The Association between Home Healthcare and Burdensome Transitions at the End-of-Life in People with Dementia: A 12-Year Nationwide Population-Based Cohort Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Background/Rationale
1.2. Objectives
2. Materials and Methods
2.1. Setting
2.2. Data Source and Ethics
2.3. Cohort Definition
2.4. Case Identification
2.5. Exposure Measurements and Covariates
2.6. Statistical Analysis
3. Results
3.1. Participants
3.2. Descriptive Data
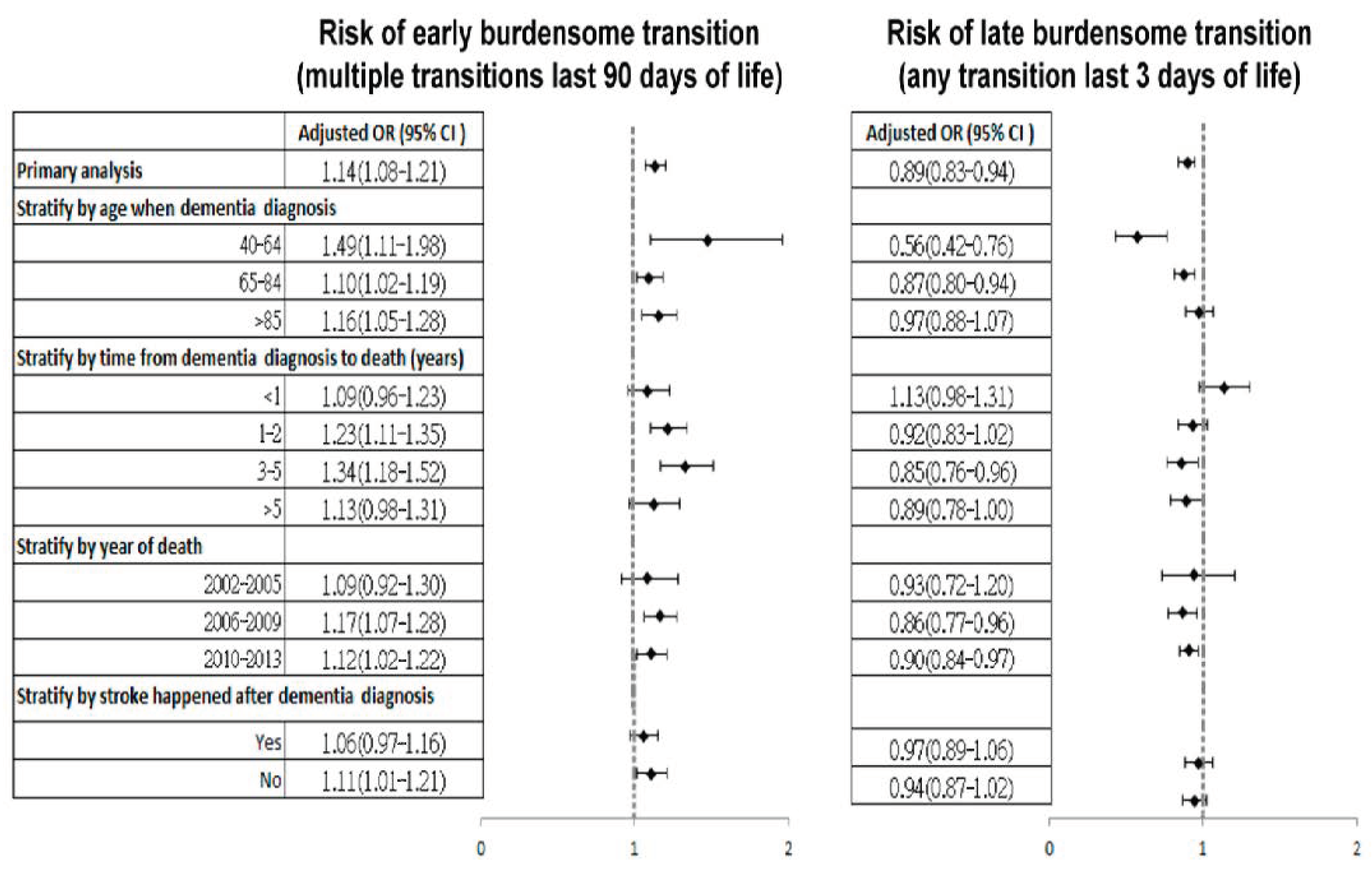
3.3. Main Results
4. Discussion
4.1. End-of-Life Transitions and Hospital/ICU Utilisations
4.2. Impact of HHC on Burdensome End-of-Life Transitions
4.3. Integration of Various Home-Based Services for Better End-of-Life Care
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | ICD-9-CM code |
|---|---|
| Dementia | 290.1x–209.4x, 291.2, 292.82, 294.1x, 294.8, 331.0, 331.1x, 331.2, 331.82 |
| Stroke | 430–438 |
| Cancer | 140–208 |
| Heart Failure | 428 |
| Chronic obstructive pulmonary disease | 491, 492, 494, 496 |
| Liver cirrhosis/ chronic liver disease | 571 |
| Renal failure | 585.4, 585.5, 585.6, 586 |
| Hypertension | 401, 402, 403, 404, 405 |
| Diabetes | 250, 251 |
| Coronary artery disease | 410–414 |
| Hyperlipidaemia | 272 |
| Atrial fibrillation | 427.31 |
| Depression | 296.2–296.36, 300.4, 311 |
| Code in NHIRD | Definition |
|---|---|
| A. In common area | |
| 05307C | Fee for physician visit (per time)—for the first to fourth patient visited by one physician on the same day |
| 05309C | Fee for physician visit (per time)—for the fifth to eighth patient visited by one physician on the same day |
| 05301C | Fee for nurse visit (per time)—RUG 1, within reasonable caseload |
| 05328C | Fee for nurse visit (per time)—RUG 1, beyond reasonable caseload |
| 05303C | Fee for nurse visit (per time)—RUG 2, within reasonable caseload |
| 05330C | Fee for nurse visit (per time)—RUG 2, beyond reasonable caseload |
| 05305C | Fee for nurse visit (per time)—RUG 3, within reasonable caseload |
| 05332C | Fee for nurse visit (per time)—RUG 3, beyond reasonable caseload |
| 05321C | Fee for nurse visit (per time)—RUG 4, within reasonable caseload |
| 05334C | Fee for nurse visit (per time)—RUG 4, beyond reasonable caseload |
| B. In specific rural area | |
| 05308C | Fee for physician visit (per time)—for the first to fourth patient visited by one physician on the same day |
| 05310C | Fee for physician visit (per time)—for the fifth to eighth patient visited by one physician on the same day |
| 05302C | Fee for nurse visit (per time)—RUG 1, within reasonable caseload |
| 05329C | Fee for nurse visit (per time)—RUG 1, beyond reasonable caseload |
| 05304C | Fee for nurse visit (per time)—RUG 2, within reasonable caseload |
| 05331C | Fee for nurse visit (per time)—RUG 2, beyond reasonable caseload |
| 05306C | Fee for nurse visit (per time)—RUG 3, within reasonable caseload |
| 05333C | Fee for nurse visit (per time)—RUG 3, beyond reasonable caseload |
| 05322C | Fee for nurse visit (per time)—RUG 4, within reasonable caseload |
| 05335C | Fee for nurse visit (per time)—RUG 4, beyond reasonable caseload |

| Early Burdensome Transition | Late Burdensome Transition | |||
|---|---|---|---|---|
| Cases | Controls | Cases | Controls | |
| Primary analysis | ||||
| No HHC | 6255 (71.87) | 12755 (73.28) | 6475 (73.98) | 12,485 (71.33) |
| HHC | 2448 (28.13) | 4651 (26.72) | 2277 (26.02) | 5019 (28.67) |
| Stratify by age when cohort entry | ||||
| 40–64 | ||||
| No HHC | 477 (81.12) | 899 (85.05) | 584 (89.02) | 893 (82.08) |
| HHC | 111 (18.88) | 158 (14.95) | 72 (10.98) | 195 (17.92) |
| 65–84 | ||||
| No HHC | 3715 (71.77) | 7296 (72.80) | 3799 (73.68) | 7007 (70.74) |
| HHC | 1461 (28.23) | 2726 (27.20) | 1357 (26.32) | 2898 (29.26) |
| >85 | ||||
| No HHC | 2063 (71.19) | 4560 (72.07) | 2092 (71.16) | 4585 (70.42) |
| HHC | 876 (29.81) | 1767 (27.93) | 848 (28.84) | 1926 (29.58) |
| Stratify by time from dementia diagnosis to death (years) | ||||
| <1 | ||||
| No HHC | 2642 (83.98) | 4337 (84.71) | 1900 (85.55) | 3674 (84.44) |
| HHC | 504 (16.02) | 783 (15.29) | 321 (14.45) | 677 (15.56) |
| 1 to 2 | ||||
| No HHC | 1983 (68.71) | 4377 (72.17) | 2198 (74.91) | 4186 (72.93) |
| HHC | 903 (31.29) | 1688 (27.83) | 736 (25.09) | 1554 (27.07) |
| 3–5 | ||||
| No HHC | 982 (62.59) | 2362 (68.31) | 1259 (68.65) | 2404 (64.42) |
| HHC | 587 (37.41) | 1096 (31.69) | 575 (31.35) | 1328 (35.58) |
| >5 | ||||
| No HHC | 648 (58.80) | 1679 (60.77) | 1118 (63.41) | 2221 (60.34) |
| HHC | 454 (41.20) | 1084 (39.23) | 645 (36.59) | 1460 (39.66) |
| Stratify by year of death | ||||
| 2002–2005 | ||||
| No HHC | 1196 (82.71) | 2400 (82.99) | 560 (83.71) | 1099 (82.14) |
| HHC | 250 (17.29) | 492 (17.01) | 109 (16.29) | 239 (17.86) |
| 2006–2009 | ||||
| No HHC | 2628 (72.20) | 5386 (73.98) | 2043 (76.40) | 3913 (73.17) |
| HHC | 1012 (27.80) | 1894 (26.02) | 631 (23.60) | 1435 (26.83) |
| 2010–2013 | ||||
| No HHC | 2431 (67.21) | 4969 (68.69) | 3872 (71.58) | 7473 (69.08) |
| HHC | 1186 (32.79) | 2265 (31.31) | 1537 (28.42) | 3345 (30.92) |
| Stratify by stroke happened after cohort entry | ||||
| Yes | ||||
| No HHC | 2007 (56.73) | 3632 (56.72) | 1631 (56.67) | 3715 (55.50) |
| HHC | 1531 (43.27) | 2771 (43.28) | 1247 (43.33) | 2979 (44.50) |
| No | ||||
| No HHC | 4248 (82.25) | 9123 (82.91) | 4844 (82.47) | 8770 (81.13) |
| HHC | 917 (17.75) | 1880 (17.09) | 1030 (17.53) | 2040 (18.87) |
| Early Burdensome Transition | Late Burdensome Transition | |||
|---|---|---|---|---|
| Adjusted OR | 95 % CI | Adjusted OR | 95 % CI | |
| All people in the matched cases and controls | ||||
| No HHC | 1 | (Reference) | 1 | (Reference) |
| HHC | 1.14 | 1.08–1.21 | 0.89 | 0.83–0.94 |
| After deleting the people with missing data in urbanisation variable | ||||
| No HHC | 1 | (Reference) | 1 | (Reference) |
| HHC | 1.10 | 1.01–1.19 | 0.87 | 0.80–0.94 |
References
- Sleeman, K.E.; De Brito, M.; Etkind, S.; Nkhoma, K.; Guo, P.; Higginson, I.J.; Gomes, B.; Harding, R. The escalating global burden of serious health-related suffering: Projections to 2060 by world regions, age groups, and health conditions. Lancet 2019, 7, E883–E892. [Google Scholar] [CrossRef] [Green Version]
- Patel, V. Deaths Registered in England and Wales (Series DR): 2017; Office for National Statistics: London, UK, 2018. [Google Scholar]
- Ellen, A.; Kramarow, B.T.-V. Dementia Mortality in the United States, 2000–2017. Natl. Vital Stat. Rep. 2019, 68, 1–29. [Google Scholar]
- Shepherd, H.; Livingston, G.; Chan, J.; Sommerlad, A. Hospitalisation rates and predictors in people with dementia: A systematic review and meta-analysis. BMC Med. 2019, 17, 130. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Ho, C.H.; Huang, C.C.; Hsu, Y.W.; Chen, Y.C.; Chen, P.J.; Chen, G.T.; Wang, J.J. Comparison of healthcare utilization and life-sustaining interventions between elderly patients with dementia and those with cancer near the end of life: A nationwide, population-based study in Taiwan. Geriatr. Gerontol. Int. 2017, 17, 2545–2551. [Google Scholar] [CrossRef]
- Aaltonen, M.; Rissanen, P.; Forma, L.; Raitanen, J.; Jylha, M. The impact of dementia on care transitions during the last two years of life. Age Ageing 2012, 41, 52–57. [Google Scholar] [CrossRef] [Green Version]
- Sleeman, K.E.; Perera, G.; Stewart, R.; Higginson, I.J. Predictors of emergency department attendance by people with dementia in their last year of life: Retrospective cohort study using linked clinical and administrative data. Alzheimers Dement. 2018, 14, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Aaltonen, M.; Raitanen, J.; Forma, L.; Pulkki, J.; Rissanen, P.; Jylha, M. Burdensome transitions at the end of life among long-term care residents with dementia. J. Am. Med. Dir. Assoc. 2014, 15, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Gozalo, P.; Teno, J.M.; Mitchell, S.L.; Sinner, J.; Bynum, J.; Tyler, D.; Mor, V. End-of-life transitions among nursing home residents with cognitive issues. N. Engl. J. Med. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leniz, J.; Higginson, I.J.; Stewart, R.; Sleeman, K.E. Understanding which people with dementia are at risk of inappropriate care and avoidable transitions to hospital near the end-of-life: A retrospective cohort study. Age Ageing 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.J.; Liang, F.W.; Ho, C.H.; Cheng, S.Y.; Chen, Y.C.; Chen, Y.H.; Chen, Y.C. Association between palliative care and life-sustaining treatments for patients with dementia: A nationwide 5-year cohort study. Palliat. Med. 2018, 32, 622–630. [Google Scholar] [CrossRef]
- Miller, S.C.; Lima, J.C.; Mitchell, S.L. Influence of hospice on nursing home residents with advanced dementia who received Medicare-skilled nursing facility care near the end of life. J. Am. Geriatr. Soc. 2012, 60, 2035–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenwax, L.; Spilsbury, K.; Arendts, G.; McNamara, B.; Semmens, J. Community-based palliative care is associated with reduced emergency department use by people with dementia in their last year of life: A retrospective cohort study. Palliat. Med. 2015, 29, 727–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vleminck, A.; Morrison, R.S.; Meier, D.E.; Aldridge, M.D. Hospice Care for Patients With Dementia in the United States: A Longitudinal Cohort Study. J. Am. Med. Dir. Assoc. 2018, 19, 633–638. [Google Scholar] [CrossRef]
- Sachs, G.A.; Shega, J.W.; Cox-Hayley, D. Barriers to excellent end-of-life care for patients with dementia. J. Gen. Intern. Med. 2004, 19, 1057–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, R.; Bunn, F.; Lynch, J.; Van den Block, L.; Goodman, C. Palliative care for people with dementia living at home: A systematic review of interventions. Palliat. Med. 2019, 33, 726–742. [Google Scholar] [CrossRef] [Green Version]
- WHO. The Growing Need for Home Health Care for the Elderly; World Health Organization, Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2015. [Google Scholar]
- Landers, S.; Madigan, E.; Leff, B.; Rosati, R.J.; McCann, B.A.; Hornbake, R.; MacMillan, R.; Jones, K.; Bowles, K.; Dowding, D.; et al. The Future of Home Health Care: A Strategic Framework for Optimizing Value. Home Health Care Manag. Pract. 2016, 28, 262–278. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, C.S. Population Health and Tailored Medical Care in the Home: The Roles of Home-Based Primary Care and Home-Based Palliative Care. J. Pain Symptom Manag. 2018, 55, 1041–1046. [Google Scholar] [CrossRef] [Green Version]
- Shepperd, S.; Iliffe, S.; Doll, H.A.; Clarke, M.J.; Kalra, L.; Wilson, A.D.; Goncalves-Bradley, D.C. Admission avoidance hospital at home. Cochrane Database Syst. Rev. 2016, 9, CD007491. [Google Scholar] [CrossRef] [Green Version]
- Jennings, L.A.; Turner, M.; Keebler, C.; Burton, C.H.; Romero, T.; Wenger, N.S.; Reuben, D.B. The Effect of a Comprehensive Dementia Care Management Program on End-of-Life Care. J. Am. Geriatr. Soc. 2019, 67, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, S.L.; Morris, J.N.; Park, P.S.; Fries, B.E. Terminal care for persons with advanced dementia in the nursing home and home care settings. J. Palliat. Med. 2004, 7, 808–816. [Google Scholar] [CrossRef]
- NHIA. National Health Insurance Annual Statistical Report, 2018; National Health Insurance Administration: Taipei City, Taiwan, 2018. Available online: https://www.nhi.gov.tw/english/Content_List.aspx?n=AB41B66610EAC01A&topn=616B97F8DF2C3614 (accessed on 11 April 2020).
- NHIA. Integrated Home Healthcare Program, 2016; National Health Insurance Administration: Taipei City, Taiwan, 2016. Available online: https://www.nhi.gov.tw/Content_List.aspx?n=229E6EBB8F3CF41B&topn=5FE8C9FEAE863B46 (accessed on 11 April 2020).
- Chang, H.T.; Lai, H.Y.; Hwang, I.H.; Ho, M.M.; Hwang, S.J. Home healthcare services in Taiwan: A nationwide study among the older population. BMC Health Serv. Res. 2010, 10, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHIA. Reimbursement Items and Payment Regulations of Healthcare in National Health Insurance. In Home Health Care Payment Regulations; National Health Insurance Administration: Taipei, Taiwan, 2015. [Google Scholar]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating Development Stratification of Taiwan Townships into Sampling Design of Large Scale Health Interview Survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar] [CrossRef]
- Van den Block, L.; Pivodic, L.; Pardon, K.; Donker, G.; Miccinesi, G.; Moreels, S.; Vega Alonso, T.; Deliens, L.; Onwuteaka-Philipsen, B. Transitions between health care settings in the final three months of life in four EU countries. Eur. J. Public Health 2015, 25, 569–575. [Google Scholar] [CrossRef]
- Lee, Y.H.; Lu, C.W.; Huang, C.T.; Chang, H.H.; Yang, K.C.; Kuo, C.S.; Chang, Y.K.; Hsu, C.C.; Huang, K.C. Impact of a home health care program for disabled patients in Taiwan: A nationwide population-based cohort study. Medicine (Baltimore) 2019, 98, e14502. [Google Scholar] [CrossRef] [PubMed]
- Mondor, L.; Maxwell, C.J.; Hogan, D.B.; Bronskill, S.E.; Gruneir, A.; Lane, N.E.; Wodchis, W.P. Multimorbidity and healthcare utilization among home care clients with dementia in Ontario, Canada: A retrospective analysis of a population-based cohort. PLoS Med. 2017, 14, e1002249. [Google Scholar] [CrossRef]
- Gravelle, H.; Dusheiko, M.; Sheaff, R.; Sargent, P.; Boaden, R.; Pickard, S.; Parker, S.; Roland, M. Impact of case management (Evercare) on frail elderly patients: Controlled before and after analysis of quantitative outcome data. BMJ 2007, 334, 31. [Google Scholar] [CrossRef] [Green Version]
- Huntley, A.L.; Thomas, R.; Mann, M.; Huws, D.; Elwyn, G.; Paranjothy, S.; Purdy, S. Is case management effective in reducing the risk of unplanned hospital admissions for older people? A systematic review and meta-analysis. Fam. Pract. 2013, 30, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Jee, S.H.; Cabana, M.D. Indices for continuity of care: A systematic review of the literature. Med. Care Res. Rev. 2006, 63, 158–188. [Google Scholar] [CrossRef]
- Amjad, H.; Carmichael, D.; Austin, A.M.; Chang, C.H.; Bynum, J.P. Continuity of Care and Health Care Utilization in Older Adults With Dementia in Fee-for-Service Medicare. JAMA Intern. Med. 2016, 176, 1371–1378. [Google Scholar] [CrossRef]
- Cheng, S.H.; Chen, C.C.; Hou, Y.F. A longitudinal examination of continuity of care and avoidable hospitalization: Evidence from a universal coverage health care system. Arch. Intern. Med. 2010, 170, 1671–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.; Jackson, S.S.; Bullman, T.A.; Cobbs, E.L. Impact of a home-based primary care program in an urban Veterans Affairs medical center. J. Am. Med. Dir. Assoc. 2009, 10, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Huggins, M.; McGregor, M.J.; Cox, M.B.; Bauder, K.; Slater, J.; Yap, C.; Mallery, L.; Moorhouse, P.; Rusnak, C. Advance Care Planning and Decision-Making in a Home-Based Primary Care Service in a Canadian Urban Centre. Can. Geriatr. J. 2019, 22, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Moller, A.D.; Christiansen, D.H.; Bell, C.; Fredberg, U.; Vedsted, P. 24-hour access outpatient clinic for patients with exacerbation of chronic disease: A before-after cohort study of differences in acute healthcare utilisation. BMC Health Serv. Res. 2018, 18, 663. [Google Scholar] [CrossRef]
- Gomes, B.; Calanzani, N.; Curiale, V.; McCrone, P.; Higginson, I.J. Effectiveness and cost-effectiveness of home palliative care services for adults with advanced illness and their caregivers. Cochrane Database Syst. Rev. 2013, 6, CD007760. [Google Scholar] [CrossRef] [Green Version]
- Shepperd, S.; Goncalves-Bradley, D.C.; Straus, S.E.; Wee, B. Hospital at home: Home-based end-of-life care. Cochrane Database Syst. Rev. 2016, 2, CD009231. [Google Scholar] [CrossRef]
- Nakanishi, M.; Ogawa, A.; Nishida, A. Availability of home palliative care services and dying at home in conditions needing palliative care: A population-based death certificate study. Palliat. Med. 2020, 34, 504–512. [Google Scholar] [CrossRef] [Green Version]
- Brian Cassel, J.; Kerr, K.M.; McClish, D.K.; Skoro, N.; Johnson, S.; Wanke, C.; Hoefer, D. Effect of a Home-Based Palliative Care Program on Healthcare Use and Costs. J. Am. Geriatr. Soc. 2016, 64, 2288–2295. [Google Scholar] [CrossRef]
- van der Steen, J.T.; Radbruch, L.; Hertogh, C.M.; de Boer, M.E.; Hughes, J.C.; Larkin, P.; Francke, A.L.; Junger, S.; Gove, D.; Firth, P.; et al. White paper defining optimal palliative care in older people with dementia: A Delphi study and recommendations from the European Association for Palliative Care. Palliat. Med. 2014, 28, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.-Y.; Chen, P.-J.; Wu, Y.-L.; Cheng, C.-H.; Yu, S.-J.; Huang, C.-H.; Li, C.-M.; Wang, Y.-W.; Zhang, K.-P.; Liu, I.T.; et al. HOme-based Longitudinal Investigation of the multidiSciplinary Team Integrated Care (HOLISTIC): Protocol of a prospective nationwide cohort study. BMC Geriatr. 2020, 20, 511. [Google Scholar] [CrossRef]



| All Decedents N = 61,399 | Decedents Included in the Nested Case-Control Analysis | ||||
|---|---|---|---|---|---|
| No Burdensome End-of-Life Transitions (Matched Controls) N = 34,910 | Burdensome End-of-Life Transitions (Matched Cases) N = 17,455 | ||||
| Early
Transition Only (Multiple Transitions Last 90 Days) N = 7891 | Late
Transition Only (Any Transition Last 3 Days) N = 8752 | Both
Early and Late Transitions N = 812 | |||
| Age when death, mean (SD) | 83.2 (9.7) | 83.5 (9.6) | 82.3 (9.6) | 82.7 (10.1) | 82.2 (10.2) |
| Gender (female), n (%) | 29,595 (48.2) | 17,099 (49.0) | 3266 (41.4) | 4486 (51.2) | 339 (41.8) |
| Characteristics at time of dementia diagnosis | |||||
| SES—Income #,
n (%) Dependent Fair High Very high | 11,934 (19.4) 32,609 (53.1) 16,076 (26.2) 780 (1.3) | 6968 (20.0) 18,575 (53.2) 8955 (25.7) 412 (1.2) | 1307 (16.6) 4660 (59.1) 1828 (23.2) 96 (1.2) | 1776 (20.3) 4212 (48.1) 2621 (30.0) 143 (1.6) | 143 (17.6) 426 (52.5) 239 (29.4) 4 (0.5) |
| SES—Urbanisation, n (%)
1 most urbanised 2 3 4 most ruralised | (Missing, n = 25,381; 41.3%) 15,745 (43.7) 15,494 (43.0) 4097 (11.4) 682 (1.9) | (Missing, n = 14,722; 42.2%) 8806 (43.6) 8733 (43.3) 2281 (11.3) 368 (1.8) | (Missing, n = 3153; 40.0%) 2005 (42.3) 2060 (43.5) 580 (12.2) 93 (2.0) | (Missing, n = 3580; 40.9%) 2356 (45.6) 2170 (42.0) 538 (10.4) 108 (2.1) | (Missing, n = 316; 38.9%) 211 (42.5) 218 (44.0) 55 (11.1) 12 (2.4) |
| Age-adjusted CCI, mean (SD) | 7.4 (2.8) | 7.3 (2.8) | 7.7 (2.9) | 7.3 (2.8) | 7.9 (3.0) |
| Comorbidities | |||||
| Cancer, n (%) | 8520 (13.9) | 4699 (13.5) | 1323 (16.8) | 1101 (12.6) | 158 (19.5) |
| Heart failure, n (%) | 10,806 (17.6) | 5998 (17.2) | 1484 (18.8) | 1573 (18.0) | 174 (21.4) |
| COPD, n (%) | 21,466 (35.0) | 12,033 (34.5) | 3066 (38.9) | 2875 (32.9) | 339 (41.8) |
| Liver cirrhosis/ chronic liver Disease, n (%) | 11,946 (19.5) | 6552 (18.8) | 1768 (22.4) | 1634 (18.7) | 177 (21.8) |
| Renal failure, n (%) | 1565 (2.6) | 886 (2.5) | 230 (2.9) | 203 (2.3) | 23 (2.8) |
| Hypertension, n (%) | 40,441 (65.9) | 22,805 (65.3) | 5266 (66.7) | 5720 (65.4) | 555 (68.4) |
| Diabetes, n (%) | 18,953 (30.9) | 10,413 (29.8) | 2664 (33.8) | 2775 (31.7) | 259 (31.9) |
| Coronary artery disease, n (%) | 22,871 (37.3) | 12,755 (36.5) | 3082 (39.1) | 3265 (37.3) | 330 (40.6) |
| Hyperlipidaemia, n (%) | 13,578 (22.1) | 7408 (21.2) | 1647 (20.9) | 2181 (24.9) | 174 (21.4) |
| Atrial fibrillation, n (%) | 3954 (6.4) | 2192 (6.3) | 559 (7.1) | 581 (6.6) | 56 (6.9) |
| Depression, n (%) | 8015 (13.1) | 4321 (12.4) | 1019 (12.9) | 1313 (15.0) | 121 (14.9) |
| Characteristics in the follow-up | |||||
| Time from cohort entry to death (days), mean (SD) | 1030.7 (872.8) | 1038.7 (859.4) | 841.0 (770.4) | 1093.5 (898.8) | 887.2 (816.6) |
| HHC related factors | |||||
| HHC, n (%) | 17,046 (27.8) | 9670 (27.7) | 2197 (27.8) | 2277 (26.0) | 251 (30.9) |
| HHC (total counts/person), mean (SD) | 22.2 (27.4) | 22.8 (27.3) | 16.8 (21.8) | 23.8 (28.8) | 17.0 (24.1) |
| Duration of HHC (days), median (Q1–Q3) | 234 (57–648) | 245 (61–654) | 151 (28–496) | 256 (59–728) | 127 (15–499) |
| Frequency of HHC (counts /year/person), mean (SD) | 9.8 (6.7) | 10.1 (6.7) | 8.4 (6.4) | 10.0 (6.8) | 8.3 (6.5) |
| Resource utilisation group of first HHC, n (%) 1 2 3 4 | (missing n = 20; 0.1%) 895 (5.3) 11,958 (70.2) 3888 (22.8) 285 (1.7) | (missing n = 10; 0.1%) 487 (5.0) 6766 (70.0) 2242 (23.2) 165 (1.7) | (missing n = 4; 0.2%) 118 (5.4) 1458 (66.5) 567 (25.9) 50 (2.3) | (missing n = 5; 0.2%) 147 (6.5) 1663 (73.2) 437 (19.2) 25 (1.1) | 11 (4.4) 168 (66.9) 68 (27.1) 4 (1.6) |
| Time from cohort entry to first HHC (days), median (Q1–Q3) | 520 (145–1179) | 520 (147–1165) | 455 (133–1020) | 578 (151–1255) | 488 (115–1068) |
| Time from last HHC to death, (days), median (Q1–Q3) | 29 (15–67) | 30 (17–69) | 46 (22–89) | 18 (9–32) | 22 (9–52) |
| Early Burdensome Transition (Multiple Transitions Last 90 Days of Life) | Late Burdensome Transition (Any Transition Last 3 Days of Life) | |||||||
|---|---|---|---|---|---|---|---|---|
| Cases (n) | Controls (n) | Adjusted OR | 95 % CI | Cases (n) | Controls (n) | Adjusted OR | 95 % CI | |
| RUG | ||||||||
| 1 | 105 | 229 | (Reference) | 147 | 258 | (Reference) | ||
| 2 | 1278 | 3223 | 0.85 | 0.67–1.08 | 1663 | 3543 | 0.94 | 0.81–1.10 |
| 3 | 486 | 1106 | 0.96 | 0.74–1.24 | 437 | 1136 | 0.91 | 0.80–1.03 |
| 4 | 29 | 88 | 0.71 | 0.44–1.15 | 25 | 77 | 0.91 | 0.79–1.06 |
| HHC by professionals | ||||||||
| HHC by nurse only | 410 | 783 | (Reference) | 410 | 748 | (Reference) | ||
| HHC by physician and nurse | 2034 | 3863 | 1.01 | 0.88–1.15 | 1862 | 4266 | 0.80 | 0.70–0.91 |
| Duration of HHC (days) | ||||||||
| ≤30 | 670 | 861 | (Reference) | 413 | 894 | (Reference) | ||
| >30 and ≤120 | 471 | 821 | 0.80 | 0.66–0.98 | 404 | 840 | 0.69 | 0.56–0.85 |
| >120 and ≤365 | 528 | 1157 | 0.58 | 0.48–0.71 | 504 | 1208 | 0.56 | 0.46–0.69 |
| >365 | 779 | 1812 | 0.50 | 0.42–0.60 | 956 | 2077 | 0.60 | 0.50–0.73 |
| Frequency of HHC (counts/year) | ||||||||
| ≤4 | 933 | 1263 | (Reference) | 636 | 1318 | (Reference) | ||
| 5–8 | 435 | 899 | 0.66 | 0.57–0.76 | 407 | 899 | 0.94 | 0.81–1.10 |
| 9–16 | 744 | 1598 | 0.64 | 0.56–0.72 | 789 | 1801 | 0.91 | 0.80–1.03 |
| >16 | 336 | 891 | 0.52 | 0.45–0.61 | 445 | 1001 | 0.91 | 0.79–1.06 |
| Time between the dementia diagnosis and receiving the first HHC (years) | ||||||||
| <1 | 1084 | 2079 | (Reference) | 895 | 1943 | (Reference) | ||
| 1–2 | 804 | 1478 | 1.03 | 0.92–1.15 | 697 | 1526 | 0.99 | 0.87–1.11 |
| 3–4 | 210 | 434 | 0.91 | 0.76–1.10 | 230 | 566 | 0.87 | 0.73–1.03 |
| >4 | 350 | 660 | 1.00 | 0.86–1.17 | 455 | 984 | 0.99 | 0.86–1.14 |
| Time between receiving the last HHC and death (days) | ||||||||
| >90 | 569 | 999 | (Reference) | 265 | 994 | (Reference) | ||
| 31–90 | 944 | 1303 | 1.28 | 1.12–1.46 | 334 | 1534 | 0.82 | 0.68–0.98 |
| 16–30 | 484 | 1245 | 0.69 | 0.59–0.80 | 692 | 1384 | 1.88 | 1.59–2.21 |
| 0–15 | 451 | 1104 | 0.73 | 0.62–0.84 | 986 | 1107 | 3.35 | 2.85–3.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-J.; Ho, C.-H.; Liao, J.-Y.; Smits, L.; Hsiung, C.A.; Yu, S.-J.; Zhang, K.-P.; Petersen, I.; Sampson, E.L. The Association between Home Healthcare and Burdensome Transitions at the End-of-Life in People with Dementia: A 12-Year Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 9255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249255
Chen P-J, Ho C-H, Liao J-Y, Smits L, Hsiung CA, Yu S-J, Zhang K-P, Petersen I, Sampson EL. The Association between Home Healthcare and Burdensome Transitions at the End-of-Life in People with Dementia: A 12-Year Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(24):9255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249255
Chicago/Turabian StyleChen, Ping-Jen, Chung-Han Ho, Jung-Yu Liao, Lisanne Smits, Chao A. Hsiung, Sang-Ju Yu, Kai-Ping Zhang, Irene Petersen, and Elizabeth L. Sampson. 2020. "The Association between Home Healthcare and Burdensome Transitions at the End-of-Life in People with Dementia: A 12-Year Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 17, no. 24: 9255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249255