Health Care Workers’ Perspectives of the Influences of Disrespectful Maternity Care in Rural Kenya



Abstract
:1. Introduction
2. Methods
2.1. Study Context
2.2. Study Sample Participants
2.3. Methods
2.4. Interview Process
2.5. Data Management and Analysis
3. Findings
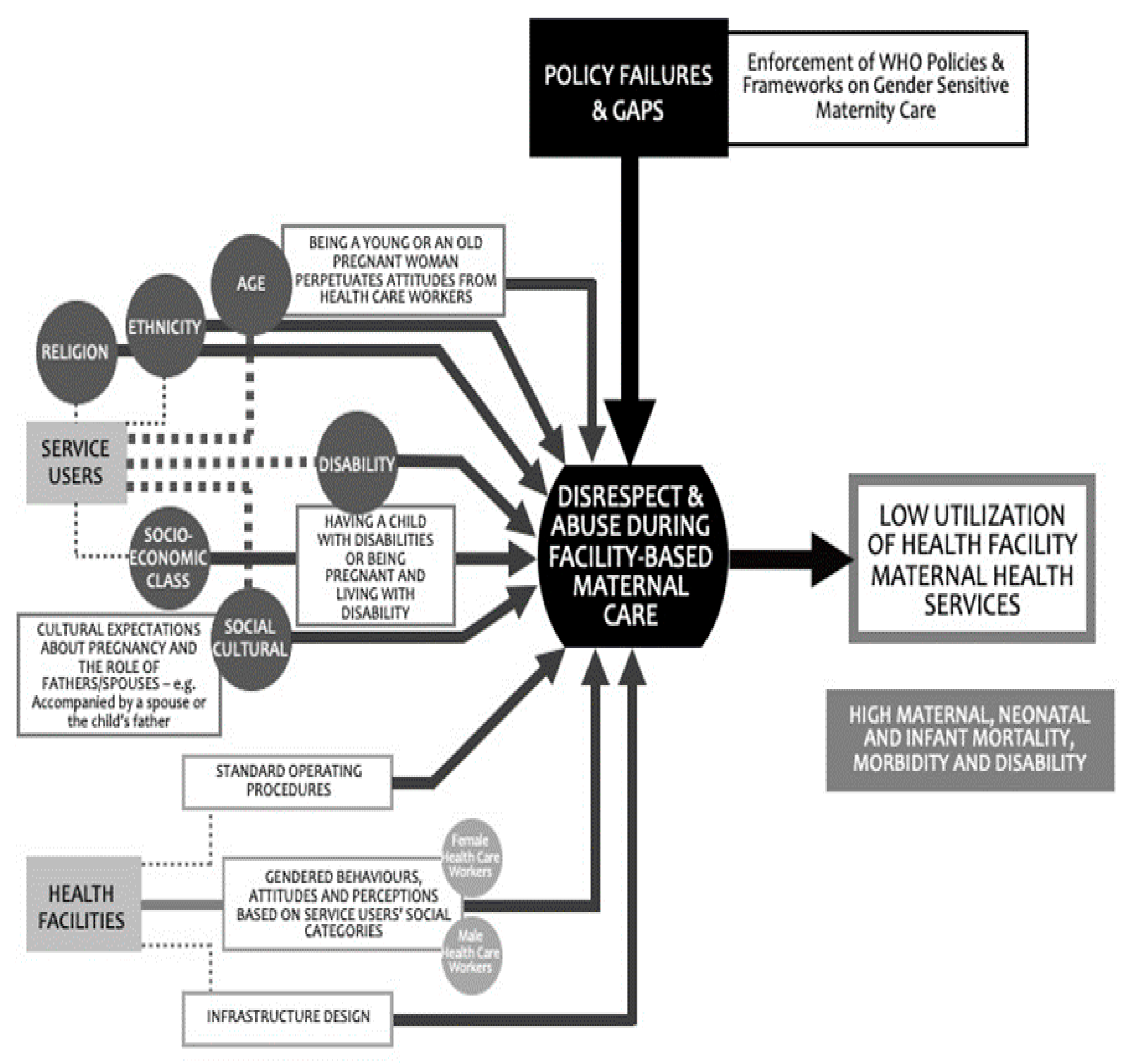
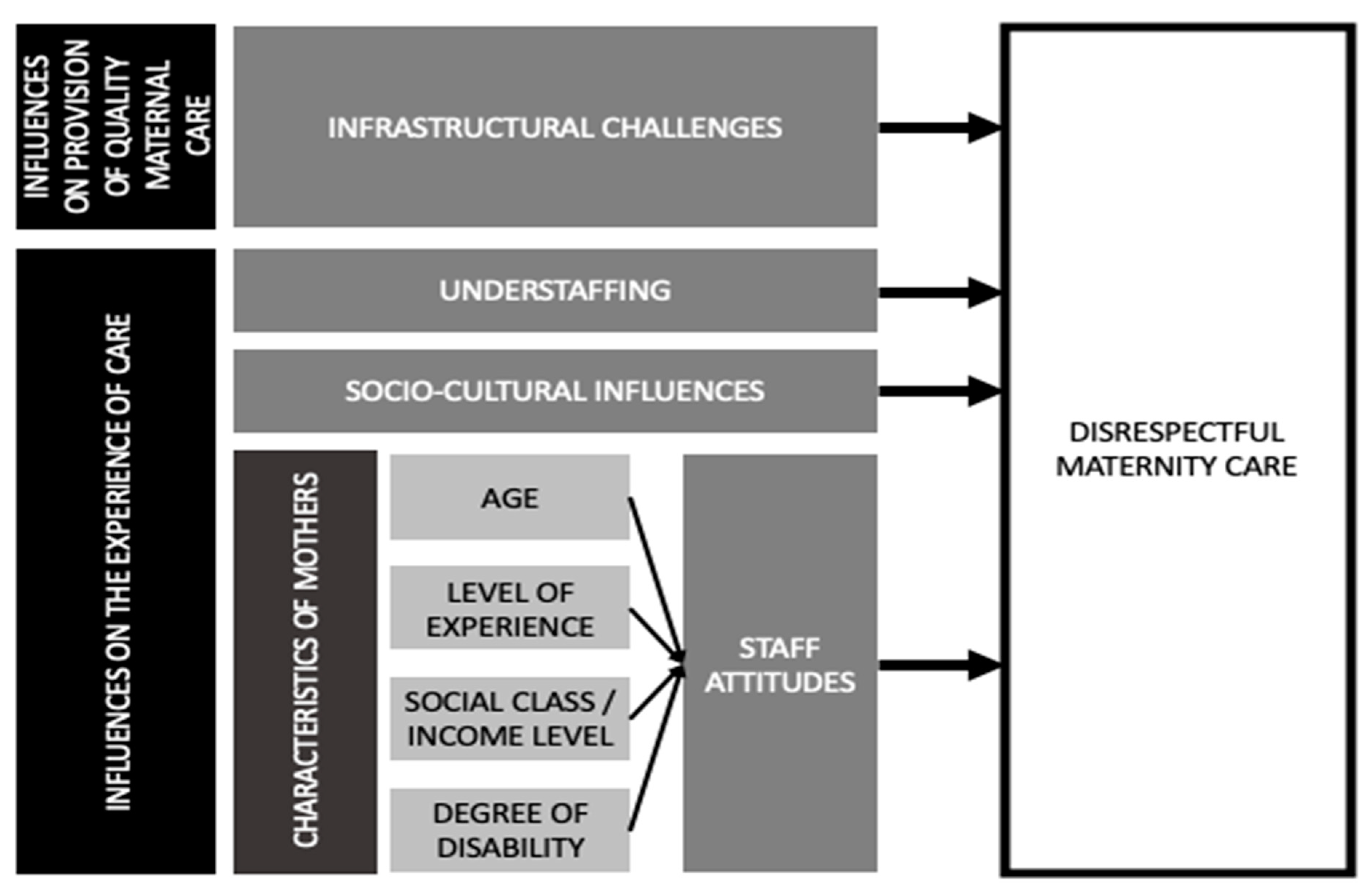
- Infrastructural challenges, including a lack of privacy spaces, equipment, and commodities, hindered the provision of respectful maternity care.
- Understaffing of health care workers due to health worker shortages at the study facilities caused burnout and fatigue and resulted in frustrations that were reflected in poor attitudes towards clients.
- Sociocultural differences between health care workers and clients surrounding birthing preferences, expectations, and practices caused communication barriers and tension.
- Health care workers’ poor attitudes towards clients based on the social and economic status of the clients, including age, disability, and wealth (i.e., poor mothers were more likely to experience DMC; adolescent mothers were likely to be judged harshly by HCWs, as they disapproved of them for becoming pregnant at an early age; mothers living with disabilities were also likely to be discriminated against).
3.1. Infrastructural Challenges
3.1.1. Lack of Privacy Spaces
“…I see it’s challenging, because of space, our facility not enough. So, we, I have an idea that a mother in labor or delivery, I should offer that privacy …”IDI: Nurse–Kilifi
“…for privacy we need, we’ll need space, which is very important, because we are having very many mothers who actually need service. We have even the doctors, they don’t have anywhere to do their examination, they are using the same couch; so, I think the most important thing to be done here in xxx hospital is space, we need space for that…”IDI: Nurse–Kilifi
3.1.2. Lack of Equipment and Commodities
“…This mother may not know, but for our case we know that we don’t have enough equipment. So it was a challenge because you go ahead using the surgical plate and code gloves. Yes. Because these other ones they have to go through the process of sterilization then to be reused. Contamination all those…”IDI: Nurse–Kisii
“…The first thing, if we can get enough equipment which is needed in the maternity. Secondly, we need like there’s supposed to be a screen when a mother is in the delivery couch even the sub staff who is doing cleaning should not see that mother…”IDI: Nurse–Kisii
“… availability of maternity commodities, at times you may get stock-outs, things like cotton, they may get out of stock, things like gauze ….”IDI: Nursing Officer–Kilifi
3.2. Understaffing
3.2.1. High Patient-Staff Ratios
“…shortage of staff it comes in, suppose the person is alone there are many active cases, now that also contributes, there are burnouts…”IDI: Nurse–Kisii
“…You find another mother wants to deliver, there’s another one who’s bleeding on the other side, the child is having fever on the other side, you see they are competing tasks. You find that if it is a staff who is alone, you find now is overwhelmed and a staff who has been overwhelmed can talk anything…”IDI: Nurse–Kisii
“…This staff is alone, or they are two and they have more clients or many clients in labor and they have to attend to all of them. So that one can bring that tension....”IDI: Nurse–Kilifi
“In many facilities, yes, you can get it that maybe, a staff has 5 mothers, and you are only one staff who is operating in that room. You want to take care of the Post Natal Care department and then laboring those who are still in first stage of labor and you are the same nurse who is supposed to conduct the deliveries, obviously you will be overwhelmed.”IDI: Nurse–Kilifi
3.2.2. Burnout and Fatigue
“… now for example in our setup here, you find yourself during the whole night, you are alone, so you handle this case, this case, this case, even you yourself you find that you don’t have that strength let’s say, or you get tired, explaining to that mother that I want us to do this, and this, and this, so because of that you will find that someone doesn’t have even that morale of explaining because you find that they do a lot of work, and they are tired…”IDI: Nurse–Kisii
“…Also to get enough staff because when you are alone even if you provide it reaches a time you get tired and yet you have clients, so it means you will not provide quality services…”IDI: Nurse–Kisii
“…you know sometimes you get a person doing a lot of work, you can say we were two on duty and then we have like five deliveries, or two deliveries, so if somebody comes, at around 5 am in the morning, so you find the nurse is already tired, so if a mother comes let’s say a preemie, she is told push, push then she is not up to what she wants, you’ll find her shouting at her “I wasn’t there when you got pregnant” something like that…”IDI: Nurse–Kisii
3.3. Sociocultural Influences
3.3.1. Client Preferences for Female Health Care Workers
“…like when you get the Somalis a man could not deliver this mother…”
“…What I think about it, she might need this man, the woman to deliver her but in the real sense the female staff is not there. So, this one as I have said, they need to be health educated, to be, those about the, about the cultures…”IDI-Nurse–Kisii
“…Okay, here in our setup, they most likely women to deliver them…”
“…Yes, because of the, I can also call the tradition; it’s a traditional belief woman believe that a man cannot look at me…”IDI: Nurse–Kisii
“…With that study, have, okay I only experienced it when I was working in [xxx] county where a mother could come, a pregnant mother, the Somalis and prefer a female nurse to attend to the same as compared to this other communities…”IDI: Nurse–Kilifi
3.3.2. Women’s Cultural Beliefs and Practices Regarding Birthing Practices
“…Okay me what I can say about the cultural beliefs what is supposed to be done this people need to be educated. About the cultural beliefs, about the norms, because you cannot encourage them to continue practicing, to continue practicing the, to continue with their norms. So, if it’s delivery, if it’s delivery but not herbs me what I can say in delivery…”IDI: Nurse–Kisii
“…Okay, like in where we are, a negative believe if I may take, like the believe, if you don’t deliver within the time they consider the right time there are those concoctions they normally take and if they take those concoctions, of course there are those, the precautions about the baby so, those are things that we will advise them on the negatives about whatever they take…”IDI: Nurse–Kilifi
3.3.3. Women’s Preference for Home Deliveries
“A mother who has been forced to come deliver at the hospital, maybe she is used to squatting, sometimes they do squat, she tells you, I am used to delivering while squatting and maybe you want her to lie on the beds available so she can’t squat. And if you tell her she resists, so it forces you to be harsh for her to lie in the position you can manage to support the baby, something like that.”IDI: Nurse–Kilifi
“…Mostly, these women they give birth at home, the previous pregnancies, many of the previous babies they give birth at home so if you see this woman has come to the hospital she has maneuvered herself there at home, until she has known that, I won’t deliver by myself at home, so, she comes. So, if she comes there, she is like she has delivered children, so, for a health worker and there is that feeling, so, you expect that woman is used to deliver, is the same woman who is like behaving funny... So, you are trying to advice, but she can’t take that advice … so, she looks like you are treating her as if she has not got some babies before…”IDI: Nurse–Kilifi
“…Yes, there are beliefs in the community, but for example there is a belief, issues of substitution, for example if they eat eggs, they are going to be very fat and there are religions which don’t allow people to deliver in a health facility...”IDI: Nurse–Kisii
3.4. Staff Attitudes Towards Marginalized Women
3.4.1. Health Care Workers’ Attitudes Influenced by Women’s Socioeconomic Status
“…These low economic mothers they just come the way they are. You may get the mother is coming to deliver, when you see this mother she has not even taken bath, so from there the service provider goes ahead to tell the mother that you have to take a bath before you deliver. There is water there, do what, shower. And yet there are other mothers who are there to deliver. So this mother who is with that information feeling that she has not been handled well…”IDI: Nurse–Kisii
“…Okay, I may not say I have experienced it or I have, but in me I think also because some of this things, the triggers of this things it depends also with the approach of the, of the client because there are times you find there are those learned clients who come very pushy and in the process things may come up to be negative, so you see that somebody who has a high social status. So, but okay usually that could be also possible the low social status…”IDI: Nurse–Kilifi
“…So, it is true, some people judge mothers they will give very good and quality care to mothers who maybe looked maybe look to be they are employed teachers or those who look to be economically…”IDI: Nurse–Kilifi
“…with this issue of classifying mothers depending on their social standards of life is an aspect that is there. So, a mother comes and the other one is, belongs to the higher standard of, social standards of life, then the preference of the, the health provider, health provider, service provider will attend to the one who is well off than the other one…”IDI: Nurse–Kilifi
3.4.2. Disability
“…Okay these disabled mothers, before the service provider, the problem we have are that we judge this mother before we get the information. Like now you may get that the service provider thinks that this mother cannot deliver normally. So before you get the whole information, you just tell the mother no you go to the facility that has theater. So you have informed the mother what is not there and maybe you get this mother already she has other two babies she has delivered normally but you see she is unable you just judge it and you decide what to happen…”IDI: Nurse–Kisii
“…No, I think they are given the best service those that I have witnessed. Because there is that empathy you feel for that…”IDI: Nurse–Kilifi
“…this disabled mother or this the poor mother the rich one, all of them there’s that what we call equality and there’s that what we call first come first served. You can’t abandon the, or you can’t ignore the poor mother or the disabled and you run for the woman who has a car. So, to me I don’t see…”IDI: Nurse–Kisii
3.4.3. HCW Attitudes towards Young Adolescent Pregnant Women
“…Youth, the adolescents…”
“…They are young, and they are the most at risk, so if you don’t handle well, they see it as lack of respect…”
“…Because they don’t even know how to express themselves, and also the attitude we have, that they are so young they are supposed to be maybe in school, they engaged in premarital sex at a tender age…”IDI: Nurse–Kisii
“…An adolescent mother, I mean, girl who has gotten pregnancy and at the age of where she is supposed to be still in school and whoever be is in the ANC clinic is somebody who is aged at the age of her mother, sometimes they start some kind of stigma like: why are you here? Why do ask? Why have you come to this place? You know there is that attitude, it is the attitude for the staff, which is against the professional code of ethics, but it is instilled in them. So, it is like she is going to ask more questions that are relating to very specific personal needs apart from those which are generalized as per the condition this young mother has come for, simply because of the stigma and attitude that mother, I mean that health worker has towards that client. Yes, it is there…”IDI: Nurse–Kilifi
“…Teenagers, some, there are some who can treat them like it’s not me who got you pregnant, and such things, you are a student, but it is not good. You just take them because it has happened. You can’t throw them away because next time she can even tell the others there; there you are insulted badly, or you are beaten. So, we just treat them but in most of the cases, teenagers, they are, mostly they are mistreated. …”IDI: Nurse–Kisii
“But sometimes you see the adolescents dealing with them is hard, you want to do a vaginal exam and she doesn’t want to open the thighs, it’s hard, sometime you find that you talk in a harsh way, but later she will comply and you do the vaginal exam. So, maybe sometimes you may try to communicate with the youth and maybe it will come out in a harsh way because you want to do that vaginal exam to help her to know the progress of labor.”IDI: Nurse–Kilifi
“…most of the young women, we know some of them are shy in nature, they not easy to give out information so may be the service provider may feel tired for asking so many questions that the client is not responding so they may be tempted to be harsh to them.”IDI: Nurse–Kilifi
“…Sometimes, it can be age, because this one is young and the other one is older. And another thing its communication, because first you must communicate to me what you want to do for me and then, so once you have communicated back to me, am ready maybe you are going to do vaginal examination, so that one is “sleep there” I think its communication and then age difference…”IDI: Nurse–Kisii
3.5. Summary of Findings
4. Discussion
4.1. Proposed Recommendations
4.2. Proposed Research
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ANC | Antenatal care |
| AKFC | Aga Khan Foundation Canada |
| AKU | Aga Khan University |
| AQCESS | Access to Quality Care through Extending and Strengthening Health Systems |
| DMC | Disrespectful Maternity Care |
| GAC | Global Affairs Canada |
| GoC | Government of Canada |
| HCW | Health Care workers |
| IDIs | In-Depth Interviews |
| LMIC | Low- to Middle-Income Countries |
| MERL | Monitoring and Evaluation and Research Learning |
| MNCH | Maternal new child health |
| NACOSTI | National Commission for Science, Technology, and Innovation |
| PNC | Postnatal care |
| RMC | Respectful Maternity Care |
| SSA | sub-Saharan Africa |
| TBA | Traditional Birth Attendants |
Appendix A
Interviewer Guide on Respectful Maternity Care
- (1)
- What is your understanding of respectful maternity care (RMC)?Prompts:
- (a)
- Respect for beliefs, traditions, and culture
- (b)
- Continuity of care
- (c)
- Right to information and privacy
- (d)
- Good communication between client and provider
- (e)
- Consented care
- (f)
- Confidential care
- (g)
- Nonabandonment in care
- (h)
- No physical abuse
- (i)
- The right to information and privacy
- (j)
- Empowerment of women and her family to become active participants in health care
- (2)
- How did you learn about the information you have given me above? (Prompt: previously as part of college training; on job training, continued medical education (CMEs), or continued professional development (CPD)).
- (a)
- Follow-up: If he/she has attended any of the training, then ask: Could you tell me how long ago you attended the above training? (probe for period of time, not exact year).
- (b)
- Follow-up: What was covered in the training? Or what was the course content?
- (c)
- Follow-up: Who sponsored the training? (Government, Ministry of Health (MOH), Non-Governmental Organization (NGOs), health facilities, etc.).
- (1)
- What support is in place to promote RMC in this facility? (Prompts: guidelines, debriefing sessions, refresher courses, teamwork, etc.)
- (2)
- From your understanding and knowledge about RMC that you have explained (remind them: good communication, etc.), what aspects are embraced/practiced in this facility?
- (3)
- Moving forward, I would like to find out if you have in any way witnessed maternity care that is considered to be disrespectful (Prompts: by colleagues, by themselves, from feedback of clients/patients, the media).
- (4)
- If they have witnessed disrespectful maternity care, then ask the following question: In your view, what do you think is the root cause of this, or what circumstances could lead to this?
- (5)
- Do you think something needs to be done to ensure respectful maternity care? If yes, what?
- (6)
- If he/she mentions cases of disrespectful maternity care, ask: Which service users are likely to experience disrespectful maternity care? Prompts: Young females, old women, poor women, women with children living with disabilities?
- (7)
- In your view, why are the service users you have mentioned above disrespected?
- (1)
- What are your views about disrespectful maternity care with respect to:
- (a)
- women being verbally and physically abused during delivery?
- (b)
- young pregnant women being abused and humiliated when seeking maternity care?
- (c)
- mothers with children living with disabilities being stigmatized when seeking facility care?
- (2)
- What would you say informs your views on these issues? (Prompts: traditional or religious beliefs, cultural norms, medical ethics, personal values, or lack of knowledge.)
- (3)
- Would you say that other service providers have similar views to the ones you provided or different? What might those views be?
Appendix B
Consent Forms
- I have read/information has been read to me, and I have understood the information sheet and have had the opportunity to ask questions about the study.
- I agree to take part in this study and agree for my data to be used for the purpose of this study.
- I understand my participation is voluntary and I may withdraw (at any time) for any reason without my rights being affected.
- I understand that my verbalizations will be audio recorded, and I agree to the audio recording of the interview.
- I understand my responses will be anonymized in reports of the study.
- I understand that I may be quoted directly in reports of the research but that my name will not be used.
Appendix C
Debriefing Forms
References
- Lusambili, A.M.; Naanyu, V.; Wade, T.J.; Mossman, L.; Mantel, M.; Pell, R.; Ngetich, A.; Mulama, K.; Nyaga, L.; Obure, J.; et al. Deliver on Your Own: Disrespectful Maternity Care in rural Kenya. PLoS ONE 2020, 15, e0214836. [Google Scholar] [CrossRef] [Green Version]
- Moindi, R.O.; Ngari, M.M.; Nyambati, V.C.S.; Mbakaya, C. Why mothers still deliver at home: Understanding factors associated with home deliveries and cultural practices in rural coastal Kenya, a cross-section study Global health. BMC Public Health 2016, 16, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebrehiwot, T.; Goicolea, I.; Edin, K.; Sebastian, M.S. Making pragmatic choices: Women’s experiences of delivery care in Northern Ethiopia. BMC Pregnancy Childbirth 2012, 12, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honikman, S.; Fawcus, S.; Meintjes, I. Abuse in South African maternity settings is a disgrace: Potential solutions to the problem. SAMJ 2015, 105, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Kyei-Nimakoh, M.; Carolan-Olah, M.; McCann, T.V. Access barriers to obstetric care at health facilities in sub-Saharan Africa—A systematic review. Syst. Rev. 2017, 6, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, V.B.; Walker, N.; Kanyangarara, M. Estimating the global impact of poor quality of care on maternal and neonatal outcomes in 81 low- and middle-income countries: A modeling study. PLoS Med. 2019, 16, e1002990. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Nurmatov, U.B.; Nwaru, B.I.; Mukherjee, M.; Grant, L.; Pagliari, C. Effectiveness of mHealth interventions for maternal, newborn and child health in low- and middle-income countries: Systematic review and meta-analysis. J. Glob. Health 2016, 6, 010401. [Google Scholar] [CrossRef] [PubMed]
- Chersich, M.; Blaauw, D.; Dumbaugh, M.; Penn-Kekana, L.; Thwala, S.B.P.; Bijlmakers, L.; Vargas, E.; Kern, E.; Kavanagh, J.; Dhana, A.; et al. Mapping of research on maternal health interventions in low- and middle-income countries: A review of 2292 publications between 2000 and 2012. Glob. Health 2016, 12, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. WHO Recommendation on Respectful Maternity Care during Labour and Childbirth. 2018. Available online: https://extranet.who.int/rhl/topics/preconception-pregnancy-childbirth-and-postpartum-care/care-during-childbirth/who-recommendation-respectful-maternity-care-during-labour-and-childbirth (accessed on 26 August 2020).
- WHO. WHO Standards of Care to Improve Maternal and Newborn Quality of Care in Facilities. 2017. Available online: https://www.who.int/maternal_child_adolescent/topics/quality-of-care/quality-of-care-brief-standards.pdf (accessed on 26 August 2020).
- Reis, V.; Deller, B.; Carr, C.; Smith, J. Respectful Maternity Care: Country Experiences; MCHIP/USAID: Washington, DC, USA, 2012. [Google Scholar]
- Odallo, B.; Opondo, E.; Onyango, M. Litigating to ensure access to quality maternal health care for women and girls in Kenya. Reprod. Health Matters 2018, 23, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, C.; Njuki, R.; Abuya, T.; Ndwiga, C.; Maingi, G.; Serwanga, J.; Mbehero, F.; Muteti, L.; Njeru, A.; Karanja, J.; et al. Study protocol for promoting respectful maternity care initiative to assess, measure and design interventions to reduce disrespect and abuse during childbirth in Kenya. BMC Pregnancy Childbirth 2013, 13, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, L.M.; Caldas, J.P. Migration and maternal health: Experiences of Brazilian women in Portugal. Rev. Bras. Saúde Mater. Infant. 2013, 13, 309–316. [Google Scholar] [CrossRef]
- Dempsey, M.; Peeren, S. Keeping things under control: Exploring migrant Eastern European womens’ experiences of pregnancy in Ireland. J. Reprod. Infant Psychol. 2016, 34, 370–382. [Google Scholar] [CrossRef]
- Straus, L.; McEwen, A.; Hussein, F.M. Somali women’s experience of childbirth in the UK: Perspectives from Somali health workers. Midwifery 2009, 25, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Tobin, C.; Murphy-Lawless, J.; Tatano Beck, C. Childbirth in exile: Asylum seeking women’s experience of childbirth in Ireland. Midwifery 2014, 30, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Fair, F.; Raben, L.; Watson, H.; Vivilaki, V.; van den Muijsenbergh, M.; Soltani, H.; ORAMMA Team. Migrant women’s experiences of pregnancy, childbirth and maternity care in European countries: A systematic review. PLoS ONE 2020, 15, e0228378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohren, M.A.; Vogel, J.P.; Tunçalp, Ö.; Fawole, B.; Titiloye, M.A.; Olutayo, A.O.; Ogunlade, M.; Oyeniran, A.A.; Osunsan, O.R.; Metiboba, L.; et al. Mistreatment of women during childbirth in Abuja, Nigeria: A qualitative study on perceptions and experiences of women and healthcare providers. Reprod. Health 2017, 14, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohren, M.A.; Hunter, E.C.; Munthe-Kaas, H.M.; Souza, J.P.; Vogel, J.P.; Gülmezoglu, A.M. Facilitators and barriers to facility-based delivery in low- and middle-income countries: A qualitative evidence synthesis. Reprod. Health 2014, 11, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D-Zomeku, V.M.; Mensah, B.A.B.; Nakua, E.K.; Agbadi, P.; Lori, J.R.; Donkor, P. Exploring midwives’ understanding of respectful maternal care in Kumasi, Ghana: Qualitative inquiry. PLoS ONE 2020, 15, e0238278. [Google Scholar] [CrossRef]
- Kenya National Bureau of Statistics; Ministry of Health/Kenya; National AIDS Control Council/Kenya; Kenya Medical Research Institute; National Council for Population and Development/Kenya; ICF International, Rockville, MD, USA. Kenya Demographic and Health Survey 2014. 2015. Available online: http://dhsprogram.com/pubs/pdf/FR308/FR308.pdf (accessed on 26 August 2020).



{kind=link}
{kind=link}
| Codes | Categories | Themes |
|---|---|---|
| We have fewer maternity equipment. We have dysfunctional equipment. We have fewer beds. We lack basic commodities. We lack private spaces for our doctors. We lack private spaces for our clients. | 1.1 Inadequate infrastructure 1.2 Lack of equipment 1.3 Stock out of commodities | 1. Infrastructural Challenges |
| We are the only two on the night shift. I am alone on the shift. I cannot manage alone—the patients are many. I have many clients during a shift. I get exhausted. It is difficult. | 2.1 Fatigue and Burnout | 2. Understaffing |
| Muslim/Tribal beliefs about female/male nurses. Home deliveries versus facility-based deliveries Cultural beliefs relating to birthing practices. Use of herbs during delivery. | 3.1 Preference for female health care worker due to culture 3.2 Use of herbs during pregnancy 3.3 Differences in cultural beliefs between clients and health care workers 3.4 Client preference | 3. Sociocultural Influences |
| Being a young adolescent mother. Being a mother living with disabilities. Being poor/rich—poor mothers are ignored. | 4.1 Stigma and discrimination based on socioeconomic characteristics of mothers | 4. Staff attitudes towards marginalized women |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lusambili, A.; Wisofschi, S.; Shumba, C.; Obure, J.; Mulama, K.; Nyaga, L.; Wade, T.J.; Temmerman, M. Health Care Workers’ Perspectives of the Influences of Disrespectful Maternity Care in Rural Kenya. Int. J. Environ. Res. Public Health 2020, 17, 8218. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218218
Lusambili A, Wisofschi S, Shumba C, Obure J, Mulama K, Nyaga L, Wade TJ, Temmerman M. Health Care Workers’ Perspectives of the Influences of Disrespectful Maternity Care in Rural Kenya. International Journal of Environmental Research and Public Health. 2020; 17(21):8218. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218218
Chicago/Turabian StyleLusambili, Adelaide, Stefania Wisofschi, Constance Shumba, Jerim Obure, Kennedy Mulama, Lucy Nyaga, Terrance J. Wade, and Marleen Temmerman. 2020. "Health Care Workers’ Perspectives of the Influences of Disrespectful Maternity Care in Rural Kenya" International Journal of Environmental Research and Public Health 17, no. 21: 8218. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218218