Early Phase Management of the SARS-CoV-2 Pandemic in the Geographic Area of the Veneto Region, in One of the World’s Oldest Populations

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Study Group
2.3. Parameters
2.4. Statistical Analysis
3. Results and Discussion
3.1. The Virus
3.2. Infection, Disease, and Gender Differences
- By air, through saliva and aerosol secretions from the upper airways through coughing and/or sneezing;
- By close direct contact as a result of a handshake before touching the mucous membranes of the mouth, nose, and eyes with contaminated hands;
- By the fecal–oral route.
- The immune response, both innate and adaptive, which is more effective in women than in men [3],
- Genetics: The COVID-19 virus penetrates into cells by binding to the ACE2 receptor, which is an enzyme that regulates arterial vasoconstriction. It is expressed on the cells of the lung epithelium, where it protects the lung from damage caused by infections, inflammation, and stress. When the virus enters the cell, it reduces the ACE2 expression and therefore its protective function [4]. Female cells have two X chromosomes and to prevent the redundant expression of the products of the genes present in double copies on the X chromosomes, physiological epigenetic random inactivation of one of the two chromosomes occurs. However, some chromosomal loci escape the inactivation and can be overexpressed. ACE2 is encoded in a non-inactivated region of the X chromosome, supporting the hypothesis of a greater expression in the lungs of women, thus ensuring its protective function, even during infection [5]. Finally, it should be emphasized that the role of the TMPRSS2 serine protease, which is structurally and functionally integrated in the ACE2 receptor, increases the entry of the virus into cells almost 100-fold [6]. The expression of TMPRSS2 is androgen-dependent, thereby explaining its disadvantage in males [7].
3.3. ULSS 5 Population
3.4. Population Genetics: Beta Thalassemia and Blood Types
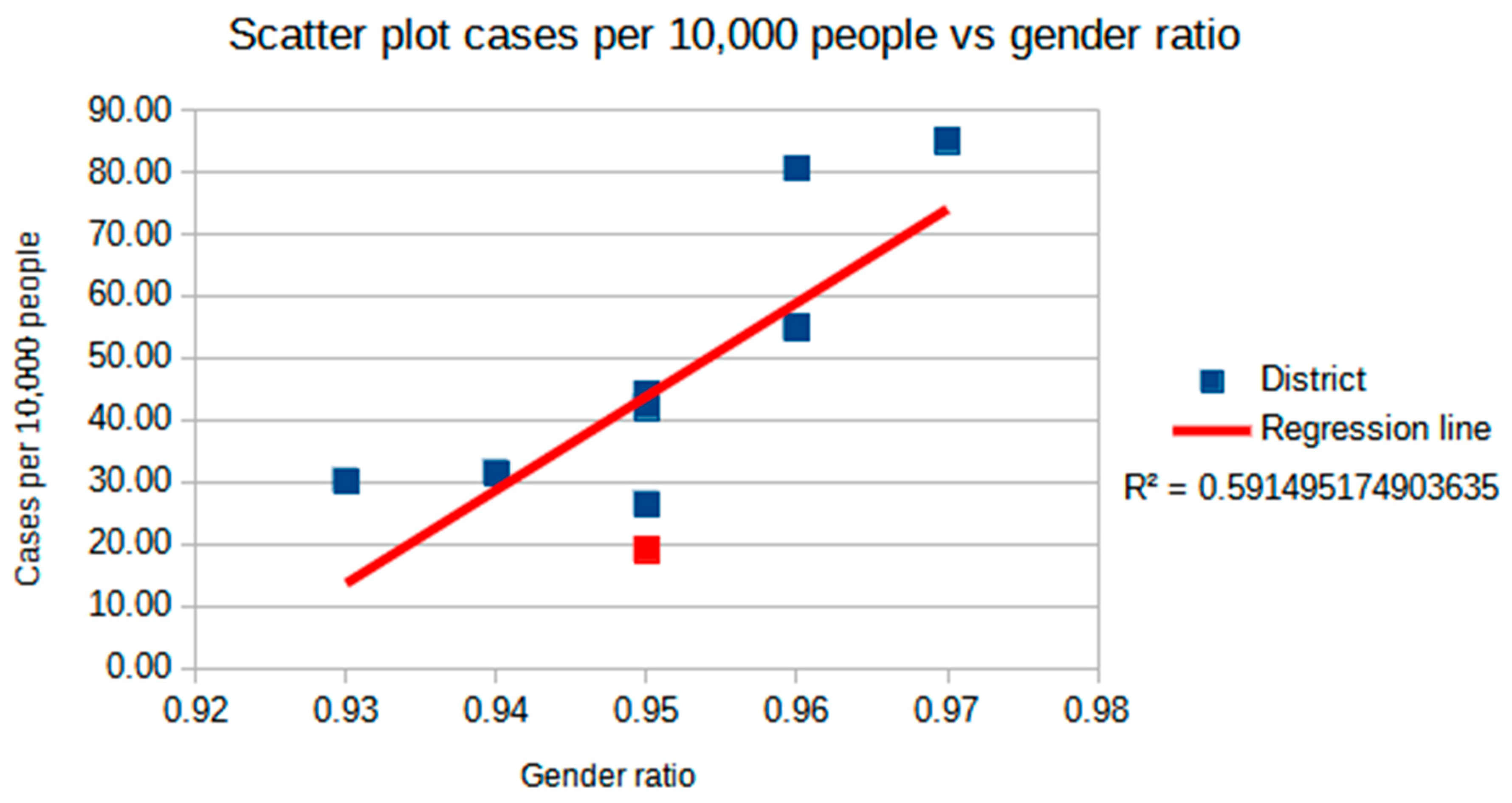
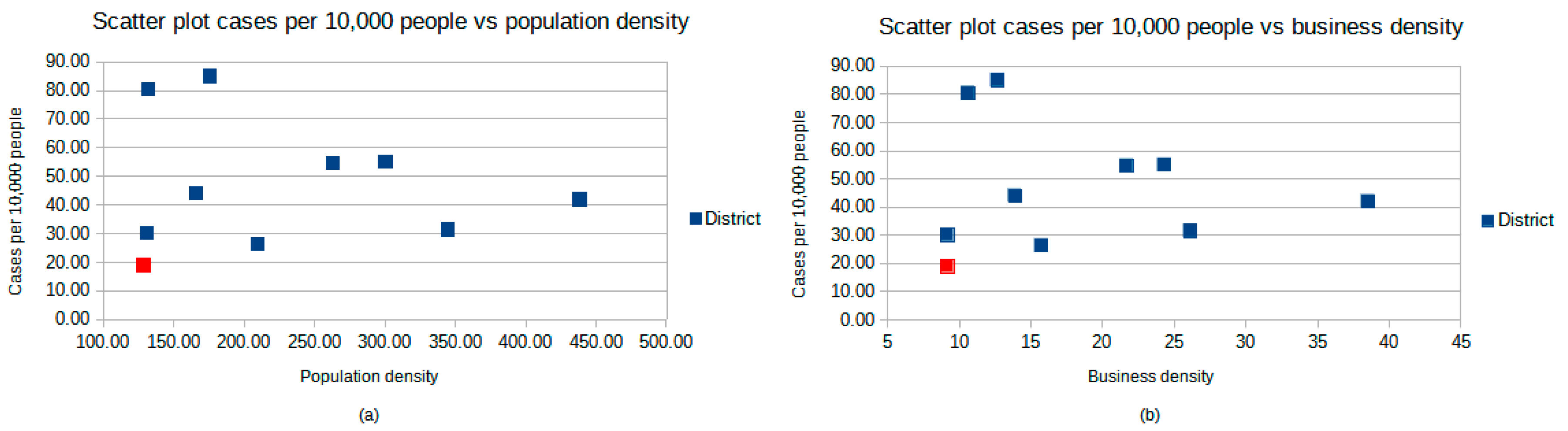
3.5. The Territory and Orography of the Province of Rovigo/ULSS 5, Pollution, and Economic Activities
3.6. Timing of Events in an Unstable and Unclear Landscape of Laws and Regulations
- At 30 days before our 0 time (end of January/start of February): Active telephone surveillance and names provided to the police forces for about 50 students returning from the Chinese New Year celebrations. China had already informed students to remain in isolation and ULSS 5 immediately activated a voluntary isolation procedure of 14 days, despite the absence of regulatory norms by the region or the ministry;
- At 30 days (28 January): First letter to schools to activate the passive surveillance of Chinese students who had returned from risk areas (the first regional provision in this sense was on 11 February);
- +1 (22 February): Even in the absence of precise indications on isolation, all subjects of the district of Rovigo who had passed through Vo’ or Schiavonia hospital were placed in isolation. At the end of February, 220 subjects had been placed in solitary confinement;
- +2 (23 February): A systematic epidemiological investigation began with the isolation of all close and not close contacts of positive subjects (first contact). On 30 June, there were 19,286 SARS-CoV-2 positive cases in the Veneto region, of which 444 were from the district of Rovigo, with 51 subjects in home isolation. The number of swabs performed from 21 February to 30 June was 46,443.
3.7. Integrated Approach of Activities: Public Health, Territorial Assistance, and Nursing Homes
3.7.1. Governance
3.7.2. Timeliness
3.7.3. Integration
- The “immediate availability” of the professionals mentioned above, in synergy with healthcare professionals already in place in the Hygiene and Public Health Service;
- The integration of a nursing coordinator from the ULSS within the settings affected by epidemic outbreaks, in order to offer local support in emergency management;
- Specific training, e-learning (distance learning and online training) or face-to-face training sessions, organized where required, provided by the ULSS 5 Training Center;
- Additional and customized supplies of personal protective equipment (PPE), according to needs.
3.8. ULSS 5’s Integrated Approach with “External” Institutions
3.9. External Communication towards Population Management and Internal Organization
3.10. Strong “Military” Command Chain and Change in the Organizational/Productive Model
3.11. Personal Protective Equipment (PPE) Management
3.12. Molecular Diagnostics as Routine and Rapid 24 h Response
- Standard molecular diagnostics with 24 h TAT;
- Rapid molecular diagnostics with 4 h TAT;
- Serological tests for antibody research.
3.12.1. Standard Molecular Test
3.12.2. Rapid Molecular Test
3.12.3. Serological Diagnostics
4. Conclusions
- Chain of command in centralized Directorate General Management with “military-style” characteristics: Cascade transmission of decisions with rapid changes by hospital/territorial organizations in the face of data and situations that gradually followed one another;
- Ability of the Directorate General Management to inform and involve local structures/institutions in decisions quickly and consistently;
- Management’s ability to “stay on course”, align the organization on decisions, and translate the numerous regional and national regulations into concrete and clear actions;
- Use of the fastest and simplest digital tools for the transmission of directives to the OUs and territorial units to spread awareness and reach as many people as possible on the outside;
- Ability of healthcare workers to understand the singularity of the emergency by accepting directives that did not respect the classic formal bureaucratic model of the public administration in terms of the content and distribution.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dossier Coronavirus. Available online: https://portale.fnomceo.it/wp-content/uploads/2020/04/dossier_coronavirus_del_13-05-2020-compresso.pdf (accessed on 1 September 2020).
- Ministero della Salute Covid-19—Situazione nel Mondo. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5338&area=nuovoCoronavirus&menu=vuoto (accessed on 10 October 2020).
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Lodi, E.; Scavone, A.; Reggianini, L.; Modena, M.G. COVID-19: A gendered disease? Possible interpretations and knowledge limitations. G. Ital. Cardiol. 2020, 21, 570–574. [Google Scholar] [CrossRef]
- EpiCentro Differenze di Genere in COVID-19: Possibili Meccanismi. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-differenze-genere-possibili-meccanismi (accessed on 10 October 2020).
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Montopoli, M.; Zumerle, S.; Vettor, R.; Rugge, M.; Zorzi, M.; Catapano, C.V.; Carbone, G.M.; Cavalli, A.; Pagano, F.; Ragazzi, E.; et al. Androgen-deprivation therapies for prostate cancer and risk of infection by SARS-CoV-2: A population-based study (N = 4532). Ann. Oncol. 2020, 31, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Lansiaux, E.; Pébaÿ, P.P.; Picard, J.-L.; Son-Forget, J. COVID-19: Beta-thalassemia subjects immunised? Med. Hypotheses 2020, 142, 109827. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Li, H. COVID-19: Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism; Organización Panamericana de la Salud: Washington, DC, USA, 2020. [Google Scholar]
- Setti, L.; Passarini, F.; De Gennaro, G.; Barbieri, P.; Licen, S.; Perrone, M.G.; Piazzalunga, A.; Borelli, M.; Palmisani, J.; Di Gilio, A.; et al. Potential role of particulate matter in the spreading of COVID-19 in Northern Italy: First observational study based on initial epidemic diffusion. BMJ Open 2020, 10, e039338. [Google Scholar] [CrossRef] [PubMed]
- Martelletti, L.; Martelletti, P. Air Pollution and the Novel Covid-19 Disease: A Putative Disease Risk Factor. SN Compr. Clin. Med. 2020, 2, 383–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazzini, M.; Baresi, C.; Bisci, C.; Bna, C.; Cecili, A.; Giuliacci, A.; Illuminati, S.; Pregliasco, F.; Miccadei, E. Preliminary Analysis of Relationships between COVID19 and Climate, Morphology, and Urbanization in the Lombardy Region (Northern Italy). Int. J. Environ. Res. Public Health 2020, 17, 6955. [Google Scholar] [CrossRef] [PubMed]
- Rosario, D.K.A.; Mutz, Y.S.; Bernardes, P.C.; Conte-Junior, C.A. Relationship between COVID-19 and weather: Case study in a tropical country. Int. J. Hyg. Environ. Health 2020, 229, 113587. [Google Scholar] [CrossRef]
- Kodera, S.; Rashed, E.A.; Hirata, A. Correlation between COVID-19 Morbidity and Mortality Rates in Japan and Local Population Density, Temperature, and Absolute Humidity. Int. J. Environ. Res. Public Health 2020, 17, 5477. [Google Scholar] [CrossRef]
- Coccia, M. An index to quantify environmental risk of exposure to future epidemics of the COVID-19 and similar viral agents: Theory and Practice. Environ. Res. 2020, 110155. [Google Scholar] [CrossRef] [PubMed]
- Kadi, N.; Khelfaoui, M. Population density, a factor in the spread of COVID-19 in Algeria: Statistic study. Bull. Natl. Res. Centre 2020, 44, 138. [Google Scholar] [CrossRef] [PubMed]
- Copiello, S.; Grillenzoni, C. The spread of 2019-nCoV in China was primarily driven by population density. Comment on “Association between short-term exposure to air pollution and COVID-19 infection: Evidence from China” by Zhu et al. Sci. Total Environ. 2020, 744, 141028. [Google Scholar] [CrossRef] [PubMed]
- Fortaleza, C.M.C.B.; Guimarães, R.B.; de Almeida, G.B.; Pronunciate, M.; Ferreira, C.P. Taking the inner route: Spatial and demographic factors affecting vulnerability to COVID-19 among 604 cities from inner São Paulo State, Brazil. Epidemiol. Infect. 2020, 148, e118. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Zhang, H.; Yang, Y.; Wan, H.; Wang, Y. Impacts of geographic factors and population density on the COVID-19 spreading under the lockdown policies of China. Sci. Total Environ. 2020, 746, 141347. [Google Scholar] [CrossRef]
- Bherwani, H.; Anjum, S.; Kumar, S.; Gautam, S.; Gupta, A.; Kumbhare, H.; Anshul, A.; Kumar, R. Understanding COVID-19 transmission through Bayesian probabilistic modeling and GIS-based Voronoi approach: A policy perspective. Environ. Dev. Sustain. 2020, 1–19. [Google Scholar] [CrossRef]
- Hamidi, S.; Ewing, R.; Sabouri, S. Longitudinal analyses of the relationship between development density and the COVID-19 morbidity and mortality rates: Early evidence from 1165 metropolitan counties in the United States. Health Place 2020, 64, 102378. [Google Scholar] [CrossRef]
- Hamidi, S.; Sabouri, S.; Ewing, R. Does Density Aggravate the COVID-19 Pandemic? Early Findings and Lessons for Planners. J. Am. Plan. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Tammes, P. Social distancing, population density, and spread of COVID-19 in England: A longitudinal study. BJGP Open 2020, 4. [Google Scholar] [CrossRef]
- Bontempi, E.; Vergalli, S.; Squazzoni, F. Understanding COVID-19 diffusion requires an interdisciplinary, multi-dimensional approach. Environ. Res. 2020, 188, 109814. [Google Scholar] [CrossRef]
- Liu, Y.; Gu, Z.; Xia, S.; Shi, B.; Zhou, X.-N.; Shi, Y.; Liu, J. What are the underlying transmission patterns of COVID-19 outbreak? An age-specific social contact characterization. EClinicalMedicine 2020, 22, 100354. [Google Scholar] [CrossRef] [PubMed]
- Bavel, J.J.V.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Sugg, M.M.; Spaulding, T.J.; Lane, S.J.; Runkle, J.D.; Harden, S.R.; Hege, A.; Iyer, L.S. Mapping community-level determinants of COVID-19 transmission in nursing homes: A multi-scale approach. Sci. Total Environ. 2020, 752, 141946. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Temkin-Greener, H.; Shan, G.; Cai, X. COVID-19 Infections and Deaths among Connecticut Nursing Home Residents: Facility Correlates. J. Am. Geriatr. Soc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, G.V.; Biedron, C.; Fink, L.R.; Hatfield, K.M.; Polistico, J.M.F.; Meyer, M.P.; Noe, R.S.; Copen, C.E.; Lyons, A.K.; Gonzalez, G.; et al. Initial and Repeated Point Prevalence Surveys to Inform SARS-CoV-2 Infection Prevention in 26 Skilled Nursing Facilities—Detroit, Michigan, March–May 2020. MMWR 2020, 69, 882–886. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, K.M.; Reddy, S.C.; Forsberg, K.; Korhonen, L.; Garner, K.; Gulley, T.; James, A.; Patil, N.; Bezold, C.; Rehman, N.; et al. Facility-Wide Testing for SARS-CoV-2 in Nursing Homes—Seven U.S. Jurisdictions, March-June 2020. MMWR 2020, 69, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.; O’Laughlin, K.; Ehrlich, H.Y.; Campbell, L.; Harizaj, A.; Durante, A.; Leung, V. Point Prevalence Testing of Residents for SARS-CoV-2 in a Subset of Connecticut Nursing Homes. JAMA 2020. [Google Scholar] [CrossRef]
- Trabucchi, M.; De Leo, D. Nursing homes or besieged castles: COVID-19 in northern Italy. Lancet Psychiatry 2020, 7, 387–388. [Google Scholar] [CrossRef]
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Schwartz, N.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef]
- Abrams, H.R.; Loomer, L.; Gandhi, A.; Grabowski, D.C. Characteristics of U.S. Nursing Homes with COVID-19 Cases. J. Am. Geriatr. Soc. 2020, 68, 1653–1656. [Google Scholar] [CrossRef]
- ECDC Public Health Emergency Team; Danis, K.; Fonteneau, L.; Georges, S.; Daniau, C.; Bernard-Stoecklin, S.; Domegan, L.; O’Donnell, J.; Hauge, S.H.; Dequeker, S.; et al. High impact of COVID-19 in long-term care facilities, suggestion for monitoring in the EU/EEA, May 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- Kemenesi, G.; Kornya, L.; Tóth, G.E.; Kurucz, K.; Zeghbib, S.; Somogyi, B.A.; Zöldi, V.; Urbán, P.; Herczeg, R.; Jakab, F. Nursing homes and the elderly regarding the COVID-19 pandemic: Situation report from Hungary. GeroScience 2020, 1–7. [Google Scholar] [CrossRef]
- Kittang, B.R.; von Hofacker, S.; Solheim, S.P.; Krüger, K.; Løland, K.K.; Jansen, K. Outbreak of COVID-19 at three nursing homes in Bergen. Tidsskr. Norske Laegeforen. 2020, 140. [Google Scholar] [CrossRef]
- Survey Nazionale sul Contagio COVID-19 Nelle Strutture Residenziali e Sociosanitarie. Istituto Superiore di Sanità. 2020. Available online: https://www.epicentro.iss.it/coronavirus/pdf/sars-cov-2-survey-rsa-rapporto-finale.pdf (accessed on 1 September 2020).
- Indagine di Sieroprevalenza sul Sars-CoV-2. Istituto Nazionale di Statistica. 2020. Available online: https://www.istat.it/it/files/2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 7 September 2020).
- COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 7 October 2020).




{kind=link}
{kind=link}
{kind=link}
| District | Inhabitants (N.) | Men (N.) | Women (N.) | Gender Ratio | Area (km2) | Population Density (Inhabitants/km2) | Mean Age | Percentage of Population Aged 65 and over (%) | Ageing Index | Confirmed Cases at 06.30 (N.) | Cases per 10,000 People (N.) | Business per km2 (N.) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ROVIGO | 233,366 | 113,665 | 119,721 | 0.95 | 1819.35 | 128.27 | 48.5 | 26.4 | 242.4 | 444 | 19.03 | 9.163163 |
| PADUA | 939,672 | 458,805 | 480,867 | 0.95 | 2144.15 | 438.25 | 45.8 | 22.8 | 175.8 | 3954 | 42.08 | 38.50897 |
| FERRARA | 344,840 | 166,031 | 178,809 | 0.93 | 2635.12 | 130.86 | 49.2 | 28.2 | 260.6 | 1040 | 30.16 | 9.165048 |
| VERONA | 930,339 | 456,445 | 473,894 | 0.96 | 3096.39 | 300.46 | 45.1 | 22.2 | 161.9 | 5127 | 55.11 | 24.28828 |
| PARMA | 453,930 | 222,062 | 231,868 | 0.96 | 3447.48 | 131.67 | 45.8 | 23.2 | 176.1 | 3657 | 80.56 | 10.62428 |
| FORLI’ CESENA | 394,833 | 192,398 | 202,435 | 0.95 | 2378.4 | 166.01 | 46.5 | 24.5 | 189.1 | 1740 | 44.07 | 13.88539 |
| MANTUA | 411,062 | 202,127 | 208,935 | 0.97 | 2341.44 | 175.56 | 46.2 | 23.9 | 182.3 | 3496 | 85.05 | 12.65802 |
| RAVENNA | 389,634 | 189,505 | 200,129 | 0.95 | 1859.44 | 209.54 | 47.4 | 25.5 | 205 | 1030 | 26.44 | 15.71548 |
| VENICE | 851,663 | 413,709 | 437,954 | 0.94 | 2472.91 | 344.4 | 47.1 | 24.8 | 204.5 | 2682 | 31.49 | 26.11256 |
| MODENA | 707,292 | 346,686 | 360,606 | 0.96 | 2688.02 | 263.13 | 45.5 | 23.0 | 168.6 | 3873 | 54.76 | 21.67841 |
| Timing in Chronological Order | Decisions Made by ULSS 5 |
|---|---|
| 28 January (−25 days) | Active surveillance of Chinese students returned from Chinese New Year celebrations. |
| 6 February (−15 days) | Task force with family doctors and pediatricians of free choice. |
| 21 February (0 time) | First cases of SARS-CoV-2 infection in Vo’. |
| 22 February (+1 day) | Vo’ Euganeo becomes a red zone. All those who have passed through the outbreak areas are immediately placed in isolation. Timely closure of RSAs to outsiders. Meeting and coordination with institutional bodies. Contingent distribution of PPE. |
| 24 February (+3 days) | Committee of general practitioners and pediatricians for unitary and shared coordination for management of the pandemic. |
| 25 February (+4 days) | Conference with mayors and meeting with pharmacists for unitary and shared coordination for management of the pandemic. |
| 26 February (+6 days) | Start of monitoring of older homes. |
| 2 March (+10 days) | At Trecenta hospital, a genetics laboratory is adapted into a laboratory for the analysis of nasopharyngeal swabs using molecular diagnostics. |
| 10 March (+18 days) | Reorganization of hospital withdrawal centers with booking obligation and social distancing. |
| 18 March (+26 days) | Identification of COVID-19 contact for all RSAs in the area. |
| 20 March (+27 days) | Start of Facebook streaming by the Director General to share the bulletin on the evolution of the pandemic. |
| 23 March (+30 days) | The COVID-19 laboratory of Trecenta obtains the authorization general reference laboratory to analyze swabs; the analysis capacity is supplemented by the purchase of new instruments. |
| 24 March (+31 days) | Reorganization of the COVID-19 staff at the Trecenta laboratory. |
| 1 April (+40 days) | First creation of a Public Health Plan (PSP). |
| 4 April (+42 days) | Beginning of rapid immunochromatographic serological tests on capillary blood. |
| 7 April (+46 days) | Establishment of a small working group with three representatives of the directors of RSAs, the General Manager, and the Director of Social and Health Services. |
| 4 May (+68 days) | 24 h laboratory creation for swab analysis. |
| 18 May (+82 days) | Hiring of new technicians for swab analysis in the laboratory h24. |
| 24 May (+88 days) | Building works begin for a new molecular biology laboratory with a COVID-19 area. |
| 17 June (+114 days) | ISTAT serum prevalence assessment in collaboration with the Italian Red Cross. |
| 23 June (+120 days) | Serological diagnostics on hospital operators. |
| 30 June (+127 days) | Contagion curve stable, with no new cases. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camerotto, A.; Sartorio, A.; Mazzetto, A.; Gusella, M.; Luppi, O.; Lucianò, D.; Sofritti, O.; Pelati, C.; Munno, E.; Tessari, A.; et al. Early Phase Management of the SARS-CoV-2 Pandemic in the Geographic Area of the Veneto Region, in One of the World’s Oldest Populations. Int. J. Environ. Res. Public Health 2020, 17, 9045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239045
Camerotto A, Sartorio A, Mazzetto A, Gusella M, Luppi O, Lucianò D, Sofritti O, Pelati C, Munno E, Tessari A, et al. Early Phase Management of the SARS-CoV-2 Pandemic in the Geographic Area of the Veneto Region, in One of the World’s Oldest Populations. International Journal of Environmental Research and Public Health. 2020; 17(23):9045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239045
Chicago/Turabian StyleCamerotto, Alessandro, Andrea Sartorio, Anna Mazzetto, Milena Gusella, Ornella Luppi, Domenica Lucianò, Olga Sofritti, Cristiano Pelati, Emilia Munno, Andrea Tessari, and et al. 2020. "Early Phase Management of the SARS-CoV-2 Pandemic in the Geographic Area of the Veneto Region, in One of the World’s Oldest Populations" International Journal of Environmental Research and Public Health 17, no. 23: 9045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239045