A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
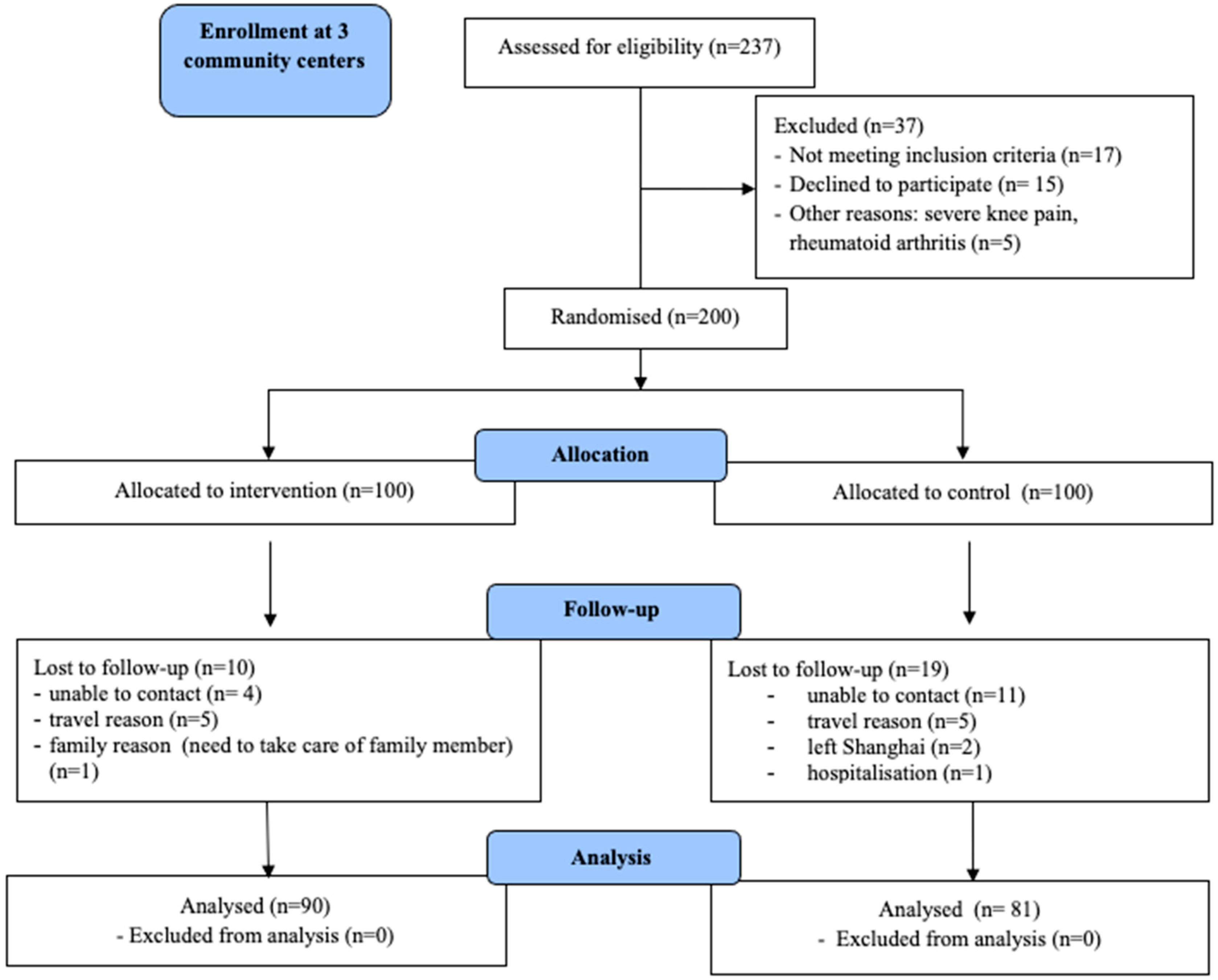
2.2. Participants
2.3. Sample Size
2.4. Procedures
2.5. Dependent Variables
2.6. Independent Variable
2.7. Equipment and Its Reliability
2.8. Student Feedback on Clinical Application of the HIC
2.9. Statistical Analyses
3. Results
3.1. Biometric Measure
3.2. Changes in Lifestyle Behaviour
3.3. Changes in Health and Well Being Questionnaire Scores
3.4. Students Responses
4. Discussion
4.1. Limitations
4.2. Utility of the HIC and Future Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. Available online: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf (accessed on 9 August 2020).
- Langenbrunner, J.C.M.; Patricio, V.; Wang, S. Toward a Healthy and Harmonious Life in China: Stemming the Rising Tide of Non-Communicable Diseases (English). 2011. Available online: http://documents.worldbank.org/curated/en/618431468012000892/Toward-a-healthy-and-harmonious-life-in-China-stemming-the-rising-tide-of-non-communicable-diseases (accessed on 9 August 2020).
- Beaglehole, R.; Bonita, R.; Alleyne, G.; Horton, R.; Li, L.; Lincoln, P.; Mbanya, J.C.; Mckee, M.; Moodie, R.; Nishtar, S.; et al. UN High-Level Meeting on Non-Communicable Diseases: Addressing four questions. Lancet 2011, 378, 449–455. [Google Scholar] [CrossRef]
- China Population. 2020. Available online: http://worldpopulationreview.com/countries/china-population (accessed on 9 August 2020).
- Shanghai Bureau of Statistics. Shanghai Statistical Yearbook. 2019. Available online: http://tjj.sh.gov.cn/tjnj/20200427/4aa08fba106d45fda6cb39817d961c98.html (accessed on 9 August 2020).
- WHPA Health Improvement Card User Guide for Health Professionals. 2018. Available online: https://www.whpa.org/sites/default/files/2018-12/ncd_health_improvement_card_professionals.pdf (accessed on 9 August 2020).
- Health Improvement Card. 2018. Available online: https://www.whpa.org/sites/default/files/2018-12/ncd_Health-Improvement-Card_web.pdf (accessed on 9 August 2020).
- Wu, X.; Jones, A.Y.M.; Bai, Y.; Han, J.; Dean, E. Use of the Health Improvement Card by Chinese physical therapy students: A pilot study. PLoS ONE 2019, 14, e0221630. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Dockray, S.; Wardle, J. Positive affect and psychobiological processes relevant to health. J. Pers. 2009, 76, 1747–1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.Y.; Li, C.B.; Qian, J.; Cui, H.S.; Wu, W.Y. Reliability and validity of a generalized anxiety disorder scale in general hospital outpatient. Shanghai Arch. Psychiatry 2010, 22, 200–203. [Google Scholar] [CrossRef]
- Wang, W.; Bian, Q.; Zhao, Y.; Li, X.; Wang, W.; Du, J.; Zhang, G.; Zhou, Q.; Zhao, M. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2014, 36, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.S.; Wang, S.Y.; Wang, M.Y.; Su, C.T.; Yang, T.T.; Huang, C.J.; Fang, S.C. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, H.M.; Shen, Y. Chinese SF-36 Health Survey: Translation, cultural adaptation, validation, and normalisation. J. Epidemiol. Community Health 2003, 57, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Rasch, D.; Teuscher, F.; Guiard, V. How robust are tests for two independent samples? J. Stat. Plan. Inference 2007, 137, 2706–2720. [Google Scholar] [CrossRef]
- Petridou, A.; Siopi, A.; Mougios, V. Exercise in the management of obesity. Metabolism 2019, 92, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sword, O.D. Exercise as a management strategy for the overweight and obese. Strength Cond. J. 2012, 34, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Nordstoga, A.L.; Zotcheva, E.; Svedahl, E.R.; Nilsen, T.L.; Skarpsno, E.S. Long-term changes in body weight and physical activity in relation to all-cause and cardiovascular mortality: The HUNT study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 45. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.B.; Kim, K.; Kim, C.; Kang, S.J.; Kim, H.J.; Yoon, S.; Shin, Y.A. Effects of exercise on the body composition and lipid profile of individuals with obesity: A systematic review and meta-analysis. JOMES 2019, 28, 278–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toussaint, A.; Husing, P.; Gumz, A.; Wingenfeld, K.; Harter, M.; Schramm, E.; Lowe, B. Sensitivity to change and minimal clinically important difference of the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7). J. Affect. Disord. 2020, 265, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.M.W.; Crane, P.K.; Simon, G. A comparison of individual change using item response theory and sum scoring on the Patient Health Questionnaire-9: Implications for measuremet-based care. Ann. Depress. Anxiety 2019, 6, id1098. [Google Scholar]
- Badhiwala, J.H.; Witiw, C.D.; Nassiri, F.; Akbar, M.A.; Jaja, B.; Wilson, J.R.; Fehlings, M.G. Minimum clinically important difference in SF-36 scores for use in degenerative cervical myelopathy. Spine 2018, 43, E1260–E1266. [Google Scholar] [CrossRef] [PubMed]
- Escobar, A.; Quintana, J.M.; Bilbao, A.; Arostegui, I.; Laufente, I.; Vidaurreta, I. Responsiveness and clinically important differences for the WOMAC and SF-36 after total knee replacement. Osteoarthr. Cartil. 2007, 15, 273–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thichumpa, W.; Howteerakul, N.; Suwannapong, N.; Tantrakul, V. Sleep quality and associated factors among the elderly living in rural Chiang Rai, northern Thailand. Epidemiol. Health 2018, 40, e2018018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, E.; Skinner, M.; Myezwa, H.; Mkumbuzi, V.; Mostert-Wentzel, K.; Perez, D.P.; Shirley, D.; Söderlund, A.; Dornelas de Andrade, A.; Abaraogu, U.O.; et al. Health competency standards in physical therapist practice. Phys. Ther. 2019, 99, 1242–1254. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.Y.M.; Skinner, M.; Dean, E. Evolution of physical therapy education in China and use of simulation-based learning to maximize clinical placement outcomes. Rehabil. Med. 2015, 25, 44–49. [Google Scholar] [CrossRef]
- Tan, X.; Zhang, Y.; Shao, H. Healthy China 2030, a breakthrough for improving health. Glob. Health Promot. 2019, 26, 96–99. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | HIC- Intervention Group | Control Group | p Value |
|---|---|---|---|
| (n = 90) | (n = 81) | ||
| Sex, (men/women) | 17/73 | 22/59 | 0.20 * |
| Age, y (Mean ± SD) | 69.5 ± 8.5 | 67.1 ± 10.7 | 0.16 # |
| 50–59 | 7 (7.8) | 8 (9.9) | |
| 60–69 | 44 (48.9) | 40 (49.4) | |
| 70–79 | 26 (28.9) | 28 (34.6) | |
| 80–89 | 13 (14.4) | 5 (6.2) | |
| Education | 0.72 * | ||
| Illiterate | 11 (12.2) | 6 (7.4) | |
| Primary school | 17 (18.9) | 18 (22.2) | |
| Junior high | 52 (57.8) | 47 (58) | |
| Secondary school | 7 (7.8) | 8 (9.9) | |
| Post-secondary | 2 (2.2) | 1 (1.2) | |
| Smoker | 13 (14.4) | 15 (18.5) | 0.43 * |
| Alcohol (> 1glass/day) | 13 (14.4) | 15 (18.5) | 0.76 * |
| Hypertension * | 31 (34.4%) | 34 (41.9%) | 0.40 * |
| Diabetes * | 13 (14.4%) | 4 (17.3%) | 0.61 * |
| Outcome | Time | HIC-Intervention Group (n = 90) | Control Group (n = 81) | Mean Difference of Between-Group Change Scores (95% CI) (p Value) # | ||
|---|---|---|---|---|---|---|
| Mean Score (SD) | Mean Change from Baseline to Follow-up (SD) (p Value) * | Mean Score (SD) | Mean Change from Baseline to Follow-up (SD) (p Value) * | |||
| BMI (kg/m2) | Baseline | 25.21 (3.42) | 0.40 (0.85) (< 0.001) | 24.99 (2.99) | 0.12 (1.14) (0.353) | 0.28 (−0.02 to 0.58) (0.069) |
| Follow-up | 24.82 (3.39) | 24.88 (2.92) | ||||
| WC (cm) | Baseline | 91.52 (10.18) | 1.57 (6.51) (0.024) | 91.81 (9.00) | 0.70 (6.45) (0.335) | 0.88 (−1.08 to 2.84) (0.379) |
| Follow-up | 89.95 (9.75) | 91.11 (7.64) | ||||
| RBS (mmol/L) | Baseline Follow-up | 7.86 (3.61) 7.92 (3.28) | −0.06 (3.68) (0.874) | 7.02 (2.17) 6.87 (1.80) | 0.15 (2.13) (0.527) | −0.21 (−1.13 to 0.71) (0.650) |
| TC (mmol/l) | Baseline | 4.26 (1.08) | −0.18 (1.16) (0.145) | 4.01 (0.95) | −0.12 (1.03) (0.308) | −0.06 (−0.40 to 0.27) (0.718) |
| Follow-up | 4.44 (1.07) | 4.13 (0.85) | ||||
| SBP (mmHg) | Baseline | 132.80 (14.15) | 0.99 (14.74) (0.526) | 132.74 (12.89) | 2.25 (16.98) (0.237) | −1.26 (−6.05 to 3.53) (0.605) |
| Follow-up | 131.81 (12.99) | 130.49 (14.56) | ||||
| DBP (mmHg) | Baseline | 80.80 (8.18) | 3.60 (9.98) (0.001) | 80.75 (7.93) | 1.69 (12.16) (0.214) | 1.91 (−1.44 to 5.25) (0.262) |
| Follow-up | 77.20 (10.04) | 79.06 (11.76) | ||||
| Parameters | HIC-Intervention Group (n = 90) | Control Group (n = 81) | ||
|---|---|---|---|---|
| Baseline | Follow-up | Baseline | Follow-up | |
| High|Medium|Low | High|Medium|Low | High|Medium|Low | High|Medium|Low | |
| Body mass index | 9|37|44 | 8|34|48 | 5|34|42 | 6|37|38 |
| Random blood sugar | 38|37|15 | 40|37|13 | 31|31|19 | 32|33|16 |
| Total cholesterol | 5|15|70 | 6|13|71 | 3|6|72 | 3|6|72 |
| Blood pressure | 31|45|14 | 25|46|19 | 42|23|15 | 44|21|16 |
| Healthy diet | 4|58|28 | 0|44|46 | 4|43|34 | 3|39|39 |
| Physical activity | 12|28|50 | 4|7|79 | 9|39|33 | 8|38|35 |
| Tobacco use | 5|85 (High|Low) | 5|85 (High|Low) | 9|72 (High|Low) | 9|72 (High|Low) |
| Alcohol use | 0|1|89 | 0|1|89 | 4|2|75 | 4|2|75 |
| Lifestyle Practice | HIC-Intervention Group | Control Group | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-up | Change Number (%) (95%CI) | p Value * | Baseline | Follow-up | Change Number (%) (95%CI) | p Value * | |
| Physical Activity | 50 (55.6%) | 79 (87.8%) | 29 (32.2%) (19.6–44.9%) | <0.001 | 33 (40.7%) | 35 (43.2%) | 2 (2.5%) (−11.6 to 16.6%) | 0.864 |
| Diet | 28 (31.1%) | 46 (51.1%) | 18 (20.0%) (10.7–29.3%) | <0.001 | 34 (42.0%) | 39 (48.1%) | 5 (6.2%) (−1.0 to 13.3%) | 0.180 |
| Physical Activity + Diet | 16 (17.8%) | 42 (46.7%) | 26 (28.9%) (18.1–39.7%) | <0.001 | 12 (14.8%) | 20 (24.7%) | 8 (9.9%) (0.4–19.3%) | 0.077 |
| Out-come | Time | HIC-Intervention Group (n = 90) | Control Group (n = 81) | Mean Difference of Between-Group Change Scores (95% CI) (p Value) # | ||
|---|---|---|---|---|---|---|
| Mean Score (SD) | Mean Change from Baseline to Follow-up (SD) (p Value) * | Mean Score (SD) | Mean Change from Baseline to Follow-up (SD) (p Value) * | |||
| GAD-7 | Baseline | 1.14 (2.26) | −0.02 (1.82) (0.908) | 1.63 (3.23) | 0.30 (2.38) (0.267) | −0.32 (−0.97 to 0.33) (0.332) |
| Follow-up | 1.17 (1.98) | 1.33 (3.04) | ||||
| PHQ-9 | Baseline | 1.72 (2.67) | −0.80 (2.22) (0.001) | 2.42 (3.44) | 0.14 (3.06) (0.400) | −0.94 (−1.74 to −0.13) (0.022) |
| Follow-up | 2.52 (2.97) | 2.28 (2.96) | ||||
| PSQI | Baseline | 7.84 (4.29) | 0.16 (3.83) (0.701) | 8.28 (4.61) | 0.93 (3.70) (0.027) | −0.77 (−1.91 to 0.37) (0.184) |
| Follow-up | 7.69 (4.70) | 7.36 (4.86) | ||||
| SF-36 PCS | Baseline | 82.74 (15.52) | 2.45 (13.96) (0.100) | 80.70 (16.64) | 3.97 (17.54) (0.045) | −1.52 (−6.29 to 3.24) (0.529) |
| Follow-up | 85.18 (12.80) | 84.67 (14.34) | ||||
| SF-36 MCS | Baseline | 90.09 (11.30) | −0.45 (12.34) (0.732) | 86.33 (16.60) | 1.03 (14.65) (0.530) | −1.47 (−5.55 to 2.60) (0.476) |
| Follow-up | 89.64 (10.71) | 87.36 (13.37) | ||||
| Mental Health Parameters | Outcome | HIC-Intervention Group (n = 90) | Control Group (n = 81) | ||
|---|---|---|---|---|---|
| Baseline | Follow-up | Baseline | Follow-up | ||
| Anxiety Severity GAD-7 Scale Score | Minimal, 0–4 | 84 (93.4) | 82 (91.1) | 74 (91.4) | 74 (91.4) |
| Mild, 5–9 Moderate, 10–14 Severe, 16–21 | 4 (4.4) | 8 (8.9) | 4 (4.9) | 5 (6.2) | |
| 2 (2.2) | 0 (0) | 2 (2.5) | 1 (1.2) | ||
| 0 (0) | 0 (0) | 1 (1.2) | 1 (1.2) | ||
| Depression Severity PHQ-9 Scale Score | Minimal, 0–4 | 80 (88.9) | 74 (82.2) | 69 (85.3) | 71 (87.7) |
| Mild, 5–9 | 9 (10.0) | 13 (14.5) | 7 (8.6) | 7 (8.6) | |
| Moderate, 10–14 | 0 (0) | 2 (2.2) | 4 (4.9) | 2 (2.5) | |
| Moderately severe, 15–19 | 1 (1.1) | 1 (1.1) | 0 (0) | 1 (1.2) | |
| Severe, 20–27 | 0 (0) | 0 (0) | 1 (1.2) | 0 (0) | |
| Sleep Quality PSQI Scale Score | Very good, 0–5 | 30 (33.3) | 35 (38.9) | 24 (29.6) | 36 (44.4) |
| Fairly good, 6–10 | 34 (37.8) | 29 (32.2) | 37 (45.7) | 25 (30.9) | |
| Fairly bad, 11–15 | 22 (24.5) | 19 (21.1) | 11 (13.6) | 12 (14.8) | |
| Very Bad, 16–21 | 4 (4.4) | 7 (7.8) | 9 (11.1) | 8 (9.9) | |
| Statements | SA * | A | D | SD | |
|---|---|---|---|---|---|
| 1 | Physiotherapists should introduce the HIC to the general public | 17 (85%) | 3 (15%) | 0 | 0 |
| 2 | I understand the purpose and role of the HIC | 18 (90%) | 2 (10%) | 0 | 0 |
| 3 | I can provide advice to my patients about the actions prescribed on the HIC | 12 (60%) | 8 (40%) | 0 | 0 |
| 4 | I can identify instances where using the HIC would improve patient outcomes | 11 (55%) | 9 (45%) | 0 | 0 |
| 5 | I can justify my reasoning for choosing to implement the HIC with my patients | 10 (50%) | 10 (50%) | 0 | 0 |
| 6 | I understand when using the HIC may NOT be appropriate for a particular patient | 6 (30%) | 14 (70%) | 0 | 0 |
| 7 | I can interpret the results and/or progress a patient using the HIC in an appropriate manner | 14 (70%) | 6 (30%) | 0 | 0 |
| 8 | I have confidence in providing advice to my patients about the actions prescribed on the HIC | 14 (70%) | 6 (30%) | 0 | 0 |
| 9 | It is useful to my learning to have the opportunity to follow up the same patient each month | 17(85%) | 3 (15%) | 0 | 0 |
| 10 | I found the HIC to be a useful tool for me to work with the patient | 15 (75%) | 5 (25%) | 0 | 0 |
| 11 | The HIC makes it easy for me to set healthy lifestyle targets for the patient | 14 (70%) | 6 (30%) | 0 | 0 |
| 12 | Participation in this HIC project has given me some understanding of the physiotherapist’s role in the community | 19 (95%) | 1 (5%) | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, Y.; Wu, X.; Tsang, R.C.; Yun, R.; Lu, Y.; Dean, E.; Jones, A.Y. A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative. Int. J. Environ. Res. Public Health 2020, 17, 8065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218065
Bai Y, Wu X, Tsang RC, Yun R, Lu Y, Dean E, Jones AY. A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative. International Journal of Environmental Research and Public Health. 2020; 17(21):8065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218065
Chicago/Turabian StyleBai, Yiwen, Xubo Wu, Raymond CC Tsang, Ruisheng Yun, Yan Lu, Elizabeth Dean, and Alice YM Jones. 2020. "A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative" International Journal of Environmental Research and Public Health 17, no. 21: 8065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218065