Prevalence and Associated Factors of Fecal Incontinence and Double Incontinence among Rural Elderly in North China



Abstract
:1. Introduction
2. Methods
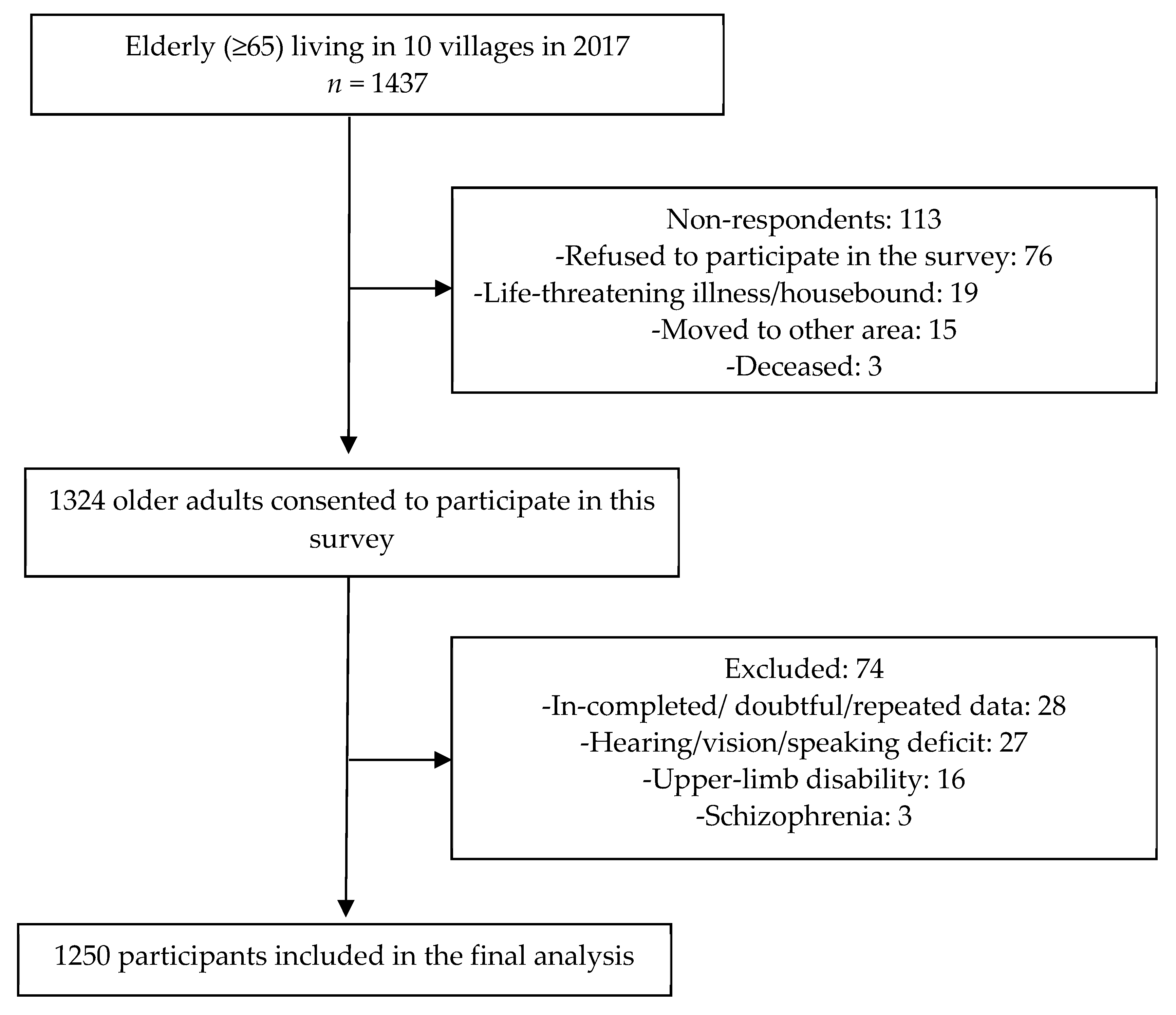
2.1. Study Design and Population
2.2. Study Procedures
2.3. Instruments
2.3.1. Assessment of FI
2.3.2. Assessment of DI
2.3.3. Associated Factors of FI and DI
Socio-Demographic Assessments
Health-Related Factors
2.4. Data Analysis
3. Results
3.1. Basic Characteristic of Participants
3.2. Prevalence of FI and DI
3.3. Associated Factors of FI and DI
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- 6th International Consultation on incontinence. Incontinence 6th Edition. Available online: https://www.ics.org/members/shop/incontinence6thedition (accessed on 9 August 2019).
- Sharma, A.; Yuan, L.; Marshall, R.J.; Merrie, A.E.; Bissett, I.P. Systematic review of the prevalence of faecal incontinence. Br. J. Surg. 2016, 103, 1589–1597. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.S.; Sivakumaran, Y.; Nassar, N.; Gladman, M.A. Fecal Incontinence: Community Prevalence and Associated Factors—A Systematic Review. Dis. Colon Rectum 2015, 58, 1194–1209. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.M.; Matthews, C.A.; Vaughan, C.P.; Markland, A.D. Urinary, fecal, and dual incontinence in older U.S. Adults. J. Am. Geriatr. Soc. 2015, 63, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.A.; Whitehead, W.E.; Townsend, M.K.; Grodstein, F. Risk factors for urinary, fecal, or dual incontinence in the Nurses’ Health Study. Obstet. Gynecol. 2013, 122, 539–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slieker-ten Hove, M.C.; Pool-Goudzwaard, A.L.; Eijkemans, M.J.; Steegers-Theunissen, R.P.; Burger, C.W.; Vierhout, M.E. Prevalence of double incontinence, risks and influence on quality of life in a general female population. Neurourol. Urodyn. 2010, 29, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Markland, A.D.; Goode, P.S.; Burgio, K.L.; Redden, D.T.; Richter, H.E.; Sawyer, P.; Allman, R.M. Correlates of urinary, fecal, and dual incontinence in older African-American and white men and women. J. Am. Geriatr. Soc. 2008, 56, 285–290. [Google Scholar] [CrossRef]
- Teunissen, T.A.; van den Bosch, W.J.; van den Hoogen, H.J.; Lagro-Janssen, A.L. Prevalence of urinary, fecal and double incontinence in the elderly living at home. Int. Urogynecology J. Pelvic Floor Dysfunct. 2004, 15, 10–13; discussion 13. [Google Scholar] [CrossRef]
- Brown, H.W.; Guan, W.; Schmuhl, N.B.; Smith, P.D.; Whitehead, W.E.; Rogers, R.G. If We Don’t Ask, They Won’t Tell: Screening for Urinary and Fecal Incontinence by Primary Care Providers. J. Am. Board Fam. Med. JABFM 2018, 31, 774–782. [Google Scholar] [CrossRef]
- Saga, S.; Vinsnes, A.G.; Mørkved, S.; Norton, C.; Seim, A. What characteristics predispose to continence in nursing home residents?: A population-based cross-sectional study. Neurourol. Urodyn. 2015, 34, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Sievert, K.D.; Amend, B.; Toomey, P.A.; Robinson, D.; Milsom, I.; Koelbl, H.; Abrams, P.; Cardozo, L.; Wein, A.; Smith, A.L.; et al. Can we prevent incontinence? ICI-RS 2011. Neurourol. Urodyn. 2012, 31, 390–399. [Google Scholar] [CrossRef]
- Bliss, D.Z.; Gurvich, O.V.; Eberly, L.E.; Savik, K.; Harms, S.; Wyman, J.F.; Mueller, C.; Virnig, B.; Wiltzen, K. Racial disparities in primary prevention of incontinence among older adults at nursing home admission. Neurourol. Urodyn. 2017, 36, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Ricks, M. Nursing Older People at a Glance, first edition. Int. J. Orthop. Trauma Nurs. 2019, 33, 55. [Google Scholar] [CrossRef]
- Islam, R.M.; Oldroyd, J.; Rana, J.; Romero, L.; Karim, M.N. Prevalence of symptomatic pelvic floor disorders in community-dwelling women in low and middle-income countries: A systematic review and meta-analysis. Int. Urogynecology J. 2019, 30, 2001–2011. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Wang, L.; Huang, S.S.; Wu, Q.; Wu, D.L. Prevalence and risk factors of urinary incontinence among Chinese women in Shanghai. Int. J. Clin. Exp. Med. 2014, 7, 686–696. [Google Scholar] [PubMed]
- Ge, J.; Yang, P.; Zhang, Y.; Li, X.; Wang, Q.; Lu, Y. Prevalence and risk factors of urinary incontinence in Chinese women: A population-based study. Asia-Pac. J. Public Health 2015, 27, NP1118–NP1131. [Google Scholar] [CrossRef] [PubMed]
- Walker, G.J.; Gunasekera, P. Pelvic organ prolapse and incontinence in developing countries: Review of prevalence and risk factors. Int. Urogynecol. J. 2011, 22, 127–135. [Google Scholar] [CrossRef]
- Yuan, Y.; Qiu, L.; Li, Z.Y.; Zhang, L.; Xu, T.; Lang, J.H.; Li, Z.A.; Gong, J.; Liu, Q.; Liu, X.C.; et al. An epidemiology study of fecal incontinence in adult Chinese women living in urban areas. Chin. Med. J. 2020, 133, 262–268. [Google Scholar] [CrossRef]
- Sze, E.H.; Barker, C.D.; Hobbs, G. A cross-sectional survey of the relationship between fecal incontinence and constipation. Int. Urogynecol. J. 2013, 24, 61–65. [Google Scholar] [CrossRef]
- Zhang, X.; Dupre, M.E.; Qiu, L.; Zhou, W.; Zhao, Y.; Gu, D. Urban-rural differences in the association between access to healthcare and health outcomes among older adults in China. BMC Geriatr. 2017, 17, 151. [Google Scholar] [CrossRef]
- Heward, J.; Stone, L.; Paddick, S.M.; Mkenda, S.; Gray, W.K.; Dotchin, C.L.; Kissima, J.; Collingwood, C.; Swai, B.; Walker, R.W. A longitudinal study of cognitive decline in rural Tanzania: Rates and potentially modifiable risk factors. Int. Psychogeriatr. 2018, 30, 1333–1343. [Google Scholar] [CrossRef]
- Feng, Z.; Zhan, H.J.; Feng, X.; Liu, C.; Sun, M.; Mor, V. An industry in the making: The emergence of institutional elder care in urban china. J. Am. Geriatr. Soc. 2011, 59, 738–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Z.; Liu, Q.; Meng, H.; Liu, D.; Dobbs, D.; Hyer, K.; Conner, K.O. Factors associated with willingness to enter long-term care facilities among older adults in Chengdu, China. PLoS ONE 2018, 13, e0202225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norton, C.; Whitehead, W.E.; Bliss, D.Z.; Harari, D.; Lang, J. Management of fecal incontinence in adults. Neurourol. Urodyn. 2010, 29, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Ditah, I.; Devaki, P.; Luma, H.N.; Ditah, C.; Njei, B.; Jaiyeoba, C.; Salami, A.; Ditah, C.; Ewelukwa, O.; Szarka, L. Prevalence, trends, and risk factors for fecal incontinence in United States adults, 2005-2010. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2014, 12, 636–643.e2. [Google Scholar] [CrossRef]
- Avery, K.; Donovan, J.; Peters, T.J.; Shaw, C.; Gotoh, M.; Abrams, P. ICIQ: A brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol. Urodyn. 2004, 23, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Xie, Y.N. Reliability and validity of the simplified coping style questionnaire [in Chinese]. Chin. J. Clin. Psychol. 1998, 6, 114–115. [Google Scholar]
- Wu, J.; Liu, J.; Qin, J.; Lan, C.; Yang, H.; Yang, L. Mental Health Status and Coping Behaviors of the Guangxi Baiku Yao Population in Response to Life Events. Med Sci. Monit. 2017, 23, 580–587. [Google Scholar] [CrossRef]
- Lawton, M.P.; Bro0dy, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Chen, Y.; Yin, Z.; Xie, Q. Suggestions to ameliorate the inequity in urban/rural allocation of healthcare resources in China. Int. J. Equity Health 2014, 13, 34. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, W.E.; Borrud, L.; Goode, P.S.; Meikle, S.; Mueller, E.R.; Tuteja, A.; Weidner, A.; Weinstein, M.; Ye, W. Fecal incontinence in US adults: Epidemiology and risk factors. Gastroenterology 2009, 137, 512–517.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, C.R.; Santos, V.L. Prevalence of self-reported double incontinence in the urban population of a Brazilian city. Neurourol. Urodyn. 2011, 30, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Coppola, L.; Caserta, F.; Grassia, A.; Mastrolorenzo, L.; Altrui, L.; Tondi, G.; Verde, S.; Coppola, A. Urinary incontinence in the elderly: Relation to cognitive and motor function. Arch. Gerontol. Geriatr. 2002, 35, 27–34. [Google Scholar] [CrossRef]
- Omli, R.; Hunskaar, S.; Mykletun, A.; Romild, U.; Kuhry, E. Urinary incontinence and risk of functional decline in older women: Data from the Norwegian HUNT-study. BMC Geriatr. 2013, 13, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, J.J.; Liu, S.P.; Lin, H.C. Traumatic brain injury increases the risk of female urinary incontinence. Neurourol. Urodyn. 2013, 32, 354–358. [Google Scholar] [CrossRef]
- Foxx-Orenstein, A.; Kolakowsky-Hayner, S.; Marwitz, J.H.; Cifu, D.X.; Dunbar, A.; Englander, J.; Francisco, G. Incidence, risk factors, and outcomes of fecal incontinence after acute brain injury: Findings from the Traumatic Brain Injury Model Systems national database. Arch. Phys. Med. Rehabil. 2003, 84, 231–237. [Google Scholar] [CrossRef]
- Nakanishi, N.; Tatara, K.; Naramura, H.; Fujiwara, H.; Takashima, Y.; Fukuda, H. Urinary and fecal incontinence in a community-residing older population in Japan. J. Am. Geriatr. Soc. 1997, 45, 215–219. [Google Scholar] [CrossRef]
- Kuoch, K.L.; Hebbard, G.S.; O’Connell, H.E.; Austin, D.W.; Knowles, S.R. Urinary and faecal incontinence: Psychological factors and management recommendations. N.Z. Med. J. 2019, 132, 25–33. [Google Scholar]
- Yip, S.O.; Dick, M.A.; McPencow, A.M.; Martin, D.K.; Ciarleglio, M.M.; Erekson, E.A. The association between urinary and fecal incontinence and social isolation in older women. Am. J. Obstet. Gynecol. 2013, 208, 146.e1–146.e7. [Google Scholar] [CrossRef] [Green Version]
- Ruella, Y.; Saint-Onge, K.; Fraser, S.; Southall, K.; Frechette-Chaine, E.; Morin, M.; Dumoulin, C. Peer support: Does it hold the key to decreasing self-stigma and improving self-management in older women with urinary incontinence? Neurourol. Urodyn. 2017, 36, S384–S385. [Google Scholar]
- Botlero, R.; Bell, R.J.; Urquhart, D.M.; Davis, S.R. Prevalence of fecal incontinence and its relationship with urinary incontinence in women living in the community. Menopause 2011, 18, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Stenzelius, K.; Mattiasson, A.; Hallberg, I.R.; Westergren, A. Symptoms of urinary and faecal incontinence among men and women 75+ in relations to health complaints and quality of life. Neurourol. Urodyn. 2004, 23, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Yuaso, D.R.; Santos, J.L.F.; Castro, R.A.; Duarte, Y.A.O.; Girão, M.; Berghmans, B.; Tamanini, J.T.N. Female double incontinence: Prevalence, incidence, and risk factors from the SABE (Health, Wellbeing and Aging) study. Int. Urogynecol. J. 2018, 29, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; McMunn, A.; Demakakos, P.; Hamer, M.; Steptoe, A. Social isolation and loneliness: Prospective associations with functional status in older adults. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2017, 36, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Erekson, E.A.; Ciarleglio, M.M.; Hanissian, P.D.; Strohbehn, K.; Bynum, J.P.; Fried, T.R. Functional disability and compromised mobility among older women with urinary incontinence. Female Pelvic Med. Reconstr. Surg. 2015, 21, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Hirayama, F.; Lee, A.H. Green tea drinking is inversely associated with urinary incontinence in middle-aged and older women. Neurourol. Urodyn. 2011, 30, 1262–1265. [Google Scholar] [CrossRef]
- Tettamanti, G.; Altman, D.; Pedersen, N.L.; Bellocco, R.; Milsom, I.; Iliadou, A.N. Effects of coffee and tea consumption on urinary incontinence in female twins. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Jeong, B.C.; Kim, B.S.; Kim, J.I.; Kim, H.H. Effects of green tea on urinary stone formation: An in vivo and in vitro study. J. Endourol. 2006, 20, 356–361. [Google Scholar] [CrossRef]
- Renno, W.M.; Abdeen, S.; Alkhalaf, M.; Asfar, S. Effect of green tea on kidney tubules of diabetic rats. Br. J. Nutr. 2008, 100, 652–659. [Google Scholar] [CrossRef]
- Ryan, L.; Petit, S. Addition of whole, semiskimmed, and skimmed bovine milk reduces the total antioxidant capacity of black tea. Nutr. Res. 2010, 30, 14–20. [Google Scholar] [CrossRef]
- Yeoh, E.K.; Wong, M.C.S.; Wong, E.L.Y.; Yam, C.; Poon, C.M.; Chung, R.Y.; Chong, M.; Fang, Y.; Wang, H.H.X.; Liang, M.; et al. Benefits and limitations of implementing Chronic Care Model (CCM) in primary care programs: A systematic review. Int. J. Cardiol. 2018, 258, 279–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, W.W.; Ross, J.S.; Boockvar, K.S.; Siu, A.L. Recent trends in chronic disease, impairment and disability among older adults in the United States. BMC Geriatr. 2011, 11, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerez-Roig, J.; Souza, D.L.; Amaral, F.L.; Lima, K.C. Prevalence of fecal incontinence (FI) and associated factors in institutionalized older adults. Arch. Gerontol. Geriatr. 2015, 60, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.J.; Brown, J.S.; Thom, D.H.; Fink, H.A.; Yaffe, K. Urinary incontinence in older community-dwelling women: The role of cognitive and physical function decline. Obstet. Gynecol. 2007, 109, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Schumpf, L.F.; Theill, N.; Scheiner, D.A.; Fink, D.; Riese, F.; Betschart, C. Urinary incontinence and its association with functional physical and cognitive health among female nursing home residents in Switzerland. BMC Geriatr. 2017, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Drennan, V.M.; Rait, G.; Cole, L.; Grant, R.; Iliffe, S. The prevalence of incontinence in people with cognitive impairment or dementia living at home: A systematic review. Neurourol. Urodyn. 2013, 32, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment--beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Drennan, V.M.; Greenwood, N.; Cole, L.; Fader, M.; Grant, R.; Rait, G.; Iliffe, S. Conservative interventions for incontinence in people with dementia or cognitive impairment, living at home: A systematic review. BMC Geriatr. 2012, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Zhang, W.; Gu, L.; Qu, Z.; Sa, Z.; Zhang, X.; Tian, D. Aging village doctors in five counties in rural China: Situation and implications. Hum. Resour. Health 2014, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Vinsnes, A.G.; Harkless, G.E.; Haltbakk, J.; Bohm, J.; Hunskaar, S. Healthcare personnel’s attitudes towards patients with urinary incontinence. J. Clin. Nurs. 2001, 10, 455–462. [Google Scholar] [CrossRef]
- Saxer, S.; de Bie, R.A.; Dassen, T.; Halfens, R.J. Nurses’ knowledge and practice about urinary incontinence in nursing home care. Nurse Educ. Today 2008, 28, 926–934. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total N (%) | FI | DI | |||||
|---|---|---|---|---|---|---|---|---|
| No FI N (%) | FI N (%) | p Value | No DI N (%) | DI N (%) | p Value | |||
| Participants | 1250 (100.0) | 1096 (87.7) | 154 (12.3) | - | 1134 (90.7) | 116 (9.3) | - | |
| Demographics | ||||||||
| Sex | Male | 550 (44.0) | 485 (44.3) | 65 (42.2) | 0.632 | 507 (44.7) | 43 (37.1) | 0.114 |
| Female | 700 (56.0) | 611 (55.7) | 89 (57.8) | 627 (55.3) | 73 (62.9) | |||
| Age (years) | 65~69 | 433 (34.6) | 386 (35.2) | 47 (30.5) | 0.077 | 401 (35.4) | 32 (27.6) | 0.011 |
| 70~74 | 393 (31.4) | 346 (31.6) | 47 (30.5) | 354 (31.2) | 39 (33.6) | |||
| 75~79 | 261 (20.9) | 217 (19.8) | 44 (28.6) | 225 (19.8) | 36 (31.0) | |||
| 80~ | 163 (13.0) | 147 (13.4) | 16 (10.4) | 154 (13.6) | 9 (7.8) | |||
| Education | Illiteracy | 135 (10.8) | 121 (11.0) | 14 (9.1) | 0.203 | 125 (11.0) | 10 (8.6) | 0.209 |
| Primary school | 614 (49.1) | 528 (48.2) | 86 (55.8) | 548 (48.3) | 66 (56.9) | |||
| ≥Secondary school | 501(40.1) | 447 (40.8) | 54 (35.1) | 461 (40.7) | 40 (34.5) | |||
| Marital status | Married | 861 (68.9) | 752 (68.6) | 109 (70.8) | 0.587 | 778 (68.6) | 83 (71.6) | 0.514 |
| Divorced/Widowed | 389 (31.1) | 344 (31.4) | 45 (29.2) | 356 (31.4) | 33 (28.4) | |||
| Income | Subsidies ※ | 631 (50.5) | 540 (49.3) | 91 (59.1) | 0.002 | 565 (49.8) | 66 (56.9) | 0.003 |
| Poverty | 260 (20.8) | 223 (20.3) | 37 (24.0) | 228 (20.1) | 32 (27.6) | |||
| Nonpoverty | 359 (28.7) | 333 (30.4) | 26 (16.9) | 341 (30.1) | 18 (15.5) | |||
| Medical expenses | <Average | 814 (65.1) | 728 (66.4) | 86 (55.8) | 0.010 | 751 (66.2) | 63 (54.3) | 0.010 |
| ≥Average | 436 (34.9) | 368 (33.6) | 68 (44.2) | 383 (33.8) | 53 (45.7) | |||
| Lifestyle | ||||||||
| Regular house/farm work | 886 (70.9) | 791 (72.2) | 95 (61.7) | 0.007 | 813 (71.7) | 73 (62.9) | 0.048 | |
| Smoking | 244 (19.6) | 218 (19.9) | 26 (17.2) | 0.435 | 227 (20.1) | 17 (14.9) | 0.187 | |
| Alcohol consumption | Never | 1106 (88.8) | 969 (88.5) | 137 (90.7) | 0.508 | 1000 (88.3) | 106 (93.0) | 0.208 |
| Sometimes | 95 (7.6) | 87 (7.9) | 8 (5.3) | 91 (8.0) | 4 (3.5) | |||
| Often | 45 (3.6) | 39 (3.6) | 6 (4.0) | 41 (3.6) | 4 (3.5) | |||
| Tea consumption | 205 (16.4) | 188 (17.2) | 17 (11.0) | 0.055 | 197 (17.4) | 8 (6.9) | 0.004 | |
| Psychosocial factors | ||||||||
| Living alone | 139 (11.1) | 125 (11.4) | 14 (9.1) | 0.392 | 129 (11.4) | 10 (8.6) | 0.369 | |
| Sleep quality | Good | 791 (63.3) | 707 (64.5) | 84 (54.5) | 0.041 | 733 (64.6) | 58 (50.0) | 0.005 |
| Moderate | 306 (24.5) | 262 (23.9) | 44 (28.6) | 270 (23.8) | 36 (31.0) | |||
| Poor | 153 (12.2) | 127 (11.6) | 26 (16.9) | 131 (11.6) | 22 (19.0) | |||
| Social interaction in neighborhood | Good | 411 (32.9) | 390 (35.6) | 21 (13.6) | <0.001 | 392 (34.6) | 19 (16.4) | <0.001 |
| Satisfactory | 804 (64.3) | 676 (61.7) | 128 (83.1) | 709 (62.5) | 95 (81.9) | |||
| Poor | 35 (2.8) | 30 (2.7) | 5 (3.2) | 33 (2.9) | 2 (1.7) | |||
| Memory complaint | 1034 (82.7) | 893 (81.5) | 141 (91.6) | 0.002 | 925 (81.6) | 109 (94.0) | 0.001 | |
| Coping | Negative | 125 (10.0) | 104 (9.5) | 21 (13.6) | 0.108 | 109 (9.6) | 16 (13.8) | 0.153 |
| Positive | 1125 (90.0) | 992 (90.5) | 133 (86.4) | 1025 (90.4) | 100 (86.2) | |||
| Characteristics | Total N (%) | FI | DI | |||||
|---|---|---|---|---|---|---|---|---|
| No FI N (%) | FI N (%) | p Value | No DI N (%) | DI N (%) | p Value | |||
| BMI (kg/m2) | Underweight | 90 (7.2) | 75 (6.8) | 15 (9.7) | 0.427 | 78 (6.9) | 12 (10.3) | 0.388 |
| Normal | 605 (48.4) | 533 (48.6) | 72 (46.8) | 551 (48.6) | 54 (46.6) | |||
| Overweight | 555 (44.4) | 488 (44.5) | 67 (43.5) | 505 (44.5) | 50 (43.1) | |||
| Waist circumference (cm) | Normal | 509 (40.7) | 446 (40.7) | 63 (40.9) | 0.959 | 459 (40.5) | 50 (43.1) | 0.583 |
| High | 741 (59.3) | 650 (59.3) | 91 (59.1) | 675 (59.5) | 66 (56.9) | |||
| Hearing | Good | 351 (28.1) | 323 (29.5) | 28 (18.2) | 0.003 | 332 (29.3) | 19 (16.4) | 0.003 |
| Moderate | 505 (40.4) | 443 (40.4) | 62 (40.3) | 458 (40.4) | 47 (40.5) | |||
| Poor | 394 (31.5) | 330 (30.1) | 64 (41.6) | 344 (30.3) | 50 (43.1) | |||
| Weak Vision | 105 (8.4) | 89 (8.1) | 16 (10.4) | 0.342 | 91 (8.0) | 14 (12.1) | 0.135 | |
| Chronic disease | 0 | 290 (23.2) | 259 (23.6) | 31 (20.1) | 0.005 | 266 (23.5) | 24 (20.7) | 0.071 |
| 1 | 464 (37.1) | 422 (38.5) | 42 (27.3) | 431 (38.0) | 33 (28.4) | |||
| 2 | 318 (25.4) | 268 (24.5) | 50 (32.5) | 281 (24.8) | 37 (31.9) | |||
| ≥3 | 178 (14.2) | 147 (13.4) | 31 (20.1) | 156 (13.8) | 22 (19.0) | |||
| Hypertension | 613 (49.0) | 527 (48.1) | 86 (55.8) | 0.071 | 554 (48.9) | 59 (50.9) | 0.680 | |
| Diabetes | 105 (8.4) | 91 (8.3) | 14 (9.1) | 0.741 | 95 (8.4) | 10 (8.6) | 0.928 | |
| Cerebrovascular disease | 94 (7.5) | 68 (6.2) | 26 (16.9) | <0.001 | 74 (6.5) | 20 (17.2) | <0.001 | |
| Heart disease | 327 (26.2) | 284 (25.9) | 43 (27.9) | 0.595 | 291 (25.7) | 36 (31.0) | 0.210 | |
| Hyperlipidemia | 140 (11.2) | 125 (11.4) | 15 (9.7) | 0.540 | 129 (11.4) | 11 (9.5) | 0.538 | |
| Traumatic brain injury | 97 (7.8) | 66 (6.0) | 31 (20.1) | <0.001 | 74 (6.5) | 23 (19.8) | <0.001 | |
| Chronic constipation | 385 (30.8) | 333 (30.4) | 52 (33.8) | 0.395 | 342 (30.2) | 43 (37.1) | 0.125 | |
| Urinary incontinence | 582 (46.6) | 466 (42.5) | 116 (75.3) | <0.001 | - | - | - | |
| ADL dependence | 89 (7.1) | 70 (6.4) | 19 (12.3) | 0.007 | 73(6.4) | 16 (13.8) | 0.003 | |
| Physical ADL dependence | 705 (56.4) | 588 (53.6) | 117 (76.0) | <0.001 | 598 (52.7) | 107 (92.2) | <0.001 | |
| IADL dependence | 409 (32.7) | 351 (32.0) | 58 (37.7) | 0.168 | 364 (32.1) | 45(38.8) | 0.143 | |
| Cognitive impairment | 536 (42.9) | 463 (42.2) | 73 (47.4) | 0.226 | 476 (42.0) | 60 (51.7) | 0.043 | |
| Characteristics | FI | DI | |||
|---|---|---|---|---|---|
| Prevalence (95%CI) | OR (95%CI) | Prevalence (95%CI) | OR (95%CI) | ||
| Total | 12.3 (10.5, 14.0) | 9.3 (7.7, 10.9) | |||
| Sex | Male (ref.) | 11.8 (9.1, 14.5) | 7.8 (5.6, 10.0) | ||
| Female | 12.7 (10.2, 15.2) | 1.09 (0.77–1.53) | 10.4 (8.0, 12.8) | 1.37 (0.93–2.04) | |
| Age (years) | 65~69 (ref.) | 10.9 (8.0, 13.8) | 7.4 (4.9, 9.9) | ||
| 70~74 | 12 (8.9, 15.1) | 1.12 (0.73–1.71) | 9.9 (7.0, 12.8) | 1.38 (0.85–2.25) | |
| 75~79 | 16.9 (12.4, 21.4) | 1.67 (1.07–2.60) | 13.8 (9.7, 17.9) | 2.01 (1.21–3.32) | |
| 80~ | 9.8 (5.3, 14.3) | 0.89 (0.49–1.63) | 5.5 (2.0, 9.0) | 0.73 (0.34–1.57) | |
| Education | Illiteracy (ref.) | 10.4 (5.3, 15.5) | 7.4 (2.9, 11.9) | ||
| Primary school | 14 (11.3, 16.7) | 1.41 (0.77–2.56) | 10.7 (8.3, 13.1) | 1.51 (0.75–3.01) | |
| ≥Secondary school | 10.8 (8.1, 13.5) | 1.04 (0.56–1.94) | 8 (5.6, 10.4) | 1.09 (0.53–2.23) | |
| Marital status | Married (ref.) | 11.6 (8.5, 14.7) | 9.6 (7.6, 11.6) | ||
| Divorced/Widowed | 12.3 (10.5, 14.1) | 0.90 (0.62–1.31) | 8.5 (5.8, 11.2) | 0.87 (0.57–1.33) | |
| Income | Subsidies (ref.) ※ | 14.4 (11.7, 17.1) | 10.5 (8.1, 12.9) | ||
| Poverty | 14.2 (9.9, 18.5) | 0.99 (0.65–1.49) | 12.3 (8.4, 16.2) | 1.20 (0.76–1.88) | |
| Nonpoverty | 7.2 (4.5, 9.9) | 0.46 (0.29–0.73) | 5 (2.6, 7.4) | 0.45 (0.26–0.77) | |
| Medical expenses | <Average (ref.) | 10.6 (8.4, 12.8) | 7.7 (5.9, 9.5) | ||
| ≥Average | 15.6 (12.3, 18.9) | 1.56 (1.11–2.20) | 12.2 (9.1, 15.3) | 1.65 (1.12–2.43) | |
| Regular house/farm work | No (ref.) | 16.2 (12.5, 19.9) | 11.8 (8.5, 15.1) | ||
| Yes | 10.7 (8.7, 12.7) | 0.62 (0.44–0.88) | 8.2 (6.4, 10.0) | 0.67 (0.45–0.99) | |
| Smoking | No (ref.) | 12.5 (10.5, 14.5) | 9.7 (7.9, 11.5) | ||
| Yes | 10.7 (6.8, 14.6) | 0.84 (0.54–1.31) | 7 (3.9, 10.1) | 0.70 (0.41–1.19) | |
| Alcohol consumption | Neve r(ref.) | 12.4 (10.4, 14.4) | 9.6 (7.8, 11.4) | ||
| Sometimes | 8.4 (2.9, 13.9) | 0.65 (0.31–1.37) | 4.2 (0.1, 8.3) | 0.42 (0.15–1.15) | |
| Often | 13.3 (3.3, 23.3) | 1.09 (0.45–2.62) | 8.9 (0.7, 17.1) | 0.92 (0.32–2.62) | |
| Tea consumption | No (ref.) | 13.1 (11.1, 15.1) | 10.3 (8.5, 12.1) | ||
| Yes | 8.3 (4.6, 12.0) | 0.60 (0.35–1.02) | 3.9 (1.2, 6.6) | 0.35 (0.17–0.73) | |
| Living alone | No (ref.) | 12.6 (10.6, 14.6) | 9.5 (7.7, 11.3) | ||
| Yes | 10.1 (5.0, 15.2) | 1.29 (0.72–2.30) | 7.2 (2.9, 11.5) | 1.36 (0.69–2.67) | |
| Sleep quality | Good (ref.) | 10.6 (8.4, 12.8) | 7. 3 (5.5, 9.1) | ||
| Moderate | 14.4 (10.5, 18.3) | 1.41 (0.96–2.09) | 11.8 (8.3, 15.3) | 1.69 (1.09–2.61) | |
| Poor | 17 (11.1, 22.9) | 1.72 (1.07–2.78) | 14.4 (8.9, 19.9) | 2.12 (1.26–3.59) | |
| Social interaction in neighborhood | Good (ref.) | 5.1 (2.9, 7.3) | 4.6 (2.6, 6.6) | ||
| Satisfactory | 15.9 (13.4, 18.4) | 3.52 (2.18–5.67) | 11.8 (9.6, 14.0) | 2.76 (1.66–4.59) | |
| Poor | 14.3 (2.7, 25.9) | 3.10 (1.09–8.79) | 5.7 (0.0, 13.3) | 1.25 (0.28–5.60) | |
| Memory complaint | No (ref.) | 6 (2.9, 9.1) | 3.2 (0.8, 5.6) | ||
| Yes | 13.6 (11.4, 15.8) | 2.47 (1.37–4.44) | 10.5 (8.5, 12.5) | 3.52 (1.62–7.67) | |
| Coping | Negative (ref.) | 16.8 (10.3, 23.3) | 12.8 (6.9, 18.7) | ||
| Positive | 11.8 (9.8, 13.8) | 0.66 (0.40–1.10) | 8.9 (7.3, 10.5) | 0.67 (0.38–1.17) | |
| Characteristics | FI | DI | |||
|---|---|---|---|---|---|
| Prevalence (95%CI) | OR (95%CI) | Prevalence (95%CI) | OR (95%CI) | ||
| BMI (kg/m2) | Underweight (ref.) | 12.3 (10.5, 14.1) | 13.3 (6.2, 20.4) | ||
| Normal | 16.7 (9.1, 24.3) | 0.68 (0.37–1.24) | 8.9 (6.5, 11.3) | 0.64 (0.33–1.24) | |
| Overweight | 11.9 (9.4, 14.4) | 0.69 (0.37–1.26) | 9 (6.6, 11.4) | 0.64 (0.33–1.26) | |
| Waist circumference (cm) | Normal (ref.) | 12.4 (9.5, 15.3) | 9.3 (7.7, 10.9) | ||
| High | 12.3 (9.9, 14.7) | 0.99 (0.70–1.40) | 9.8 (7.3, 12.3) | 0.90 (0.61–1.32) | |
| Hearing | Good (ref.) | 8 (5.3, 10.7) | 5.4 (3.0, 7.8) | ||
| Moderate | 12.3 (9.4, 15.2) | 1.61 (1.01–2.58) | 9.3 (6.8, 11.8) | 1.79 (1.03–3.11) | |
| Poor | 16.2 (12.5, 19.9) | 2.24 (1.4–3.58) | 12.7 (9.4, 16.0) | 2.54 (1.47–4.40) | |
| Vision | Normal | 12.1 (10.1, 14.1) | 8.9 (7.3, 10.5) | ||
| Weak | 15.2 (8.3, 22.1) | 1.31 (0.75–2.30) | 13.3 (6.8, 19.8) | 1.57 (0.87–2.86) | |
| Chronic disease | 0 (ref.) | 10.7 (7.2, 14.2) | 8.3 (5.2, 11.4) | ||
| 1 | 9.1 (6.6, 11.6) | 0.83 (0.51–1.36) | 7.1 (4.7, 9.5) | 0.85 (0.49–1.47) | |
| 2 | 15.7 (11.8, 19.6) | 1.56 (0.97–2.52) | 11.6 (8.1, 15.1) | 1.46 (0.85–2.51) | |
| ≥3 | 17.4 (11.9, 22.9) | 1.76 (1.03–3.02) | 12.4 (7.5, 17.3) | 1.56 (0.85–2.88) | |
| Hypertension | No (ref.) | 10.7 (8.3, 13.1) | 8.9 (6.7, 11.1) | ||
| Yes | 14 (11.3, 16.7) | 1.37 (0.97–1.92) | 9.6 (7.2, 12.0) | 1.08 (0.74–1.59) | |
| Diabetes | No (ref.) | 12.2 (10.2, 14.2) | 9.3 (7.5, 11.1) | ||
| Yes | 13.3 (6.8, 19.8) | 1.10 (0.61–1.99) | 9.5(3.8, 15.2) | 1.03 (0.52–2.04) | |
| Cerebrovascular disease | No (ref.) | 11.1 (9.3, 12.9) | 8.3 (6.7, 9.9) | ||
| Yes | 27.7 (18.7, 36.7) | 3.07 (1.89–5.00) | 21.3 (13.1, 29.5) | 2.98 (1.75–5.10) | |
| Heart disease | No (ref.) | 12 (9.8, 14.2) | 8.7 (6.9, 10.5) | ||
| Yes | 13.1 (9.4, 16.8) | 1.11 (0.76–1.62) | 11 (7.7, 14.3) | 1.30 (0.86–1.98) | |
| Hyperlipidemia | No (ref.) | 10.7 (8.3, 13.1) | 9.5 (7.7, 11.3) | ||
| Yes | 14 (11.3, 16.7) | 0.84 (0.48–1.47) | 7.9 (3.4, 12.4) | 0.82 (0.43–1.56) | |
| Traumatic brain injury | No (ref.) | 10.7 (8.9, 12.5) | 8.1 (6.5, 9.7) | ||
| Yes | 32(22.8, 41.2) | 3.93 (2.47–6.27) | 23.7 (15.3, 32.1) | 3.54 (2.12–5.92) | |
| Chronic constipation | No (ref.) | 11.8 (9.6, 14.0) | 8.4 (6.6, 10.2) | ||
| Yes | 13.5 (10.2, 16.8) | 1.17 (0.82–1.67) | 11.2 (8.1, 14.3) | 1.36 (0.92–2.03) | |
| Urinary incontinence | No (ref.) | 5.7 (3.9, 7.5) | - | ||
| Yes | 19.9 (16.6, 23.2) | 4.13 (2.81–6.07) | - | - | |
| ADL dependence | No (ref.) | 11.6 (9.8, 13.4) | 8.6 (7.0, 10.2) | ||
| Yes | 21.3 (12.9, 29.7) | 2.06 (1.21–3.53) | 18 (10.0, 26.0) | 2.33 (1.30–4.15) | |
| Physical ADL dependence | No (ref.) | 6.8 (4.6, 9.0) | 1.7 (0.7, 2.7) | ||
| Yes | 16.6 (13.9, 19.3) | 2.73 (1.85–4.03) | 15.2 (12.5, 17.9) | 10.66 (5.35–21.25) | |
| IADL dependence | No (ref.) | 11.4 (9.2, 13.6) | 8.4 (6.4, 10.4) | ||
| Yes | 14.2 (10.9, 17.5) | 1.28 (0.90–1.82) | 11 (8.1, 13.9) | 1.34 (0.90–1.99) | |
| Cognitive impairment (MMSE) | No (ref.) | 11.3 (8.9, 13.7) | 7.8 (5.8, 9.8) | ||
| Yes | 13.6 (10.7, 16.5) | 1.23 (0.88–1.73) | 11.2 (8.5, 13.9) | 1.48 (1.01–2.17) | |
| Variables | FI | DI | |
|---|---|---|---|
| OR (95%CI) | OR (95%CI) | ||
| Age (years) | 65~69 (ref.) | ||
| 70~74 | 0.74 (0.46–1.20) | 0.93 (0.54–1.61) | |
| 75~79 | 1.04 (0.62–1.75) | 1.25 (0.70–2.25) | |
| 80~ | 0.52 (0.26–1.05) | 0.43 (0.18–1.01) | |
| Female sex | 0.75 (0.49–1.16) | 0.82 (0.51–1.34) | |
| Income | Subsidies (ref.) ※ | ||
| Poverty | 0.92 (0.57–1.49) | 1.22 (0.72–2.08) | |
| Nonpoverty | 0.52 (0.31–0.87) | 0.56 (0.31–1.02) | |
| Medical expenses (≥average vs. < average) | 1.21 (0.81–1.80) | 1.27 (0.81–1.98) | |
| Regular house/farm work (yes vs. no) | 0.77 (0.48–1.22) | 1.02 (0.61–1.73) | |
| Tea consumption (yes vs. no) | 0.76 (0.42–1.37) | 0.44 (0.19–0.98) | |
| Sleep quality | Good (ref.) | ||
| Moderate | 1.21 (0.79–1.87) | 1.49 (0.92–2.41) | |
| Poor | 1.44 (0.85–2.47) | 1.83 (1.02–3.28) | |
| Social interaction in neighborhood | Good (ref.) | ||
| Satisfactory | 3.73(2.24–6.20) | 2.95 (1.70–5.13) | |
| Poor | 2.69(0.87–8.26) | 0.91 (0.17–4.79) | |
| Memory complaint (yes vs. no) | 1.53 (0.79–2.96) | 2.24 (0.96–5.25) | |
| Cognitive impairment (MMSE) (yes vs. no) | - | 1.00 (0.64–1.55) | |
| Hearing | Good (ref.) | ||
| Moderate | 1.00(0.59–1.61) | 1.07 (0.58–1.98) | |
| Poor | 1.37 (0.78–2.38) | 1.36 (0.72–2.58) | |
| Chronic disease | 0 (ref.) | ||
| 1 | 0.54 (0.30–0.97) | 0.58 (0.32–1.05) | |
| 2 | 0.62 (0.31–1.23) | 0.72 (0.39–1.35) | |
| ≥3 | 0.46 (0.20–1.09) | 0.50 (0.23–1.10) | |
| Hypertension (yes vs. no) | 1.55 (0.94–2.55) | - | |
| Cerebrovascular disease (yes vs. no) | 1.86 (1.00–3.47) | 1.77 (0.90–3.48) | |
| Traumatic brain injury (yes vs. no) | 2.96 (1.62–5.42) | 2.80 (1.44–5.46) | |
| Urinary incontinence (yes vs. no) | 5.17 (2.86–9.45) | - | |
| ADL dependence (yes vs. no) | 1.15 (0.58–2.26) | 0.88 (0.44–1.76) | |
| Physical ADL dependence (yes vs. no) | 0.70 (0.38–1.32) | 9.21 (4.47–18.96) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Y.; Wang, K.; Zou, P.; Li, X.; He, J.; Wang, J. Prevalence and Associated Factors of Fecal Incontinence and Double Incontinence among Rural Elderly in North China. Int. J. Environ. Res. Public Health 2020, 17, 9105. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239105
Luo Y, Wang K, Zou P, Li X, He J, Wang J. Prevalence and Associated Factors of Fecal Incontinence and Double Incontinence among Rural Elderly in North China. International Journal of Environmental Research and Public Health. 2020; 17(23):9105. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239105
Chicago/Turabian StyleLuo, Yan, Kai Wang, Ping Zou, Xiaomei Li, Jinjie He, and Jing Wang. 2020. "Prevalence and Associated Factors of Fecal Incontinence and Double Incontinence among Rural Elderly in North China" International Journal of Environmental Research and Public Health 17, no. 23: 9105. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239105