1. Introduction
Ehlers–Danlos Syndromes (EDS) are characterized as rare diseases. In the European Union, a disease is categorized as “rare” if less than one in 2000 people is affected [
1]. Approximately 29 million people in the European Union are suffering from at least one of 5000–8000 different rare diseases. In Germany alone, there are probably more than four million people suffering from these diseases [
2]. The EDS describe hereditary connective tissue diseases, which were originally subdivided into 11 subtypes according to the Berlin Nosology from 1988 [
3]. With growing information about the origin of EDS, the nosology was revised in 1997 and the six-type distinctive Villefranche nosology was established [
4]. Today, the syndromes can be classified into 13 subtypes according to the International Classification of Ehlers–Danlos Syndromes established in 2017 [
5].
Almost 90% of persons suffering from EDS are affected by the classical EDS type and the hypermobile EDS type. The vascular type of EDS affects up to 10% of the patients. The periodontal type, which is particularly relevant in dentistry, occurs rather rarely [
3,
4,
6,
7]. The characteristic manifestations of the Ehlers–Danlos Syndromes are hypermobility of the joints, increased ductility of the skin, and weakness of the connective tissue. These symptoms can be attributed to flawed collagen synthesis or mutations [
8]. The most frequently affected types are particularly type I, type III, and type V collagens (COL1A1, COL3A1, COL5A1). The affected genes encode for the fibrillary collagens and, through mutations, lead to common symptoms such as hypermobility of the joints, fragile skin, or even vascular damage [
8]. The periodontal types lead to missense mutations in the C1R and C1S gene sections of Complement Factor 1 [
9].
Since collagens are found in every connective tissue of the body, manifestations of EDS can also be seen in the teeth, mouth, and jaw areas. These oral and mandibular manifestations include thin and fragile mucosa, poor wound healing with increased tendency to bleeding, increased tooth mobility, and tooth and root form anomalies. Moreover, cranio-mandibular dysfunctions (CMD) occur more often [
10]. The periodontal type is characterized by an early onset of severe periodontitis, which is accompanied by lack of attached gingiva and serious hematomas with bruises [
5,
11,
12].
A study by Berglund et al. [
13] identified four conditions “living with fear, living with pain, feeling stigmatized, and experiences of non-affirmation in healthcare”, which all lead to a reduced oral health-related quality of life (OHRQoL). The study shows just how many different aspects restrict the lives of patients with EDS in various ways, thus hindering a “normal life”. Bohner et al. [
14] observed that patients affected by rare diseases and who report oral symptoms have an Oral Health Impact Profile (OHIP) score 6.45 points higher than patients without oral symptoms. Similarly, each year of delayed diagnosis has a negative impact on OHRQoL. The oral manifestations are, therefore, associated with a reduced oral health-related quality of life (OHRQoL) in patients with EDS.
Practitioners often lack knowledge about rare diseases, making it difficult for them to adequately treat patients suffering from a rare disease. This is why those patients are often dissatisfied with the healthcare system here in Germany [
15]. Further studies are needed to examine how much practitioners know about rare diseases and what the German healthcare system must do to better the situation for those affected.
So far, however, it has only been demonstrated that patients with EDS are subjectively affected by a worse OHRQoL compared to the general populace. Because of the oral manifestations of EDS, the patients can also experience symptoms of impaired oral health. As a primary question of this study, we hypothesized that there is a significant correlation between objectively measured and subjectively reported oral health, i.e., H0: |r| = 0.
4. Discussion
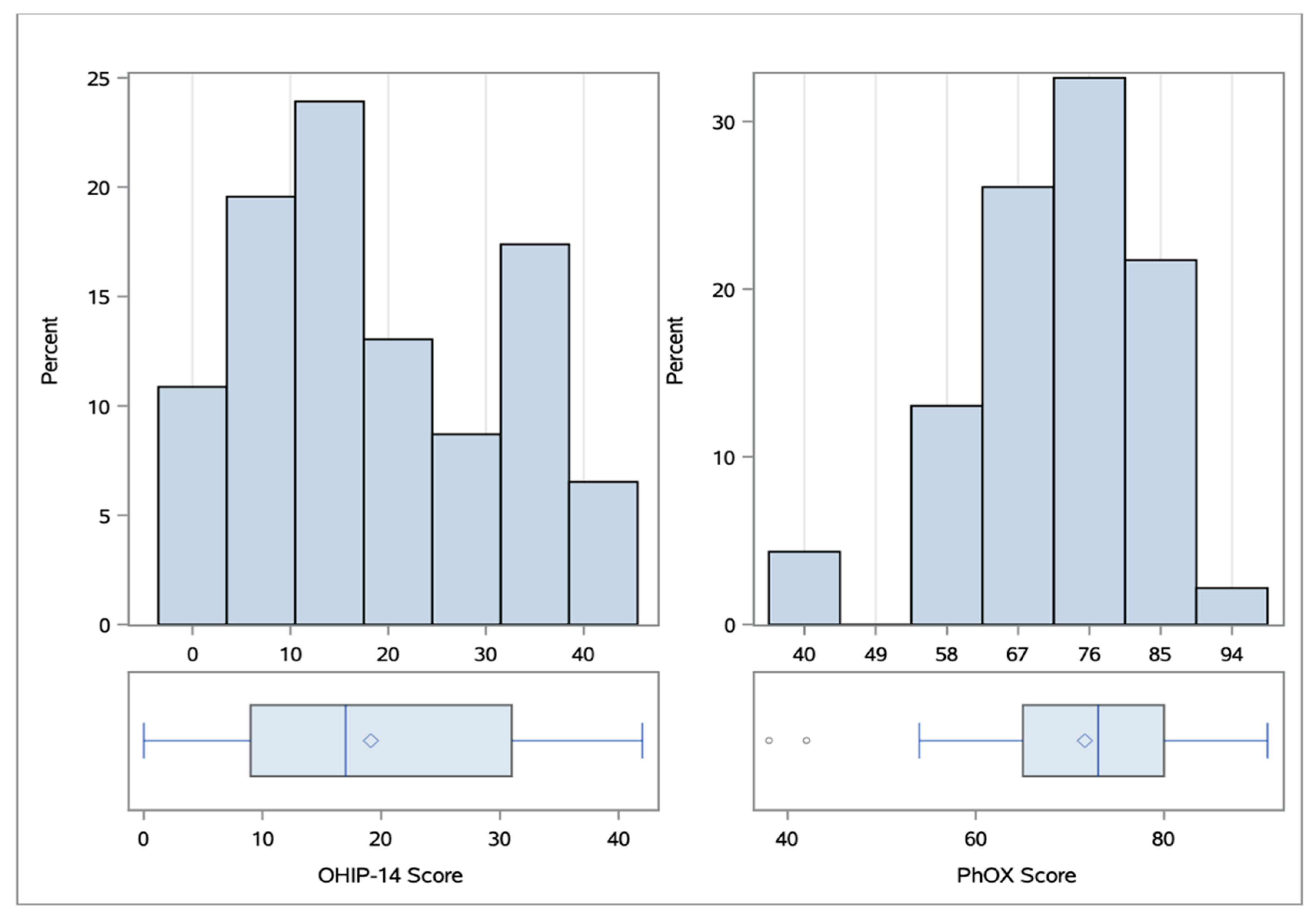
The aim of this study was to find out if this subjective perception of the OHRQoL correlates with objectively measured oral health. The evaluated OHIP 14 scores of this study (median 17, IQR 23, range 0–42) are comparable with the findings of similar studies on OHRQoL for patients with Ehlers–Danlos Syndromes (Hanisch et al. 2018 [
15]; Berglund et al. 2012 [
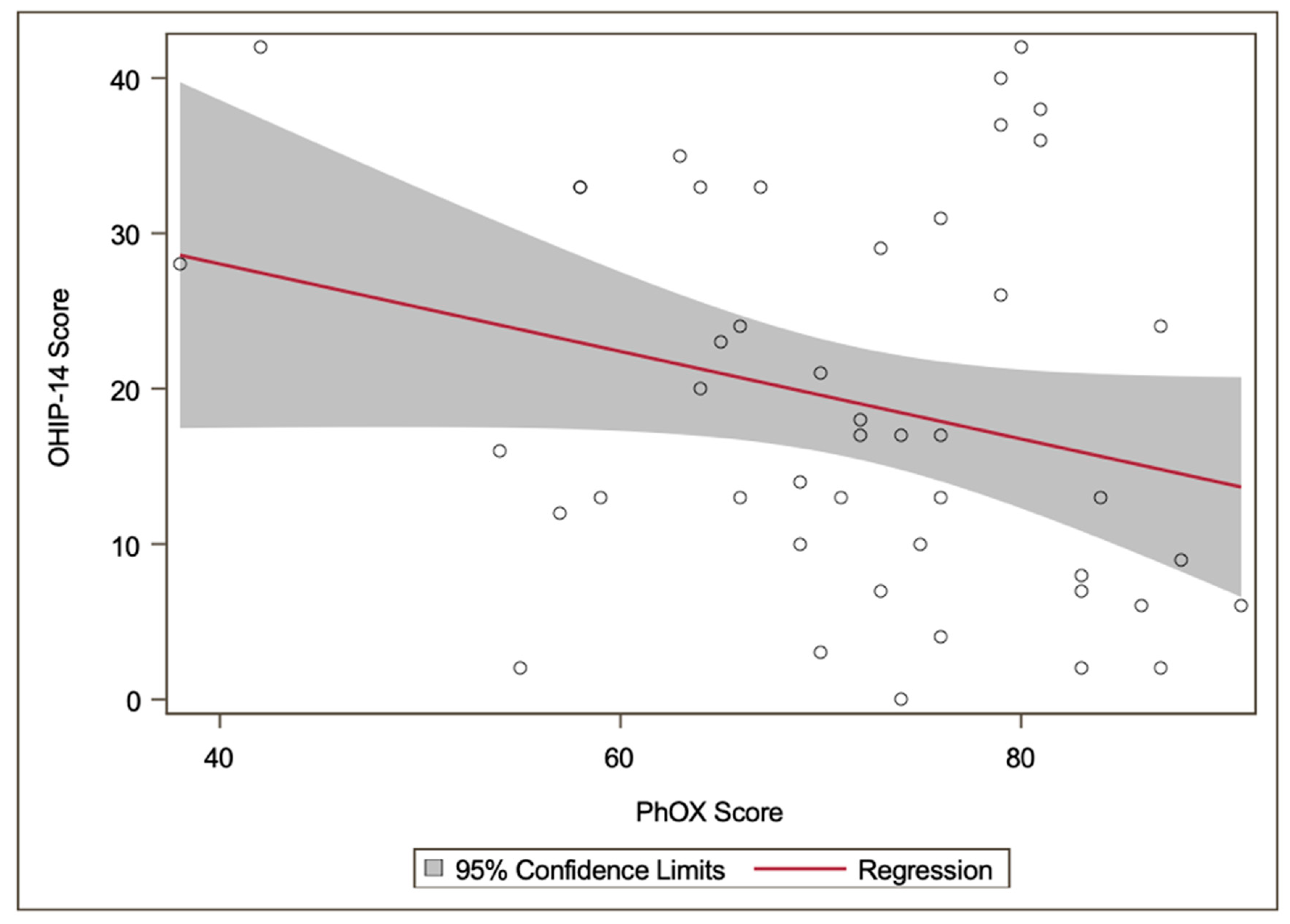
19]). A study by Reissmann et al. [
18] yielded a correlation (
r = 0.41) between the OHIP-14 and PhOX by analyzing 609 dental patients, because of which we hypothesized that there is a significant correlation between the OHRQoL and the objectively measured oral health in our cohort.
However, patients with EDS sometimes report problems and restrictions even with good oral health, even if these problems cannot be objectively understood from a dental perspective. The results showed that the objectively measured oral health of participants with EDS often appears good, even if the participants suffer from a low OHRQoL.
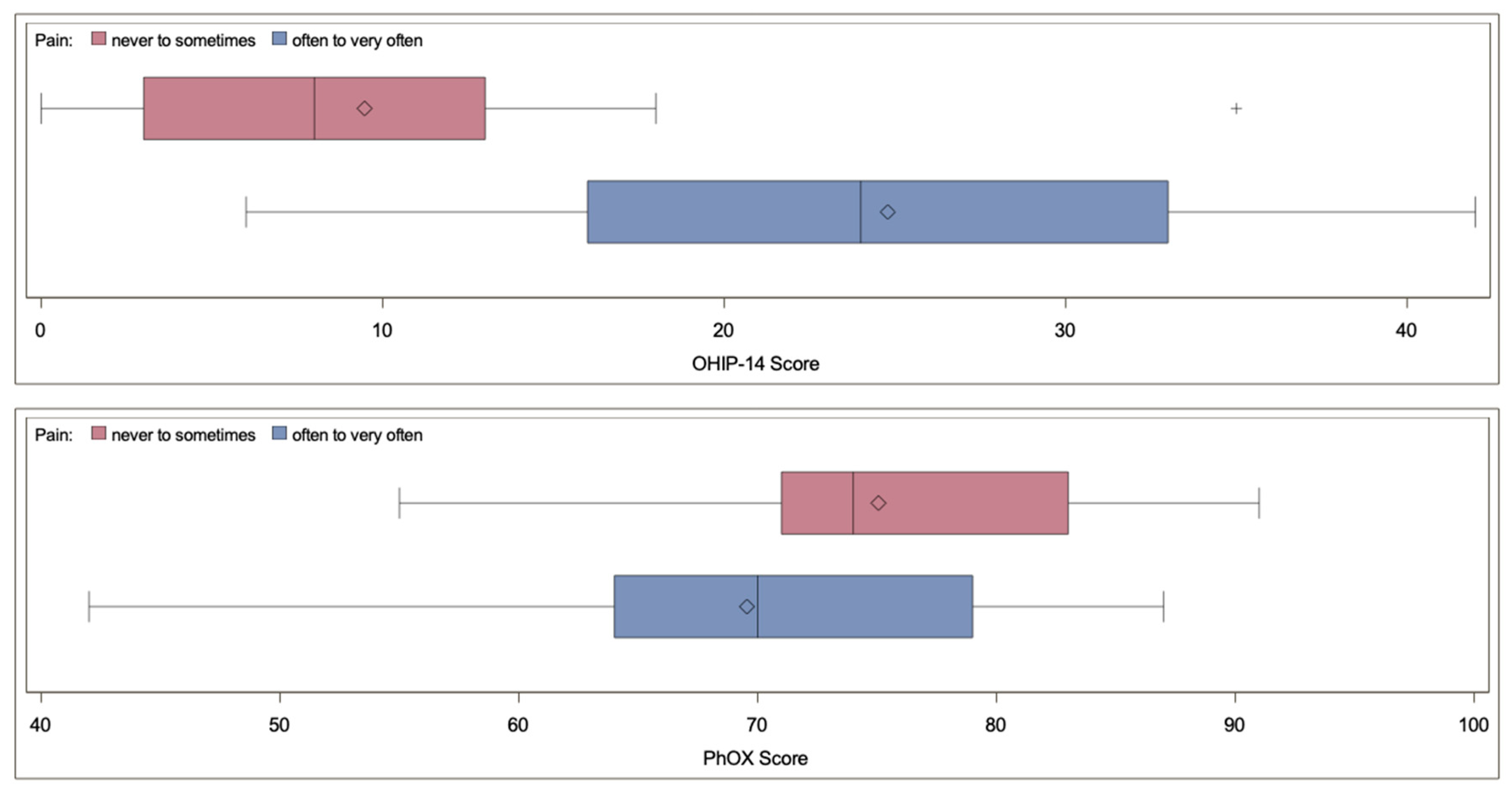
In our cohort, pain was a significant factor worsening the OHRQoL, as seen in
Table 4. Since more than 50% of the participants had pain often to very often, this item had the single biggest negative impact on the OHIP-14 score. This is comparable to similar findings in the Berglund study, in which pain was also a significant factor with a negative influence on the OHRQoL.
We observed that the OHIP-14 score for participants who often or very often experienced pain in the mouth area had higher scores compared to participants who never or only rarely felt pain (p < 0.01), without showing a difference in the PhOX score (p > 0.05). This discrepancy may possibly complicate the care of patients with EDS in daily clinical practice and increase the level of distress for those patients, as the causes of pain cannot be identified from a dental perspective.
The problem that pain cannot necessarily be clinically verified was described previously by patients with EDS. In 1977, Sancheti et al. demonstrated that chronic pain is a manifestation of Ehlers–Danlos Syndromes [
20]. In future studies, the possible association between chronic pain and reduced OHRQoL should be addressed.
In addition to chronically manifested pain, patients with EDS often suffer from craniomandibular dysfunction [
10]. In our cohort, only 11 participants (23.9%) did not feel any pain on palpation of the salivary glands, chewing muscles, or mandibular joint. Pain on palpation, especially of the chewing muscles and mandibular joints, is a common symptom in the diagnosis of CMD [
21]. Previous studies have shown that patients with EDS have a significant higher prevalence of CMD symptoms compared to a control group [
22]. In addition to affecting the temporomandibular joint, patients with EDS often show an increased mouth opening (for 69.5% of our cohort the maximal incisal edge was above 40mm), having a higher risk of sudden meniscal and/or condylar jaw dislocation, which can lead to inflammation of the affected regions [
23].
To help those patients who suffer from CMD and to increase their OHRQoL, CMD-specific physiotherapy is recommended to counteract damage to the temporomandibular joint (TMJ) [
23]. This therapy can involve both changes in body posture and changes in everyday life, such as chewing habits or stress management techniques. Mitakides et al. even recommended this therapy preventively for all patients with EDS [
23]. They also pointed out that the treatment of EDS patients can be quite challenging even for therapists experienced in handling CMD and recommended treatment by specialists who are well versed with EDS symptoms [
10].
Another well-known problem in patients with rare diseases is the long period between the first appearance of symptoms and the diagnosis. On average, it takes 7 years until patients with rare diseases are finally diagnosed. This long time period is accompanied by a lot of stress and uncertainty for the affected patients [
24]. With a median of 20 years, the period in this study was considerably higher, negatively impacting the patients and their OHRQoL even more. Due to the long diagnosis period, the pain with which patients have to live is further increased and can manifest itself chronically [
25].
On one hand, this presents the therapist with a complex task of providing adequate care for the patients. On the other hand, patients with EDS can quickly become dissatisfied. The study by Hanisch et al. (2018) showed that the patients were more satisfied with the therapist, but rather perceived the support provided by the German health system as insufficient [
15]. One aim should be to train the therapists in such a way that they can identify an EDS patient as such and treat them adequately or to point out specific points of contact.
Practitioners are faced with the difficult task of treating patients adequately, even if the patient is not showing corresponding clinical symptoms. The aim should be to assess the OHRQoL of each patient independent of the objectively measured oral health and treat the patient accordingly. To achieve this and to better the OHRQoL in patients with EDS in general, the awareness of rare diseases such as EDS must increase, shortening the time period of diagnosis and relieving patients of their restricted lives.
Limitations
Both the OHIP-14 and the PhOX are validated scores which have previously been used in studies. The participation in the study revealed an enormous imbalance between the sexes. Out of the 46 participants, only four were male. This could be explained by the fact that women are more often involved in support groups as observed in a similar study by Hanisch et al. [
26]. However, a previous study showed that there was no connection with sex for measuring OHRQoL in patients with rare diseases [
14]. Therefore, it is unlikely that the imbalance between sexes has an impact on the outcome of the study. Further studies with higher numbers of participants would be desirable, but high numbers of participants are often difficult to realize, especially in people with rare diseases.

 ,
, 



{kind=link}
{kind=link}
{kind=link}