabolic syndrome and hepatocellular carcinoma: Two growing epidemics with a potential link. Cancer 2009, 115, 5651–5661. [Google Scholar] [CrossRef] [Green Version]
- Osaki, Y.; Taniguchi, S.; Tahara, A.; Okamoto, M.; Kishimoto, T. Metabolic syndrome and incidence of liver and breast cancers in Japan. Cancer Epidemiol. 2012, 36, 141–147. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Cancers | Without Cancer (n = 80,574) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All (n = 80,574) | Esophagus (n = 3088) | Stomach (n = 8220) | Colorectum (n = 16,961) | Liver (n = 8710) | Lung (n = 28,282) | Breast (n = 11,231) | Cervix (n = 2623) | Thyroid (n = 1459) | ||
| All | 3 [1,2,3,4,5,6] | 2 [1,2,3,4,5] | 2 [1,2,3,4,5] | 2 [1,2,3,4,5] | 4 [2,3,4,5,6] | 4 [2,3,4,5,6,7] | 2 [1,2,3,4] | 2 [1,2,3,4] | 2 [1,2,3,4] | 2 [1,2,3,4] |
| By gender | ||||||||||
| Male | 3 [1,2,3,4,5,6] | 2 [1,2,3,4,5] | 2 [1,2,3,4,5] | 2 [1,2,3,4,5] | 4 [2,3,4,5,6] | 4 [2,3,4,5,6,7] | —— | —— | 2 [1,2,3,4,5] | 2 [1,2,3,4] |
| Female | 3 [1,2,3,4,5] | 3 [1,2,3,4,5] | 3 [1,2,3,4,5] | 3 [1,2,3,4,5] | 4 [2,3,4,5,6] | 4 [2,3,4,5,6,7] | 2 [1,2,3,4] | 2 [1,2,3,4] | 2 [1,2,3,4] | 2 [1,2,3,4,5] |
| By age | ||||||||||
| 60–70 | 3 [1,2,3,4,5] | 2 [1,2,3,4,5] | 2 [1,2,3,4] | 2 [1,2,3,4,5] | 4 [2,3,4,5,6] | 4 [2,3,4,5,6,7] | 2 [1,2,3,4] | 2 [1,2,3] | 2 [1,2,3,4] | 2 [1,2,3,4] |
| 70–80 | 3 [1,2,3,4,5,6] | 2 [1,2,3,4,5] | 3 [1,2,3,4,5] | 3 [1,2,3,4,5] | 4 [2,3,4,5,6] | 4 [2,3,4,5,6,7] | 3 [1,2,3,4,5,6] | 2 [1,2,3,4] | 2 [1,2,3,4,5] | 2 [1,2,3,4,5] |
| ≥80 | 4 [2,3,4,5,6,7,8] | 3 [1,2,3,4,5] | 4 [2,3,4,5,6,7] | 4 [1,2,3,4,5,6,7] | 5 [2,3,4,5,6,7,8] | 5 [2,3,4,5,6,7,8] | 4 [1,2,3,4,5,6] | 4 [2,3,4,5] | 5 [2,3,4,5,6,7,8] | 3 [1,2,3,4,5] |
| Comorbid Disease Categories | ICD-10 Codes | Patients with Cancer n (%) | Patients without Cancer n (%) | PRs(95%CI) | p Value |
|---|---|---|---|---|---|
| Infectious diseases | A00-B99 | 5501(6.79) | 1823(2.26) | 3.00(2.85–3.16) | <0.001 |
| Blood system diseases | D50-D89 | 8037(9.92) | 3913(4.86) | 2.04(1.97–2.12) | <0.001 |
| Metabolic diseases | E00-E89 | 19,617(24.20) | 29,110(36.13) | 0.67(0.66–0.68) | <0.001 |
| Mental, Behavioral and Neurodevelopmental disorders | F01-F99 | 58(0.07) | 388(0.48) | 0.15(0.11–0.20) | <0.001 |
| Diseases of the nervous system | G00-G99 | 1354(1.67) | 3920(4.87) | 0.34(0.32–0.37) | <0.001 |
| Diseases of the eye, adnexa, ear and mastoid process | H00-H95 | 238(0.29) | 4143(5.14) | 0.08(0.07–0.09) | <0.001 |
| Cardiovascular diseases | I00-I99 | 28,457(35.11) | 46,245(57.39) | 0.61(0.61–0.62) | <0.001 |
| Diseases of the respiratory system | J00-J99 | 19,083(23.54) | 12,548(15.57) | 1.51(1.48–1.54) | <0.001 |
| Diseases of the digestive system | K00-K95 | 23,992(29.60) | 13,421(16.66) | 1.78(1.74–1.81) | <0.001 |
| Diseases of the skin and subcutaneous tissue | L00-L99 | 455(0.56) | 884(1.10) | 0.51(0.46–0.57) | <0.001 |
| Diseases of the musculoskeletal system | M00-M99 | 2283(2.82) | 5685(7.06) | 0.40(0.38–0.42) | <0.001 |
| Diseases of the genitourinary system | N00-N99 | 9705(11.97) | 9476(11.76) | 1.02(0.99–1.05) | 0.185 |
| Congenital anomalies | Q00-Q99 | 343(0.42) | 658(0.82) | 0.52(0.46–0.59) | <0.001 |
| Symptoms, signs and ill-defined conditions | R00-R99 | 7931(9.79) | 6191(7.68) | 1.27(1.23–1.32) | <0.001 |
| Injury, poisoning and certain other consequences of external causes | S00-T88 | 620(0.76) | 2429(3.01) | 0.25(0.23–0.28) | <0.001 |
| Comorbid Disease Categories | Esophagus PR (95% CI) | Stomach PR (95% CI) | Colorectum PR (95% CI) | Liver PR (95% CI) | Lung PR (95% CI) | Breast PR (95% CI) | Cervix PR (95% CI) | Thyroid PR (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Infectious diseases | 1.23(1.00–1.52) | 1.25(1.10–1.43) * | 1.30(1.18–1.44) * | 16.85(15.98–17.76) * | 1.70(1.58–1.83) * | 0.70(0.61–0.82) * | 1.15(0.90–1.46) | 0.58(0.37–0.90) |
| Blood system diseases | 1.69(1.49–1.91) * | 3.29(3.11–3.49) * | 1.83(1.73–1.94) * | 3.66(3.46–3.86) * | 1.84(1.75–1.93) * | 0.93(0.85–1.02) | 2.61(2.35–2.90) * | 0.54(0.39–0.74) * |
| Metabolic diseases | 0.55(0.51–0.59) * | 0.64(0.62–0.67) * | 0.58(0.56–0.60) * | 0.78(0.76–0.81) * | 0.73(0.72–0.75) * | 0.56(0.54–0.59) * | 0.58(0.54–0.63) * | 1.29(1.22–1.36) * |
| Mental, behavioral and neurodevelopmental disorders | 0.13(0.03–0.54) * | 0.13(0.05–0.31) * | 0.15(0.08–0.26) * | 0.12(0.05–0.29) * | 0.17(0.11–0.26) * | 0.13(0.06–0.27) * | 0.18(0.05–0.74) | 0.14(0.02–1.01) |
| Diseases of the nervous system | 0.25(0.18–0.34) * | 0.29(0.24–0.34) * | 0.25(0.22–0.29) * | 0.25(0.21–0.30) * | 0.51(0.47–0.55) * | 0.17(0.14–0.21) * | 0.17(0.11–0.25) * | 0.21(0.13–0.35) * |
| Diseases of the eye, adnexa, ear and mastoid process | 0.04(0.02–0.09) * | 0.07(0.05–0.10) * | 0.06(0.04–0.07) * | 0.09(0.07–0.13) * | 0.08(0.07–0.10) * | 0.11(0.08–0.14) * | 0.03(0.01–0.08) * | 0.15(0.08–0.26) * |
| Cardiovascular diseases | 0.56(0.53–0.59) * | 0.46(0.44–0.48) * | 0.49(0.48–0.50) * | 0.55(0.53–0.57) * | 0.81(0.80–0.82) * | 0.52(0.51–0.54) * | 0.44(0.41–0.47) * | 0.53(0.49–0.57) * |
| Diseases of the respiratory system | 1.61(1.52–1.72) * | 0.93(0.88–0.98) | 0.76(0.72–0.79) * | 0.89(0.84–0.94) * | 2.84(2.78–2.90) * | 0.55(0.51–0.58) * | 0.32(0.27–0.38) * | 0.99(0.87–1.11) |
| Diseases of the digestive system | 1.49(1.40–1.59) * | 2.09(2.03–2.16) * | 2.17(2.12–2.23) * | 4.14(4.05–4.23) * | 1.28(1.24–1.31) * | 0.90(0.86–0.94) * | 0.73(0.65–0.81) * | 0.68(0.58–0.78) * |
| Diseases of the skin and subcutaneous tissue | 0.30(0.16–0.55) * | 0.49(0.36–0.66) * | 0.55(0.45–0.67) * | 0.68(0.53–0.87) | 0.58(0.50–0.68) * | 0.34(0.25–0.46) * | 0.17(0.07–0.42) * | 0.31(0.13–0.75) |
| Diseases of the musculoskeletal system | 0.21(0.16–0.28) * | 0.21(0.18–0.25) * | 0.30(0.27–0.33) * | 0.30(0.26–0.35) * | 0.55(0.51–0.58) * | 0.44(0.39–0.49) * | 0.22(0.16–0.30) * | 0.66(0.52–0.83) * |
| Diseases of the genitourinary system | 0.84(0.76–0.94) | 1.05(0.99–1.11) | 1.08(1.04–1.13) * | 1.28(1.21–1.35) * | 1.13(1.09–1.17) * | 0.52(0.49–0.56) * | 1.12(1.02–1.24) | 0.53(0.43–0.65) * |
| Congenital anomalies | 0.63(0.39–1.04) | 0.69(0.51–0.92) | 0.59(0.47–0.74) * | 0.72(0.54–0.95) | 0.42(0.34–0.52) * | 0.39(0.28–0.55) * | 0.14(0.05–0.44) * | 0.84(0.45–1.56) |
| Symptoms, signs and ill-defined conditions | 1.36(1.22–1.51) * | 1.48(1.38–1.58) * | 1.09(1.04–1.16) * | 2.31(2.19–2.43) * | 1.33(1.27–1.38) * | 0.63(0.58–0.69) * | 0.72(0.61–0.84) * | 0.85(0.70–1.03) |
| Injury, poisoning and certain other consequences of external causes | 0.27(0.18–0.40) * | 0.20(0.15–0.26) * | 0.35(0.30–0.41) * | 0.19(0.14–0.25) * | 0.28(0.25–0.32) * | 0.15(0.11–0.20) * | 0.24(0.15–0.38) * | 0.07(0.02–0.21) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mu, X.-M.; Wang, W.; Wu, F.-Y.; Jiang, Y.-Y.; Ma, L.-l.; Feng, J. Comorbidity in Older Patients Hospitalized with Cancer in Northeast China based on Hospital Discharge Data. Int. J. Environ. Res. Public Health 2020, 17, 8028. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218028
Mu X-M, Wang W, Wu F-Y, Jiang Y-Y, Ma L-l, Feng J. Comorbidity in Older Patients Hospitalized with Cancer in Northeast China based on Hospital Discharge Data. International Journal of Environmental Research and Public Health. 2020; 17(21):8028. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218028
Chicago/Turabian StyleMu, Xiao-Min, Wei Wang, Fang-Yi Wu, Yu-Ying Jiang, Ling-ling Ma, and Jia Feng. 2020. "Comorbidity in Older Patients Hospitalized with Cancer in Northeast China based on Hospital Discharge Data" International Journal of Environmental Research and Public Health 17, no. 21: 8028. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218028