Acceptability and Barriers to Use of the ASMAN Provider-Facing Electronic Platform for Peripartum Care in Public Facilities in Madhya Pradesh and Rajasthan, India: A Qualitative Study Using the Technology Acceptance Model-3

 , , , ,
, , , , 
Abstract
:1. Introduction
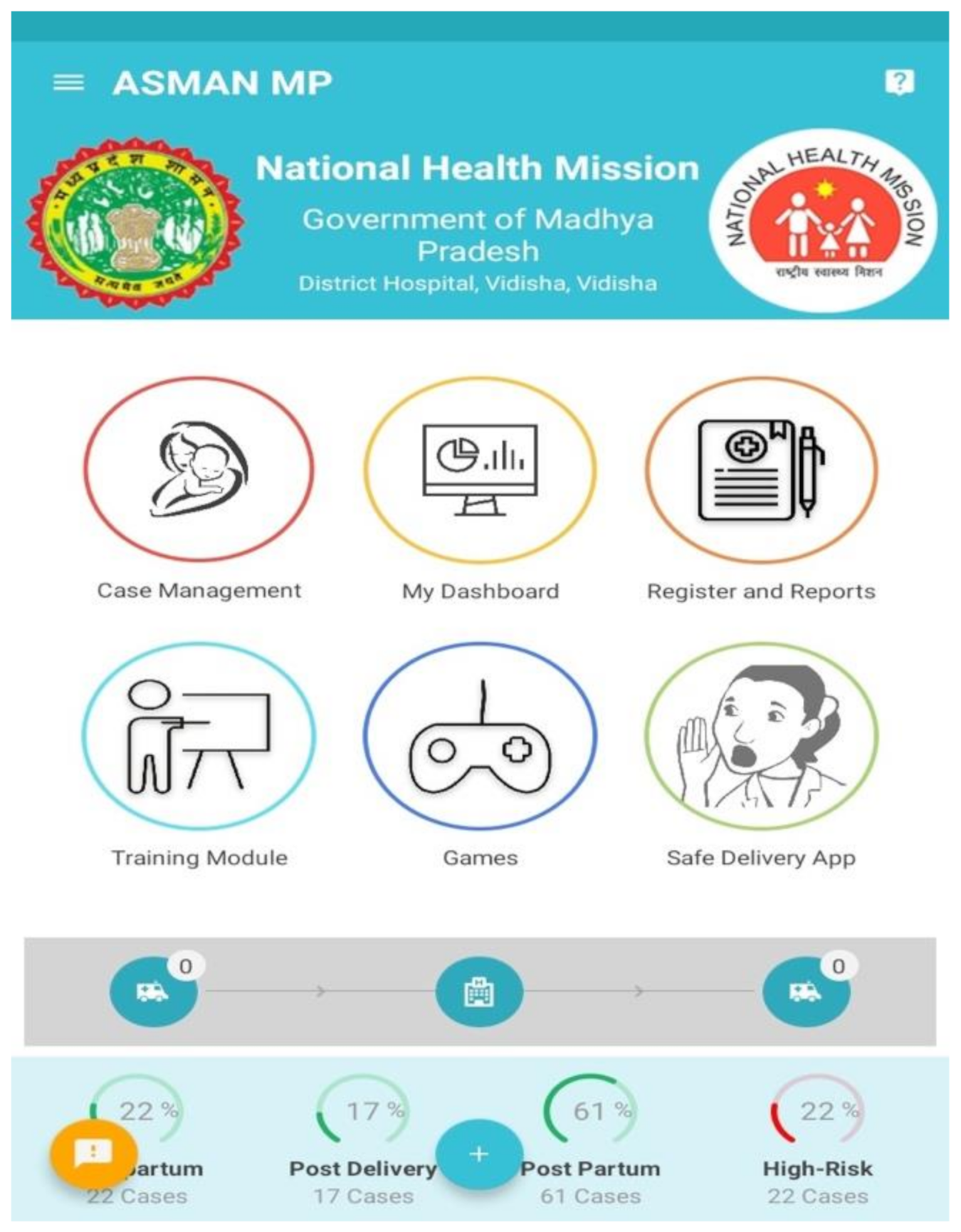
1.1. ASMAN: A Provider-Facing mHealth Package for Peripartum Care in India
- Case management: A digitized case sheet is used from admission until discharge with integrated clinical rules (admission notes, e-partograph, Safe Childbirth Checklist, delivery notes, post-delivery monitoring, post-natal care, discharge slip, referral slip, events section, alerts and notifications).
- Dashboards and reports: System-generated dashboards and reports allow data in ASMAN to be reported to respective health facilities, districts, and state level managers.
- E-learning content: All GoI training modules, guidelines, and tutorials are included in the ASMAN platform and were available in audio, video, or written formats in English or in Hindi.
- ASMAN Complication Management Game: This case-based game is intended to improve management of intrapartum and immediate postpartum/postnatal complications for developing the critical thinking skills of health workers around safe childbirth.
- Safe Delivery App: Developed by the Maternity Foundation, the University of Southern Denmark, and the University of Copenhagen, this feature within the ASMAN platform gives users instant access to up-to-date clinical guidelines on basic emergency obstetrics and neonatal care.
- Remote support center: Staffed 24/7 by obstetricians and senior nurses at the district referral hospital, the support center provides guidance in cases of unclear management. Staff at the remote support system have access to all cases where expert opinion was sought.
1.2. Research Aims
2. Methods
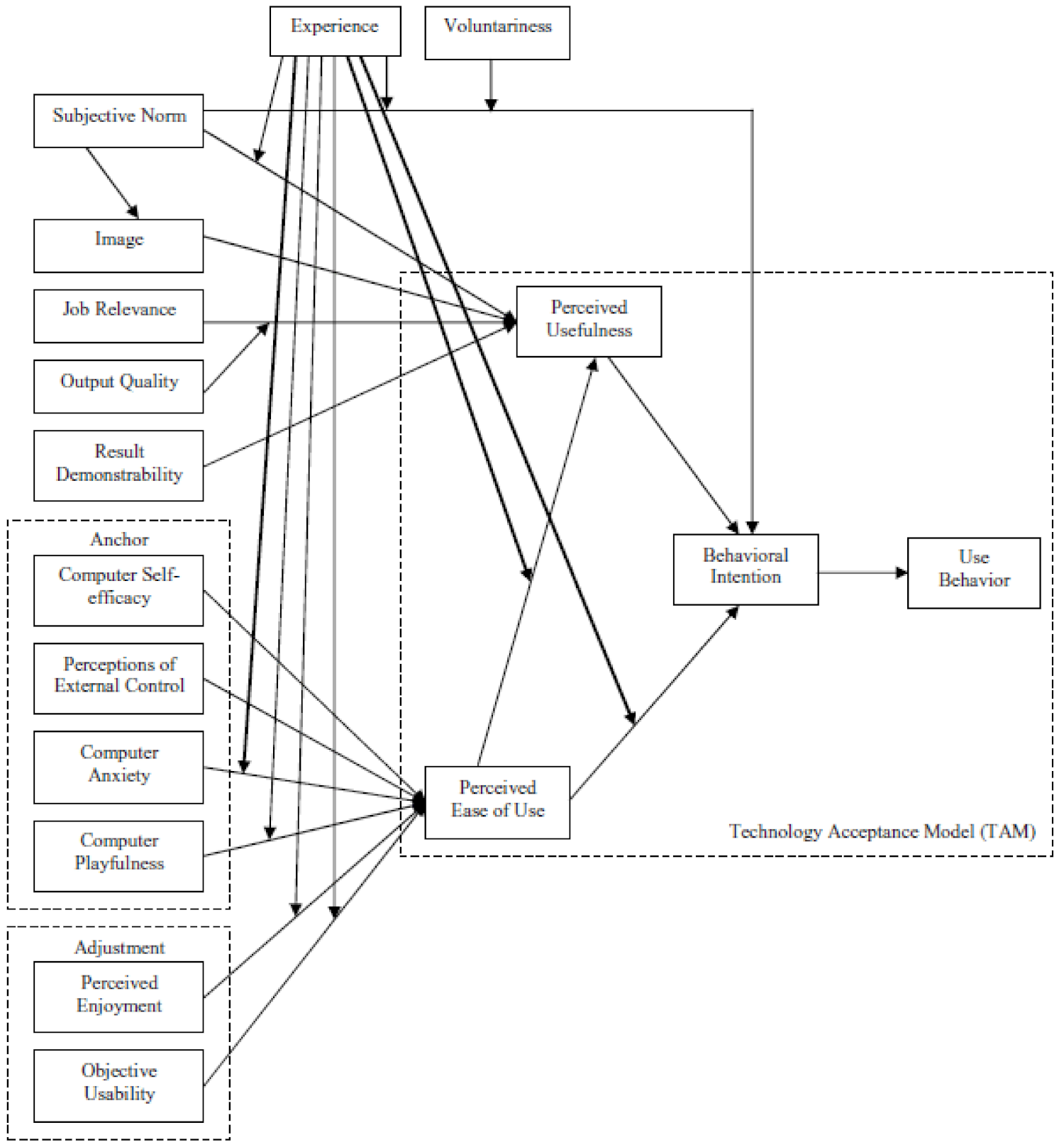
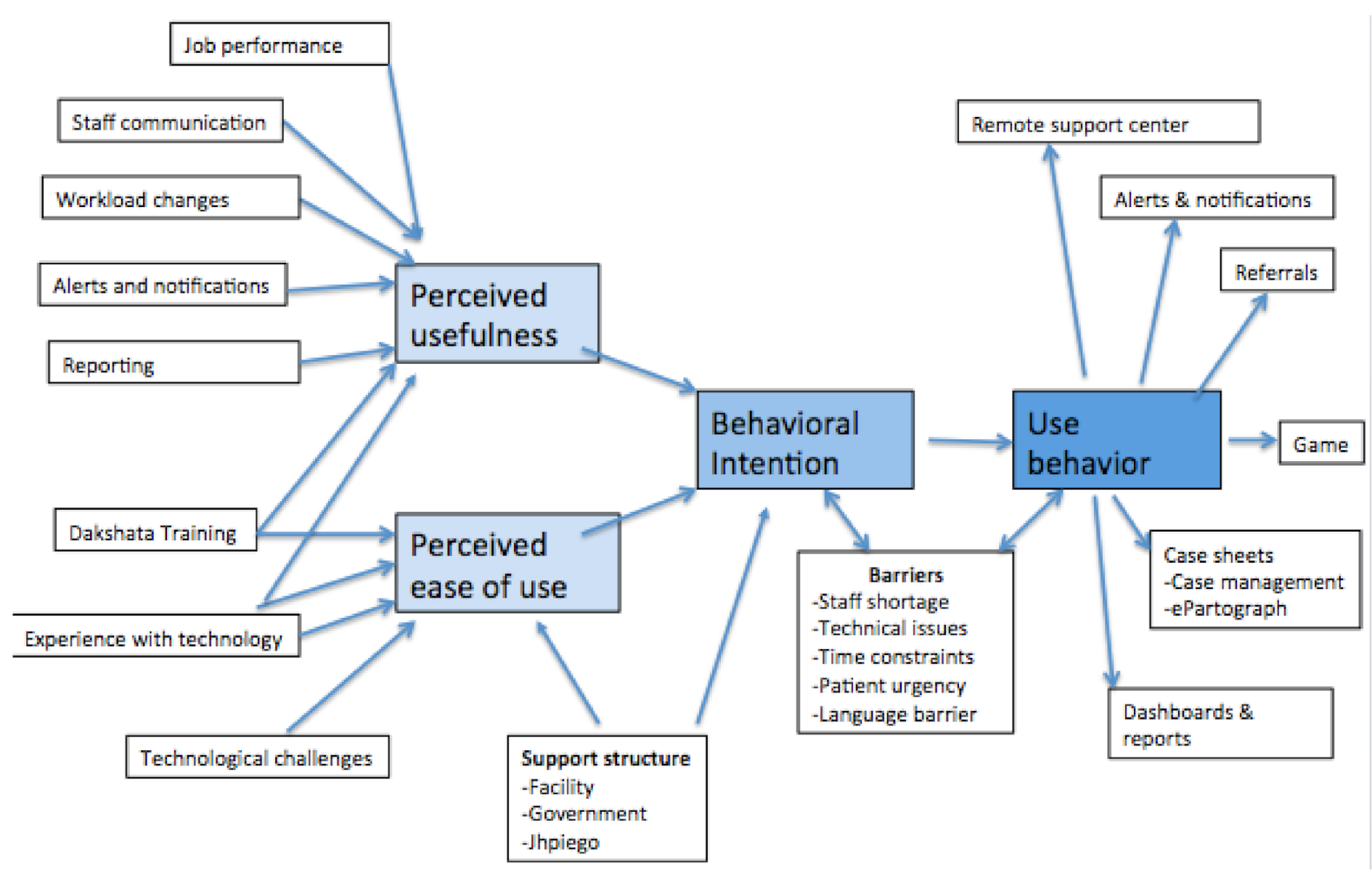
2.1. Conceptualizing Technology Acceptance and Adoption: The TAM-3 Model
2.2. Study Design and Selection of Health Facilities
2.3. Study Respondents
2.4. Data Collection
2.5. Data Management and Confidentiality
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Perceived Ease of Use
3.1.1. Experience with Technology
Initially we were a bit hesitant to use this application but after training, using it seemed very easy, just like using a mobile phone… We can get all required information about a patient with this application.—Labor Room Supervisor, low-utilization CHC
Initially operating this application was a big deal for some staff, like one elderly staff person was there who had never used a smartphone… She does not know how to write properly, but she is an expert at using this application.—Medical Officer, high-utilization subdistrict hospital
3.1.2. Technological Challenges
3.2. Perceived Usefulness
3.2.1. Dakshata Training
[T]hey had explained in detail about dosages to be given, there was detailed discussion on PPH [postpartum hemorrhage]. If I had attended, I would have known all that so training is really beneficial.—Staff Nurse, high-utilization CHC
3.2.2. Workload Changes
Our workload has increased… We are managing detailed information in the application, as well as in the register, which is time-consuming. If all documentation were restricted only to this application, then it would reduce our workload.—Staff Nurse, low-utilization CHC
3.2.3. Job Performance
Earlier we were not filling the details of everything that was happening in reality during the delivery process… we used to forget some things. But in the app, all the points and fields cover the whole process of delivery, from admission to discharge… we are doing it more carefully now.—Staff Nurse, low-utilization CHC
Now we become alert like if there is prolonged labor above 12 h, there is no progress, dilatation is not exceeding more than three fingers, and we also see level of the pains, etc. so we refer the patient.—Labor Room Supervisor, high-utilization CHC
No timely monitoring was done [before ASMAN] because there was no requirement. High-risk cases used to be referred mostly because nobody called the remote support center. Without timely monitoring, then high-risk cases like obstructed labor or prolonged labor will go wrong. Maternal deaths and stillbirths were happening more often back then… ASMAN has made us more disciplined. Now we know the proper way to manage the patient. It has improved staff knowledge.—Labor Room Supervisor, high-utilization CHC
Sometimes, upon getting a high-risk alert, they [medical officers/specialists] tell us directly to refer the patient. Like if they get an alert of low hemoglobin (which is 7 gm), then they call us and tell us the condition of the patient and instruct us to refer the patient to a higher facility.—Labor Room Supervisor, high-utilization CHC
3.2.4. Improved Outcomes
We have reduced referrals, we have managed high-risk cases, and we have also stopped stillbirths by referring on time.—Labor Room Supervisor, high-utilization CHC
We can show our work to the doctors, directors, and everyone. You were not able to show your work to others via paperwork before. Now we can show that we are doing well and get appreciation.—Labor Room Supervisor, high-utilization CHC
3.3. Behavioral Intentions
[Using ASMAN] is our duty and we must do it for the betterment of the patient… But surely everything would be smoother if we had more staff and ample time.—Labor Room Supervisor, low-utilization CHC
- Staff shortages: Well over half of respondents (60%) said staff shortages posed a huge problem for real-time data entry. Often limited to one nurse per shift, respondents said it was impossible to enter data while providing patient care.
We are fully satisfied [with ASMAN] but our main problem is shortage of staff. It is very difficult for a single staff person to handle 8–10 deliveries per night. We do around 500 deliveries here per month.—Staff Nurse, low-utilization district hospital
- 2.
- Patient urgency: Urgent patient needs often delayed data entry, especially amongst staff nurses.
Seventy percent of the delivery cases come in full dilatation; in such cases we only complete admission and the rest of the entries are done later. In such cases, we have to manage the patient first.—Staff Nurse, low-utilization CHC
- 3.
- Time constraints: High caseloads and staff shortages limited the time available to use certain features of the application, notably the game. Data entry was also compromised. Medical officers and labor room supervisors cited time constraints as a barrier more frequently than staff nurses.
Sometimes when I get busy, I forget to enter some data. I do not intentionally omit anything but being only [a nurse at the labor room], I have to handle everything from the outpatient department to attending deliveries, emergency cases, everything.—Labor Room Supervisor, low-utilization CHC
- 4.
- Language barriers: One labor room supervisor noted that some of her staff felt uncomfortable playing the game in ASMAN because there was no Hindi version. Two other respondents also noted the application was in English, a potential barrier for some staff.
3.4. Use Behavior
3.4.1. Case Management
Alerts are very helpful… The patient came with a normotensive BP [blood pressure]… After the delivery, I went home. Suddenly the BP of the patient rose, I got the alert, and I came immediately.—Medical Officer, high-utilization subdistrict hospital
Such a function [alerts] is not in operation here. Our doctor madam has never told us about this alert notification. If this function is there, then it will help us by keeping us alert about any complicating situation.—Labor Room Supervisor, low-utilization CHC
Now, when a referral patient is coming and she is from a referral facility, then we can know in advance that she is coming and we prepare accordingly. I remember… [one patient] had postpartum hemorrhage and we noted in the ASMAN app that she was having postpartum hemorrhage, we then checked her other parameters and those were also in critical condition, so we arranged blood transfusions and everything else in advance and when she came everything was ready. When she reached us, she had a cervical tear, so we transfused blood and repaired the tear. Then the patient stabilized… Earlier, when we were doing everything offline, we would never know that such a patient was coming.—Staff Nurse, low-utilization district hospital
3.4.2. Dashboards and Reports
3.4.3. ASMAN Complication Management Game
In the game, there are different complicated scenarios about high-risk patients, and you have to determine what to do as a first priority… As you complete all the levels, you get ideas from the games about what is first priority, what should be second, and what should be third. It is very useful for case management.—Staff Nurse, high-utilization subdistrict hospital
3.4.4. Remote Support Center
…Once there was a case of severe postpartum hemorrhage, her uterus was not contracting and she was bleeding profusely, we were unable to even refer her to somewhere else, so we called the call center. They explained emergency management and we were able to stop the bleeding. Then we referred her on time.—Staff Nurse, high-utilization CHC
3.5. Differences Between High-Utilization and Low-Utilization Facilities
4. Discussion
4.1. Perceived Ease of Use
4.2. Perceived Usefulness
4.3. Barriers to ASMAN Use Behavior
4.4. Sustainability Considerations
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies: Second Global Survey on eHealth; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Free, C.; Phillips, G.; Watson, L.; Galli, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technologies to Improve Health Care Service Delivery Processes: A Systematic Review and Meta-Analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef] [PubMed]
- Balikuddembe, M.S.; Tumwesigye, N.M.; Wakholi, P.K.; Tylleskär, T. Computerized Childbirth Monitoring Tools for Health Care Providers Managing Labor: A Scoping Review. JMIR Med. Inform. 2017, 5, e14. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, M.W.M.; Smeulers, M.; Vermeulen, H.; Peute, L.W. Effects of clinical decision-support systems on practitioner performance and patient outcomes: A synthesis of high-quality systematic review findings. J. Am. Med. Inform. Assoc. 2011, 18, 327–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labrique, A.B.; Vasudevan, L.; Kochi, E.; Fabricant, R.; Mehl, G. mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Glob. Health Sci. Pract. 2013, 1, 160–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, A.X.; Adhikari, N.K.J.; Mcdonald, H.; Rosas-Arellano, P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, B.R.B. Effects of Computerized Clinical Decision Support Systems on Practitioner Performance and Patient Outcomes A Systematic Review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef]
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. Br. Med. J. 2005, 330, 765–768. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.I.; Aturinda, I.; Mwesigwa, E.; Burns, B.; Santorino, D.; Haberer, J.E.; Bangsberg, D.R.; Holden, R.J.; Ware, N.C.; Siedner, M.J. The Technology Acceptance Model for Resource-Limited Settings (TAM-RLS): A Novel Framework for Mobile Health Interventions Targeted to Low-Literacy End-Users in Resource-Limited Settings. AIDS Behav. 2017, 21, 3129–3140. [Google Scholar] [CrossRef]
- Praveen, D.; Patel, A.; Raghu, A.; Clifford, G.D.; Maulik, P.K.; Mohammad Abdul, A.; Mogulluru, K.; Tarassenko, L.; MacMahon, S.; Peiris, D. SMARTHealth India: Development and Field Evaluation of a Mobile Clinical Decision Support System for Cardiovascular Diseases in Rural India. JMIR mHealth uHealth 2014, 2, e54. [Google Scholar] [CrossRef]
- Anchala, R.; Kaptoge, S.; Pant, H.; Di Angelantonio, E.; Franco, O.H.; Prabhakaran, D. Evaluation of effectiveness and cost-effectiveness of a clinical decision support system in managing hypertension in resource constrained primary health care settings: Results from a cluster randomized trial. J. Am. Heart Assoc. 2015, 4, e001213. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, M.; Rotheram-Borus, M.; Swartz, L.; Tsai, A. Scaling up mHealth: Where is the evidence? PLoS Med. 2013, 10, e1001382. [Google Scholar] [CrossRef] [Green Version]
- Blaya, J.A.; Fraser, H.S.F.; Holt, B. E-health technologies show promise in developing countries. Health Aff. 2010, 29, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, M.P.; Ngangue, P.; Payne-Gagnon, J.; Desmartis, M. M-Health adoption by healthcare professionals: A systematic review. J. Am. Med. Inform. Assoc. 2016, 23, 212–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunçalp, Ӧ.; Were, W.M.; Maclennan, C.; Oladapo, O.T.; Gülmezoglu, A.M.; Bahl, R.; Daelmans, B.; Mathai, M.; Say, L.; Kristensen, F.; et al. Quality of care for pregnant women and newborns—The WHO vision. BJOG Ann. Int. J. Obstet. Gynaecol. 2015, 122, 1045–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey (NFHS-4); Ministry of Health and Family Welfare: Mumbai, India, 2017.
- Lim, S.S.; Dandona, L.; Hoisington, J.A.; James, S.L.; Hogan, M.C.; Gakidou, E. India’s Janani Suraksha Yojana, a conditional cash transfer programme to increase births in health facilities: An impact evaluation. Lancet 2010, 375, 2009–2023. [Google Scholar] [CrossRef]
- Graham, W.J.; McCaw-Binns, A.; Munjanja, S. Translating Coverage Gains into Health Gains for All Women and Children: The Quality Care Opportunity. PLoS Med. 2013, 10, e1001368. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Yadav, V.; Balasubramaniam, S.; Jain, Y.; Joshi, C.S.; Saran, K.; Sood, B. Effectiveness of the WHO SCC on improving adherence to essential practices during childbirth, in resource constrained settings. BMC Pregnancy Childbirth 2016, 16, 345. [Google Scholar] [CrossRef] [Green Version]
- Varghese, B.; Copas, A.; Kumari, S.; Bandyopadhyay, S.; Sharma, J.; Saha, S.; Yadav, V.; Kumar, S. Does the safe childbirth checklist (SCC) program save newborn lives? Evidence from a realistic quasi-experimental study, Rajasthan, India. Matern. Heal. Neonatol. Perinatol. 2019, 5, 3. [Google Scholar] [CrossRef] [Green Version]
- Maternal Health Division; Ministry of Health and Family Welfare; Government of India. DAKSHATA: Empowering Providers for Improved MNH Care During Institutional Deliveries. A strategic Initiative to Strengthen Quality of Intra- and Immediate Postpartum Care. Operational Guidelines; Maternal Health Division Ministry of Health & Family Welfare Government of India: New Delhi, India, 2015.
- Semrau, K.E.A.; Hirschhorn, L.R.; Delaney, M.M.; Singh, V.P.; Saurastri, R.; Sharma, N.; Tuller, D.E.; Firestone, R.; Lipsitz, S.; Dhingra-Kumar, N.; et al. Outcomes of a coaching-based WHO safe childbirth checklist program in India. N. Engl. J. Med. 2017, 377, 2313–2324. [Google Scholar] [CrossRef]
- Spector, J.M.; Agrawal, P.; Kodkany, B.; Lipsitz, S.; Lashoher, A.; Dziekan, G.; Bahl, R.; Merialdi, M.; Mathai, M.; Lemer, C.; et al. Improving quality of care for maternal and newborn health: Prospective pilot study of the who safe childbirth checklist program. PLoS ONE 2012, 7, e35151. [Google Scholar] [CrossRef]
- Kruk, M.E.; Kujawski, S.; Moyer, C.A.; Adanu, R.M.; Afsana, K.; Cohen, J.; Glassman, A.; Labrique, A.; Reddy, K.S.; Yamey, G. Next generation maternal health: External shocks and health-system innovations. Lancet 2016, 388, 2296–2306. [Google Scholar] [CrossRef] [Green Version]
- Endehabtu, B.F.; Endehabtu, B.F.; Tadesse, Y.; Gelagay, A.A.; Tilahun, B.; Mekonnen, Z.A.; Gashu, K.D. Willingness to Use Mobile based e-Partograph and Associated Factors among Care Providers in North Gondar Zone, Northwest Ethiopia. Online J. Public Health Inform. 2019, 11, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Office of the Registrar General and Census Commissioner. India SRS Statistical Report 2016; Office of the Registrar General and Census Commissioner: New Delhi, India, 2016.
- Office of the Registrar General and Census Commissioner. Special Bulletin on Maternal Mortality in India 2016–2018: Sample Registration System; Office of the Registrar General and Census Commissioner: New Delhi, India, 2020.
- Dearing, J.W. Applying diffusion of innovation theory to intervention development. Res. Soc. Work Pract. 2009, 19, 503–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legris, P.; Ingham, J.; Collerette, P. Why do people use information technology? A critical review of the technology acceptance model. Inf. Manag. 2003, 40, 191–204. [Google Scholar] [CrossRef]
- Rahimi, B.; Nadri, H.; Afshar, H.L.; Timpka, T. A systematic review of the technology acceptance model in health informatics. Appl. Clin. Inform. 2018, 9, 604–634. [Google Scholar] [CrossRef] [Green Version]
- Maruping, L.M.; Bala, H.; Venkatesh, V.; Brown, S.A. Going beyond intention: Integrating behavioral expectation into the unified theory of acceptance and use of technology. J. Assoc. Inf. Sci. Technol. 2017, 68, 623–637. [Google Scholar] [CrossRef]
- Venkatesh, V.; Bala, H. Technology Acceptance Model 3 and a Research Agenda on Interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Gagnon, M.P.; Orruño, E.; Asua, J.; Abdeljelil, A.B.; Emparanza, J. Using a modified technology acceptance model to evaluate healthcare professionals’ adoption of a new telemonitoring system. Telemed. e-Health 2012, 18, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Suresh, V.; Prabhakar, K.; Santhanalakshmi, K.; Maran, K. Applying technology acceptance (TAM) model to determine the factors of acceptance in out-patient information system in private hospital sectors in Chennai city. J. Pharm. Sci. Res. 2016, 8, 1373–1377. [Google Scholar]
- Lakshmi, K.B.; Rajaram, M. Impact of information technology reliance and innovativeness on rural healthcare services: Study of Dindigul district in Tamil Nadu, India. Telemed. J. E Heal. 2012, 18, 360–370. [Google Scholar] [CrossRef]
- Manimaran, S.; Lakshmi, K.B. Development of model for assessing the acceptance level of users in rural healthcare system of Tamil Nadu, India. Technol. Heal. Care 2013, 21, 479–492. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How Many Interviews Are Enough? Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Macqueen, K.M.; Mclellan-Lemal, E.; Bartholow, K.; Milstein, B. Team-based Codebook Development: Structure, Process, and Agreement. In Handbook for Team-Based Qualitative Research; Guest, G., MacQueen, K.M., Eds.; AltaMira Press: Lanham, MD, USA, 2008; pp. 119–135. [Google Scholar]
- Emad, H.; El-Bakry, H.M.; Asem, A. A Modified Technology Acceptance Model for Health Informatics. Int. J. Artif. Intell. Mechatron. 2016, 4, 153–161. [Google Scholar]
- Holden, R.J.; Karsh, B.T. The Technology Acceptance Model: Its past and its future in health care. J. Biomed. Inform. 2010, 43, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dedoose Version 80.35, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data 2018; SocioCultural Research Consultants, LLC: Los Angeles, CA, USA, 2018.
- Yusof, M.M.; Stergioulas, L.; Zugic, J. Health information systems adoption: Findings from a systematic review. Stud. Health Technol. Inform. 2007, 129, 262–266. [Google Scholar] [PubMed]
- Khairat, S.; Marc, D.; Crosby, W.; Al Sanousi, A. Reasons for physicians not adopting clinical decision support systems: Critical analysis. J. Med. Internet Res. 2018, 20, e24. [Google Scholar] [CrossRef]
- Lai, F.; Macmillan, J.; Daudelin, D.; Kent, D. The potential of training to increase acceptance and use of computerized decision support systems for medical diagnosis. Hum. Factors 2006, 48, 95–108. [Google Scholar] [CrossRef]
- Khalifa, M. Clinical decision support: Strategies for success. Procedia Comput. Sci. 2014, 37, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Sittig, D. Electronic Health Records: Challenges in Design and Implementation; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. NPJ Digit. Med. 2020, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, S.; Sharma, S.K.; Fausto, D.J.; Viernes, S.; Kharrazi, H. Barriers and Facilitators to Clinical Decision Support Systems Adoption: A Systematic Review. J. Bus. Adm. Res. 2014, 3, 36. [Google Scholar] [CrossRef] [Green Version]
- Haberman, S.; Feldman, J.; Merhi, Z.O.; Markenson, G.; Cohen, W.; Minkoff, H. Effect of Clinical-Decision Support on Documentation Compliance in an Electronic Medical Record. Obstet. Gynecol. 2009, 114, 311–317. [Google Scholar] [CrossRef]
- Zakane, S.A.; Gustafsson, L.L.; Sie, A.; Tomson, G.; Loukanova, S.; Bastholm-Rahmner, P. Opportunities and obstacles using a clinical decision support system for maternal care in Burkina Faso. Online J. Public Health Inform. 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambasivan, M.; Esmaeilzadeh, P.; Kumar, N.; Nezakati, H. Intention to adopt clinical decision support systems in a developing country: Effect of Physician’s perceived professional autonomy, involvement and belief: A cross-sectional study. BMC Med. Inform. Decis. Mak. 2012, 12, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esmaeilzadeh, P.; Sambasivan, M.; Kumar, N.; Nezakati, H. Adoption of clinical decision support systems in a developing country: Antecedents and outcomes of physician’s threat to perceived professional autonomy. Int. J. Med. Inform. 2015, 84, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, K.; Sheikh, A. Organizational issues in the implementation and adoption of health information technology innovations: An interpretative review. Int. J. Med. Inform. 2013, 82, e73–e86. [Google Scholar] [CrossRef]
- Liberati, E.G.; Ruggiero, F.; Galuppo, L.; Gorli, M.; González-Lorenzo, M.; Maraldi, M.; Ruggieri, P.; Friz, H.P.; Scaratti, G.; Kwag, K.H.; et al. What hinders the uptake of computerized decision support systems in hospitals? A qualitative study and framework for implementation. Implement. Sci. 2017, 12, 1–13. [Google Scholar] [CrossRef]
- Khalifa, M.; Zabani, I. Improving utilization of clinical decision support systems by reducing alert fatigue: Strategies and recommendations. Stud. Health Technol. Inform. 2016, 226, 51–54. [Google Scholar]
- Zelellw, D.; Tegegne, T. The use and perceived barriers of the partograph at public health institutions in East Gojjam Zone, Northwest Ethiopia. Ann. Glob. Heal. 2018, 84, 198–203. [Google Scholar] [CrossRef] [Green Version]
- Litwin, L.E.; Maly, C.; Khamis, A.R.; Hiner, C.; Zoungrana, J.; Mohamed, K.; Drake, M.; Machaku, M.; Njozi, M.; Muhsin, S.A.; et al. Use of an electronic Partograph: Feasibility and acceptability study in Zanzibar, Tanzania. BMC Pregnancy Childbirth 2018, 18, 147. [Google Scholar] [CrossRef] [Green Version]
- Sanghvi, H.; Mohan, D.; Litwin, L.; Bazant, E.; Gomez, P.; Macdowell, T.; Onsase, L.; Wabwile, V.; Waka, C.; Qureshi, Z.; et al. Effectiveness of an electronic partogram: A mixed-method, quasi-experimental study among skilled birth attendants in Kenya. Glob. Heal. Sci. Pr. 2019, 7, 521–539. [Google Scholar] [CrossRef] [Green Version]
- Sukums, F.; Mensah, N.; Mpembeni, R.; Massawe, S.; Duysburgh, E.; Williams, A.; Kaltschmidt, J.; Loukanova, S.; Haefeli, W.E.; Blank, A. Promising adoption of an electronic clinical decision support system for antenatal and intrapartum care in rural primary healthcare facilities in sub-Saharan Africa: The QUALMAT experience. Int. J. Med. Inform. 2014, 84, 647–657. [Google Scholar] [CrossRef]
- Jean dit Gautier, E.; Bot-Robin, V.; Libessart, A.; Doucède, G.; Cosson, M.; Rubod, C. Design of a Serious Game for Handling Obstetrical Emergencies. JMIR Serious Games 2016, 4, e21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; DeMaria, S.; Goldberg, A.; Katz, D. A Systematic Review of Serious Games in Training Health Care Professionals. Simul. Healthc. J. Soc. Simul. Healthc. 2016, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Amoakoh-Coleman, M.; Borgstein, A.B.J.; Sondaal, S.F.V.; Grobbee, D.E.; Miltenburg, A.S.; Verwijs, M.; Ansah, E.K.; Browne, J.L.; Klipstein-Grobusch, K. Effectiveness of mHealth interventions targeting health care workers to improve pregnancy outcomes in low- and middle-income countries: A systematic review. J. Med. Internet Res. 2016, 18, e226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chigona, W.; Nyemba-Mudenda, M.; Metfula, A.S. A review on mHealth research in developing countries. J. Community Inform. 2013, 9. [Google Scholar]
- Mukisa, M.T.; Orwa Ochieng, D.; Waiganjo, P.W. Evaluating the Sustainability of mHealth Systems in Developing Countries: The Knowledge Gap. Int. J. Sci. Res. 2015, 6, 2319–7064. [Google Scholar]
- Tamrat, T.; Kachnowski, S. Special delivery: An analysis of mhealth in maternal and newborn health programs and their outcomes around the world. Matern. Child Health J. 2012, 16, 1092–1101. [Google Scholar] [CrossRef]
- Sundin, P.; Callan, J.; Mehta, K. Why do entrepreneurial mHealth ventures in the developing world fail to scale? J. Med. Eng. Technol. 2016, 40, 444–457. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| State | Type of Health Facility | Utilization of ASMAN (Based on % of Fields Completed) | |
|---|---|---|---|
| High | Low | ||
| Madhya Pradesh | District or subdistrict hospital | 1 | 1 |
| Community health center (CHC) | 2 | 2 | |
| Rajasthan | District or subdistrict hospital | 2 | 1 |
| Community health center (CHC) | 1 | 2 | |
| Total | 6 | 6 | |
| Characteristics of Respondents | Madhya Pradesh | Rajasthan | Total |
|---|---|---|---|
| Level of facility | |||
| Community health centers | 14 | 12 | 26 |
| Subdistrict/district hospitals | 6 | 12 | 18 |
| Cadre of health provider | |||
| Medical officers | 3 | 6 | 9 |
| Labor room supervisors | 3 | 7 | 10 |
| Staff nurse | 13 | 12 | 25 |
| Age of providers | |||
| Average age | 33 | 42 | 38 |
| Work experience | |||
| Median work time in the same facility (years) | 4 | 3 | 5 |
| Median total work experience (years) | 7 | 6 | 10 |
| Total | 20 | 24 | 44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usmanova, G.; Gresh, A.; Cohen, M.A.; Kim, Y.-M.; Srivastava, A.; Joshi, C.S.; Bhatt, D.C.; Haws, R.; Wadhwa, R.; Sridhar, P.; et al. Acceptability and Barriers to Use of the ASMAN Provider-Facing Electronic Platform for Peripartum Care in Public Facilities in Madhya Pradesh and Rajasthan, India: A Qualitative Study Using the Technology Acceptance Model-3. Int. J. Environ. Res. Public Health 2020, 17, 8333. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228333
Usmanova G, Gresh A, Cohen MA, Kim Y-M, Srivastava A, Joshi CS, Bhatt DC, Haws R, Wadhwa R, Sridhar P, et al. Acceptability and Barriers to Use of the ASMAN Provider-Facing Electronic Platform for Peripartum Care in Public Facilities in Madhya Pradesh and Rajasthan, India: A Qualitative Study Using the Technology Acceptance Model-3. International Journal of Environmental Research and Public Health. 2020; 17(22):8333. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228333
Chicago/Turabian StyleUsmanova, Gulnoza, Ashley Gresh, Megan A. Cohen, Young-Mi Kim, Ashish Srivastava, Chandra Shekhar Joshi, Deepak Chandra Bhatt, Rachel Haws, Rajni Wadhwa, Pompy Sridhar, and et al. 2020. "Acceptability and Barriers to Use of the ASMAN Provider-Facing Electronic Platform for Peripartum Care in Public Facilities in Madhya Pradesh and Rajasthan, India: A Qualitative Study Using the Technology Acceptance Model-3" International Journal of Environmental Research and Public Health 17, no. 22: 8333. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228333