Key Determinants of Anemia among Youngsters under Five Years in Senegal, Malawi, and Angola


Abstract
:1. Introduction
2. Methods and Materials
2.1. Source of Data
2.2. Variables
2.2.1. Outcome Variable
2.2.2. Explanatory Variables
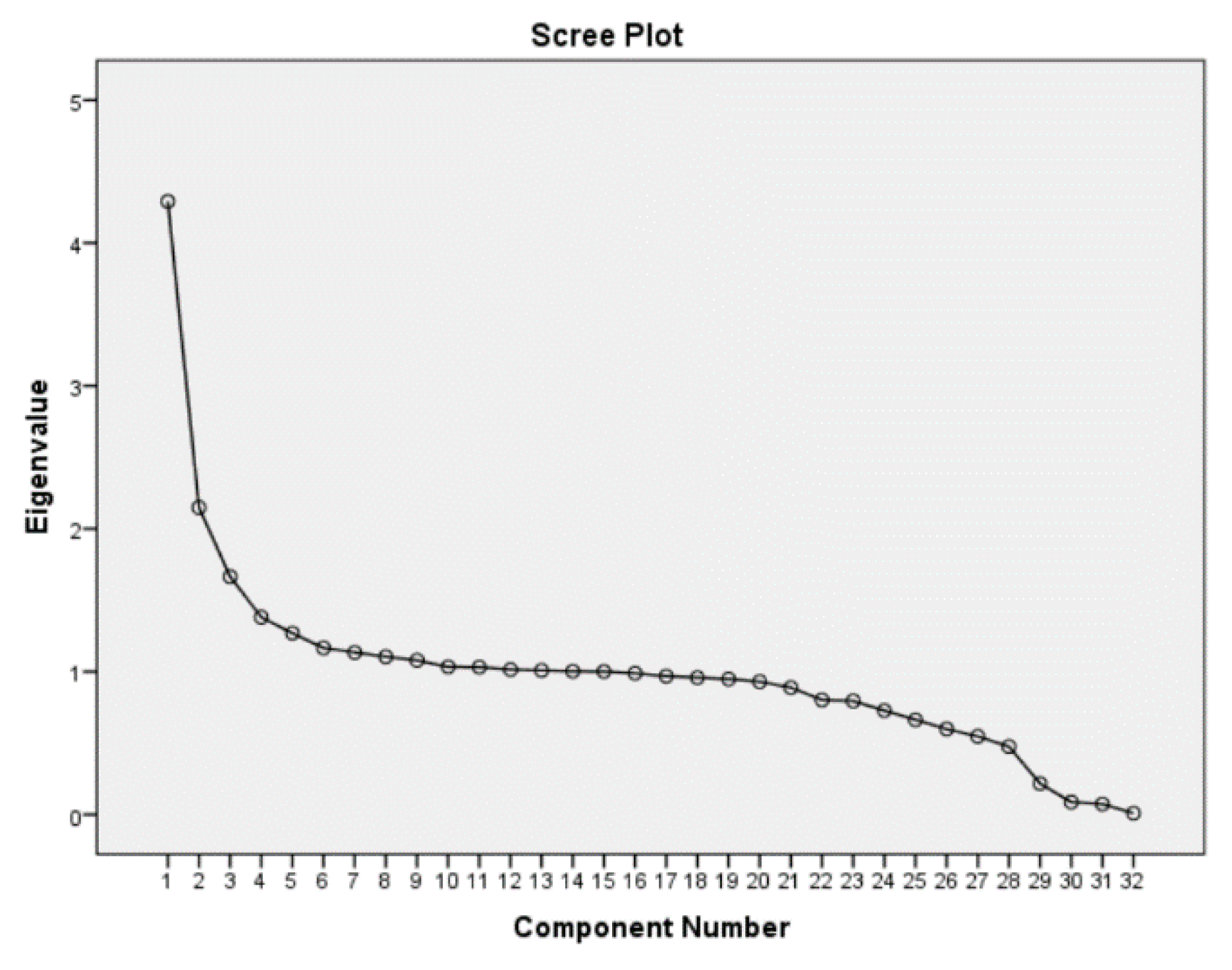
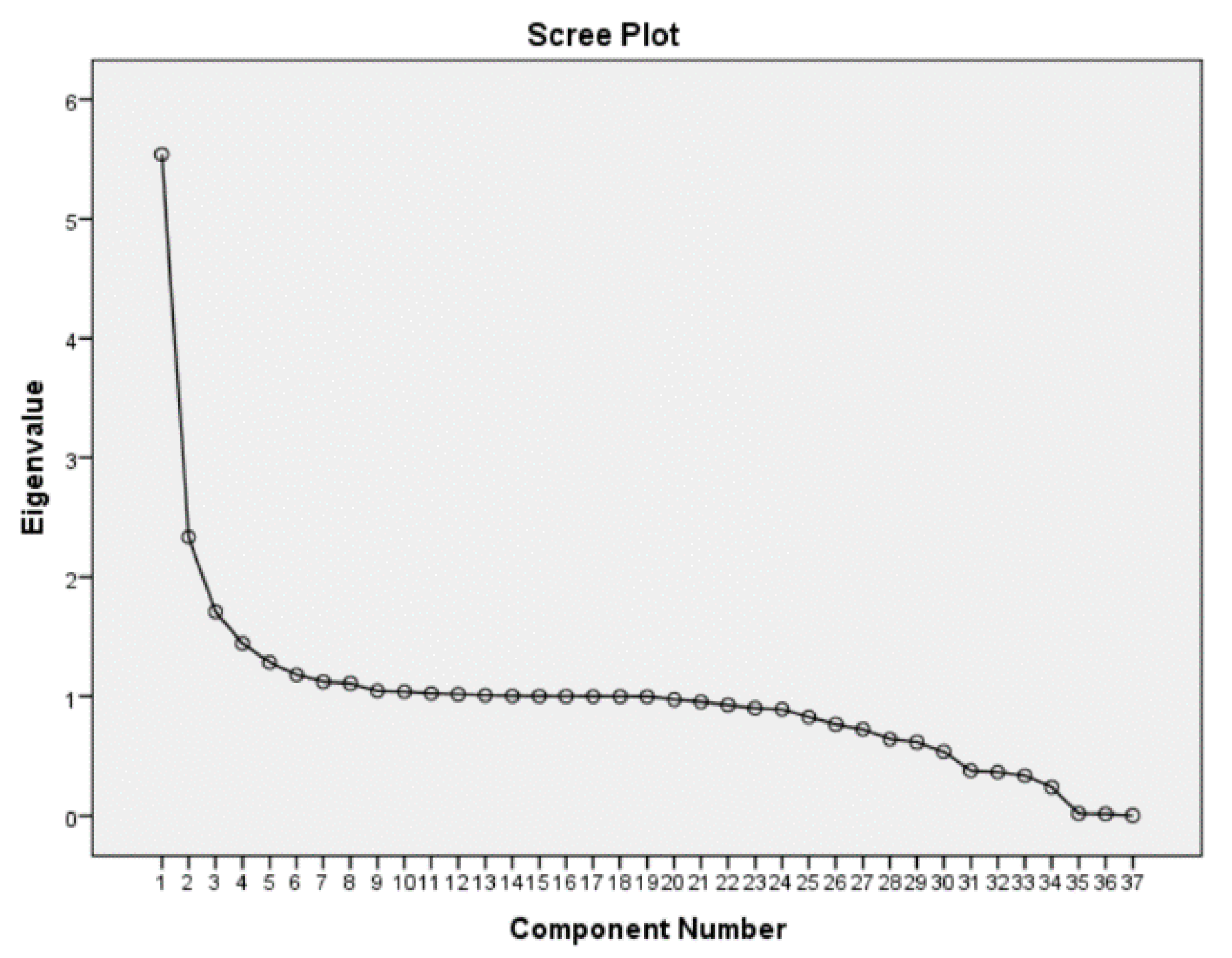
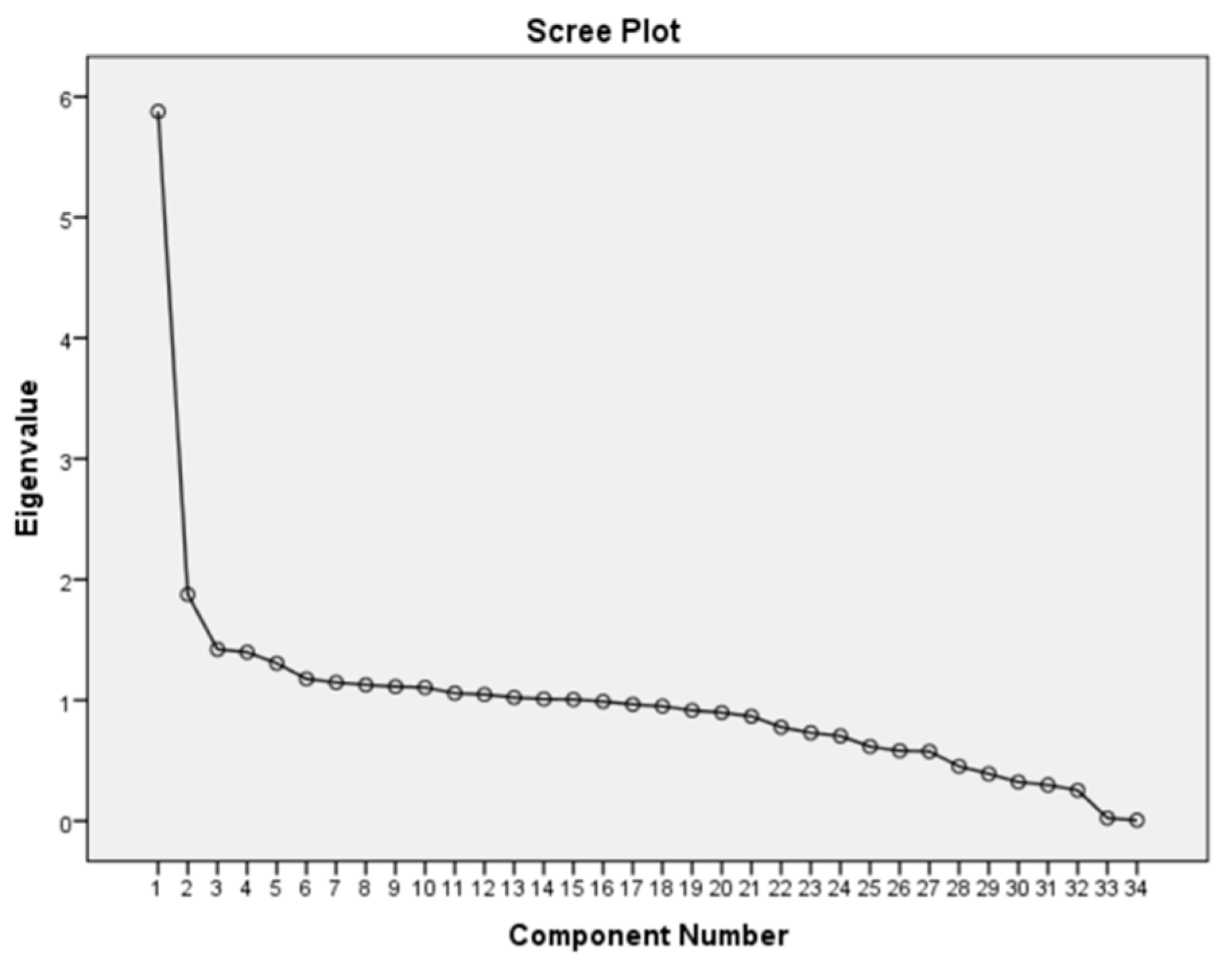
2.2.3. Computation of Wealth Index Using Principle Component Analysis (PCA)
2.3. Analyses
2.3.1. Descriptive Analysis
2.3.2. Multilevel Analysis
3. Results
3.1. Descriptive Analyses Interpretation
3.2. Multilevel Application
β4 Mother schoolingij + β5 Birth intervalij + β6 Wealth statusij + β7 Nutritional statusij + bi + bij
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gebreegziabiher, G.; Etana, B.; Niggusie, D. Determinants of anemia among children aged 6–59 months living in Kilte Awulaelo Woreda, Northern Ethiopia. Hindawi 2014, 2014, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kejo, D.; Petrucka, P.M.; Martin, H.; Kimanya, M.E.; Mosha, T.C.E. Prevalence and predictors of anemia among children under 5 years of age in Arusha District, Tanzania. Prediatric Health Med. Ther. 2016, 9, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschovis, P.P.; Wiens, M.O.; Arlingtona, L.; Antsygina, O.; Hayden, D.; Dzik, W.; Kiwanuka, J.P.; Christiani, D.C.; Hibberd, P.L. Individual, maternal and household risk factors for anemia among young children in sub-Saharan Africa: A cross sectional study. BMJ Open 2016, 8, 1–14. [Google Scholar]
- Kuziga, F.; Adoke, Y.; Wanyenze, R.K. Prevalence and factors associated with anemia among children aged 6 to 59 months in Namutumba district, Uganda: Across- sectional study. BMC Pediatrics 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beatty, A.; Ingwersen, N.; Leith, W.; Null, C. Anemia Prevalence and Correlates among Young Children and Pregnant Women in Indonesia; Mathematica Policy Research: Washington, DC, USA, 2017. [Google Scholar]
- World Health Organization The Globan Prevalence of Anemia in 2011; World Health Organization: Geneva, Switzerland, 2015.
- Sop, S.M.K.; Mananga, M.J.; Tetanye, E.; Gouado, I. Risk factors of anemia among young children in rural Cameron. Int. J. Curr. Microbiol. Appl. Sci. 2015, 4, 925–935. [Google Scholar]
- Iannotti, L.L.; Delnatus, J.R.; Odom, A.R.; Eaton, J.C.; Gribbs, J.J.; Brown, S.; Wol, P.B. Determinants of anemia and hemoglobin concentration in Haitian school-aged children. Am. J. Trop. Med. Hyg. 2015, 93, 1092–1098. [Google Scholar] [CrossRef] [Green Version]
- Foote, E.M.; Sullivan, K.M.; Ruth, L.J.; Oremo, J.; Sadumah, I.; Williams, T.N.; Suchdev, P.S. Determinants of anemia among preschool children in rural, Western Kenya. Am. J. Trop. Med. Hyg. 2013, 88, 757–764. [Google Scholar] [CrossRef] [Green Version]
- Gaston, T.R.; Ramroop, S.; Habyarimana, F. Determinants of factors associated with anemia among children under ve years in Lesotho. Afr. Popul. Stud. 2018, 32, 3893–3902. [Google Scholar]
- Ngwira, A.; Kazembe, L.N. Analysis of severity of childhood anemia in Malawi: A Bayesian ordered categories model. Open Access Med. Stat. 2016, 6, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Brabin, B.J.; Kalanda, B.F.; Verhoe, F.H.; Chimsuku, L.H.; Broadhead, R.L. Risk factors for fetal anemia in a malarias area of Malawi. Ann. Trop. Paediatr. 2004, 4, 311–321. [Google Scholar] [CrossRef]
- Ntenda PA, M.; Chaung, K.Y.; Tiruneh, F.N.; Chaung, Y.C. Multilevel analysis of the effects of individual and community level facotrs on childhood anemia, severe anemia and hemoglobin concentration in Malawi. J. Trop. Pediatrics 2004, 64, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Rosario EV, N.; Costa, D.; Francisco, D.; Brito, M. DHSS pro le: The Dande Health and Demographic Surveillance System (Dande HDSS, Angola). Int. J. Epidemiol. 2004, 46, 1094g. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Figueiredo, J.C.; Gamboa, D.; Pedro, J.M.; Fancony, C.; Langa, A.J.; Megalhaes RJ, S.; Stothard, J.R.; Nery, S.V. Epidemiology of malaria, schistosomiasis, geohelminths, anemia and malnutrition in the context of a Demographic surveillance System in Northern Angola. PLoS ONE 2012, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Diouf, S.; Sylla, A.; Diop, F.; Diallo, A.; Sarr, M. Anemia among apparently health Senegalese children aged 9–15 months. Int. J. Child Health Nutr. 2013, 2, 9–14. [Google Scholar]
- Tine RC, K.; Ndiaye, M.; Hansson, H.H.; Ndour, C.T.; Faye, B.; Alifrangis, M.; Sylla, K.; Ndiaye, J.L.; Magnussen, P.; Bygbjerg, I.C.; et al. The association between malaria parasitaemia, erythrocyte polymorphisms, malnutrition and anemia in children less than 10 years in Senegal: A case control study. BMC Res. 2012, 5, 1–10. [Google Scholar]
- McCuskee, S.; Brickley, E.B.; Wood, A.; Mossialos, E. Malaria and Macronutrient Deficiency as Correlates of Anemia in Young Children: A Systematic Review of Observational Studies. Ann. Glob. Health 2014, 80, 458–465. [Google Scholar] [CrossRef] [Green Version]
- Unicef. World Health Orginazation and World Bank Group. Levels and Trends in Child Malnutrition, 2017th ed.; World Bank Group: Washington, DC, USA, 2015. [Google Scholar]
- Fançony, C.; Lavinha, J.; Brito, M.; Barros, H. Anemia in preschool children from Angola: A review of the evidence. Porto Biomed. J. 2020, 5, 1–9. [Google Scholar] [CrossRef]
- Takele, K.; Zewotir, T.; Ndanguza, D. Understanding correlates of child stunting in Ethiopia using generalized linear mixed models. BMC Public Health 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, S.V.; Perkins, J.M.; Ozaltin, E.; Smith, G.D. Weight of nations: A socioeconomic analysis of women in low-to middle-income countries. Am. J. Clin. Nutr. 2011, 93, 413–421. [Google Scholar] [CrossRef] [Green Version]
- Neuman, M.; Kawachi, I.; Gortmaker, S.; Subramanian, S.V. Urban-rural differences in BMI in low- and middle-income countries: The role of socioeconomic status. Am. J. Clin. Nutr. 2013, 93, 428–436. [Google Scholar] [CrossRef] [Green Version]
- Khulu, C.; Ramroop, S. Determinants of malnutrition in under five children in Angola, Malawi and Senegal. Open Public Health J. 2020, 13, 3–9. [Google Scholar] [CrossRef]
- Muchie, K.F. Determinants of severity levels of anemia among children aged 6–59 months in Ethiopia: Further analysis of the 2011 Ethiopia Demographic and Health Survey. BMC Nutr. 2016, 2, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kawo, K.N.; Asfaw, Z.G.; Yohannes, N. Multilevel Analysis of Determinants of Anemia Preva-lence among Children Aged 659 Months in Ethiopia: Classical and Bayesian Approaches. Hindawi 2018, 2018, 1–13. [Google Scholar]
- Habyarimana, F.; Zewotir, T.; Ramroop, S. A proportional odds model with complex sampling design to identify key determinants of malnutrition of children under ve years in Rwanda. MCSER 2014, 5, 1642–1648. [Google Scholar]
- Ray, S.; Chandra, J.; Bhattachatjee, J.; Sharma, S.; Agarwal, A. Determinants of nutritional anemia in children less that ve years age. Int. J. Contemp. Pediatrics 2016, 3, 403–408. [Google Scholar] [CrossRef]
- Journee, M.; Nesterov, Y.; Richtarik, P.; Sepulchre, R. Generalized Power Method for Sparse Principal Component Analysis. J. Mach. Learn. Res. 2010, 11, 517–553. [Google Scholar]
- Anderson, R.; Black, W.; Hair, J.; Tatham, R. Multivariate Data Analysis, 5th ed.; Prentice Hall: New York, NY, USA, 1998. [Google Scholar]
- Talukder, A. Factors associated with malnutrition among under five children: Illustration using Bangladesh Demographic and Health Survey, 2014 data. MDPI 2017, 4, 88. [Google Scholar] [CrossRef] [Green Version]
- Feddag, M.L.; Mesbah, M. Approximate estimation in Generalized Linear Mixed Models with applications to the Rasch Model. Comput. Math. Appl. 2006, 51, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, R.G. 8.1.1 SPPSS Syntax-Six Reasons You Should Use It, SPSS Tutorial, Viewed 17 May 2016 2013. Available online: http://www.spss-tutorials.com/spss-combining-data-with-syntax-and-output (accessed on 20 August 2020).
- Schabenberger, O. Introducing the GLIMMIX Procedure for Generalized Linear Mixed Models; Paper 196-30; SAS Institute Inc.: Cary, NC, USA, 2014. [Google Scholar]
- Ncogo, P.; Romay-Barja, M.; Benito, A.; Aparicio, P.; Nseng, G.; Berzosa, P.; Santana-Morales, M.A.; Riloha, M.; Valladares, B.; Herrador, Z. Prevalence of anemia and associated factors in children living in urban and rural settings from Bata District, Equatorial Guinea. PLoS ONE 2017, 12, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Khan, J.R.; Awan, N.; Misu, F. Determinant of anemia among 6–59 months aged children in Bangladesh: Evidence from natially representative data. BMC Pediatr. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zhoa, A.; Zhang, Y.; Peng, Y.; Li, J.; Yang, T.; Liu, Z.; Lv, Y.; Wang, P. Prevalence of anemia and its risk factors among children 6–36 months old in Burma. Am. J. Trop. Med. Hyg. 2012, 87, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Woldie, H.; Kebede, Y.; Tariku, A. Factors associated with Anemia among children aged 6–23 months attending growth monitoring at Tsitsika health center, Wag-Himra Zone, Northern Ethiopia. J. Nutr. Metab. 2014, 2015, 1–9. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Severe Anemic | Moderate Anemic | Mild Anemic |
|---|---|---|---|
| Senegal | 76 | 901 | 1881 |
| Malawi | 63 | 1310 | 2856 |
| Angola | 102 | 1257 | 3111 |
| Country | Year | Age of Children (months) | Community Type | Gender | Sample Size |
|---|---|---|---|---|---|
| Senegal | 2016 | 0–59 | Rural and Urban | Male and Female | 2858 |
| Malawi | 2015–2016 | 0–59 | Rural and Urban | Male and Female | 4229 |
| Angola | 2015–2016 | 0–59 | Rural and Urban | Male and female | 4470 |
| Factors * | Severe (%) | Moderate (%) | Mild (%) | r (p-Value) | χ2 (p-Value) |
|---|---|---|---|---|---|
| Residence setting | |||||
| Rural | 180 (2.4%) | 2396 (32.0%) | 4923 (65.6%) | - | 0.000 |
| Urban | 61 (1.5%) | 1072 (26.4%) | 2925 (72.1%) | ||
| Youngster’s age (months) | |||||
| 0–12 | 22 (3.1%) | 348 (49.8%) | 329 (47.1%) | 0.000 | - |
| 13–23 | 50 (2.9%) | 769 (44.0%) | 927 (53.1%) | ||
| 24–35 | 60 (2.4%) | 800 (32.3%) | 1620 (65.3%) | ||
| 36–47 | 71 (2.2%) | 860 (26.1%) | 2366 (71.8%) | ||
| 48–59 | 38 (1.1%) | 691 (20.7%) | 2606 (78.1%) | ||
| Gender of youngster | |||||
| Male | 147 (2.5%) | 1831 (31.4%) | 3851 (66.1%) | - | 0.000 |
| Female | 94 (1.6%) | 1637 (28.6%) | 3997 (69.8%) | ||
| Mother schooling | |||||
| Primary | 199 (2.4%) | 2615 (31.5%) | 5498 (66.1%) | 0.000 | - |
| Secondary | 29 (1.3%) | 579 (26.8%) | 1551 (71.8%) | ||
| Higher | 4 (2.6%) | 29 (18.6%) | 123 (78.8%) | ||
| Birth interval | |||||
| <24 | 20 (2.3%) | 224 (26.0%) | 616 (71.6%) | 0.046 | - |
| 24–47 | 85 (2.1%) | 1171 (29.2%) | 2755 (68.7%) | ||
| >47 | 61 (1.9%) | 1002 (30.7%) | 2204 (67.5%) | ||
| Wealth status | |||||
| Poor | 178 (3.1%) | 1921 (33.2%) | 3680 (63.7%) | 0.000 | - |
| Middle | 35 (1.4%) | 701 (28.3%) | 1739 (70.3%) | ||
| Not poor | 28 (0.8%) | 846 (25.6%) | 2429 (73.5%) | ||
| Birth order | |||||
| 2–3 | 72 (2.1%) | 1024 (29.8%) | 2344 (68.1%) | 0.221 | - |
| 4–5 | 54 (2.4%) | 658 (29.4%) | 1525 (68.2%) | ||
| >5 | 48 (1.6%) | 876 (28.9%) | 2102 (69.5%) | ||
| Nutritional status | |||||
| Severe | 76 (3.9%) | 717 (36.5%) | 1171 (59.6%) | 0.000 | - |
| Moderate | 39 (2.5%) | 477 (30.0%) | 1073 (67.5%) | ||
| Nourished | 126 (1.6%) | 2274 (28.4%) | 5604 (70.0%) | ||
| Marital status | |||||
| Married | 16 (2.0%) | 219 (28.0%) | 548 (70.0%) | - | 0.762 |
| Living together | 200 (2.1%) | 2855 (30.1%) | 6432 (67.8%) | ||
| Widowed | 23 (2.0%) | 352 (30.6%) | 776 (67.4%) |
| Factors * | Est. | Std. Error | OR | p-Values |
|---|---|---|---|---|
| Intercept | −0.685 | 0.132 | 0.035 | |
| Mild | ||||
| Intercept | 2.466 | 0.148 | 0.003 | |
| Moderate | ||||
| Residence setting | ||||
| Ref: Urban | ||||
| Rural | −0.067 | 0.062 | 0.935 | 0.280 |
| Youngster’s age | ||||
| Ref: 0–12 | ||||
| 13–23 | 0.350 | 0.120 | 1.419 | 0.004 |
| 24–35 | 0.825 | 0.117 | 2.282 | <0.001 |
| 36–47 | 1.155 | 0.116 | 3.174 | <0.001 |
| 48–59 | 1.584 | 0.118 | 4.874 | <0.001 |
| Gender of youngster | ||||
| Ref: Male | ||||
| Female | 0.180 | 0.050 | 1.197 | <0.001 |
| Mother schooling | ||||
| Ref: Higher | ||||
| Primary | 0.105 | 0.273 | 1.111 | 0.702 |
| Secondary | 0.213 | 0.076 | 1.237 | 0.005 |
| Birth interval | ||||
| Ref: 0–24 months | ||||
| 24–47 | −0.022 | 0.091 | 0.978 | 0.809 |
| >47 | −0.083 | 0.057 | 0.920 | 0.144 |
| Wealth status | ||||
| Ref: Not poor | ||||
| Poor | 0.270 | 0.076 | 1.310 | <0.001 |
| Middle | 0.194 | 0.073 | 1.214 | 0.008 |
| Nutritional status | ||||
| Ref: Nourished | ||||
| Severe | 0.400 | 0.069 | 1.492 | <0.001 |
| Moderate | 0.194 | 0.093 | 1.214 | 0.037 |
| McFadden R Squared | 0.254 |
| Factors | Num DF * | Den DF * | F Value | p Value |
|---|---|---|---|---|
| Residence | 1 | 7737 | 1.17 | 0.280 |
| Youngster’s age | 4 | 7737 | 80.02 | <0.001 |
| Gender of youngster | 1 | 7737 | 12.88 | <0.001 |
| Mother Schooling | 2 | 7737 | 3.89 | 0.021 |
| Birthing Interval | 2 | 7737 | 1.13 | 0.322 |
| Wealth Status | 2 | 7737 | 7.15 | <0.001 |
| Nutritional Status | 2 | 7737 | 18.08 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khulu, C.; Ramroop, S. Key Determinants of Anemia among Youngsters under Five Years in Senegal, Malawi, and Angola. Int. J. Environ. Res. Public Health 2020, 17, 8538. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228538
Khulu C, Ramroop S. Key Determinants of Anemia among Youngsters under Five Years in Senegal, Malawi, and Angola. International Journal of Environmental Research and Public Health. 2020; 17(22):8538. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228538
Chicago/Turabian StyleKhulu, Chris, and Shaun Ramroop. 2020. "Key Determinants of Anemia among Youngsters under Five Years in Senegal, Malawi, and Angola" International Journal of Environmental Research and Public Health 17, no. 22: 8538. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228538