Racial/Ethnic Discrimination and Intimate Partner Violence Perpetration in Latino Men: The Mediating Effects of Mental Health


Abstract
:1. Introduction
2. Racial/Ethnic Discrimination and Intimate Partner Violence Perpetration
3. Mental Health and Intimate Partner Violence Perpetration
4. Mental Health as a Mediator
5. Rationale for Current Study
6. Methods
6.1. Participants
6.2. Measures
6.2.1. Racial/Ethnic Discrimination
6.2.2. Mental Health
Anxiety Symptoms
Depression Symptoms
Posttraumatic Stress Symptoms
Alcohol Dependence Symptoms
Drug Dependence Symptoms
6.2.3. Intimate Partner Violence Perpetration
6.2.4. Immigrant Status
6.2.5. Covariates
6.2.6. Data Analysis
7. Results
7.1. Correlations
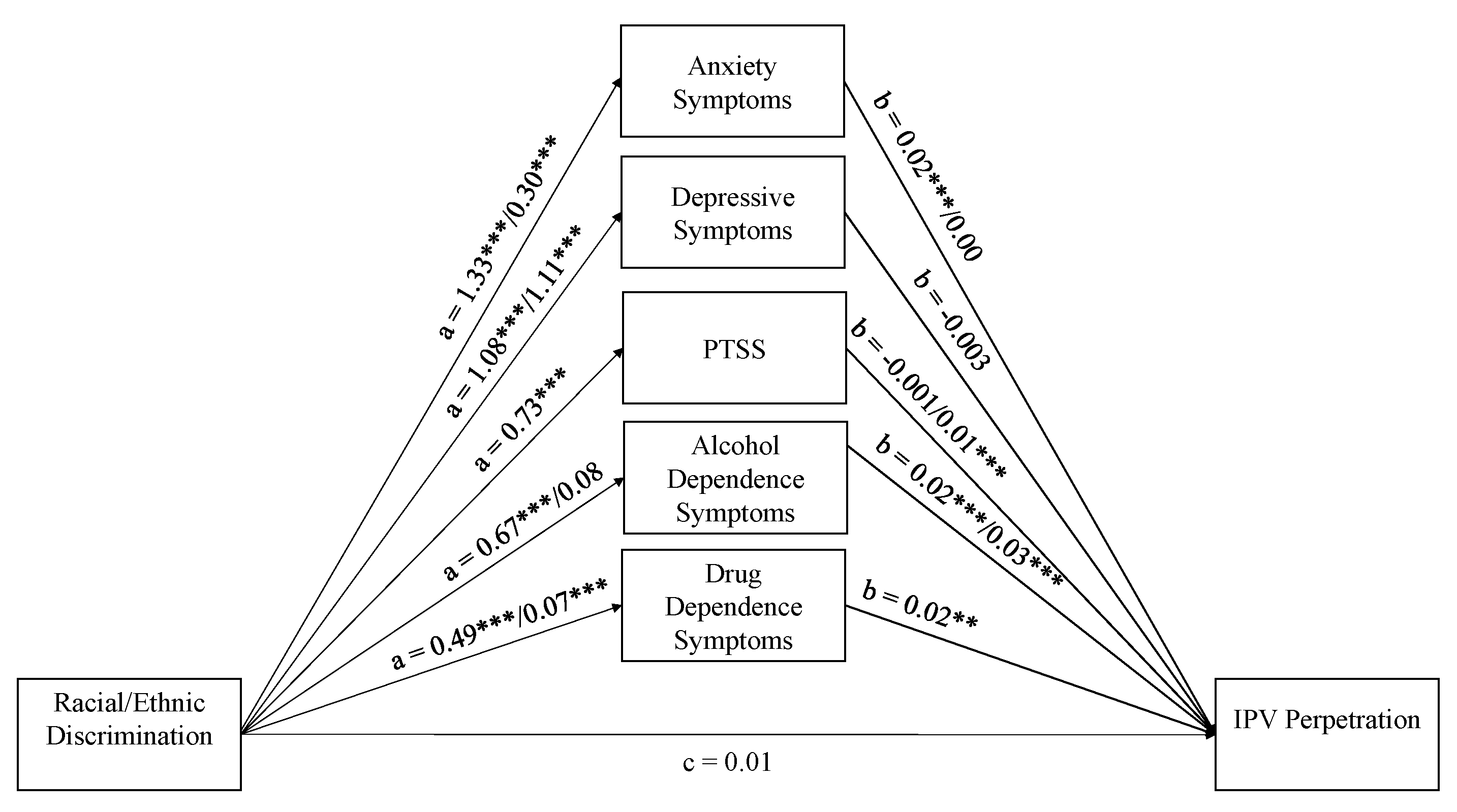
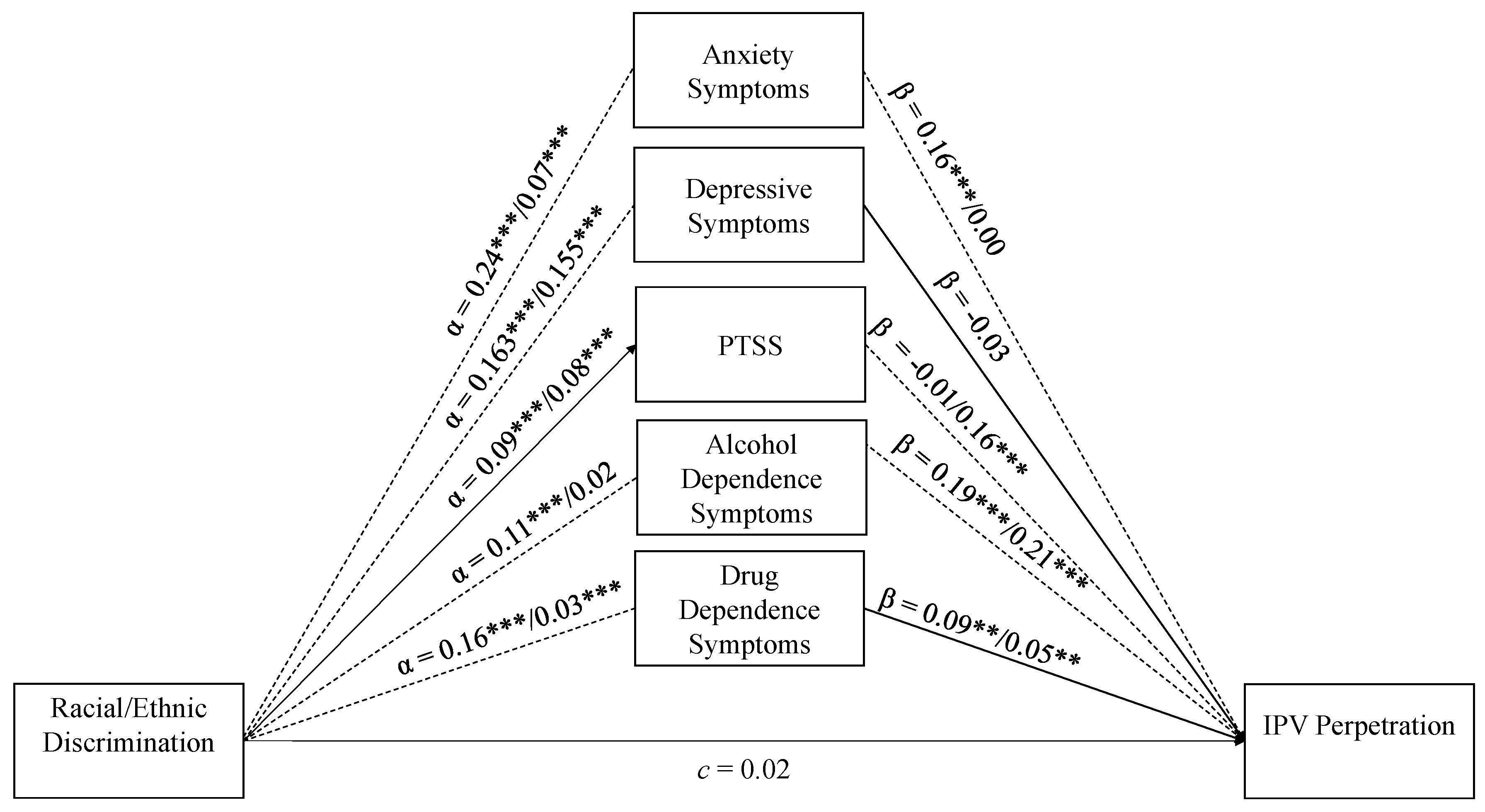
7.2. Multi-Group Structural Equation Model
7.3. Anxiety Symptoms
7.4. Depression Symptoms
7.5. Posttraumatic Stress Symptoms
7.6. Alcohol Dependence Symptoms
7.7. Drug Dependence Symptoms
7.8. Direct Effect
8. Discussion
8.1. Limitations
8.2. Implications
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Carrigan, W.D.; Webb, C. The Lynching of Persons of Mexican Origin or Descent in the United States, 1848 to 1928. J. Soc. Hist. 2003, 37, 411–438. [Google Scholar] [CrossRef]
- Hernández, K.L. Migra! A History of the U.S. Border Patrol, 1st ed.; University of California Press: Berkeley, CA, USA, 2010. [Google Scholar]
- Menchaca, M. The Mexican Outsiders: A Community History of Marginalization and Discrimination in California; University of Texas Press: Austin, TX, USA, 1995. [Google Scholar]
- Pew Research Center. More Latinos Have Serious Concerns about Their Place in America Under Trump; Pew Research Center: Washington, DC, USA, 2018. [Google Scholar]
- Pew Research Center. From 200 Million to 300 Million: The Numbers behind Population Growth; Pew Research Center: Washington, DC, USA, 2006. [Google Scholar]
- Pew Research Center. U.S. Hispanic Population Surpassed 60 Million in 2019, but Growth Has Slowed; Pew Research Center: Washington, DC, USA, 2020. [Google Scholar]
- Pew Research Center. Hispanic Population in the United States Statistical Portrait, 2015; Pew Research Center: Washington, DC, USA, 2017. [Google Scholar]
- Black, M.C.; Basile, K.C.; Breiding, M.J.; Smith, S.G.; Walters, M.L.; Merrick, M.T.; Chen, J.; Stevens, M.R. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report; National Center for Injury Prevention and Control, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2011. [Google Scholar]
- Okuda, M.; Olfson, M.; Wang, S.; Rubio, J.M.; Xu, Y.; Blanco, C. Correlates of intimate partner violence perpetration: Results from a national epidemiologic survey. J. Trauma Stress 2015, 28, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Caetano, R.; Cunradi, C.B.; Schafer, J.; Clark, C.L. Intimate partner violence and drinking patterns among white, black, and Hispanic couples in the US. J. Subst. Abus. 2000, 11, 123–138. [Google Scholar] [CrossRef]
- Reingle, J.M.; Jennings, W.G.; Connell, N.M.; Businelle, M.S.; Chartier, K. On the pervasiveness of event-specific alcohol use, general substance use, and mental health problems as risk factors for intimate partner violence. J. Interpers. Violence 2014, 29, 2951–2970. [Google Scholar] [CrossRef] [PubMed]
- Afifi, T.; Mota, N.; Sareen, J.; MacMillan, H. The relationships between harsh physical punishment and child maltreatment in childhood and intimate partner violence in adulthood. BMC Public Health 2017, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunradi, C.B. Drinking level, neighborhood social disorder, and mutual intimate partner violence. Alcohol. Clin. Exp. Res. 2007, 31, 1012–1019. [Google Scholar] [CrossRef] [PubMed]
- Field, C.A.; Caetano, R. Longitudinal Model Predicting Partner Violence Among White, Black, and Hispanic Couples in the United States. Alcohol. Clin. Exp. Res. 2003, 27, 1451–1458. [Google Scholar] [CrossRef] [Green Version]
- Field, C.A.; Caetano, R. Longitudinal Model Predicting Mutual Partner Violence Among White, Black, and Hispanic Couples in the United States General Population. Violence Vict. 2005, 20, 499–511. [Google Scholar] [CrossRef]
- Caetano, R.; Vaeth, P.A.C.; Ramisetty-Mikler, S. Intimate partner violence victim and perpetrator characteristics among couples in the United States. J. Fam. Violence 2008, 23, 507–518. [Google Scholar] [CrossRef]
- Cunradi, C.B.; Ames, G.M.; Duke, M. The relationship of alcohol problems to the risk for unidirectional and bidirectional intimate partner violence among a sample of blue-collar couples. Violence Vict. 2011, 26, 147–158. [Google Scholar] [CrossRef] [Green Version]
- McMahon, K.; Hoertel, N.; Wall, M.M.; Okuda, M.; Limosin, F.; Blanco, C. Childhood maltreatment and risk of intimate partner violence: A national study. J. Psychiatr. Res. 2015, 69, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Tjaden, P.; Thoennes, N. Prevalence and consequences of male-to-female and female-to-male intimate partner violence as measured by the National Violence Against Women Survey. Violence Against Women 2000, 6, 142–161. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. The Social-Ecological Model: A Framework for Prevention. Available online: https://www.cdc.gov/violenceprevention/publichealthissue/social-ecologicalmodel.html (accessed on 5 May 2020).
- Heise, L.L. Violence Against Women: An Integrated, Ecological Framework. Violence Against Women 1998, 4, 262–290. [Google Scholar] [CrossRef]
- Forster, M.; Grigsby, T.J.; Soto, D.W.; Sussman, S.Y.; Unger, J.B. Perceived Discrimination, Cultural Identity Development, and Intimate Partner Violence Among a Sample of Hispanic Young Adults. Cult. Divers. Ethn. Minority Psychol. 2017, 23, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Reed, E.; Silverman, J.; Ickovics, J.; Gupta, J.; Welles, S.; Santana, M.; Raj, A. Experiences of Racial Discrimination & Relation to Violence Perpetration and Gang Involvement among a sample of Urban African American Men. J. Immigr. Minority Health 2010, 12, 319. [Google Scholar]
- Spencer, C.; Mallory, A.B.; Cafferky, B.M.; Kimmes, J.G.; Beck, A.R.; Stith, S.M. Mental health factors and intimate partner violence perpetration and victimization: A meta-analysis. Psychol. Violence 2019, 9, 1–17. [Google Scholar] [CrossRef]
- Cafferky, B.M.; Mendez, M.; Anderson, J.R.; Stith, S.M. Substance use and intimate partner violence: A meta-analytic review. Psychol. Violence 2018, 8, 110. [Google Scholar] [CrossRef]
- Vaughn, M.G.; Salas-Wright, C.P.; Cooper-Sadlo, S.; Maynard, B.R.; Larson, M. Are Immigrants More Likely Than Native-Born Americans to Perpetrate Intimate Partner Violence? J. Interpers. Violence 2015, 30, 1888–1904. [Google Scholar] [CrossRef]
- Carter, R.T.; Johnson, V.E.; Kirkinis, K.; Roberson, K.; Muchow, C.; Galgay, C. A meta-analytic review of racial discrimination: Relationships to health and culture. Race Soc. Probl. 2019. [Google Scholar] [CrossRef]
- Paradies, Y.; Ben, J.; Denson, N.; Elias, A.; Priest, N.; Pieterse, A.; Gupta, A.; Kelaher, M.; Gee, G. Racism as a Determinant of Health: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Pascoe, E.A.; Richman, L.S. Perceived Discrimination and Health: A Meta-Analytic Review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [Green Version]
- Chou, T.; Asnaani, A.; Hofmann, S.G. Perception of racial discrimination and psychopathology across three US ethnic minority groups. Cult. Divers. Ethn. Minority Psychol. 2012, 18, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.L.; Ahn, S. Discrimination Against Latina/os: A Meta-Analysis of Individual-Level Resources and Outcomes. Couns. Psychol. 2012, 40, 28–65. [Google Scholar] [CrossRef]
- Torres, L.; Ong, A.D. A daily diary investigation of latino ethnic identity, discrimination, and depression. Cult. Divers. Ethn. Minority Psychol. 2010, 16, 561–568. [Google Scholar] [CrossRef] [Green Version]
- Finch, B.K.; Kolody, B.; Vega, W.A. Perceived Discrimination and Depression among Mexican-Origin Adults in California. J. Health Soc. Behav. 2000, 41, 295. [Google Scholar] [CrossRef]
- Grant, B.F.; Kaplan, K.D. Source and Accuracy Statement for the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions; National Institute on Alcohol Abuse and Alcoholism: Rockville, MD, USA, 2005. [Google Scholar]
- Grant, B.F.; Dawson, D.A. Introduction to the National Epidemiologic Survey on Alcohol and Related Conditions. Alcohol Res. Health 2006, 29, 74. [Google Scholar]
- Krieger, N.; Smith, K.; Naishadham, D.; Hartman, C.; Barbeau, E.M. Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. 2005, 61, 1576–1596. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Grant, B.F.; Goldstein, R.B.; Smith, S.M.; Jung, J.; Zhang, H.; Chou, S.P.; Pickering, R.P.; Ruan, W.J.; Huang, B.; Saha, T.D. The Alcohol Use Disorder and Associated Disabilities Interview Schedule-5 (AUDADIS-5): Reliability of substance use and psychiatric disorder modules in a general population sample. Drug Alcohol Depend. 2015, 148, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straus, M.A.; Douglas, E.M. A Short Form of the Revised Conflict Tactics Scales, and Typologies for Severity and Mutuality. Violence Vict. 2004, 19, 507–520. [Google Scholar] [CrossRef]
- Reiss, F.; Meyrose, A.-K.; Otto, C.; Lamper, T.T.; Klasen, F.; Ravens-Sieberer, U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: Results of the German BELLA cohort-study. PLoS ONE 2019, 14, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Yoon, E.; Chang, C.-T.; Kim, S.; Clawson, A.; Cleary, S.E.; Hansen, M.; Bruner, J.P.; Chan, T.K.; Gomes, A.M. A meta-analysis of acculturation/enculturation and mental health. J. Couns. Psychol. 2013, 60, 15–30. [Google Scholar] [CrossRef]
- Caetano, R.; Ramisetty-Mikler, S.; Caetano Vaeth, P.A.; Harris, T.R. Acculturation Stress, Drinking, and Intimate Partner Violence among Hispanic Couples in the U.S. J. Interpers. Violence 2007, 22, 1431–1447. [Google Scholar] [CrossRef]
- Kimber, M.; Henriksen, C.; Davidov, D.; Goldstein, A.; Pitre, N.; Tonmyr, L.; Afifi, T. The association between immigrant generational status, child maltreatment history and intimate partner violence (IPV): Evidence from a nationally representative survey. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1135–1144. [Google Scholar] [CrossRef] [Green Version]
- Marin, G.; Sabogal, F.; Marin, B.V.; Otero-Sabogal, R.; Perez-Stable, E.J. Development of a short acculturation scale for Hispanics. Hisp. J. Behav. Sci. 1987, 9, 183–205. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Ryu, E.; Cheong, J. Comparing Indirect Effects in Different Groups in Single-Group and Multi-Group Structural Equation Models. Front. Psychol. 2017, 8, 747. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Oberski, D. lavaan. survey: An R package for complex survey analysis of structural equation models. J. Stat. Softw. 2014, 57, 1–27. [Google Scholar] [CrossRef] [Green Version]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [Green Version]
- DiStefano, C.; Morgan, G.B. A comparison of diagonal weighted least squares robust estimation techniques for ordinal data. Struct. Equ. Model. Multidiscip. J. 2014, 21, 425–438. [Google Scholar] [CrossRef]
- Teruya, S.A.; Bazargan-Hejazi, S. The Immigrant and Hispanic Paradoxes: A Systematic Review of Their Predictions and Effects. Hisp. J. Behav. Sci. 2013, 35, 486–509. [Google Scholar] [CrossRef]
- Perreira, K.M.; Ornelas, I. Painful Passages: Traumatic Experiences and Post-Traumatic Stress among Immigrant Latino Adolescents and their Primary Caregivers. Int. Migr. Rev. 2013, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancera, B.M.; Dorgo, S.; Provencio-Vasquez, E. Risk Factors for Hispanic Male Intimate Partner Violence Perpetration. Am. J. Men’s Health 2017, 11, 969–983. [Google Scholar] [CrossRef] [Green Version]
- Cunradi, C.B. Intimate Partner Violence Among Hispanic Men and Women: The Role of Drinking, Neighborhood Disorder, and Acculturation-Related Factors. Violence Vict. 2009, 24, 83–96. [Google Scholar] [CrossRef]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A.; Vu, C. Understanding how discrimination can affect health. Health Serv. Res. 2019, 54, 1374–1388. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.R.; Mohammed, S.A. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2009, 32, 20–47. [Google Scholar] [CrossRef] [Green Version]
- Bryant-Davis, T.; Ocampo, C. A therapeutic approach to the treatment of racist-incident-based trauma. J. Emot. Abus. 2006, 6, 1–22. [Google Scholar] [CrossRef]
- Comas-Diaz, L. Ethnopolitical Psychology: Healing and Transformation; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2007. [Google Scholar]
- Dunbar, E. Counseling practices to ameliorate the effects of discrimination and hate events: Toward a systematic approach to assessment and intervention. Couns. Psychol. 2001, 29, 281–310. [Google Scholar] [CrossRef]
- Carter, R.T. Racism and psychological and emotional injury: Recognizing and assessing race-based traumatic stress. Couns. Psychol. 2007, 35, 13–105. [Google Scholar] [CrossRef]
- Comas-Díaz, L. Racial Trauma Recovery: A Race-Informed Therapeutic Approach to Racial Wounds; American Psychological Association: Washington, DC, USA, 2016. [Google Scholar]
- Taft, C.T.; Murphy, C.M.; Creech, S.K. Trauma-Informed Treatment and Prevention of Intimate Partner Violence; American Psychological Association: Washington, DC, USA, 2016. [Google Scholar]
- Murphy, C.M.; Richards, T.N.; Nitsch, L.M.; Green-Manning, A.; Brokmeier, A.M.; LaMotte, A.D.; Holliday, C.N. Community-Informed Relationship Violence Intervention in a High-Stress, Low-Income Urban Context; 2020; Under Review. [Google Scholar]
- Clark, R.; Anderson, N.B.; Clark, V.R.; Williams, D.R. Racism as a stressor for African Americans: A biopsychosocial model. Am. Psychol. 1999, 54, 805. [Google Scholar] [CrossRef]
- Harrell, S.P. A multidimensional conceptualization of racism-related stress: Implications for the well-being of people of color. Am. J. Orthopsychiatry 2000, 70, 42–57. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall Sample (N = 2287) | Latino Immigrants (n = 1187) | U.S.-Born Latinos (n = 1077) | ||
|---|---|---|---|---|
| % | % | % | pb | |
| Less than high school a | 35.3% | 48.5% | 17.1% | <0.001 |
| High school or equivalent a | 24.4% | 22.3% | 27.3% | ns |
| At least some college a | 40.2% | 29.2% | 55.6% | <0.001 |
| M (SE) | M (SE) | M (SE) | p | |
| Age | 40.54 (0.52) | 41.00 (0.79) | 40.04 (0.65) | ns |
| Language-based Acculturation | 2.99 (0.06) | 2.15 (0.04) | 4.16 (0.05) | <0.001 |
| Discrimination | 0.18 (0.02) | 0.16 (0.02) | 0.22 (0.02) | 0.024 |
| Anxiety Symptoms | 0.38 (0.06) | 0.25 (0.05) | 0.55 (0.12) | 0.021 |
| Depressive Symptoms | 0.83 (0.08) | 0.72 (0.09) | 0.99 (0.14) | ns |
| PTSS | 0.52 (0.07) | 0.49 (0.11) | 0.55 (0.08) | ns |
| Alcohol dependence symptoms | 1.05 (0.07) | 0.78 (0.08) | 1.41 (0.10) | <0.001 |
| Drug dependence symptoms | 0.16 (0.03) | 0.07 (0.02) | 0.28 (0.05) | <0.001 |
| IPV Perpetration a | 0.07 (0.01) | 0.05 (0.22) | 0.06 (0.23) | ns |
| RD | AS | DS | PTSS | ADS | DDS | IPV a | Edu | LBA | |
|---|---|---|---|---|---|---|---|---|---|
| Racial Discrimination (RD) | 0.24 *** | 0.16 * | 0.12 *** | 0.10 *** | 0.15 *** | 0.07 * | 0.02 | −0.09 ** | |
| Anxiety Symptoms (AS) | 0.07 | 0.45 *** | 0.34 *** | 0.05 | 0.06 | 0.15 ** | −0.02 | 0.01 | |
| Depression Symptoms (DS) | 0.16 *** | 0.37 *** | 0.25 *** | 0.14 ** | 0.17 * | 0.09 ** | −0.01 | 0.05 | |
| Post-traumatic Stress Symptoms (PTSS) | 0.07 * | 0.15 * | 0.22 *** | 0.09 * | 0.15 ** | 0.06 | 0.02 | −0.02 | |
| Alcohol Dependence Symptoms (ADS) | 0.02 | 0.07 | 0.08 * | 0.08 | 0.47 *** | 0.23 *** | −0.04 | 0.07 * | |
| Drug Dependence Symptoms (DDS) | 0.05 | 0.05 | 0.34 *** | 0.02 | 0.17 *** | 0.19 *** | −0.09 *** | 0.01 | |
| Intimate Partner Violence a (IPV) | 0.05 | 0.04 | 0.03 | 0.18 *** | 0.24 *** | 0.08 * | −0.01 | 0.06 * | |
| Education (Edu) | 0.05 | 0.03 | 0.00 | 0.00 | −0.01 | 0.03 * | −0.05 * | 0.32 *** | |
| Language-based Acculturation (LBA) | 0.12 *** | 0.04 | 0.05 | 0.02 | 0.06 | 0.10 ** | 0.06 * | 0.48 *** |
| U.S.-Born Latinos | Latino Immigrants | |||||
|---|---|---|---|---|---|---|
| Variable | Indirect Effect | Lower CI a | Upper CI a | Indirect Effect | Lower CI a | Upper CI a |
| Anxiety | 0.022 | 0.013 | 0.031 | 0.0001 | −0.0012 | 0.0015 |
| Depression | −0.0030 | −0.0065 | 0.0001 | −0.0031 | −0.0068 | 0.0002 |
| PTSS | 0.009 | 0.005 | 0.015 | −0.0007 | −0.0028 | 0.0012 |
| Alcohol Dependence | 0.012 | 0.007 | 0.019 | 0.002 | −0.003 | 0.008 |
| Drug Dependence | 0.008 | 0.003 | 0.014 | 0.0012 | 0.0004 | 0.0023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maldonado, A.I.; Cunradi, C.B.; Nápoles, A.M. Racial/Ethnic Discrimination and Intimate Partner Violence Perpetration in Latino Men: The Mediating Effects of Mental Health. Int. J. Environ. Res. Public Health 2020, 17, 8148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218148
Maldonado AI, Cunradi CB, Nápoles AM. Racial/Ethnic Discrimination and Intimate Partner Violence Perpetration in Latino Men: The Mediating Effects of Mental Health. International Journal of Environmental Research and Public Health. 2020; 17(21):8148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218148
Chicago/Turabian StyleMaldonado, Ana Isabel, Carol B. Cunradi, and Anna María Nápoles. 2020. "Racial/Ethnic Discrimination and Intimate Partner Violence Perpetration in Latino Men: The Mediating Effects of Mental Health" International Journal of Environmental Research and Public Health 17, no. 21: 8148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218148