Infection and Risk Perception of SARS-CoV-2 among Airport Workers: A Mixed Methods Study



Abstract
:1. Introduction
2. Materials and Methods
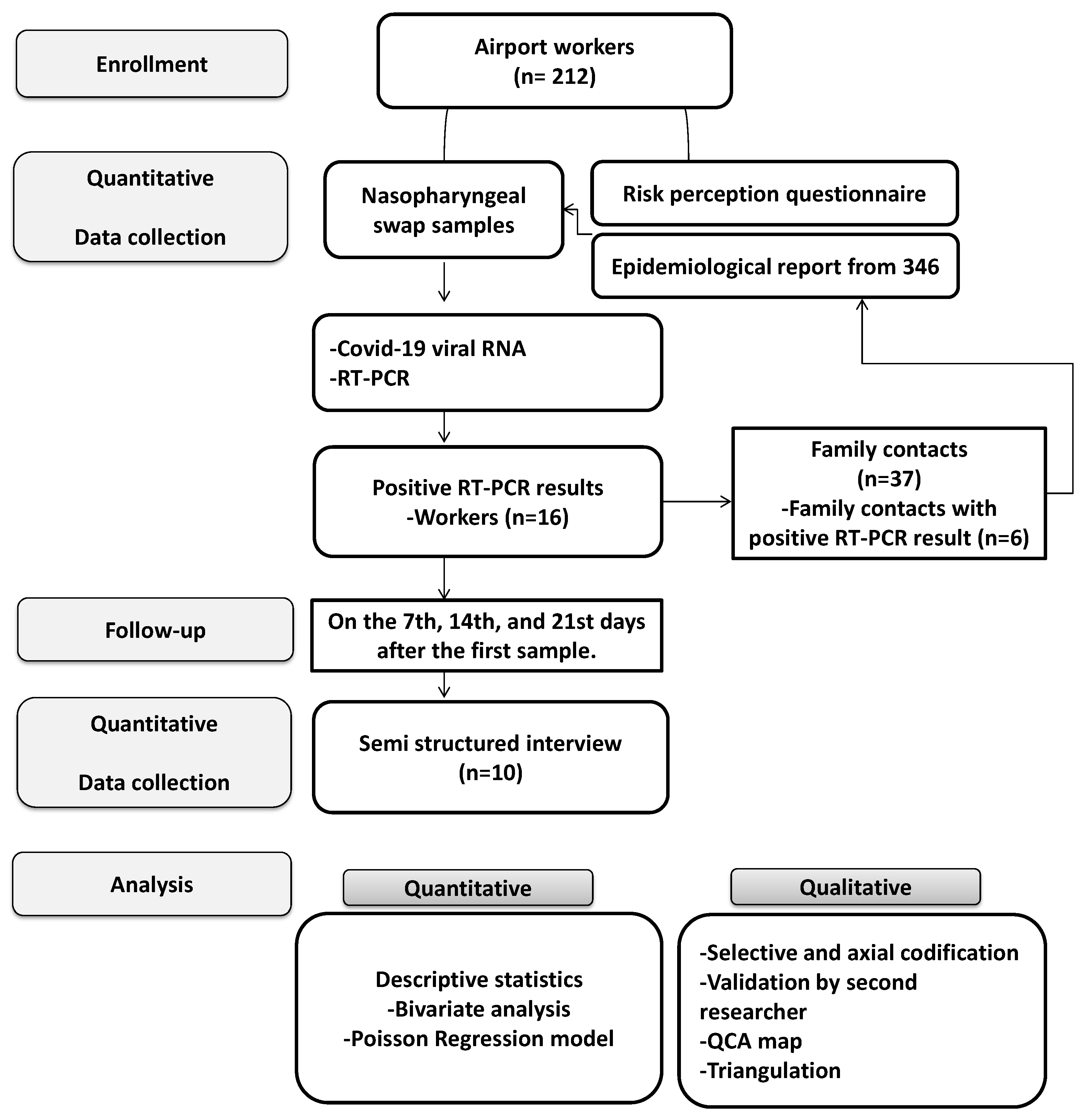
2.1. Study Design
2.2. Population
2.3. Sample and Sampling
2.4. Specific Hazard Assessment Matrix for SARS-CoV-2
2.5. The Sociodemographic Survey, Risk Perception Scale, and Epidemiological Files
2.6. Biological Samples
2.7. Worker Contacts
2.8. The Follow-Up of Cases at Home
2.9. Semistructured Interviews
2.10. Sample and Sampling
2.11. Interview Categories
2.12. Conducting the Interview
2.13. Information Processing and Analysis—Quantitative Data
2.14. Information Processing and Analysis—Qualitative Data
2.15. Triangulation and Integration of Results
2.16. Ethical Considerations
3. Results
3.1. SARS-CoV-2 Incidence, Clinical Presentation, and Risk Factors
3.2. Perception of Risk regarding COVID-19
3.3. Elements Involved in the Perception of Risk Associated with COVID-19
3.4. Semistructured Interviews
3.5. Perception of the Risk of Coronavirus Infection
Participant 1: “During the last two weeks of March, we encountered the phenomenon of having several foreign citizens at the airport, either because flights were delayed or flights were canceled, and they were stranded. This represents an inconvenience for the airport in the sense that we do not have hotel capacity, we do not have hotel facilities, so we had to improvise to be able to accommodate people”.
Participant 7: “I feel safe because, in the airport, they disinfect, and I have to go through filters and wash my hands. I feel more insecure being in the street because, at the airport, they disinfect after each shift, so I don’t feel unsafe at the airport”.
3.6. Protective Behaviors
Participant 4: “I have a disinfectant mat at home; when I arrive home, I clean my shoes, wash my hands. I take off all my clothes and put them in the washing machine. Now, I don’t go anywhere without a mask, I have stopped frequenting certain places, I do everything virtually, and as soon as deliveries arrive, I disinfect them”.
3.7. Risky Practices Associated with Coronavirus Infection
Participant 9: “I reckon that I was infected because of the roast chicken we order for delivery. We all took off our face masks; we talked and ate at the same time, reaching our hands into the box”.
Participant 2: “I feel that the immigration arrival area is narrow, and many flights conclude during the peak hours of operation between 7 and 9 at night, with about 15 or 20 flights arriving in normal operation, so I believe that the measures that are going to be taken here in the future are to space precisely these places of arrival, especially because it is congested”.
3.8. Recording Symptoms
Participant 10: “I also took my temperature every four hours. I had my Excel there until I saw that my temperature began to fluctuate between 35 and 37 degrees, I said ok, I’m fine, I stopped there”.
3.9. Changing Behavior
Participant 5: “I have become tireless with self-care, with hand washing. I carry my gel everywhere; I hardly speak in the workplace. What is necessary, what touches me? It’s a shame because I love to talk, but that is a risk for me and my family, for my colleagues. So, I wash my hands about three times an hour. And when I get home, I take off my shoes at the entrance, disinfect them and go straight for the shower”.
Participant 8: “…I stopped ordering food at home. That’s a lot of risk”.
Participant 4: “I like cycling, practicality. But the people on the street are super relaxed, and there are many people without masks, so neither, I do sports at home, on the roller, I try to support myself, and I don’t take much care of my family”.
Participant 5: “As a result of these feelings that I was going to die, I feel that God gave me another opportunity to live again. Now I talk to my mother almost every day; I thank God that I am alive and I can enjoy her”.
3.10. Sharing Experience
Participant 1: “I downloaded Resolution 666 and put it in an app, where through your cell phone you choose options such as taking a quiz and it is a contest. So, I did that with my family, with the use of masks, hand washing, social distancing, etc., and I started doing it because I felt the need to help”.
3.11. Emotions and Feelings in the Face of the Coronavirus
Participant 5: “My immediate feeling was death; I felt that I was going to die. That I was going to stop seeing my children (sobs), that I was no longer going to be with my husband. Seeing those things that happened in Spain and Italy, which people died in the street, was impressive. For me, COVID-19 is equal to death”.
Participant 4: “What I feel now individually is wanting to help. I understand that they took a sample from us to determine the existence of antibodies or not, but if I can help you, I will be in the first line to say go ahead, and right now, for me, it is a high priority, to help my family, saying don’t do this or that”.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef]
- Ministerio del Interior de Colombia. Decreto 457; 2020. Available online: https://dapre.presidencia.gov.co/normativa/normativa/DECRETO%20457%20DEL%2022%20DE%20MARZO%20DE%202020.pdf (accessed on 17 November 2020).
- OECD Food Supply Chains and COVID-19: Impacts and Policy Lessons 2020. Available online: http://www.oecd.org/coronavirus/policy-responses/food-supply-chains-and-covid-19-impacts-and-policy-lessons-71b57aea/ (accessed on 17 November 2020).
- Gosadi, I.M.; BinSaeed, A.; Al-Hazmi, A.M.; Fadl, A.A.; Alharbi, K.H.; Swarelzahab, M.M. Evaluation of applied public health emergency system at Prince Mohammed International Airport in Almedinah during Hajj season 2014: A qualitative case study. BMC Res. Notes 2015, 8, 435. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization International Health Regulations 2005. Third Edition. Available online: https://www.who.int/publications/i/item/9789241580496 (accessed on 17 November 2020).
- Mouchtouri, V.A.; Christoforidou, E.P.; van der Heiden, M.; Lemos, C.M.; Fanos, M.; Rexroth, U.; Grote, U.; Belfroid, E.; Swaan, C.; Hadjichristodoulou, C. Exit and Entry Screening Practices for Infectious Diseases among Travelers at Points of Entry: Looking for Evidence on Public Health Impact. Int. J. Environ. Res. Public Health 2019, 16, 4638. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kim, M. Estimating the number of Korean workers at high risk of COVID-19 infection. Epidemiol. Health 2020, e2020051. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.G.; Peckham, T.K.; Seixas, N.S. Estimating the burden of United States workers exposed to infection or disease: A key factor in containing risk of COVID-19 infection. PLoS ONE 2020, 15, e0232452. [Google Scholar] [CrossRef] [PubMed]
- Lupton, D. Theorizing risk. In Risk; Routledge: Abingdon, UK, 2013; p. 272. ISBN 9780415622547. [Google Scholar]
- Slovic, P. The Psychology of risk. Saúde Soc. 2010, 19, 731–747. [Google Scholar] [CrossRef]
- Lupton, D. Risk and emotion: Towards an alternative theoretical perspective. Health Risk Soc. 2013, 15, 634–647. [Google Scholar] [CrossRef]
- van der Linden, S. Determinants and Measurement of Climate Change Risk Perception, Worry, and Concern. SSRN J. 2017. [Google Scholar] [CrossRef]
- Quilty, B.J.; Clifford, S.; Flasche, S.; Eggo, R.M. Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV). Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- Haider, N.; Yavlinsky, A.; Simons, D.; Osman, A.Y.; Ntoumi, F.; Zumla, A.; Kock, R. Passengers’ destinations from China: Low risk of Novel Coronavirus (2019-nCoV) transmission into Africa and South America. Epidemiol. Infect. 2020, 148, e41. [Google Scholar] [CrossRef] [Green Version]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2020, 49, 717–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aeropuerto El Dorado Estadísticas 2019. 2020. Available online: https://eldorado.aero/comunicados/estadisticas-del-aeropuerto (accessed on 17 November 2020).
- Ivankova, N.V.; Creswell, J.W.; Stick, S.L. Using Mixed-Methods Sequential Explanatory Design: From Theory to Practice. Field Methods 2006, 18, 3–20. [Google Scholar] [CrossRef]
- Schoonenboom, J.; Johnson, R.B. How to Construct a Mixed Methods Research Design. Kölner Z. Soziologie Soz. 2017, 69, 107–131. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W. Mixed-Method Research. In Handbook of Educational Policy; Elsevier: Amsterdam, The Netherlands, 1999; pp. 455–472. ISBN 978-0-12-174698-8. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Páez, S.G.; Franco, C.; Cruz-Rivera, A.; Cerón, J.F.; Castañeda-Orjuela, C.; Páez-Salamanca, G.N.; Franco-Restrepo, C.; Zea, J.F.; Cruz-Rivera, É.; Quiroz-Salazar, A.; et al. Estimación del Número Reproductivo Efectivo de la Transmisión del COVID-19 en Colombia; Instituto Nacional de Salud: Bogotá, Colombia, 2020; p. 23. [Google Scholar]
- Dean, A.G.; Sullivan, K.M. OpenEPi: Open Source Epidemiolic Statistics for Public Health. Available online: https://www.openepi.com/BriefDoc/About.htm (accessed on 8 April 2020).
- World Health Organization. Protocol for Assessment of Potential Risk Factors for 2019-Novel Coronavirus (2019-nCoV) Infection among Health Care Workers in a Health Care Setting. Available online: https://www.who.int/publications-detail/protocol-for-assessment-of-potential-risk-factors-for-2019-novel-coronavirus-(2019-ncov)-infection-among-health-care-workers-in-a-health-care-setting (accessed on 31 March 2020).
- Pérez-Fuentes, M.D.C.; Molero Jurado, M.D.M.; Oropesa Ruiz, N.F.; Martos Martínez, Á.; Simón Márquez, M.D.M.; Herrera-Peco, I.; Gázquez Linares, J.J. Questionnaire on Perception of Threat from COVID-19. J. Clin. Med. 2020, 9, 1196. [Google Scholar] [CrossRef]
- Pedrosa, I.; Suárez-Álvarez, J.; García-Cueto, E. Evidencias sobre la Validez de Contenido: Avances Teóricos y Métodos para su Estimación [Content Validity Evidences: Theoretical Advances and Estimation Methods]. Acción Psicológica 2014, 10, 3–18. [Google Scholar] [CrossRef]
- Instituto Nacional de Salud Guía para la Vigilancia por Laboratorio del Virus de la Influenza y otros Virus Respiratorios 2017. Available online: https://www.ins.gov.co/Direcciones/ONS/Historico_Rt/Estimaci%C3%B3n%20del%20n%C3%BAmero%20reproductivo%20efectivo%20de%20la%20trasmisi%C3%B3n%20del%20Covid-19%20en%20Colombia.pdf (accessed on 17 November 2020).
- Corman, V.; Bleicker, T.; Brünink, S.; Drosten, C.; Zambon, M. Diagnostic detection of 2019-nCoV by real-time RT-PCR 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/protocol-v2-1.pdf (accessed on 17 November 2020).
- DeJonckheere, M.; Vaughn, L.M. Semistructured interviewing in primary care research: A balance of relationship and rigour. Fam. Med. Community Health 2019, 7, e000057. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Advocacy, Communication and Social Mobilization for TB Control; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Slovic, P.; Västfjäll, D. Affect, moral intuition, and risk. Psychol. Inq. 2010, 21, 387–398. [Google Scholar] [CrossRef]
- Majid, M.A.A.; Othman, M.; Mohamad, S.F.; Lim, S.A.H.; Yusof, A. Piloting for Interviews in Qualitative Research: Operationalization and Lessons Learnt. Int. J. Acad. Res. Bus. Soc. Sci. 2017, 7, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Ardila-Suárez, E.; Rueda-Arenas, J. Theoretical Saturation in Grounded Theory: Its Delimitation in the Analysis of Life Trajectories of Victims of Forced Displacement in Colombia. Rev. Colomb. Sociol. 2013, 36, 93–114. [Google Scholar]
- Riffenburgh, R.H. Chapter 6—Statistical Testing, Risks, and Odds in Medical Decisions. In Statistics in Medicine, 2nd ed.; Riffenburgh, R.H., Ed.; Academic Press: Burlington, NJ, USA, 2006; pp. 93–114. ISBN 978-0-12-088770-5. [Google Scholar]
- Freund, R.J.; Wilson, W.J.; Mohr, D.L. Nonparametric Methods. In Statistical Methods; Elsevier: Amsterdam, The Netherlands, 2010; pp. 689–719. ISBN 978-0-12-374970-3. [Google Scholar]
- IBM Corporation Métodos de Selección de Variables en el Análisis de Regresión Logística. Available online: www.ibm.com/support/knowledgecenter/es/sslvmb_sub/statistics_mainhelp_ddita/spss/regression/logistic_regression_methods.html (accessed on 13 April 2020).
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. Eur. J. Gen. Pract. 2018, 24, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elo, S.; Kääriäinen, M.; Kanste, O.; Pölkki, T.; Utriainen, K.; Kyngäs, H. Qualitative Content Analysis: A Focus on Trustworthiness. SAGE Open 2014, 4, 215824401452263. [Google Scholar] [CrossRef]
- Janesick, V.J. Peer Debriefing. In The Blackwell Encyclopedia of Sociology; Ritzer, G., Ed.; John Wiley & Sons, Ltd.: Oxford, UK, 2015; ISBN 978-1-4051-2433-1. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; AUT: Klagenfurt, Austria, 2014. [Google Scholar]
- Company-Morales, M.; Rubio, M.; Fontalba, A. Manual de Investigación Cualitativa en Enfermería. Introducción a la Investigación Cualitativa; Company-Morales: Almería, Italy, 2017. [Google Scholar]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research Through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, J.L.G.; Erdmann, A.L.; Meirelles, B.H.S.; de Lanzoni, G.M.M.; da Cunha, V.P.; Ross, R. Integração entre dados quantitativos e qualitativos em uma pesquisa de métodos mistos. Texto Context—Enferm. 2017, 26. [Google Scholar] [CrossRef]
- Malagón-Rojas, J.; Mercado-Reyes, M.M.; Gómez-Rendón, C. SARS-CoV-2 and work transmission: Results of from a prospective cohort of airport workers, 2020. Rev. Bras. Med. Trab. 2020, 19. awaiting assignment. [Google Scholar]
- Instituto Nacional de Salud Coronavirus en Colombia. Available online: https://www.ins.gov.co/Noticias/Paginas/Coronavirus.aspx (accessed on 31 March 2020).
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K. Knowledge and Perceptions of COVID-19 Among Health Care Workers: Cross-Sectional Study. JMIR Public Health Surveill. 2020, 6, e19160. [Google Scholar] [CrossRef]
- Azlan, A.A.; Hamzah, M.R.; Sern, T.J.; Ayub, S.H.; Mohamad, E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS ONE 2020, 15, e0233668. [Google Scholar] [CrossRef]
- Chen, X.; Ran, L.; Liu, Q.; Hu, Q.; Du, X.; Tan, X. Hand Hygiene, Mask-Wearing Behaviors and Its Associated Factors during the COVID-19 Epidemic: A Cross-Sectional Study among Primary School Students in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 2893. [Google Scholar] [CrossRef]
- Hillier, M.D. Using effective hand hygiene practice to prevent and control infection. Nurs. Stand. 2020, 35, 45–50. [Google Scholar] [CrossRef]
- Anderson, E.L.; Turnham, P.; Griffin, J.R.; Clarke, C.C. Consideration of the Aerosol Transmission for COVID-19 and Public Health. Risk Anal. 2020, 40, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, C.; Arija, V.; Aretouli, E.; Tsilidis, K.K.; Bulló, M. Comparing eating behaviours, and symptoms of depression and anxiety between Spain and Greece during the COVID-19 outbreak: Cross-sectional analysis of two different confinement strategies. Eur. Eat. Disord. Rev. 2020, erv.2772. [Google Scholar] [CrossRef] [PubMed]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 1–13. [Google Scholar] [CrossRef]
- Wise, T.; Zbozinek, T.D.; Michelini, G.; Hagan, C.C. Changes in risk perception and protective behavior during the first week of the COVID-19 pandemic in the United States. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Pagnini, F.; Bonanomi, A.; Tagliabue, S.; Balconi, M.; Bertolotti, M.; Confalonieri, E.; Di Dio, C.; Gilli, G.; Graffigna, G.; Regalia, C.; et al. Knowledge, Concerns, and Behaviors of Individuals During the First Week of the Coronavirus Disease 2019 Pandemic in Italy. JAMA Netw. Open 2020, 3, e2015821. [Google Scholar] [CrossRef]
- Álvarez, G.; Delgado, J. Diseño de Estudios Epidemiológicos. I. El Estudio Transversal: Tomando una Fotografía de la Salud y la Enfermedad. Bol. Clin. Hosp. Infant. Estado Sonora 2015, 32, 26–34. [Google Scholar]
- Berlin, C.-U. Main Topic: Coronavirus. Available online: https://www.charite.de/en/clinical_center/themes_hospital/main_topic_coronavirus/ (accessed on 4 June 2020).


{kind=link}
| Category | Definition | Question |
|---|---|---|
| Perception of the risk of the contagion of coronavirus in the workplace and at home [11] | Individual perception about the probability of the infection occurring in the workplace or of infecting others | -What do you know about COVID-19? -Which positions do you consider to be the highest risk for contracting coronavirus? -Are there any areas of the airport that you particularly think are more likely to infect workers? |
| Intra and extraoccupational risk practices related to the spread of SARS-CoV-2 [30] | Practices are material events that constitute social reality. The practices are linked to beliefs, emotions, and conceptions | -What practices have you implemented as a result of the coronavirus infection? -What practices do you consider risky in your work? -What practices have you implemented in your home and your workplace? |
| Emotions about the coronavirus [31] | It is the set of feelings, hunches, and beliefs around a particular situation | -What feelings does the coronavirus generate in you? -How do these feelings influence the way you do your job? |
| Question | Mean | Median | SD | Range |
|---|---|---|---|---|
| How exposed do you feel to the coronavirus in your job? | 5.88 | 6 | 2.61 | 9 |
| How much does coronavirus infection affect your life? | 7.59 | 8 | 2.38 | 9 |
| How long do you think the coronavirus infection will last? | 6.88 | 7 | 1.79 | 8 |
| Do you feel symptoms due to coronavirus infection? | 2.00 | 1 | 1.78 | 9 |
| How concerned are you about coronavirus infection? | 7.39 | 8 | 2.11 | 9 |
| How emotionally does the coronavirus infection affect you? | 5.74 | 6 | 2.47 | 9 |
| Variable | Crude RR (95% CI) | Adjusted RR (95% CI) | p |
|---|---|---|---|
| Age | 1.00 (0.99–1.01) | 1.001 (0.99–1.00) | 0.99 |
| Sex (female) | 0.89 (0.78–1.01) | 0.92 (0.81–1.06) | 0.27 |
| Socioeconomic level | 0.99 (0.93–1.06) | 1.01 (0.94–1.09) | 0.99 |
| Risk level (low) | 1.24 (1.01–1.51) | 1.27 (1.04–1.55) | 0.19 |
| Ethnic | 1.14 (1.03–1.26) | 1.08 (0.97–1.20) | 0.13 |
| Not having had symptoms of COVID-19/RT-PCR (−) | 1.03 (1.00–1.06) | 1.00 (0.97–1.12) | 0.64 |
| Having had symptoms of COVID-19/RT-PCR (+) | 1.02 (0.93–1.12) | 1.01 (0.92–1.12) | 0.73 |
| Effect on life due to the pandemic | 1.091 (1.06–1.12) | 1.06 (1.03–1.10) | 0.00 |
| Concern about the pandemic situation | 1.09 (1.06–1.12) | 1.06 (1.02–1.10) | 0.00 |
| Emotional impact by the pandemic | 1.04 (1.02–1.07) | 0.99 (0.96–1.02) | 0.56 |
| Worker Roll | Age Years | Sex | Educational Level | Marital Status | Work Experience | COVID-19 Diagnosis Date | # Days after RT-PCR Was Negative | Disease Course |
|---|---|---|---|---|---|---|---|---|
| Administrative | 52 | Male | Postgraduate | Married | 14 | 23/03/2020 | 7 | Asymptomatic |
| Administrative | 43 | Male | Postgraduate | Married | 8 | 23/03/2020 | 21 | Asymptomatic |
| Administrative | 44 | Male | Postgraduate | Married | 5 | 23/03/2020 | 14 | Mild disease |
| Operative | 38 | Female | University | Married | 6 | 7/07/2020 | 21 | Mild disease |
| Operative | 29 | Female | University | Single | 2 | 7/07/2020 | 21 | Asymptomatic |
| Administrative | 31 | Female | Postgraduate | Married | 4 | 7/07/2020 | 14 | Asymptomatic |
| Operative | 35 | Male | University | Married | 4 | 23/03/2020 | 7 | Asymptomatic |
| Operative | 38 | Male | Technical | Married | 5 | 7/07/2020 | 14 | Mild disease |
| Administrative | 35 | Female | University | Single | 4 | 7/07/2020 | 21 | Mild disease |
| Operative | 40 | Male | University | Married | 8 | 7/07/2020 | 14 | Mild disease |
| Category | Subcategory | Definition |
|---|---|---|
| Practices | Protective behaviors | Activities or behaviors that decrease the transmission of SARS-CoV-2 |
| Risky practices associated with coronavirus infection | Activities or behaviors that favor the transmission of SARS-CoV-2 | |
| Recording symptoms | Activity to get a record of the symptoms experienced | |
| Changing behavior | Set of activities carried out by people aimed at modifying their behavior in the face of a specific experience | |
| Sharing experience | Manifest activity by the worker where he or she declares the need to publicize their experience of the SARS-CoV-2 infection | |
| Emotions in the face of the coronavirus | Experienced feelings during the COVID-19 episode | Feelings or emotions expressed by people who have had COVID-19 |
| Post-COVID-19 feelings and emotions | Feelings or emotions expressed by people who have had COVID-19 |
| Quantitative Results | Qualitative Results | Mixed Methods Inference | |||
|---|---|---|---|---|---|
| Instrument | Findings | Category | Subcategory | Findings | |
| RT-PCR for SARS-CoV-2 | Accumulate incidence (7.5%) | Practices | Protective behaviors | Frequent hand-washing, after work showers, shoe disinfection was considered protective practices | Adherence to the recommendations may be influenced by the conditions in the environment, such as the availability of protective equipment, soap, and gel. Moreover, the promotion of protective behaviors should involve people with whom the worker lives. |
| Asymptomatic cases (81.25%) | Risky practices associated with the contagion of coronavirus | Risky practices are associated with keeping in touch with foreign passengers and activities out of the work (visiting shopping centers, supermarkets, banks). The risk of transmission is associated with public spaces | Recommendations to prevent the transmission of SARS-CoV-2 should not be limited to the work area. It should include the extra-work sphere. | ||
| Positive close contacts (16.2%) | Changing behavior | Increasing physical activity, avoiding crowded places, preventing using public transport and touching metallic surfaces | The transmission of the virus was associated with longer trips from home to office, independently from the mode of transport. Participants who experienced COVID-19 considered the usage of public transport as a risky practice. | ||
| No outbreaks per area reported during the period | Recording symptoms | Recording the experienced symptoms during the COVID-19 is a practice used to check the well-being | |||
| Risk factors and sociodemographic characterization | Prolonged trips from home-office increased risk | Sharing experience | Telling the experience of COVID-19 with relatives and coworkers was a practice declared by participants who had the disease. | Expressing emotions during and after the COVID-19 episode may be an opportunity to reinforce the surveillance system and communicate the risk in the workspace | |
| Workers living with a person working at home reduces the risk of infection | Emotions in the face of the coronavirus | Experimented feelings during the COVID-19 episode | Fear of death, anger, anguish, uncertainty are the feelings associated with the COVID-19 | ||
| High adherence to the usage of face mask and frequent hand washing (98%) | Post-COVID-19 feelings and emotions | Appreciation and the feeling of having a new opportunity. | |||
| COVID-19 risk perception questionnaire | Risk perception medium–high | Risk perception | Risk perception | The perception of risk is medium to high. Nevertheless, the job place is perceived as a safe place to work | The promotion of visible individual protective practices such as frequent hand washing and wearing facemask was associated with the risk of transmission of SARS-CoV-2 |
| Risk of transmission is associated with activities where passengers are involved | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malagón-Rojas, J.; Parra B, E.L.; Mercado, M. Infection and Risk Perception of SARS-CoV-2 among Airport Workers: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 9002. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239002
Malagón-Rojas J, Parra B EL, Mercado M. Infection and Risk Perception of SARS-CoV-2 among Airport Workers: A Mixed Methods Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9002. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239002
Chicago/Turabian StyleMalagón-Rojas, Jeadran, Eliana L. Parra B, and Marcela Mercado. 2020. "Infection and Risk Perception of SARS-CoV-2 among Airport Workers: A Mixed Methods Study" International Journal of Environmental Research and Public Health 17, no. 23: 9002. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239002