Cohort Profile: ZOE 2.0—A Community-Based Genetic Epidemiologic Study of Early Childhood Oral Health

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
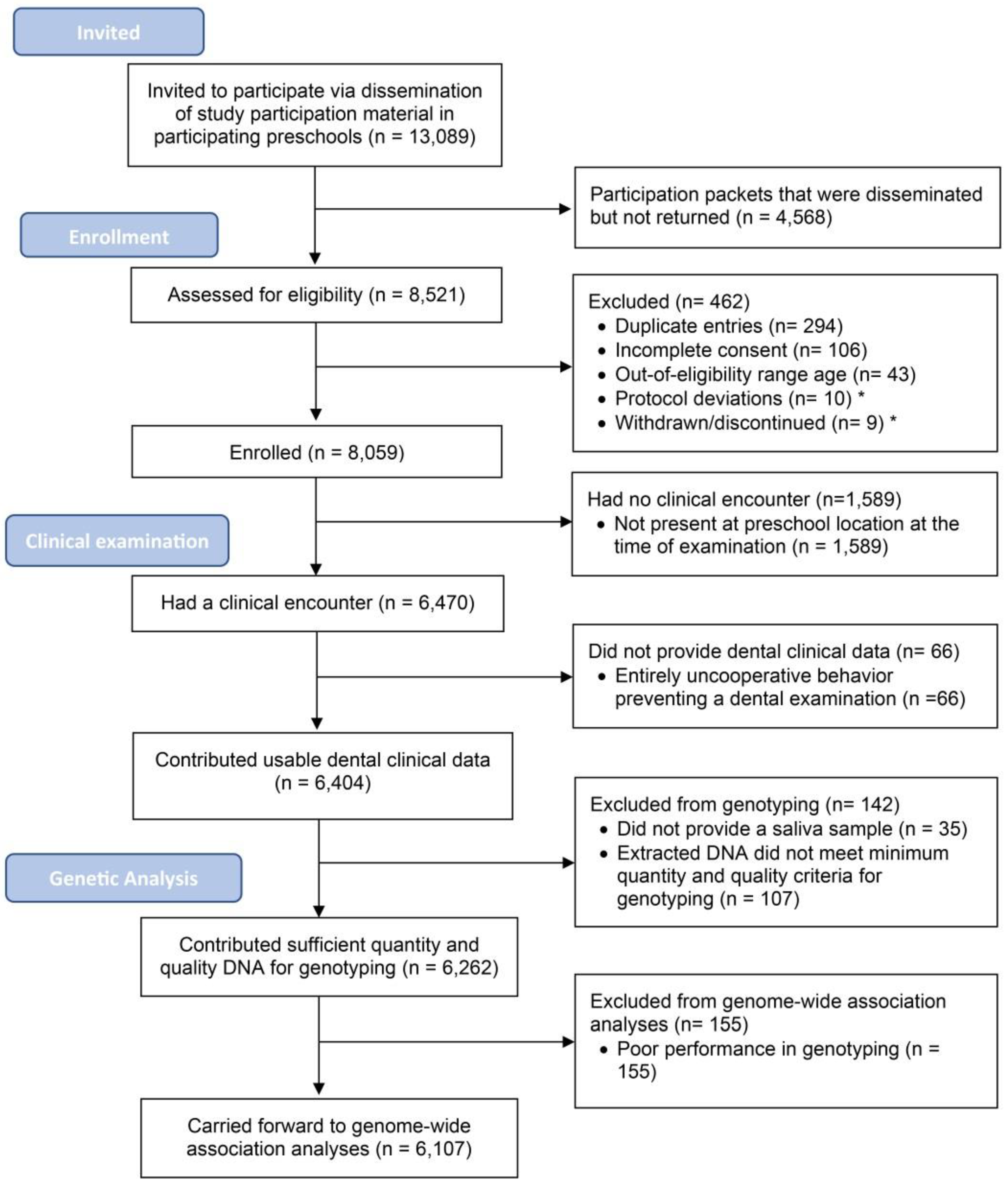
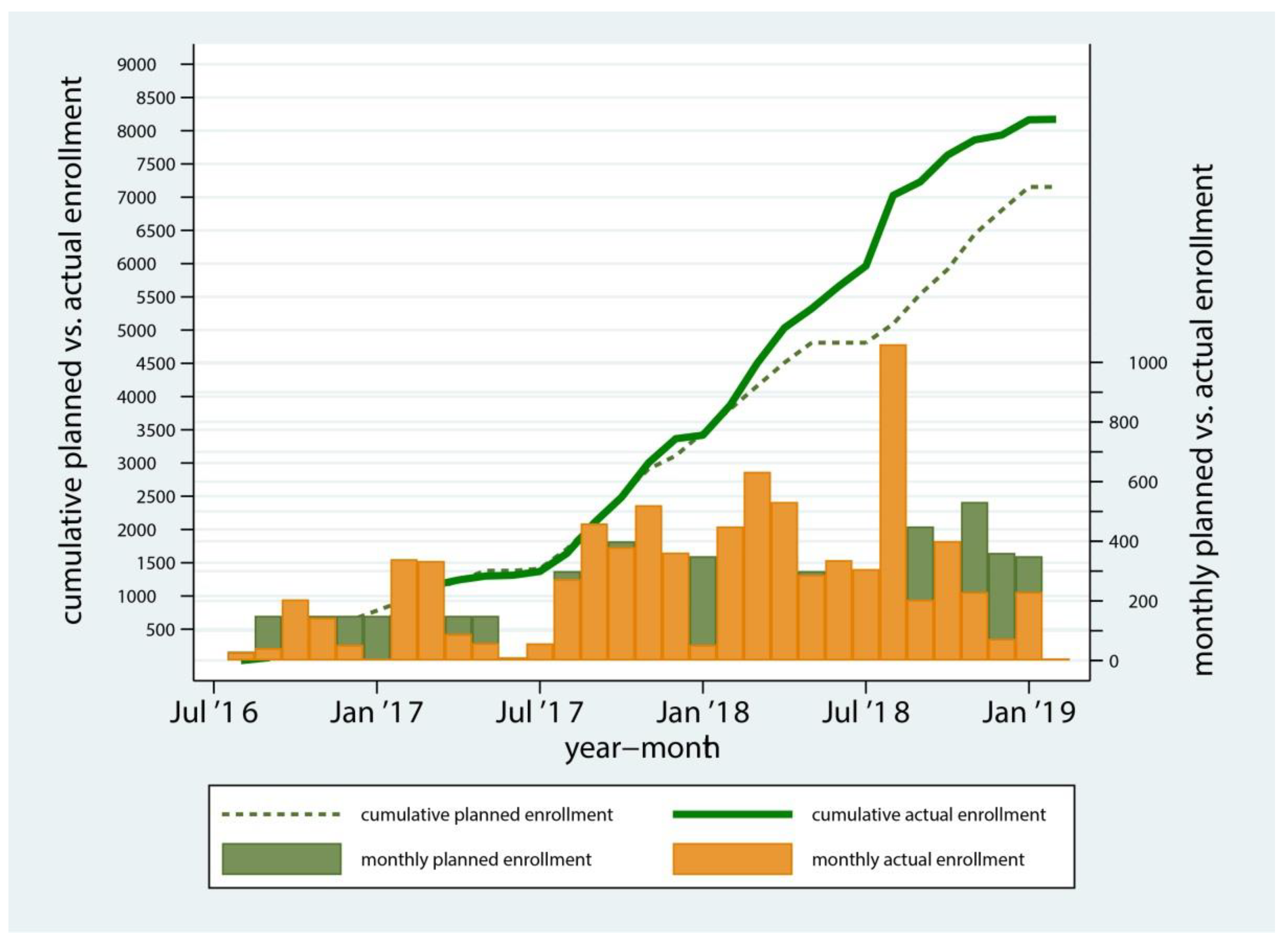
3.1. Enrollment of Study Participants
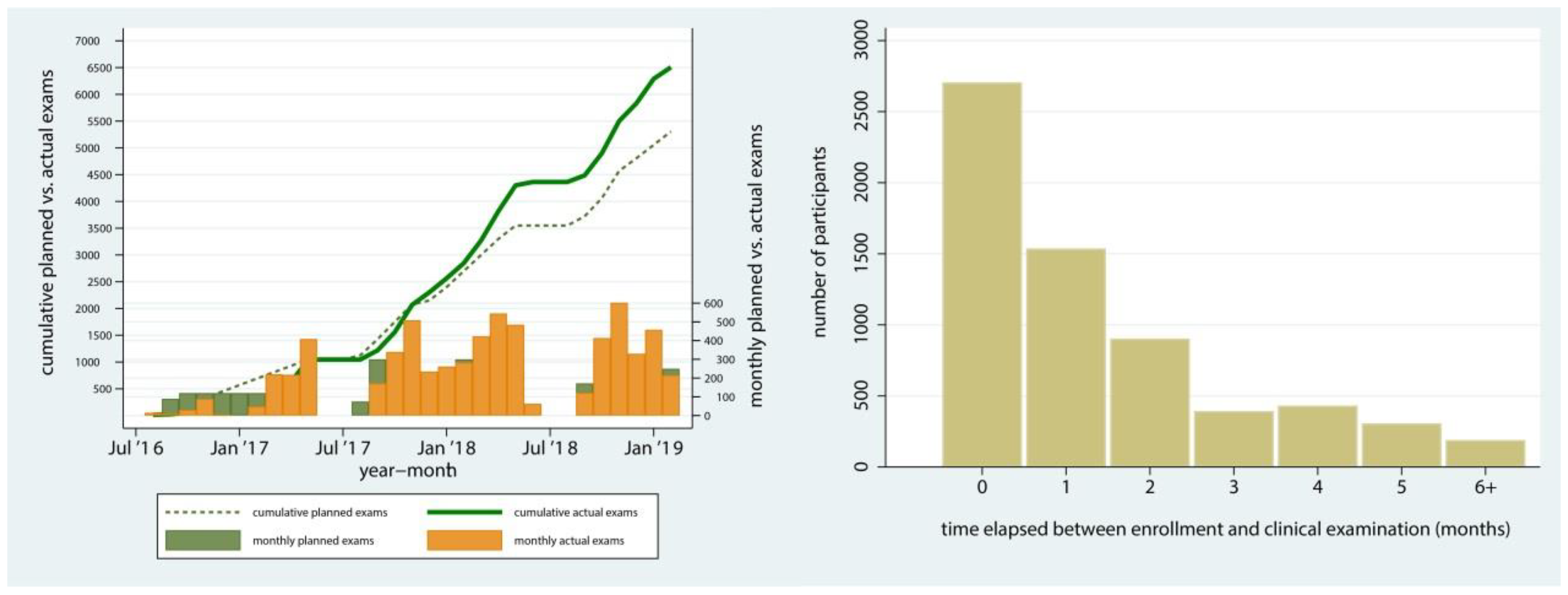
3.2. Clinical Examinations
3.3. Data Completeness
3.4. Protocol Deviations
3.5. Enrolled and Examined Participants’ Demographic Characteristics
3.6. Main Study Outcomes—ECC
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pitts, N.B.; Baez, R.J.; Diaz-Guillory, C.; Donly, K.J.; Alberto Feldens, C.; McGrath, C.; Phantumvanit, P.; Seow, W.K.; Sharkov, N.; Songpaisan, Y.; et al. Early Childhood Caries: IAPD Bangkok Declaration. Int. J. Paed. Dentistry 2019, 29, 384–386. [Google Scholar] [CrossRef] [Green Version]
- Casamassimo, P.S.; Thikkurissy, S.; Edelstein, B.L.; Maiorini, E. Beyond the dmft: The Human and Economic Cost of Early Childhood Caries. J. Am. Dent. Assoc. 2009, 140, 650–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.; Kearns, C.; et al. Oral Diseases: A Global Public Health Challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Lee, J.Y.; Divaris, K. The Ethical Imperative of Addressing Oral Health Disparities: A Unifying Framework. J. Dent. Res. 2014, 93, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental Caries. Nat. Rev. Dis. Primers. 2017, 25, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Divaris, K. Predicting Dental Caries Outcomes in Children: A “Risky” Concept. J. Dent. Res. 2016, 95, 248–254. [Google Scholar] [CrossRef]
- Lin, M.; Griffin, S.O.; Gooch, B.F.; Espinoza, L.; Wei, L.; Li, C.H.; Thornton-Evans, G.; Junger, M.L.; Robison, V.A.; Fleming, E.B.; et al. Oral Health Surveillance Report: Trends in Dental Caries and Sealants, Tooth Retention, and Edentulism, United States: 1999–2004 to 2011–2016; Centers for Disease Control and Prevention, US Dept of Health and Human Services: Atlanta, GA, USA, 2019. [Google Scholar]
- Divaris, K. Precision Dentistry in Early Childhood: The Central Role of Genomics. Dent. Clin. North. Am. 2017, 61, 619–625. [Google Scholar] [CrossRef]
- Divaris, K. The Era of the Genome and Dental Medicine. J. Dent. Res. 2019, 98, 949–955. [Google Scholar] [CrossRef]
- Morelli, T.; Agler, C.S.; Divaris, K. Genomics of Periodontal Disease and Tooth Morbidity. Periodontology 2000 2020, 82, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Ballantine, J.; Carlson, J.C.; Zandona, A.; Agler, C.S.; Zeldin, L.P.; Rozier, G.; Roberts, M.W.; Basta, P.V.; Luo, J.; Antonio-Obese, M.E.; et al. Exploring the Genomic Basis of Early Childhood Caries: A Pilot Study. Int. J. Paed. Dentistry. 2018, 28, 217–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haworth, S.; Shungin, D.; van der Tas, J.T.; Vucic, S.; Medina-Gomez, C.; Yakimov, V.; Feenstra, B.; Shaffer, J.R.; Lee, M.K.; Standl, M.; et al. Consortium-Based Genome-Wide Meta-Analysis for Childhood Dental Caries Traits. Hum. Mol. Genet. 2018, 27, 3113–3127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shungin, D.; Haworth, S.; Divaris, K.; Agler, C.S.; Kamatani, Y.; Keun Lee, M.; Grinde, K.; Hindy, G.; Alaraudanjoki, V.; Pesonen, P. Genome-Wide Analysis of Dental Caries and Periodontitis Combining Clinical and Self-Reported Data. Nat. Commun. 2019, 10, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, J.R.; Wang, X.; Feingold, E.; Lee, M.; Begum, F.; Weeks, D.E.; Cuenco, K.T.; Barmada, M.M.; Wendell, S.K.; Crosslin, D.R. Genome-Wide Association Scan for Childhood Caries Implicates Novel Genes. J. Dent. Res. 2011, 90, 1457–1462. [Google Scholar] [CrossRef] [Green Version]
- Born, C.D.; Divaris, K.; Zeldin, L.P.; Rozier, R.G. Influences on Preschool Children’s Oral Health-Related Quality of Life as Reported by English and Spanish-Speaking Parents and Caregivers. J. Public. Health. Dent. 2016, 76, 276–286. [Google Scholar] [CrossRef]
- Born, C.D.; Jackson, T.H.; Koroluk, L.D.; Divaris, K. Traumatic Dental Injuries in Preschool-Age Children: Prevalence and Risk Factors. Clin. Exp. Dent. Res. 2019, 5, 151–159. [Google Scholar] [CrossRef]
- Ginnis, J.; Ferreira Zandoná, A.G.; Slade, G.D.; Cantrell, J.; Antonio, M.E.; Pahel, B.T.; Meyer, B.D.; Shrestha, P.; Simancas-Pallares, M.A.; Joshi, A.R.; et al. Measurement of Early Childhood Oral Health for Research Purposes: Dental Caries Experience and Developmental Defects of the Enamel in the Primary Dentition. Methods. Mol. Biol. 2019, 1922, 511–523. [Google Scholar] [CrossRef]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An Integrated System for Measuring Dental Caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, D.A.; Nový, B.B.; Zeller, G.G.; Hale, R.; Hart, T.C.; Truelove, E.L. The American Dental Association Caries Classification System for Clinical Practice: A Report of the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2015, 146, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Agler, C.S.; Shungin, D.; Ferreira Zandoná, A.G.; Schmadeke, P.; Basta, P.V.; Luo, J.; Cantrell, J.; Pahel, T.D., Jr.; Meyer, B.D.; Shaffer, J.R.; et al. Protocols, Methods, and Tools for Genome-Wide Association Studies (GWAS) of Dental Traits. Methods Mol. Biol. 2019, 1922, 493–509. [Google Scholar] [CrossRef] [PubMed]
- Divaris, K.; Shungin, D.; Rodríguez-Cortés, A.; Basta, P.V.; Roach, J.; Cho, H.; Wu, D.; Ferreira Zandoná, A.G.; Ginnis, J.; Ramamoorthy, S. The Supragingival Biofilm in Early Childhood Caries: Clinical and Laboratory Protocols and Bioinformatics Pipelines Supporting Metagenomics, Metatranscriptomics, and Metabolomics Studies of the Oral Microbiome. Methods Mol. Biol. 2019, 1922, 525–548. [Google Scholar] [CrossRef] [PubMed]
- Divaris, K.; Joshi, A. The Building Blocks of Precision Oral Health in Early Childhood: The ZOE 2.0 Study. J. Public Health Dent. 2020, 80, S31–S36. [Google Scholar] [CrossRef]
- Agler, C.S.; Divaris, K. Sources of Bias in Genomics Research of Oral and Dental Traits. Community Dent. Health. 2020, 37, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lee, S.H.; Goddard, M.E.; Visscher, P.M. GCTA: A Tool for Genome-Wide Complex Trait Analysis. Am. J. Hum. Genet. 2011, 88, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, D.Y.; Tao, R.; Kalsbeek, W.D.; Zeng, D.; Gonzalez, F., 2nd; Fernández-Rhodes, L.; Graff, M.; Koch, G.G.; North, K.E.; Heiss, G. Genetic Association Analysis under Complex Survey Sampling: The Hispanic Community Health Study/Study of Latinos. Am. J. Hum. Genet. 2014, 95, 675–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasaniuc, B.; Zaitlen, N.; Lettre, G.; Chen, G.K.; Tandon, A.; Kao, W.H.; Ruczinski, I.; Fornage, M.; Siscovick, D.S.; Zhu, X. Enhanced Statistical Tests for GWAS in Admixed Populations: Assessment using African Americans from CARe and a Breast Cancer Consortium. PLoS Genet. 2011, 7, e1001371. [Google Scholar] [CrossRef] [PubMed]
- Mägi, R.; Horikoshi, M.; Sofer, T.; Mahajan, A.; Kitajima, H.; Franceschini, N.; McCarthy, M.I.; COGENT-Kidney Consortium; T2D-GENES Consortium; Morris, A.P. Trans-Ethnic Meta-Regression of Genome-Wide Association Studies Accounting for Ancestry Increases Power for discovery and Improves Fine-Mapping Resolution. Hum. Mol. Genet. 2017, 26, 3639–3650. [Google Scholar] [CrossRef] [Green Version]
- Baldassari, A.R.; Sitlani, C.M.; Highland, H.M.; Arking, D.E.; Buyske, S.; Darbar, D.; Gondalia, R.; Graff, M.; Guo, X.; Heckbert, S.R. Multi-Ethnic Genome-Wide Association Study of Decomposed Cardioelectric Phenotypes Illustrates Strategies to Identify and Characterize Evidence of Shared Genetic Effects for Complex Traits. Circ. Genom. Precis. Med. 2020, 13. [Google Scholar] [CrossRef]
- Wojcik, G.L.; Graff, M.; Nishimura, K.K.; Tao, R.; Haessler, J.; Gignoux, C.R.; Highland, H.M.; Patel, Y.M.; Sorokin, E.P.; Avery, C.L. Genetic Analyses of Diverse Populations Improves Discovery for Complex Traits. Nature 2019, 570, 514–518. [Google Scholar] [CrossRef]
- Divaris, K. Searching Deep and Wide: Advances in the Molecular Understanding of Dental Caries and Periodontal Disease. Adv. Dent. Res. 2019, 30, 40–44. [Google Scholar] [CrossRef]
- Agler, C.S.; Moss, K.; Philips, K.H.; Marchesan, J.T.; Simancas-Pallares, M.; Beck, J.D.; Divaris, K. Biologically Defined or Biologically Informed Traits Are More Heritable Than Clinically Defined Ones: The Case of Oral and Dental Phenotypes. Adv. Exp. Med. Biol. 2019, 1197, 179–189. [Google Scholar] [CrossRef]
- Zeng, Z.; Feingold, E.; Wang, X.; Weeks, D.E.; Lee, M.; Cuenco, D.T.; Broffitt, B.; Weyant, R.J.; Crout, R.; McNeil, D.W.; et al. Genome-Wide Association Study of Primary Dentition Pit-and-Fissure and Smooth Surface Caries. Caries Res. 2014, 48, 330–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psoter, W.J.; Pendrys, D.G.; Morse, D.E.; Zhang, H.P.; Mayne, S.T. Caries Patterns in the Primary Dentition: Cluster Analysis of a Sample of 5169 Arizona Children 5–59 Months of age. Int. J. Oral Sci. 2009, 1, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Biotechnology Information, U.S. National Library of Medicine, Database of Genotypes and Phenotypes (dbGaP). Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/gap/ (accessed on 31 October 2020).
- Casamassimo, P.S.; Lee, J.Y.; Marazita, M.L.; Milgrom, P.; Chi, D.L.; Divaris, K. Improving Children’s Oral Health: An Interdisciplinary Research Framework. J. Dent. Res. 2014, 93, 938–942. [Google Scholar] [CrossRef]
- Slade, G.D.; Sanders, A.E. Two Decades of Persisting Income-Disparities in Dental Caries Among U.S. Children and Adolescents. J. Public. Health. Dent. 2018, 78, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Collins, F.S.; Varmus, H. A New Initiative on Precision Medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Divaris, K. Fundamentals of Precision Medicine. Compend. Contin. Educ. Dent. 2017, 38, 30–32. [Google Scholar] [PubMed]
- Khoury, M.J.; Iademarco, M.F.; Riley, W.T. Precision Public Health for the Era of Precision Medicine. Am. J. Prev. Med. 2016, 50, 398–401. [Google Scholar] [CrossRef] [Green Version]
- Halasa-Rappel, Y.A.; Ng, M.W.; Gaumer, G.; Banks, D.A. How Useful are Current Caries Risk Assessment Tools in Informing the Oral Health Care Decision-Making Process? J. Am. Dent. Assoc. 2019, 150, 91–102. [Google Scholar] [CrossRef]
- Gomaa, N.; Glogauer, M.; Tenenbaum, H.; Siddiqi, A.; Quiñonez, C. Social-Biological Interactions in Oral Disease: A ‘Cells to Society’ View. PLoS ONE 2016, 11, e0146218. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Questionnaire data (among those with verified, consented enrollment) | 8054/8059 99.9% |
| Usable (i.e., non-missing) clinical dental data (among those with attempted clinical exams) | 6404/6470 99% |
| Usable (i.e., non-missing) anthropometric (i.e., height/weight) data (among those with attempted clinical exams) | 6442/6470 99% |
| Saliva collected (among those that had exams and have non-missing clinical data) | 6369/6404 99% |
| Supragingival plaque collected (among those that had exams and have non-missing clinical data) | 6271/6404 98% |
| Adequate quality and quantity of human DNA available (among those with non-missing clinical data that provided saliva samples) | 6262/6369 98% |
| Acceptable performance during genotyping (among those with adequate quality and quantity of human DNA) | 6107/6262 98% |
| Water sample provided for fluoride measurement (among those with attempted clinical exams) | 1613/6470 25% |
| Usable fluoride concentration information (among those who provided a domestic water sample) | 1518/1613 94% |
| Fluoride concentration data available (among those with clinical data) | 1518/6404 24% |
| Fluoride concentration and geocoding data available (among those with clinical data) | 1501/6404 23% |
| Question | % |
|---|---|
| Who brushes your child’s teeth at home? | 0.4 |
| How often are your child’s teeth brushed? | 0.4 |
| Is toothpaste with fluoride used every time your child’s teeth are brushed? | 1.1 |
| How many snacks and drinks containing sugar does your child usually have between meals? | 0.5 |
| Has your child ever gone to the dentist? | 1.1 |
| Does your child usually see a dentist for a check-up or because of dental problems? | 1.3 |
| Has your child ever been put to bed with a bottle containing something other than water? | 2.1 |
| How would you describe the condition of your child’s mouth and teeth? | 1.2 |
| How would you describe the condition of your mouth and teeth? | 2.6 |
| Has your child ever had a toothache or other dental pain (not from teething)? | 1.2 |
| Has your child been given an over-the-counter medication during the last 30 days? | 1.2 |
| What is the highest grade-level of schooling you have completed? | 2.6 |
| Are you of Hispanic or Latino origin? | 1.1 |
| What is your child’s race? | 2.9 |
| What is the primary source of your home drinking water for your child? | 1.1 |
| All Enrolled | w/ECC Information | p * | |
|---|---|---|---|
| n (Column %) | n (Column %) | ||
| Entire Sample | 8059 (100) | 6404 (100) | |
| Sex † | |||
| male | 4000 (50) | 3189 (50) | 0.6 |
| female | 4057 (50) | 3215 (50) | |
| missing | 2 | 0 | |
| Age at enrollment (years) | 0.2 | ||
| 3 | 2568 (32) | 1992 (31) | |
| 4 | 4234 (53) | 3375 (53) | |
| 5 | 1257 (16) | 1037 (16) | |
| (months), mean (SD) | 52 (7.5) | 52 (7.4) | 0.2 |
| Race | |||
| African–American | 3872 (48) | 3094 (48) | 0.7 |
| American–Indian or Alaskan Native | 236 (3) | 186 (3) | |
| Asian | 42 (1) | 32 (1) | |
| Native Hawaiian or other Pacific Islander | 7 (0.1) | 4 (0.1) | |
| White | 1765 (22) | 1385 (22) | |
| >1 race | 1067 (13) | 835 (13) | |
| other/missing | 1070 (13) | 868 (13) | |
| Hispanic ethnicity | 0.8 | ||
| yes | 1611 (20) | 1291 (20) | |
| no | 6355 (80) | 5042 (80) | |
| missing | 93 | 71 |
| Established ECC, Defined at the ICDAS ≥ 3 threshold | Classic ECC, Defined at the ICDAS ≥ 1 threshold | |||
|---|---|---|---|---|
| dmfs > 0, n (row %) | dmfs, mean (se*) | dmfs>0, n (row %) | dmfs, mean (se*) | |
| Entire Sample | 3465 (54) | 8 (0.6) | 5882 (92) | 15 (0.7) |
| Sex | ||||
| male | 1748 (55) | 8 (0.5) | 2935 (92) | 16 (0.6) |
| female | 1717 (53) | 8 (0.7) | 2947 (92) | 15 (0.7) |
| Age (years) | ||||
| 3 | 673 (45) | 5 (0.4) | 1347 (90) | 13 (0.6) |
| 4 | 1836 (55) | 8 (0.6) | 3084 (92) | 15 (0.7) |
| 5 | 956 (61) | 11 (0.8) | 1451 (93) | 17 (0.9) |
| Race | ||||
| African–American | 1622 (52) | 7 (0.5) | 2845 (92) | 14 (0.6) |
| American–Indian or Alaskan Native | 127 (68) | 15 (1.6) | 180 (97) | 22 (1.3) |
| Asian | 24 (75) | 16 (3.3) | 32 (100) | 23 (3.5) |
| Native Hawaiian or other Pacific Islander | 4 (100) | 21 (6.7) | 4 (100) | 30 (8.0) |
| White | 725 (52) | 8 (0.6) | 1251 (90) | 15 (0.9) |
| >1 race | 426 (51) | 7 (0.6) | 741 (89) | 13 (0.7) |
| other | 534 (62) | 11 (1.0) | 825 (95) | 18 (1.1) |
| Hispanic ethnicity | ||||
| yes | 788 (61) | 11 (1.0) | 1209 (94) | 18 (1.2) |
| no | 2643 (52) | 7 (0.5) | 4604 (91) | 14 (0.6) |
| missing | 34 (48) | 8 (2.4) | 69 (97) | 16 (2.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Divaris, K.; Slade, G.D.; Ferreira Zandona, A.G.; Preisser, J.S.; Ginnis, J.; Simancas-Pallares, M.A.; Agler, C.S.; Shrestha, P.; Karhade, D.S.; Ribeiro, A.d.A.; et al. Cohort Profile: ZOE 2.0—A Community-Based Genetic Epidemiologic Study of Early Childhood Oral Health. Int. J. Environ. Res. Public Health 2020, 17, 8056. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218056
Divaris K, Slade GD, Ferreira Zandona AG, Preisser JS, Ginnis J, Simancas-Pallares MA, Agler CS, Shrestha P, Karhade DS, Ribeiro AdA, et al. Cohort Profile: ZOE 2.0—A Community-Based Genetic Epidemiologic Study of Early Childhood Oral Health. International Journal of Environmental Research and Public Health. 2020; 17(21):8056. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218056
Chicago/Turabian StyleDivaris, Kimon, Gary D. Slade, Andrea G. Ferreira Zandona, John S. Preisser, Jeannie Ginnis, Miguel A. Simancas-Pallares, Cary S. Agler, Poojan Shrestha, Deepti S. Karhade, Apoena de Aguiar Ribeiro, and et al. 2020. "Cohort Profile: ZOE 2.0—A Community-Based Genetic Epidemiologic Study of Early Childhood Oral Health" International Journal of Environmental Research and Public Health 17, no. 21: 8056. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218056