Harm Reduction Practices and Needs in a Belgian Chemsex Context: Findings from a Qualitative Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Respondent Recruitment
2.2. Procedures
2.3. Data Analysis
3. Results
3.1. Respondent Characteristics
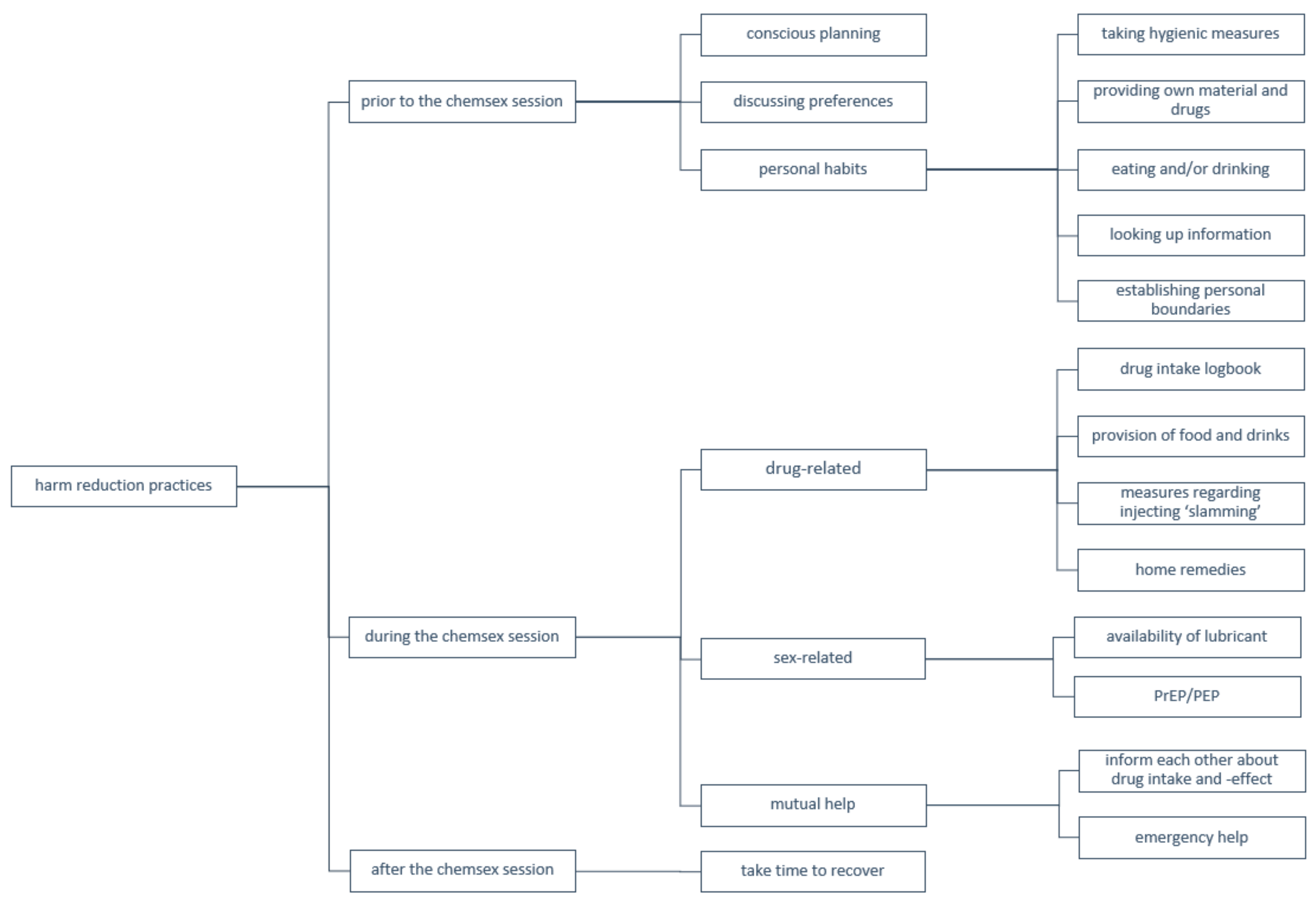
3.2. Harm Reduction Measures
3.2.1. Prior to the Chemsex Session
“From the moment I see my mate, and he says something like “Come on, we’ll put a slam tina”, then it’s like: “Okay let’s go.” And suddenly you are so horny and you start looking on Grindr, and then you’re gone for God knows how long.”(Respondent 2, 28 years old)
“I usually meet up on a Thursday night. I don’t work on Fridays, so this means that I have Friday, Saturday and Sunday to recover. My work is very important to me, and I don’t want to look like a zombie the next working day.”(Respondent 8, 45 years old)
“In small groups, it gets less out of hand. When there are more people you notice that the party gets more chaotic and unmanageable”.(Respondent 19, 48 years old)
“The first question is always: which chems do you have?”(Respondent 7, 53 years old)
“I’ve looked on the internet for certain things, I’ve done that. I don’t know which website it was, but a website with information about different drugs”.(Respondent 13, 37 years old)
3.2.2. During the Chemsex Session
Drug-Related Harm Reduction Practices
“When you suddenly say: “Shall we take another dose?” You take a look at the paper and see: “Oh it was only half an hour ago. No, not yet.” So that alone prevents so much. But also for others, when things go wrong you can just go and look: “What did he take?” That’s actually the most important thing.”(Respondent 14, 26 years old)
“When it is at our home, I always keep an eye on things. Usually the host is a bit more responsible, I guess. (…) That’s why when I go to a party somewhere else, I’m a bit more involved with the party itself.”(Respondent 13, 37 years old)
“With slamming it is important to bring your own needles. You can’t trust anyone in that regard.”(Respondent 6, 27 years old)
“Your standards fade when you take crystal meth. That’s what it does to you, blurring standards. So does GBL. It makes you push your limits, but that’s not always a good thing”.(Respondent 2, 28 years old)
“I have an occasional fist date with someone, and he actually bleeds a lot, uhm, we even have to put towels underneath. But it doesn’t bother me and it doesn’t bother him, and that’s for sure the effect of the 3-MMC. Because I swear I wouldn’t be doing that if I hadn’t taken chems”.(Respondent 9, 52 years old)
Sex-Related Harm Reduction Practices
“For STIs it’s very limited. Because first of all, you’re messing around with the condom. Also on the one hand a bit cornered by PrEP. We can’t win the jackpot anymore so, let’s go! We’ll see other STIs rise, sky high, but so be it. Those STIs are often considered as something you can get rid of easily. And, one pill or two more doesn’t matter either”.(Respondent 5, 29 years old)
Mutual Help
“What’s a pretty common thing when someone isn’t doing well, is putting him in the shower. Try to wake him up. Not too cold, not too hot water. If that doesn’t help, I always keep checking his breathing”.(Respondent 8, 45 years old)
“I always hope, if I get a little too high myself—that they’ll take care of me too. But sadly, I’m not so sure about that”.(Respondent 15, 59 years old)
“Um, the fact remains, drugs are illegal. So yeah, if it really goes wrong, calling an emergency number… that’s a very, very delicate matter”.(Respondent 14, 26 years old)
“There are a lot of people who think they know everything, but lack the right information. They claim they know it all and would even get angry if people question it”.(Respondent 3, 26 years old)
“I have to say, it’s a bit of a shame indeed. When you get into a setting like that, there’s a lot of showing off. Even though you don’t know anything, you’re not going to ask: “What’s that?” Cause then it’s like: “What are you doing here?” It’s a bit of a shame that you can’t communicate with someone like: “What chem is that? And what kind of effect does it have?””(Respondent 20, 52 years old)
3.2.3. After the Chemsex Session
“I try to sleep as much as I can. I tend to lock myself up at home at that moment. This already happened so frequently that I am beginning to know the course of things. The first day is like this, the second day like this and by the fourth day—it will take four days for me, then I’ll feel okay again”.(Respondent 4, 58 years old)
“Yes, you can’t do anything and can’t get anything done. You get so tired of it that you take something again. And then the whole thing starts over.”(Respondent 2, 28 years old)
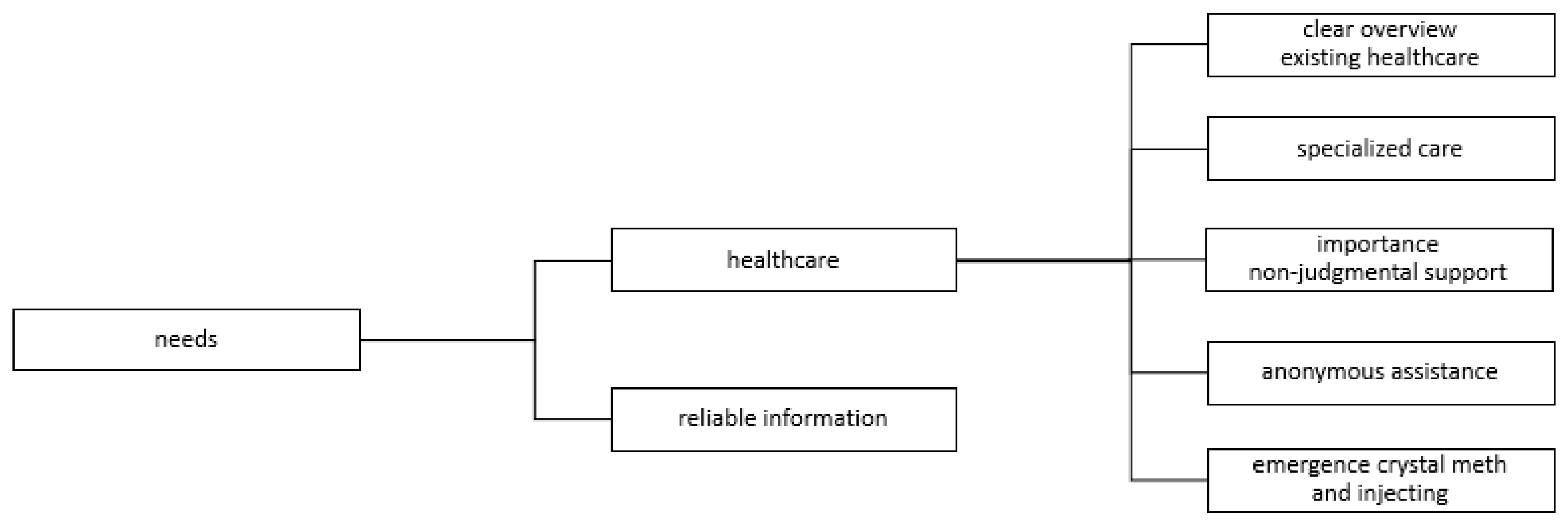
3.3. Needs of Chemsex Users
3.3.1. Reliable Information
“All you do now, if there’s something you want to know, is to Google it. But yeah (…) One says A and the other says B so, which one is true?”(Respondent 9, 52 years old)
“That when things go wrong, I think people know they should call 112, but in other light situations, there’s a lot of uncertainty and ignorance.”(Respondent 3, 26 years old)
“Above all, mixing is also an important issue. I mean, can I mix crystal meth with ketamine? But can I also use crystal meth and 3-MMC together? Can I take an XTC pill with it? Maybe two glasses of GBL, is that all right? And what about poppers? How does that relate to each other?”(Respondent 18, 28 years old)
3.3.2. Healthcare Support
“I don’t actually know because I’m here because I coincidentally told [name doctor] at the right time—I didn’t even know about the existence of certain services”.(Respondent 10, 39 years old)
“Every psychologist I ended up with had more experience in one field than another. It turned out to be very hard to find one specialized in addiction combined with sex. Uhm, yeah, I found zero good counselling”.(Respondent 4, 58 years old)
“You can only talk about it when you’re in a safe environment. At one point I had a doctor for my usual check-up and I felt that he absolutely did not agree with it. He didn’t literally say that, but I felt that he thought it was my own fault”.(Respondent 18, 28 years old)
“You never use your real name. Uhm, I also never use my personal cell phone number, but always that from work. My phone is also turned off at home. So yeah, everyone uses their own methods.”(Respondent 17, 49 years old)
“It’s getting popular really fast. So I would say; keep that in mind. Because there is no help for it. I’ve noticed it myself with my crystal meth comedown. There is no counter medication for it so you have to try to get rid of it with pure willpower. I haven’t succeeded yet.”(Respondent 6, 27 years old)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stevens, O.; Forrest, J.I. Thinking upstream: The roles of international health and drug policies in public health responses to chemsex. Sex. Health 2018, 15, 108. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, A. Sex, drugs and self-control: Why chemsex is fast becoming a public health concern. J. Fam. Plan. Reprod. Health Care 2016, 42, 291–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maxwell, S.; Shahmanesh, M.; Gafos, M. Chemsex behaviours among men who have sex with men: A systematic review of the literature. Int. J. Drug Policy 2019. [Google Scholar] [CrossRef] [PubMed]
- Bourne, A.; Reid, D.; Hickson, F.; Torres, S.; Weatherburn, R.P. The Chemsex Study: Drug Use in Sexual Settings among Gay & Bisexual Men in Lambeth, Southwark & Lewisham; Sigma Research: London, UK, 2014. [Google Scholar]
- Stuart, D. Chemsex: Origins of the word, a history of the phenomenon and a respect to the culture. Drugs Alcohol Today 2019, 19, 3–10. [Google Scholar] [CrossRef]
- Schmidt, A.J.; Bourne, A.; Weatherburn, P.; Reid, D.; Marcus, U.; Hickson, F. Illicit drug use among gay and bisexual men in 44 cities: Findings from the European MSM Internet Survey (EMIS). Int. J. Drug Policy 2016, 38, 4–12. [Google Scholar] [CrossRef]
- Stuart, D. A chemsex crucible: The context and the controversy. J. Fam. Plan. Reprod. Health Care 2016, 42, 295–296. [Google Scholar] [CrossRef] [Green Version]
- Van Acker, J. Plan. Chem? Plan. Slam? Les Plans “Sous Prod.”; Université Saint-Louis: Brussels, Belgium, 2017. [Google Scholar]
- Evers, Y.J.; Van Liere, G.A.F.S.; Hoebe, C.J.P.A.; Dukers-Muijrers, N.H.T.M. Chemsex among men who have sex with men living outside major cities and associations with sexually transmitted infections: A cross-Sectional study in the Netherlands. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Knoops, L.; Bakker, I.; Van Bodegom, R.; Zantkuijl, P. Tina En Slammen: MSM, Crystal Meth.-Gebruik En Het Injecteren van Drugs in Een Seksuele Setting; Mainline: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Kirby, T.; Thornber-Dunwell, M. Phone apps could help promote sexual health in MSM. Lancet 2014, 384, 1415. [Google Scholar] [CrossRef]
- Ahmed, A.K.; Weatherburn, P.; Reid, D.; Hickson, F.; Torres-Rueda, S.; Steinberg, P.; Bourne, A. Social norms related to combining drugs and sex (“chemsex”) among gay men in South London. Int. J. Drug Policy 2016, 38, 29–35. [Google Scholar] [CrossRef]
- Gilbart, V.L.; Simms, I.; Jenkins, C.; Furegato, M.; Gobin, M.; Oliver, I.; Hart, G.; Gill, O.N.; Hughes, G. Sex, drugs and smart phone applications: Findings from semistructured interviews with men who have sex with men diagnosed with Shigella Flexneri 3a in England and Wales. Sex. Transm. Infect. 2015, 91, 598–602. [Google Scholar] [CrossRef] [Green Version]
- Tan, R.K.J.; Wong, C.M.; Chen, M.I.C.; Chan, Y.Y.; Bin Ibrahim, M.A.; Lim, O.Z.; Chio, M.T.W.; Wong, C.S.; Chan, R.K.W.; Chua, L.J.; et al. Chemsex among gay, bisexual, and other men who have sex with men in Singapore and the challenges ahead: A qualitative study. Int. J. Drug Policy 2018. [CrossRef] [PubMed]
- Milhet, M.; Shah, J.; Madesclaire, T.; Gaissad, L. Chemsex Experiences: Narratives of Pleasure. Drugs Alcohol Today 2019, 19, 11–22. [Google Scholar] [CrossRef]
- Weatherburn, P.; Hickson, F.; Reid, D.; Torres-Rueda, S.; Bourne, A. Motivations and values associated with combining sex and illicit drugs (chemsex) among gay men in South London: Findings from a qualitative study. Sex. Transm. Infect. 2017, 93, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Nutt, D.; King, L.A.; Saulsbury, W.; Blakemore, C. Development of a rational scale to assess the harm of drugs of potential misuse. Lancet 2007, 1047–1053. [Google Scholar] [CrossRef]
- Garin, N.; Zurita, B.; Velasco, C.; Feliu, A.; Gutierrez, M.; Masip, M.; Mangues, M.A. Prevalence and clinical impact of recreational drug consumption in people living with HIV on treatment: A cross-sectional study. BMJ Open 2017, 7, 14105. [Google Scholar] [CrossRef] [Green Version]
- Sewell, J.; Cambiano, V.; Miltz, A.; Speakman, A.; Lampe, F.C.; Phillips, A.; Stuart, D.; Gilson, R.; Asboe, D.; Nwokolo, N.; et al. Changes in recreational drug use, drug use associated with chemsex, and HIV-related behaviours, among HIV-negative men who have sex with men in London and Brighton, 2013–2016. Sex. Transm. Infect. 2018, 94, 494–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakianathan, M.; Whittaker, W.; Lee, M.J.; Avery, J.; Green, S.; Nathan, B.; Hegazi, A. Chemsex and new HIV diagnosis in gay, bisexual and other men who have sex with men attending sexual health clinics. HIV Med. 2018, 19, 485–490. [Google Scholar] [CrossRef]
- Bourne, A.A.; Reid, D.; Hickson, F.; Rueda, S.T.; Weatherburn, P. The chemsex study: Executive summary. Age 2014, 13, 17. [Google Scholar]
- Smith, G.W.; Farrell, M.; Bunting, B.P.; Houston, J.E.; Shevlin, M. Patterns of polydrug use in Great Britain: Findings from a national household population survey. Drug Alcohol Depend. 2011, 113, 222–228. [Google Scholar] [CrossRef]
- Evans, E.A.; Grella, C.E.; Washington, D.L.; Upchurch, D.M. Gender and race/ethnic differences in the persistence of alcohol, drug, and poly-substance use disorders. Drug Alcohol Depend. 2017, 174, 128–136. [Google Scholar] [CrossRef]
- Lynskey, M.T.; Agrawal, A.; Bucholz, K.K.; Nelson, E.C.; Madden, P.A. Subtypes of Illicit Drug Users: A Latent Class. Analysis of Data from an Australian Twin Sample; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Romanelli, F.; Smith, K.M. Recreational use of sildenafil by HIV-positive and -negative homosexual/bisexual males. Ann. Pharmacother. 2004, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Glynn, R.W.; Byrne, N.; O’Dea, S.; Shanley, A.; Codd, M.; Keenan, E.; Ward, M.; Igoe, D.; Clarke, S. Chemsex, risk behaviours and sexually transmitted infections among men who have sex with men in Dublin, Ireland. Int. J. Drug Policy 2018, 52, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, C.; Wouters, K.; Platteau, T.; Buyze, J.; Florence, E. Increases in condomless chemsex associated with HIV acquisition in MSM but not heterosexuals attending a HIV testing center in Antwerp, Belgium. AIDS Res. Ther. 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Drückler, S.; Van Rooijen, M.S.; De Vries, H.J.C. Chemsex among men who have sex with men: A sexualized drug use survey among clients of the sexually transmitted infection outpatient clinic and users of a gay dating app in Amsterdam, the Netherlands. Sex. Transm. Dis. 2018, 45, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pufall, E.L.; Kall, M.; Shahmanesh, M.; Nardone, A.; Gilson, R.; Delpech, V.; Ward, H.; Hart, G.; Anderson, J.; Azad, Y.; et al. Sexualized drug use (‘chemsex’) and high-risk sexual behaviours in HIV-positive men who have sex with men. HIV Med. 2018, 19, 261–270. [Google Scholar] [CrossRef]
- Kohli, M.; Hickson, F.; Free, C.; Reid, D.; Weatherburn, P. Cross-sectional analysis of chemsex drug use and gonorrhoea diagnosis among men who have sex with men in the UK. Sex. Health 2019. [Google Scholar] [CrossRef]
- Prestage, G.; Hammoud, M.; Jin, F.; Degenhardt, L.; Bourne, A.; Maher, L. Mental health, drug use and sexual risk behavior among gay and bisexual men. Int. J. Drug Policy 2018, 55, 169–179. [Google Scholar] [CrossRef]
- Tomkins, A.; George, R.; Kliner, M. Sexualised drug taking among men who have sex with men: A systematic review. In Perspectives in Public Health; SAGE Publications Ltd.: Newbury Park, CA, USA, 2019; pp. 23–33. [Google Scholar] [CrossRef]
- Weatherburn, P.; Hickson, F.; Reid, D.S.; Schink, S.B.; Marcus, U.; Schmidt, A.J. The European Men-who-have-sex-with-men internet survey (EMIS): Design and methods. Sexual. Res. Soc. Policy 2013, 243–257. [Google Scholar] [CrossRef] [Green Version]
- Chemseks Een Verkennend Onderzoek in de Context van MSM & Trans.* Prostitutie/Sekswerk in Het Brussels Hoofdstedelijk Gewest En Erbuiten. Available online: https://www.academia.edu/44114653/ALIAS_vzw_2020_Verkennend_onderzoek_bij_MSM_en_trans_studenten_die_actief_zijn_in_prostitutie_sekswerk_in_het_Brussels_Hoofdstedelijk_Gewest_en_erbuiten (accessed on 29 October 2020).
- Bourne, A.; Reid, D.; Hickson, F.; Torres-Rueda, S.; Steinberg, P.; Weatherburn, P. “Chemsex” and harm reduction need among gay men in South London. Int. J. Drug Policy 2015, 26, 1171–1176. [Google Scholar] [CrossRef]
- McCall, H.; Adams, N.; Mason, D.; Willis, J.; Williw, J. What is chemsex and why does it matter? Br. Med. J. 2015, 351, h5790. [Google Scholar] [CrossRef] [Green Version]
- Platteau, T.; Herrijgers, C.; de Wit, J. Digital chemsex support and care: The potential of just-in-time adaptive interventions. Int. J. Drug Policy 2020, 85, 102927. [Google Scholar] [CrossRef] [PubMed]
- Pakianathan, M.R.; Lee, M.J.; Kelly, B.; Hegazi, A. How to assess gay, bisexual and other men who have sex with men for chemsex. Sex. Transm. Infect. 2016, 92, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Tomkins, A.; Vivancos, R.; Ward, C.; Kliner, M. How can those engaging in chemsex best be supported? An online survey to gain intelligence in greater Manchester. Int. J. STD AIDS 2018, 29, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Kirby, T.; Thornber-Dunwell, M. High-risk drug practices tighten grip on London gay scene. Lancet 2013, 381, 101–102. [Google Scholar] [CrossRef]
- Evers, Y.J.; Hoebe, C.J.P.A.; Dukers-Muijrers, N.H.T.M.; Kampman, C.J.G.; Kuizenga-Wessel, S.; Shilue, D.; Bakker, N.C.M.; Schamp, S.M.A.A.; Van Buel, H.; Van Der Meijden, W.C.J.P.M.; et al. Sexual, addiction and mental health care needs among men who have sex with men practicing chemsex—A cross-sectional study in the Netherlands. Prev. Med. Rep. 2020, 18, 101074. [Google Scholar] [CrossRef]
- Hennink, M.; Hutter, I.; Bailey, A. Qualitative Research Methods, 2nd ed.; Owens, A., Ed.; SAGE Publications: Newbury Park, CA, USA, 2020. [Google Scholar]
- Kallio, H.; Pietilä, A.M.; Johnson, M.; Kangasniemi, M. Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. J. Adv. Nurs. 2016, 2954–2965. [Google Scholar] [CrossRef]
- Schecke, H.; Lea, T.; Bohn, A.; Köhler, T.; Sander, D.; Scherbaum, N.; Deimel, D. Crystal methamphetamine use in sexual settings among German men who have sex with men. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef]
- Schmidt, A.; Weatherburn, P. European MSM Internet Survey; European Centre for Disease Prevention and Control: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Kok, G.; Gottlieb, N.H.; Peters, G.J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.C.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef]
- Peters, G.Y. A Practical guide to effective behavior change: How to identify what to change in the first place. Eur. Health Psychol. 2014, 16, 142–155. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Graf, N.; Dichtl, A.; Deimel, D.; Sander, D.; Stöver, H. Chemsex among men who have sex with men in Germany: Motives, consequences and the response of the support system. Sex. Health 2018, 15, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melendez-Torres, G.J.; Bourne, A. Illicit drug use and its association with sexual risk behaviour among MSM. Curr. Opin. Infect. Dis. 2016, 29, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Evans, K. The psychological roots of chemsex and how understanding the full picture can help us create meaningful support. Drugs Alcohol Today 2019, 19, 36–41. [Google Scholar] [CrossRef]
- Wiggins, H.; Ogaz, D.; Mebrahtu, H.; Sullivan, A.; Bowden-Jones, O.; Field, N.; Hughes, G. Demand for and availability of specialist chemsex services in the UK: A cross-sectional survey of sexual health clinics. Int. J. Drug Policy 2018, 55, 155–158. [Google Scholar] [CrossRef]
- Janghorban, R.; Roudsari, R.L.; Taghipour, A. Skype Interviewing: The New Generation of Online Synchronous Interview in Qualitative Research. Int. J. Qual. Stud. Health Well-Being 2014, 9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age | n |
| <25 years | 0 |
| 25–29 years | 6 |
| 30–39 years | 3 |
| 40–49 years | 4 |
| 50–59 years | 6 |
| ≥60 years | 1 |
| Professional Status | n |
| Employed | 14 |
| Unemployed | 4 |
| Student | 4 |
| Retired | 4 |
| Drugs Used in Previous 12 Months | n |
| XTC/MDMA | 15 |
| GHB/GBL | 13 |
| Crystal methamphetamine | 11 |
| Mephedrone | 9 |
| New psychoactive substances (NPS) | 8 |
| Cocaine | 7 |
| Ketamine | 5 |
| Injection Drug Use | n |
| Never | 12 |
| Within the last 12 months | 7 |
| >12 months ago | 1 |
| Years Active Chemsex | n |
| 1–2 years | 3 |
| 3–5 years | 8 |
| 6–10 years | 5 |
| 11–20 years | 3 |
| ≥20 years | 1 |
| Frequency Chemsex | n |
| Daily | 0 |
| More than once a week | 3 |
| Weekly | 9 |
| Monthly | 5 |
| >monthly | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrijgers, C.; Poels, K.; Vandebosch, H.; Platteau, T.; van Lankveld, J.; Florence, E. Harm Reduction Practices and Needs in a Belgian Chemsex Context: Findings from a Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 9081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239081
Herrijgers C, Poels K, Vandebosch H, Platteau T, van Lankveld J, Florence E. Harm Reduction Practices and Needs in a Belgian Chemsex Context: Findings from a Qualitative Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239081
Chicago/Turabian StyleHerrijgers, Corinne, Karolien Poels, Heidi Vandebosch, Tom Platteau, Jacques van Lankveld, and Eric Florence. 2020. "Harm Reduction Practices and Needs in a Belgian Chemsex Context: Findings from a Qualitative Study" International Journal of Environmental Research and Public Health 17, no. 23: 9081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239081