The Influence of Physical Activity, Anxiety, Resilience and Engagement on the Optimism of Older Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Instrument
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gi Gill, D.; Williams, L.; Reifsteck, E. Psychological Dynamics of Sport and Exercise, 4th ed.; Human Kinetics: Champaing, IL, USA, 2017. [Google Scholar]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J.Behav. Nutr. Phys. Activ. 2013, 10, 10–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barriopedro, M.I.; Eraña, I.; Mallol, L.L. Relación de la actividad física con la depresión y satisfacción con la vida en la tercera edad. Rev. Psicol. Dep. 2001, 10, 239–246. [Google Scholar]
- Crocker, P.; Eklund, R.; Kowalski, K. Children’s physical activity and physical self-perceptions. J. Sports Sci. 2000, 18, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Hellín, P.; Moreno, J.A.; Rodríguez, P.L. Relación de la competencia motriz percibida con la práctica físico-deportiva. Scand. J. Med. Sci. Sports 2006, 15, 219–231. [Google Scholar]
- Lindwall, L.M.; Hassmen, P. The role of exercise and gender for physical self-perceptions and importance ratings in swedish university students. Scand. J. Med. Sci. Sports 2004, 14, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Ommundsen, Y. Implicity theories of ability and self-regulation strategies in physical education classes. Educ. Psychol. 2003, 23, 141–157. [Google Scholar] [CrossRef]
- Panter, J.; Jones, A.; Van Sluijs, E.; Griffin, S. Attitudes, social support and environmental perceptions as predictors of active commuting behaviour in school children. J. Epidemiol. Commu. Health 2010, 64, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Westerberg-Jacobson, J.; Edlund, B.; Ghaderi, A. A 5-year longitudinal study of the relationship between the wish to be thinner, lifestyle behaviour and disturbed eating in 9–20 year old girls. Eur. Eat. Disord. Rev. 2010, 18, 207–219. [Google Scholar] [CrossRef]
- Arraga-Barrios, M.; Sánchez-Villaroel, M. Recreación y calidad de vida en adultos mayores que viven en instituciones geriátricas y en sus hogares. Un estudio comparativo. Espac. Abierto. Cuad. Venezol. Soc. 2007, 16, 737–756. [Google Scholar]
- Armadans, I.; Pérez, A.; Franco, N. Actividad deportiva recreativa y tercera edad: Algunos criterios de gestión para potenciar su demanda. Rev. Multidiscipl. Gerontol. 1998, 8, 341–360. [Google Scholar]
- Rejeski, W.; Brawley, L.; Shumaker, S. Physical activity and sedentary behaviour: A population-bases study of barriers, enjoyment and preference. Health Psychol. 1996, 22, 178–188. [Google Scholar]
- Méndez, A.; Fernández, J. Prescripción de la actividad física en personas mayores: Recomendaciones actuales. Revista Española de Educación Física y Deportes 2005, 3, 19–29. [Google Scholar]
- Mora, J.; González, J.L.; Mora, M. Efectos de un programa de ejercicios sobre el gasto cardiaco en una población de mujeres adultas sedentarias. Revista Española de Educación Física y Deportes 2005, 3, 31–50. [Google Scholar]
- Weisser, B.; Preuss, M.; Predel, H.G. Physical activity for prevention and therapy of internal diseases in the elderly. Med. Klin. (Munich, Germany: 1983) 2009, 104, 296–302. [Google Scholar]
- Zurita, F. Influencia de Los Factores Psicológicos Sobre las Lesiones Deportivas en Deportes de Equipo. Ph.D. Thesis, Universidad de Jaén, Jaén, España, 2015. [Google Scholar]
- Graham, G.; Holt/Hale, S.A.; Parker, M. Children Moving; Mayfield Publishing Company: Mountain View, CA, USA, 1998; pp. 4–7. [Google Scholar]
- Nieman, D.C.; Pedersen, B.K. Exercise and immune function: Recent developments. Phys. Exerc. Med. 1999, 27, 73–80. [Google Scholar] [CrossRef]
- Muñoz, J. Psicología del Envejecimiento; Pirámide: Madrid, Spain, 2002. [Google Scholar]
- Elavsky, S.; McAuley, E.; Motl, R.; Konopack, J.; Márquez, D.; Hu, L.; Jerome, G.; Diener, E. Physical activity enhances long-term quality of life in older adults. Efficacy, esteem and affective influences. Ann. Behav. Med. 2005, 30, 138–145. [Google Scholar] [CrossRef]
- Catell, R.B.; Scheier, I.H. The nature of anxiety: Areview of thrite en multivariate analysis comprissing 814 variable. Psychol. Rep. 1958, 4, 351–388. [Google Scholar] [CrossRef]
- Spielberger, C.D. Anxiety and Behavior; Academic Press: New York, NY, USA, 1996. [Google Scholar]
- Tyrer, P.J. Estados de Ansiedad in Paykel, E.: Psicopatologia de los Transtornos Afectivos; Pirámide: Madrid, Spain, 1985. [Google Scholar]
- Piqueras, R.J.; Martínez, G.A.; Ramos, L.V.; Rivero, B.R.; García, L.L.; Oblitas, G.L. Ansiedad, depresión y salud. Suma Psicol. 2008, 15, 43–73. [Google Scholar]
- Stöber, J.; Pekrun, R. Advances in test anxiety research. Anxiety Stress Coping 2004, 17, 205–211. [Google Scholar]
- Korc, E.M. Vivienda Saludable: Enlace entre la Investigación y las Políticas Públicas. Organización Panamericana de la Salud; OPS-OMS –PWR: Caracas, Venezuela, 2005. [Google Scholar]
- Ownby, R.; Harwodd, D.; Arker, W.; Duara, R. Predictors of anxiety in patiens with Alzheimer’s disease. Depress. Anxiety 2000, 11, 38–42. [Google Scholar] [CrossRef]
- Snyder, A.; Stanley, M.; Novy, D.; Averill, P.; Beck, J. Measures of depression in older adults with generalized anxiety disorder: A psychometric evaluation. Depress. Anxiety 2000, 11, 114–120. [Google Scholar] [CrossRef]
- Lasher, P.K.; Faulkender, P.J. Measurement of aging anxiety: Development of the Anxiety about Aging Scale. Int. Aging Hum. Dev. 1993, 37, 247–259. [Google Scholar] [CrossRef]
- Schiera, A. Uso y abuso del concepto de resiliencia. Revista de Investigación en Psicología 2005, 8, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The ConnorDavidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience theory and research on children and families: Past, present, and promise. J. Family Theory Rev. 2018, 10, 12–31. [Google Scholar] [CrossRef] [Green Version]
- Rutter, M. cResilience, competence, and coping. Child Abuse Neglect 2007, 31, 205–209. [Google Scholar] [CrossRef]
- Becoña, E. Resiliencia: Definición, características y utilidad del concepto. Revista de Psicopatología y Psicología Clínica 2006, 11, 125–146. [Google Scholar]
- Arrogante, O. Mediación de la resiliencia entre burnout y salud en el personal de Enfermería. Enfermería Clínica 2014, 24, 283–289. [Google Scholar] [CrossRef]
- Hu, T.; Zhang, D.; Wang, J. A meta-analysis of the trait resilience and mental health. Pers. Individ. Differ. 2015, 76, 18–27. [Google Scholar] [CrossRef]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. A Correlational Study on dispositional resilience, psychological well-being, and coping strategies in university students. Am. J. Educ. Res. 2014, 2, 463–471. [Google Scholar] [CrossRef]
- Hosseini, S.A.; Besharat, M.A. Relation of resilience whit sport achievement and mental health in a sample of athletes. Procdeia Soc. Behav. Sci. 2010, 5, 633–638. [Google Scholar] [CrossRef] [Green Version]
- García-Gómez, L.; Aldana, G. Voces infantiles en torno a la resiliencia: Las experiencias vitales de niños habitantes de una casa hogar en Ecatepec, estado de México. Uaricha. Revista de Psicología 2011, 8, 92–105. [Google Scholar]
- Lavretsky, H. Resilience, stress and mood disorders in old age. Ann. Rev. Gerontol. Greiatr. 2012, 32, 49–72. [Google Scholar]
- Rowe, J.W.; Kahn, R.L. Successful aging and disease prevention. Adv. Renal Replac. Therap. 2000, 7, 70–77. [Google Scholar] [CrossRef]
- Wagnild, G. Resilience and successful aging: Comparison among low and high income older adults. J. Gerontol. Nurs. 2003, 29, 42–49. [Google Scholar] [CrossRef]
- Meyers, E.E.; Presciutti, A.; Shaffer, K.M.; Gates, M.; Lin, A.; Rosand, J.; Vranceanu, A.-M. The Impact of Resilience Factors and Anxiety During Hospital Admission on Longitudinal Anxiety Among Dyads of Neurocritical Care Patients Without Major Cognitive Impairment and Their Family Caregivers. Neurocrit. Care 2020. [Google Scholar] [CrossRef]
- Zurita, F.; Espejo, T.; Cofré, C.; Martínez, A.; Castro, M.; Chacón, R. Influencia de la actividad física sobre la resiliencia en adultos con dolor de hombro. SPORT TK-Revista EuroAmericana de Ciencias del Deporte 2016, 5, 53–58. [Google Scholar] [CrossRef]
- Martínez-Martí, M.L.; Ruch, W. Character strengths predict resilience over and above positive affect, self-efficacy, optimism, social support, self-esteem, and life satisfaction. J. Posit. Psychol. 2017, 12, 110–119. [Google Scholar] [CrossRef]
- Ramírez-Fernández, E.; Ortega-Martínez, A.R.; Calero-García, M.J. El optimismo como mediador entre la resiliencia y estados afectivos en adultos mayores. Estudios de Psicología 2018, 39, 275–285. [Google Scholar] [CrossRef]
- Marín, E.; Ortín, F.J.; Garcés de los Fayos, E.; Tutte, V. Bibliometric analysis of burnout and optimism in sport. Revista Euroamericana de Ciencias del Deporte 2013, 2, 77–87. [Google Scholar]
- Carver, C.S.; Scheier, M. Dispositional optimism. Trends Cognitive Sci. 2014, 18, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Hart, S.L.; Vella, L.; Mohr, D.C. Relationships among depressive symptoms, benefit-finding, optimism, and positive affect in multiple sclerosis patients after psychotherapy for depression. Health Psychol. 2008, 27, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, J.; Wolford, K.; LaLonde, S.; Brunk, L.; Parker Morris, A. Dispositional optimism as a moderator of the relationship between negative life events and suicide ideation and attempts. Cogn. Ther. Res. 2007, 31, 533–546. [Google Scholar] [CrossRef]
- Díaz, A.; Ponsoda, J.M.; Beleña, A. Optimism as a key to improving mental health in family caregivers of people living with Alzheimer’s disease. Aging Ment. Health 2020, 1–9. [Google Scholar] [CrossRef]
- Extremera, N.; Durán, A.; Rey, L. Perceived emotional intelligence and dispositional optimism–pessimism: Analyzing their role in predicting psychological adjustment among adolescents. Pers. Individ. Differ. 2007, 42, 1069–1079. [Google Scholar] [CrossRef]
- He, F.; Cao, R.; Feng, Z.; Guan, H.; Peng, J. The impacts of dispositional optimism and psychological resilience on the subjective well-being of burn patients: A Structural Equation Modelling Analysis. PLoS ONE 2013, 8, e82939. [Google Scholar] [CrossRef]
- Segerstrom, S.C.; Carver, C.S.; Scheier, M.F. Optimism. In The Happy Mind Cognitive Contributions to Well-Being; Robinson, M.D., Eid, M., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 195–212. [Google Scholar] [CrossRef]
- Segovia, F.; Moore, J.L.; Linnville, S.E.; Hoyt, R.E.; Hain, R.E. Optimism predicts resilience in repatriated prisoners of war: A 37-year longitudinal study. J. Trauma. Stress 2012, 25, 330–336. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Salanova, M.; Gonzalez-Roma, V.; Bakker, A.B. The measurement of engagement and burnout and: A confirmative analytic approach. J. Happiness Stud. 2002, 3, 71–92. [Google Scholar] [CrossRef]
- Gutiérrez-Carmona, A.; Mondaca, C.A.; Urzúa, A.; Wlodarczyk, A. Puede el optimismo mediar el efecto negativo de la ansiedad rasgo sobre el bienestar psicológico? Interam. J. Psychol. 2020, 54, e916. [Google Scholar] [CrossRef]
- Navarro-Abal, Y.; López-López, M.J.; Climent-Rodríguez, J.A. Engagement (compromiso), resiliencia y empatía en auxiliares de enfermería. Enfermería Clínica 2018, 28, 103–110. [Google Scholar] [CrossRef]
- Vizoso, C.M.; Arias-Gundín, O.A. Relación entre resiliencia, optimismo y engagement en futuros educadores. IJERI Int. J. Educ. Res. Innov. 2019, 11, 33–46. [Google Scholar]
- Hernández, R.; Fernández, C.; Baptista, P. Metodología de la Investigación, 2nd ed.; DF McGraw-Hill: Mexico, 1998. [Google Scholar]
- Smith, R.E.; Smoll, F.L.; Cumming, S.P.; Grossbard, J.R. Measurement of multidimensional sport performance anxiety in children and adults: The sport anxiety scale-2. J. Sport Exerc. Psychol. 2006, 28, 479–501. [Google Scholar] [CrossRef]
- Otero, J.M.; Luengo, A.; Romero, F.; Gómez, J.A.; Castro, C. Psicología de la Personalidad. Manual de Prácticas; Ariel Practicum: Barcelona, Spain, 1998. [Google Scholar]
- Schaufeli, W.; Bakker, A. Utrecht Work Engagement Scale; Utrecht University: Utrecht, The Netherlands, 2003. [Google Scholar]
- Notario-Pacheco, B.; Solera, M.; Serrano, M.D.; Bartolomé, R.; García-Campayo, J.; Martínez-Vizcaíno, V. Reliability and validity of the Spanish version of the 10 item Connor -Davidson Resilience Scale (10 item CDRISC) in young adults. Health Qual. Life Outcomes 2011, 9, 63–68. [Google Scholar] [CrossRef] [Green Version]
- De García, A.J.; Marín, M.; Bohórquez, M. Autoestima como variable psicosocial predictora de la actividad física en personas mayores. Revista de Psicología del Deporte 2012, 21, 195–200. [Google Scholar]
- Perdomo, S. Relaciones Entre Resiliencia, Apoyo Social, Estrés, Ansiedad y Depresión Sobre la Calidad de vida de Cuidadores Informales de Personas con Alzheimer. Bachelor’s Thesis, Universidad Santo Tomás, Bogotá, Colombia, 2014. [Google Scholar]
- Suárez, L.A. Optimismo y ansiedad en estudiantes de una Universidad Estatal de Lima. Universidad Nacional Federico Villareal. Bachelor’s Thesis, Universidad Nacional Federico Villareal, Lima, Perú, 2018. [Google Scholar]
- Gil, C.; Fetecua, M.; Espinosa, J.C. Resiliencia y Engagement en Trabajadores de una Unidad de Cuidado Intensivo; Universidad del Rosario: Bogotá, Colombia, 2017. [Google Scholar]
- García-León, M.-A.; González-Gómez, A.; Robles-Ortega, H.; Padilla, J.-L.; Peralta-Ramírez, M.-I. Propiedades psicométricas de la escala de resiliencia de Connor y Davidson (CD-RISC) en población española. Anales de Psicología 2019, 35, 33–40. [Google Scholar]
- Benetti, C.; Kambouropoulos, N. Affect-regulated indirect effects of trait anxiety and trait resilience on self-esteem. Pers. Individ. Differ. 2006, 41, 341–352. [Google Scholar] [CrossRef]
- Beutel, M.E.; Glaesmer, H.; Wiltink, J.; Marian, H.; Brähler, E. Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male 2010, 13, 32–39. [Google Scholar] [CrossRef]
- Azar, D.; Ball, K.; Salmon, J.; Cleland, V. The association between physical activity and depressive symptoms in young women: A review. Ment. Health Phys. Act. 2008, 1, 82–88. [Google Scholar] [CrossRef]
- Maury-Ortiz, J.G.; Martínez-Lugo, M.E.; González-Colón, Z.L. Relación del optimismo, la personalidad resistente y el engagement con el trabajo en una muestra de empleados. Revista Puertorriqueña de Psicología 2015, 25, 280–296. [Google Scholar]
- Olmedilla, A.; Ortega, E. Práctica de la actividad física y ansiedad en mujeres: Variables sociodemográficas como factores moderadores. Revista Argentina de Clínica Psicológica 2012, 21, 25–32. Available online: http://www.redalyc.org/articulo.oa?id=281925884003 (accessed on 20 July 2020).
- McAuley, E.; Marquez, D.X.; Jerome, G.J.; Blissmer, B.; Katula, J. Physical activity and physique anxiety in older adults: Fitness, and efficacy influences. Aging Ment. Health 2002, 6, 222–230. [Google Scholar] [CrossRef]
- García-Molina, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M. Beneficios de la actividad física en personas mayores. Revista Internacional de Medicina y Ciencias de la Actividad Física y el Deporte 2010, 10, 556–576. Available online: http://cdeporte.rediris.es/revista/revista40/artbeneficios181.htm (accessed on 18 July 2020).
- Guillén, F.; Angulo, J. Análisis de rasgos de personalidad positiva y bienestar psicológico en personas mayores practicantes de ejercicio vs. no practicantes. Revista Iberoamericana de Psicología del Ejercicio y el Deporte 2016, 11, 113–122. [Google Scholar]
- Andrade, F.; Pizarro, J.P. Beneficio de la actividad física en el adulto mayor. Programa de diplomado en salud pública y salud familiar. Bachelor’s Thesis, Universidad Austral, Valdivia, Chile, 2007. [Google Scholar]
- Pavez, P.; Mena, L.; Vera-Villarroel, P. El rol de la felicidad y el optimismo como factor protector de la ansiedad. Univ. Psychol. 2012, 11, 369–380. [Google Scholar] [CrossRef]
- Vivaldi, F.; Barra, E. Bienestar psicológico, apoyo social percibido y percepción de salud en adultos mayores. Ter. Psicol. 2012, 30, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Jürschik, P.; Botigué, T.; Nuin, C.; Lavedán, A. Estado de ánimo caracterizado por soledad y tristeza: Factores relacionados en personas mayores. Gerokomos 2013, 24, 14–17. [Google Scholar]
- Losada, A.V.; Álvarez, M. Síntomas depresivos en adultos mayores de 65 años. Influencia del vivir solo o acompañado. Neurama Revista Electrónica de Psicogerontología 2014, 1, 48–62. [Google Scholar]
- Cruz, M.R. Papel de la Resiliencia en Personas Mayores Institucionalizadas. Master’s Thesis, Universidad Pontificada de Comillas, Madrid, Spain, 2015. [Google Scholar]
- Caicedo, B.; Berbesi, D. Salud autorreferida: Influencia de la pobreza y la desigualdad del área de residencia. Gac. Sanit. 2015, 29, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Alomoto, M.; Calero, S.; Vaca, M.R. Intervención con actividad físico-recreativa para la ansiedad y la depresión en el adulto mayor. Revista Cubana de Investigaciones Biomédicas 2018, 37, 47–56. [Google Scholar]
- Cárdenas, J.A.; López, D.A.L. Resiliencia en la vejez. Revista de Salud Pública 2011, 13, 528–540. [Google Scholar]
- Vizoso, C.M. Resiliencia, optimismo y estrategias de afrontamiento en estudiantes de Ciencias de la Educación. Psychol. Soc. Educ. 2019, 11, 367–377. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Mean (SD) | Cronbach’s alpha | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anxiety (SAS-2) | |||||||||||||
| 1. Total | 33.71 (10.48) | 0.880 | 1 | ||||||||||
| 2. Somatic (A-S) | 9.88 (4.31) | 0.797 | 0.865 * | 1 | |||||||||
| 3. Concern (A-P) | 13.16 (4.04) | 0.839 | 0.717 * | 0.408 * | 1 | ||||||||
| 4. Deconcentration (A-D) | 10.7 (4.52) | 0.811 | 0.861 * | 0.696 * | 0.388 * | 1 | |||||||
| Optimism (LOT-R) | |||||||||||||
| 5. Total | 14.85 (3.82) | 0.860 | −0.462 * | −0.447 * | −0.179 * | −0.483 * | 1 | ||||||
| 6. Optimism (O) | 8.82 (2.55) | 0.848 | −0.353 * | −0.365 * | −0.154 * | −0.343 * | 0.780 * | 1 | |||||
| 7. Pessimism (P) | 6.17 (2.69) | 0.850 | 0.338 * | 0.300 * | 0.166 * | 0.351 * | −0.783 * | −0.148 * | 1 | ||||
| Engagement (UWES) | |||||||||||||
| 8. Total | 4.27 (1.25) | 0.852 | −0.382 * | −0.404 * | −0.102 * | −0.423 * | 0.409 * | 0.547 * | −0.034 | 1 | |||
| 9. Vigor (E-V) | 4.23 (1.38) | 0.821 | −0.372 * | −0.379 * | −0.117 * | −0.409 * | 0.417 * | 0.530 * | −0.059 | 0.940 * | 1 | ||
| 10. Dedication (E-D) | 4.3 (1.34) | 0.790 | −0.331 * | −0.363 * | −00.074 | −0.367 * | 0.381 * | 0.519 * | −0.015 | 0.944 * | 0.843 * | 1 | |
| 11. Absorption (E-A) | 4.27 (1.29) | 0.806 | −0.369 * | −0.392 * | −00.094 | −0.410 * | 0.346 * | 0.484 * | −0.019 | 0.920 * | 0.785 * | 0.804 * | 1 |
| CD-RISC (Resilience) | 27.49 (8.23) | 0.844 | −0.369 * | −0.365 * | −0.138 * | −0.392 * | 0.542 * | 0.639 * | −0.150 * | 0.633 * | 0.588 * | 0.601 * | 0.588 * |
| Occupancy, Mean (SD) | ANOVA | eta2 | ||||
|---|---|---|---|---|---|---|
| Retired | Unemployed | Working | F (2, 377) | p-Value | ||
| Anxiety (SAS-2) | ||||||
| Total | 34.84 (10.65) a | 31.08 (10.87) b | 31.39 (9.46) b | 4.723 | 0.009 | 0.024 |
| Somatic | 10.15 (4.35) | 8.83 (3.61) | 9.45 (4.31) | 1.68 | 0.188 | 0.009 |
| Concern | 13.29 (4.01) | 12.17 (4.02) | 13.09 (4.13) | 0.864 | 0.422 | 0.005 |
| Deconcentration | 11.43 (4.64) a | 10.32 (4.61) b | 8.83 (3.58) b | 12.116 | < 0.001 | 0.061 |
| Lot | ||||||
| Total | 14.54 (3.78) | 14.48 (3.69) | 15.76 (3.89) b | 3.629 | 0.028 | 0.02 |
| Optimism | 8.78 (2).51) | 8.32 (2.90) | 9.07 (2.57) | 0.986 | 0.374 | 0.005 |
| Pessimism | 6.43 (2.70) | 5.84 (2).03) | 5.52 (2.76) | 4.307 | 0.014 | 0.022 |
| Utrecht Work Engagement Scale (UWES) | ||||||
| Total | 4.21 (1.34) a | 3.89 (1.29) b | 4.53 (0.91) | 3.645 | 0.027 | 0.019 |
| Force | 4.14 (1.48) a | 3.92 (1.38) b | 4.54 (1.02) a | 3.544 | 0.03 | 0.018 |
| Dedication | 4.23 (1.44) | 3.91 (1.32) b | 4.60 (1.01) a | 3.734 | 0.025 | 0.019 |
| Absorption | 4.24 (1.36) | 3.84 (1.28) | 4.47 (1.03) | 2.573 | 0.078 | 0.013 |
| Resilience | 27.29 (8.62) | 25.16 (9.13) | 28.67 (6.70) | 2.066 | 0.128 | 0.011 |
| Age, Mean (SD) | ANOVA | eta2 | |||||
|---|---|---|---|---|---|---|---|
| <55 | 55–64 | 65–75 | >75 | F (2, 377) | p-Value | ||
| Anxiety (SAS-2) | |||||||
| Total | 38.00 (8.56) a | 31.66 (10.26) b | 33.38 (9.90) b | 37.22 (11.51) a | 4.929 | 0.002 | 0.038 |
| Somatic | 10.86 (5.30) a | 9.59 (4.27) b | 9.32 (3.84) b | 11.52 (4.96) a | 5.159 | 0.002 | 0.04 |
| Concern | 16.29 (3.50) | 12.84 (4.34) | 13.15 (3.92) | 13.46 (3.81) | 1.783 | 0.15 | 0.014 |
| Deconcentration | 10.86 (4.88) a | 9.26 (3.94) a | 10.90 (4.38) a | 12.34 (5.09) b | 7.655 | < 0.001 | 0.058 |
| Lot | |||||||
| Total | 13.40 (4.51) | 15.46 (3.37) | 14.86 (3.70) | 13.97 (4.60) | 2.441 | 0.064 | 0.02 |
| Optimism | 7.71 (4.15) a | 9.04 (2.21) b | 9.00 (2.42) b | 8.17 (3.05) b | 2.732 | 0.044 | 0.021 |
| Pessimism | 9.14 (3.98) a | 5.64 (2.44) b | 6.21 (2.74) b | 6.53 (2.60) b | 4.951 | 0.002 | 0.038 |
| UWES | |||||||
| Total | 4.44 (0.73) a | 4.45 (1.00) a | 4.41 (1.24) a | 3.68 (1.44) b | 7.742 | < 0.001 | 0.058 |
| Force | 4.19 (0.81) a | 4.46 (1.08) a | 4.35 (1.39) a | 3.64 (1.60) b | 6.623 | < 0.001 | 0.05 |
| Dedication | 4.38 (0.95) a | 4.51 (1.07) a | 4.43 (1.35) a | 3.71 (1.52) b | 6.743 | < 0.001 | 0.051 |
| Absorption | 4.76 (0.96) a | 4.37 (1.11) a | 4.45 (1.22) a | 3.69 (1.51) b | 7.315 | < 0.001 | 0.055 |
| Resilience | 24.86 (5.76) a | 28.58 (7.06) b | 28.38 (8.21) b | 24.12 (9.23) a | 6.16 | < 0.001 | 0.047 |
| B (ET) | Beta | T | p-Value | |
|---|---|---|---|---|
| Residence (littoral or inland) | −0.30 (0.35) | −039 | −0.862 | 0.389 |
| Center type | ||||
| None | Ref. | |||
| Private | −0.10 (0.60) | −0.008 | −0.174 | 0.862 |
| Public | −0.85 (0.37) | −0.102 | −2.282 | 0.023 |
| Physical activity (Yes vs. No) | 0.47 (0.38) | 0.056 | 1.241 | 0.215 |
| UWES | 0.17 (0.18) | 0.056 | 0.976 | 0.33 |
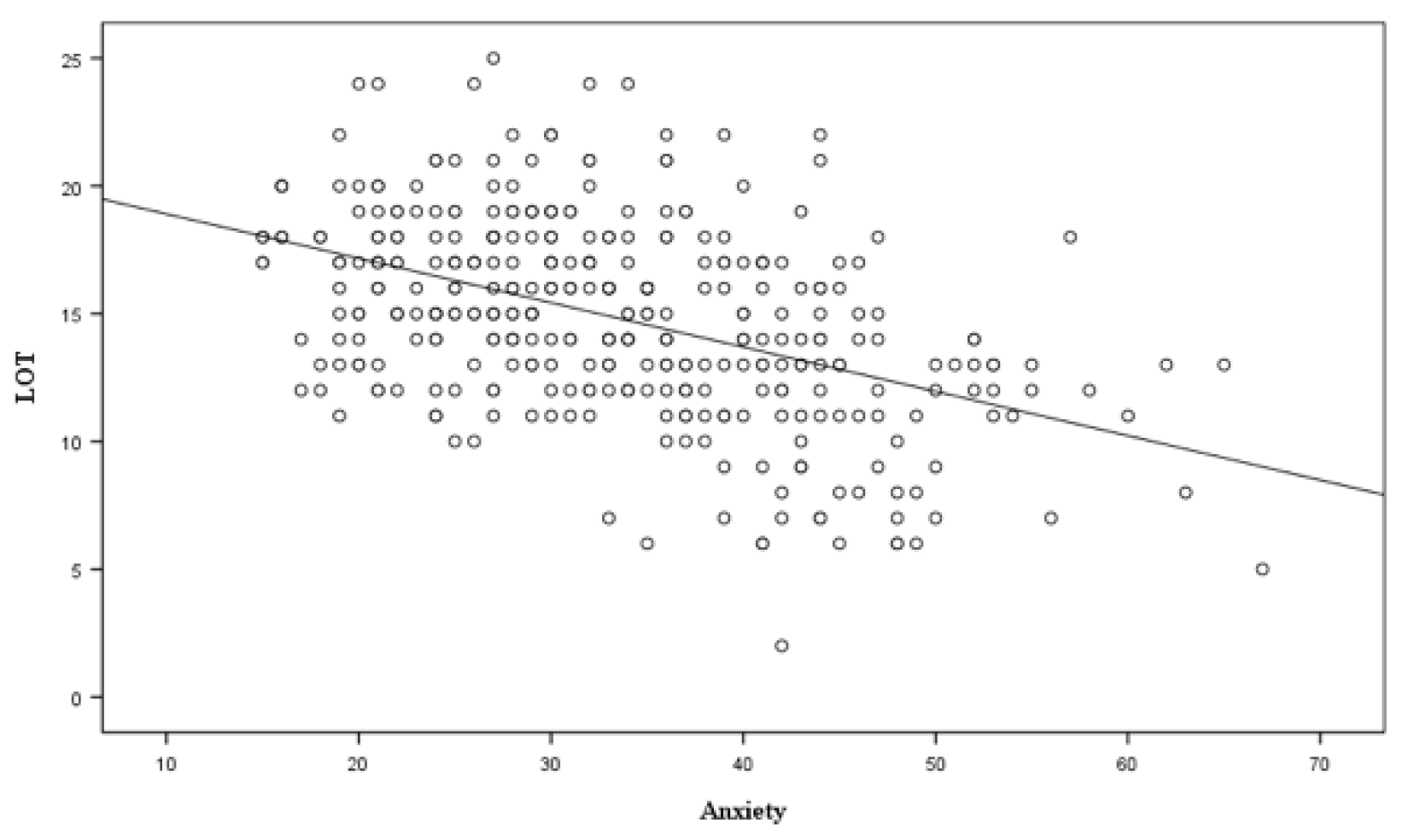
| Anxiety | −0.10 (0.02) | −0.272 | −5.73 | < 0.001 |
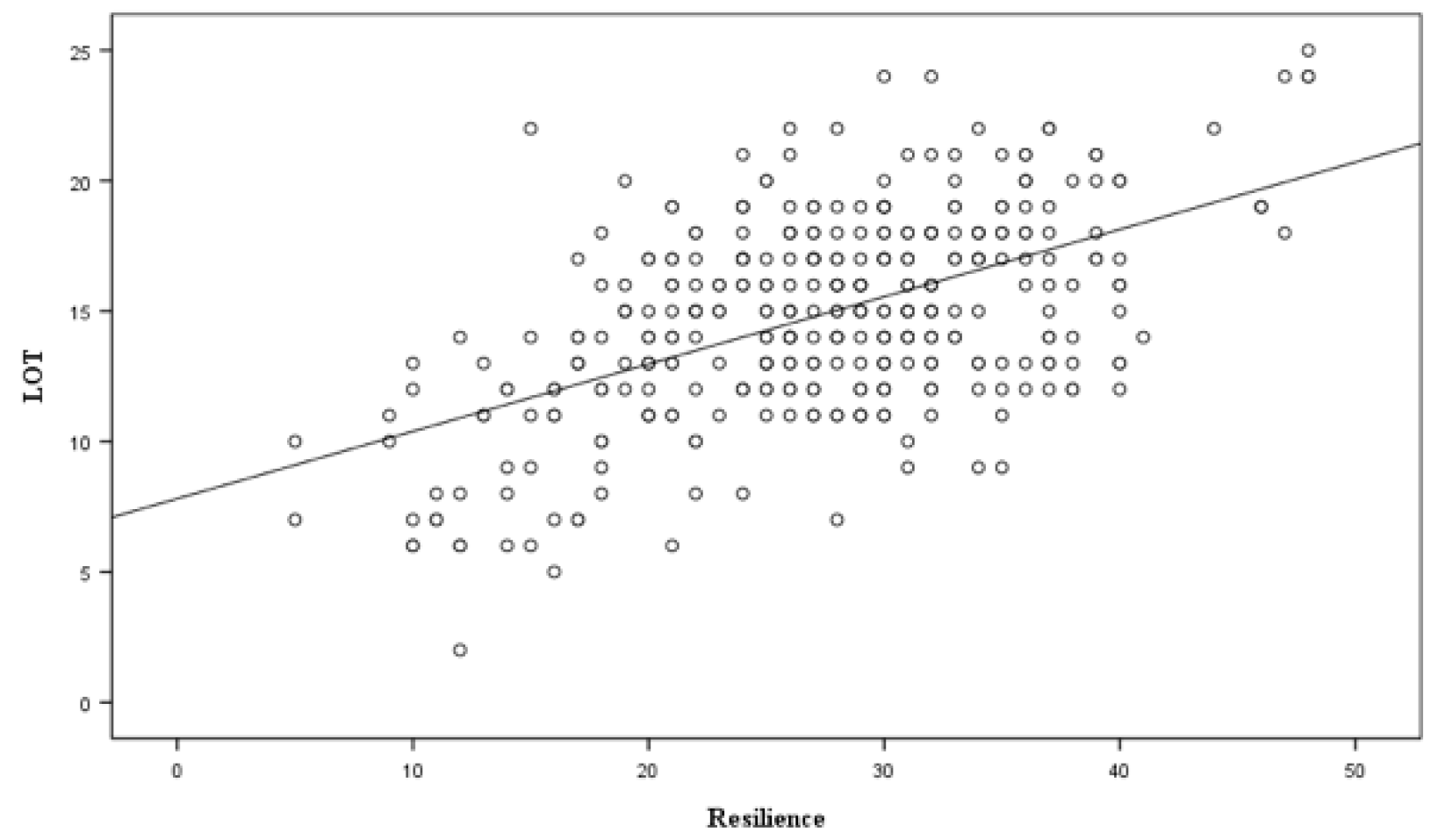
| Resilience | 0.19 (0.03) | 0.398 | 7.211 | < 0.001 |
| Assumptions | ||||
| Normality † | p = 0.200 | |||
| Independence ‡ | 2.031 | |||
| Homoscedasticity + | p = 0.721 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Moreno, A.; Ibáñez-Pérez, R.J.; Cavas-García F, F.; Cano-Noguera, F. The Influence of Physical Activity, Anxiety, Resilience and Engagement on the Optimism of Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 8284. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218284
Martínez-Moreno A, Ibáñez-Pérez RJ, Cavas-García F F, Cano-Noguera F. The Influence of Physical Activity, Anxiety, Resilience and Engagement on the Optimism of Older Adults. International Journal of Environmental Research and Public Health. 2020; 17(21):8284. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218284
Chicago/Turabian StyleMartínez-Moreno, Alfonso, Ricardo José Ibáñez-Pérez, Francisco Cavas-García F, and Francisco Cano-Noguera. 2020. "The Influence of Physical Activity, Anxiety, Resilience and Engagement on the Optimism of Older Adults" International Journal of Environmental Research and Public Health 17, no. 21: 8284. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218284