Vaccination Status and Attitude among Measles Cluster Cases in Austria, 2019

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cluster Case Definition
2.2. Case Finding and Data Collection
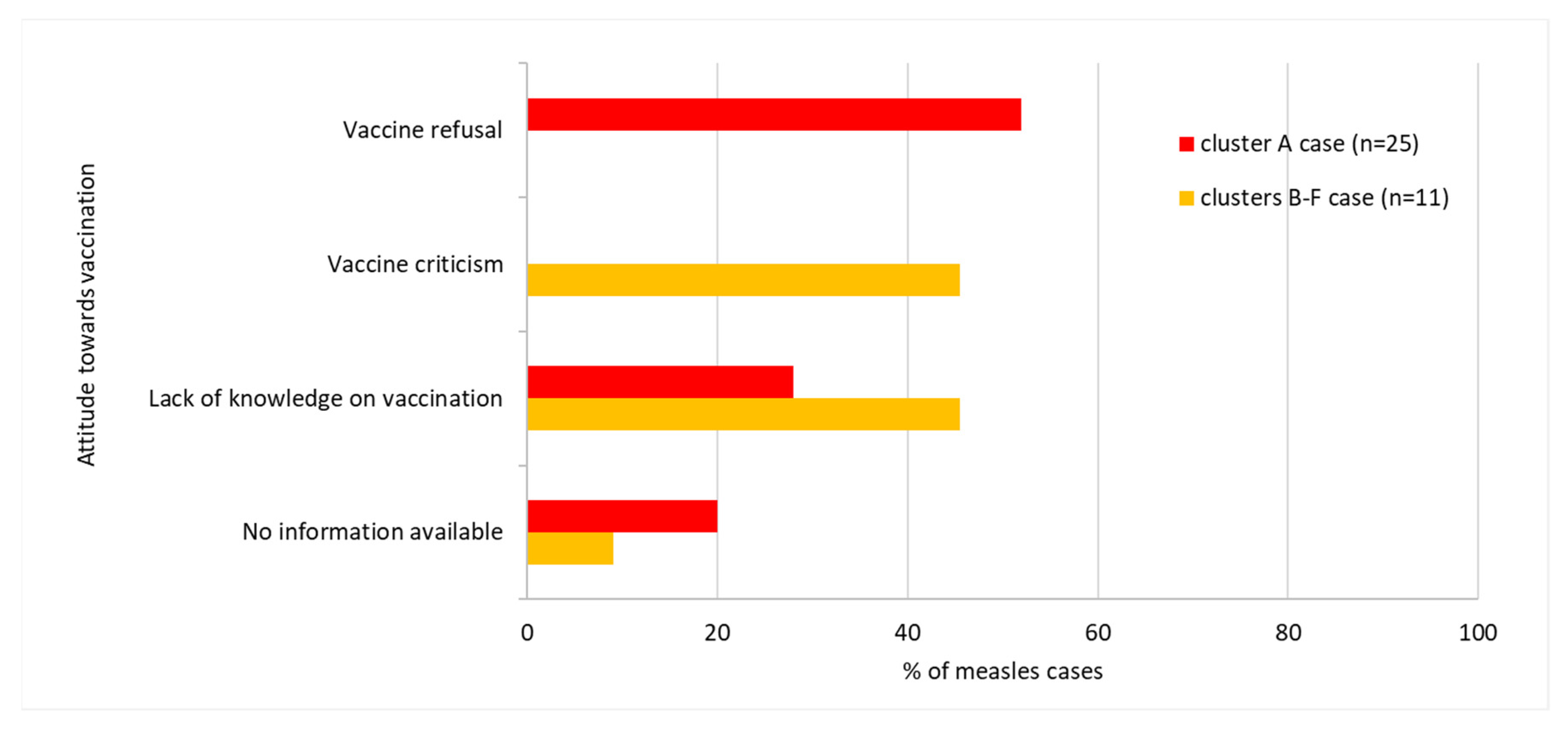
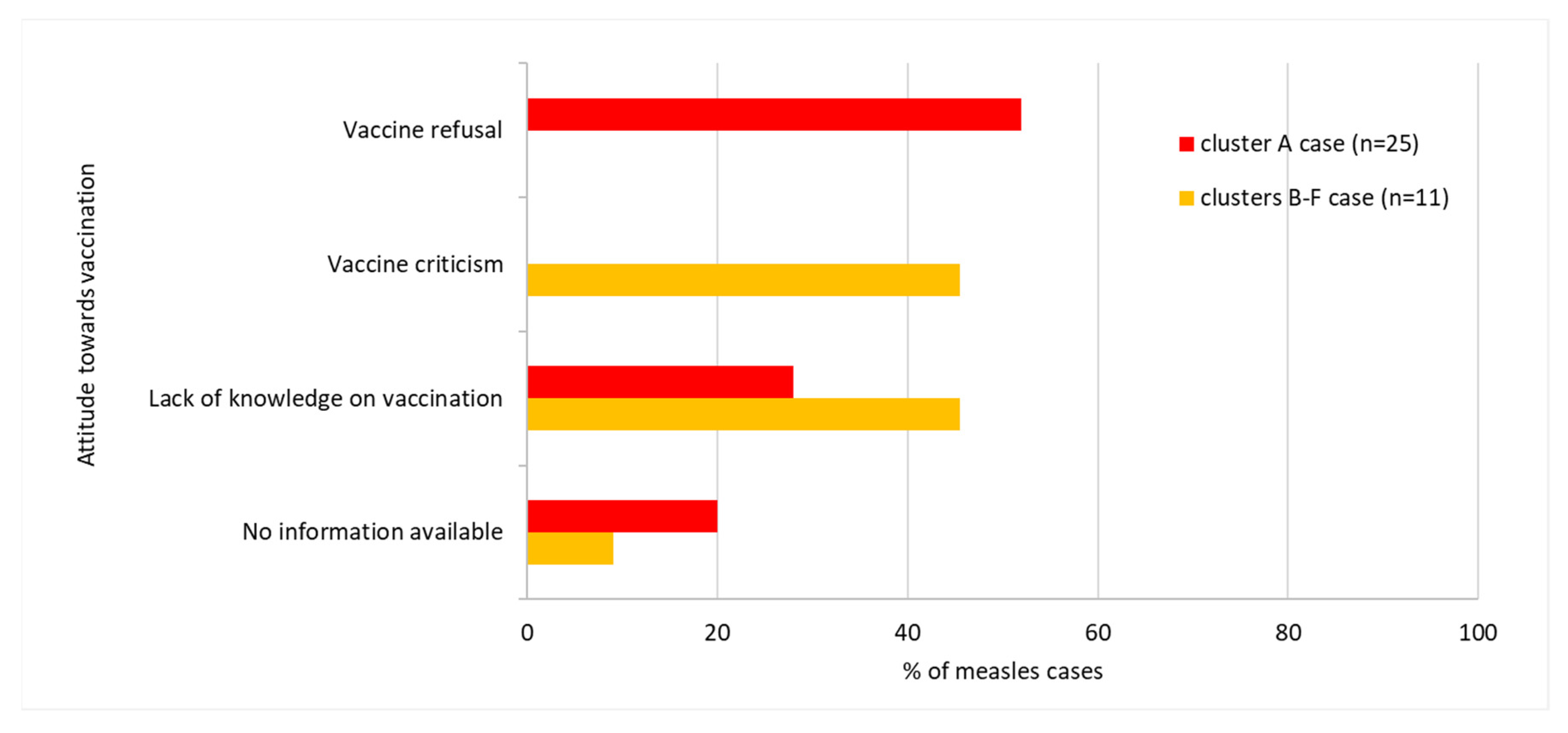
- vaccine refusal—defined as an attitude of an individual who refuses all vaccines,
- vaccine criticism—defined as an attitude of an individual whose concern about vaccines may result in the refusal or the delay of some vaccines, and
- lack of knowledge on vaccination—defined as an attitude of an individual who does not have sufficient knowledge about preventive vaccination, including vaccination plans, which may result in failure of vaccine uptake in a scheduled time.
2.3. Laboratory Methods
3. Results
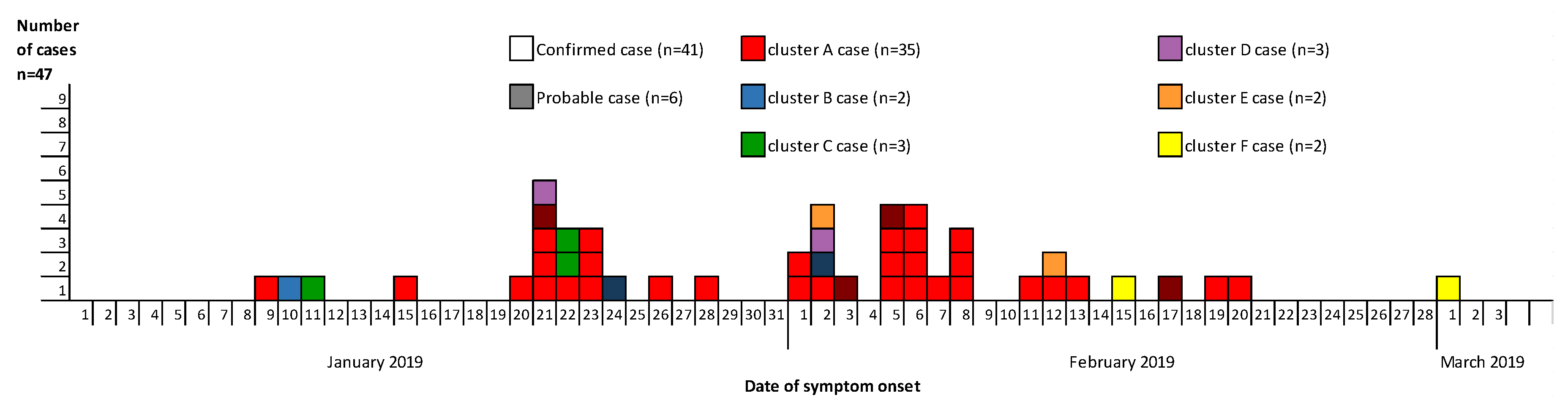
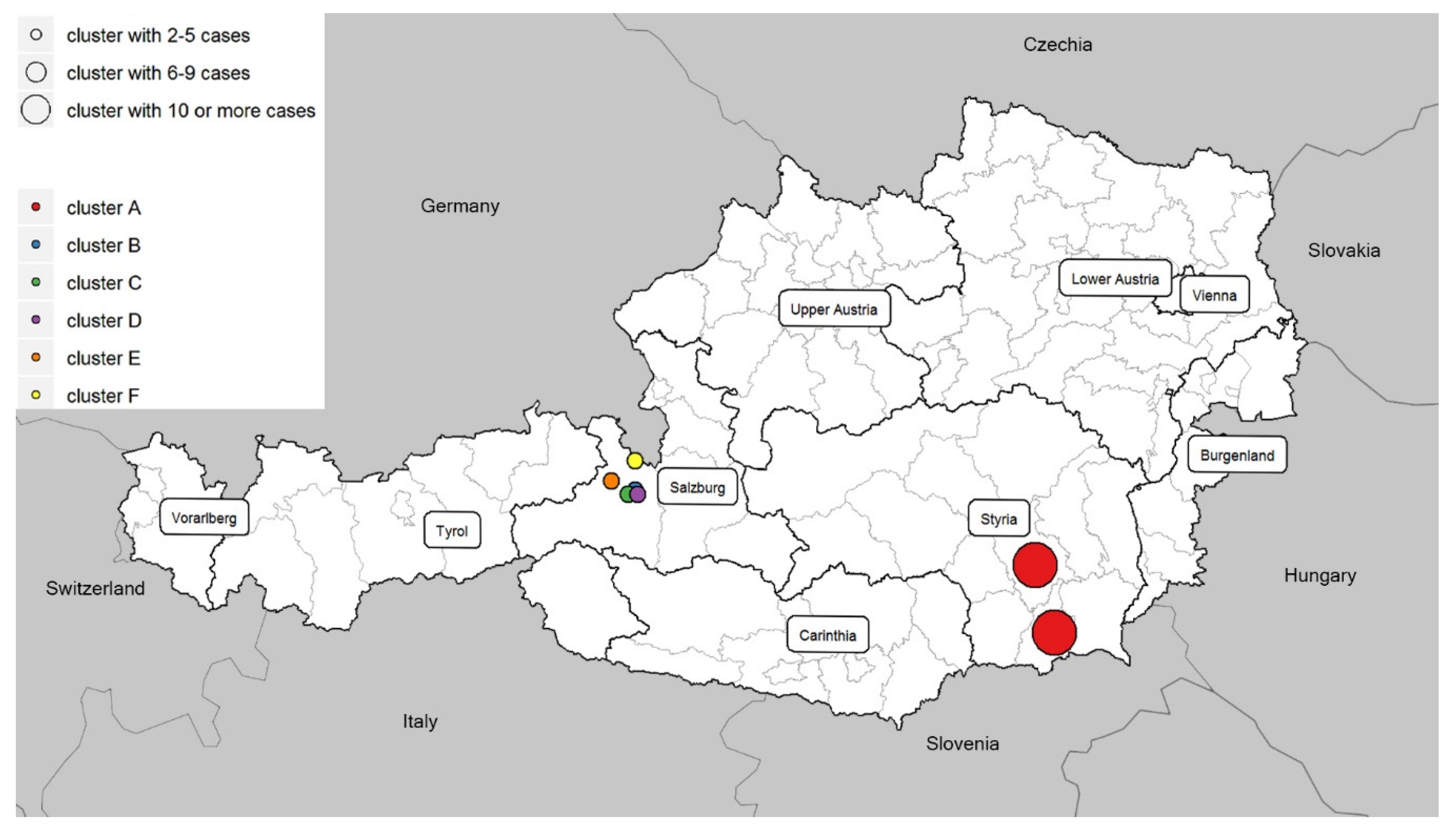
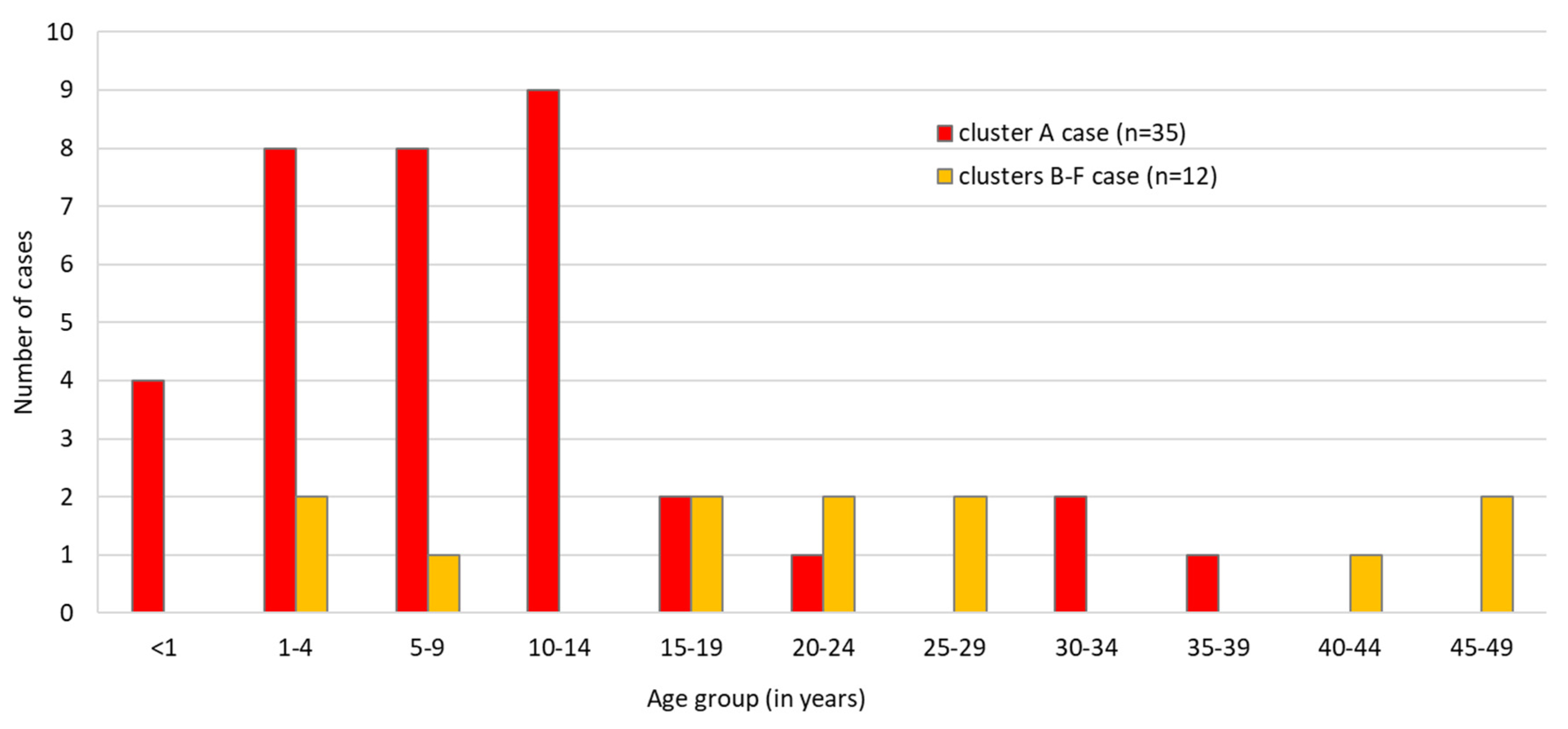
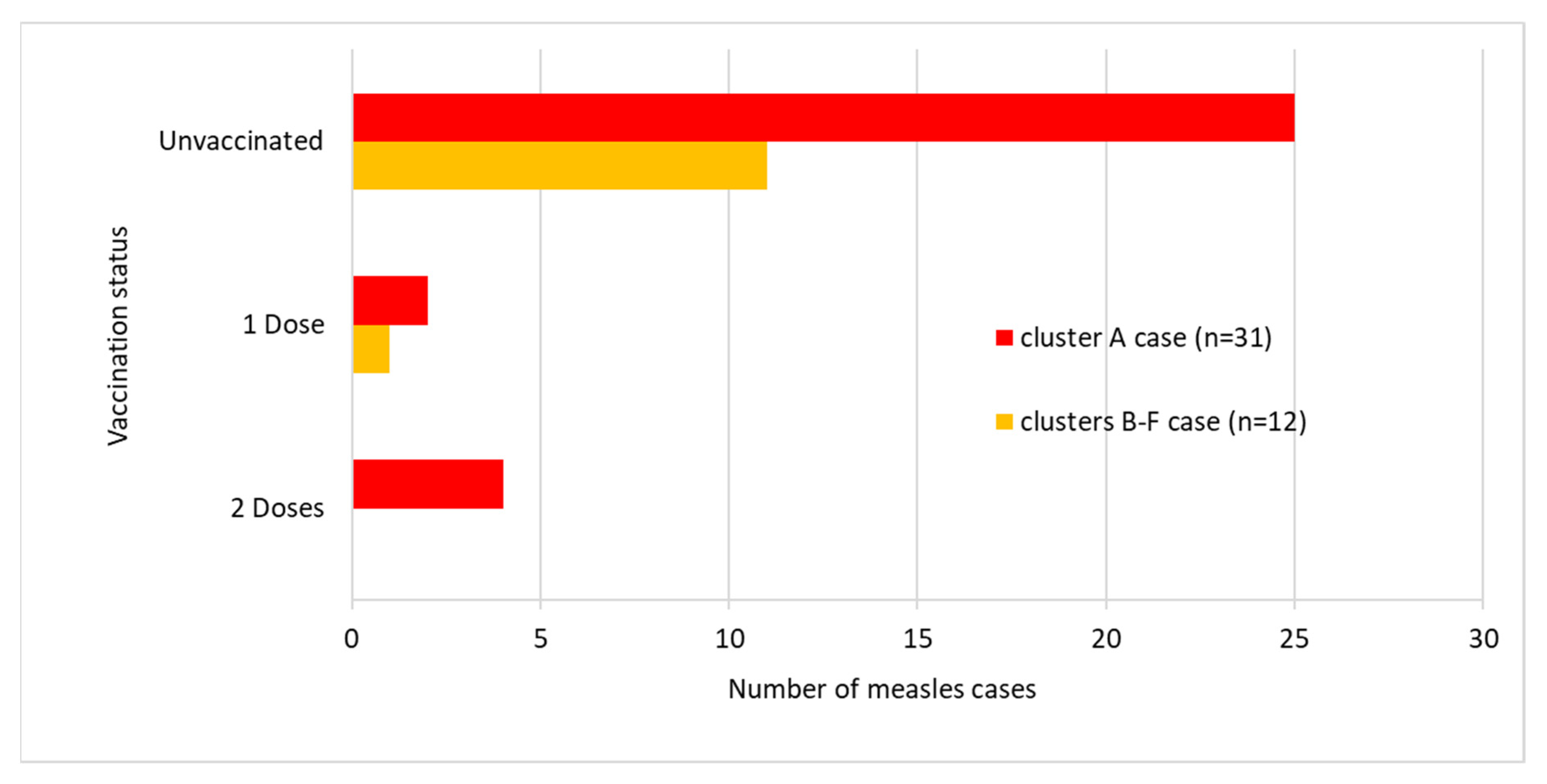
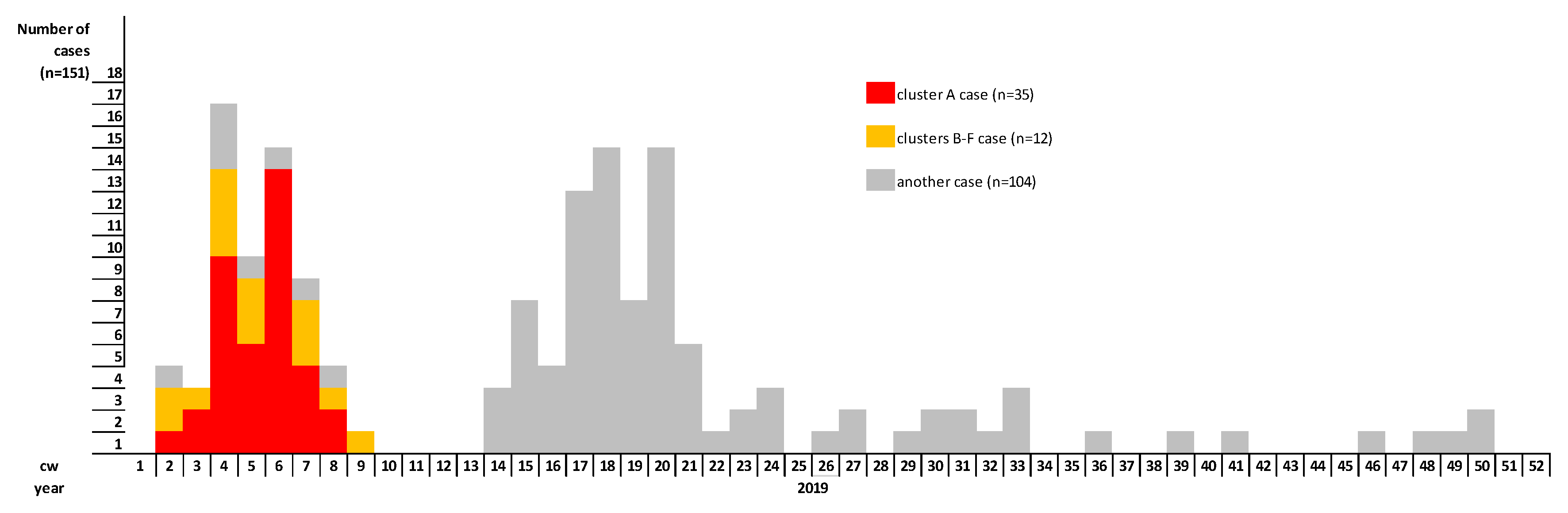
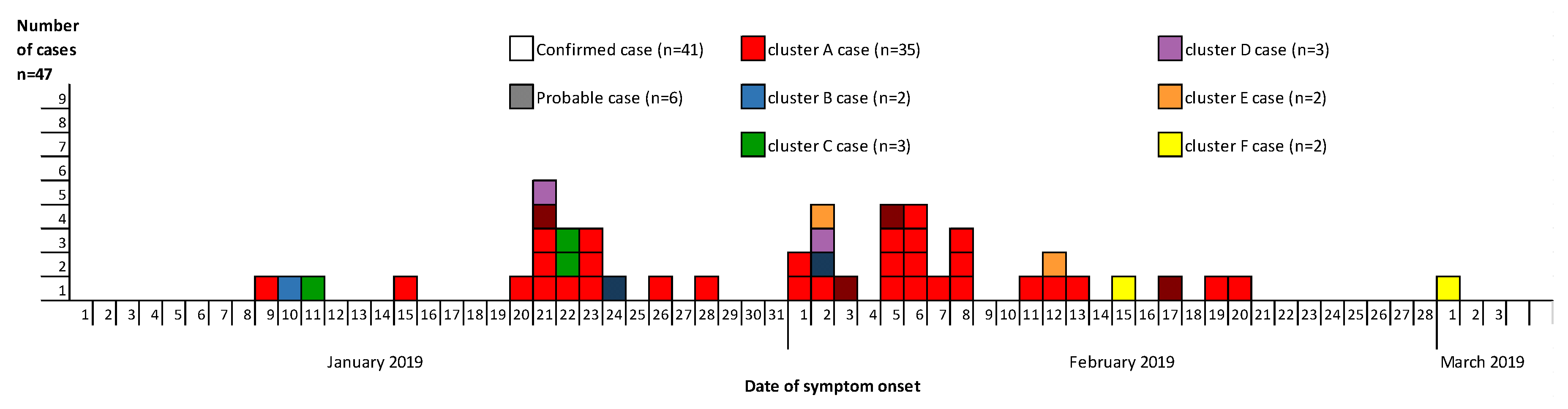
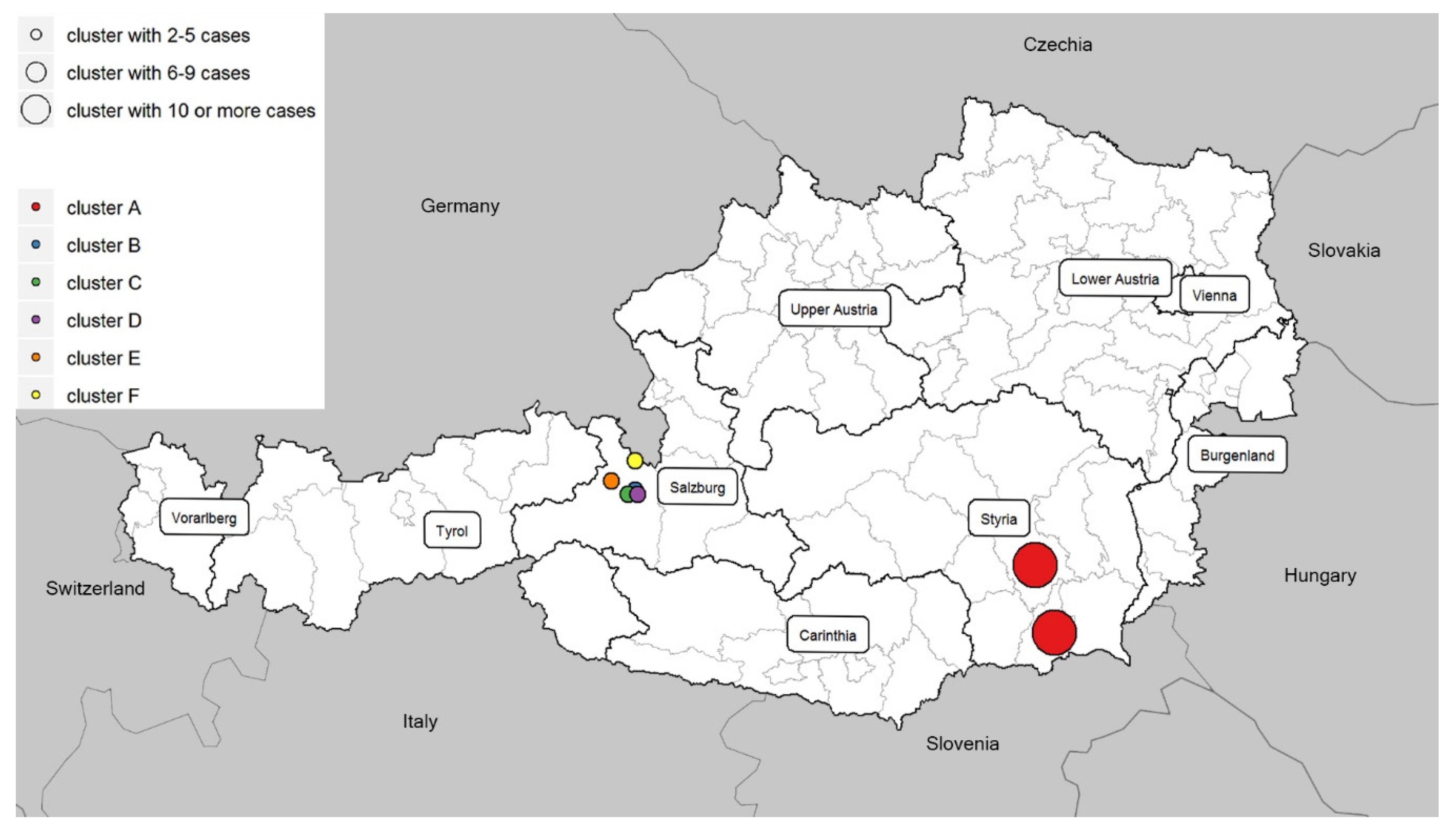
3.1. Descriptive Findings
3.1.1. Cluster A
3.1.2. Clusters B–F
3.2. Laboratory Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Gillian, L.; Crowcroft, N.S. The basic reproduction number (R(0)) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Cherry, J. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases, 7th ed.; Elsevier: Philadelphia, PA, USA, 2014; Volume 2. [Google Scholar]
- Sheikh, S.; Biundo, E.; Courcier, S.; Damm, O.; Launay, O.; Maes, E.; Marcos, C.; Matthews, S.; Meijer, C.; Poscia, A.; et al. A report on the status of vaccination in Europe. Vaccine 2018, 36, 4979–4992. [Google Scholar] [CrossRef] [PubMed]
- WHO Global Vaccine Action Plan 2011–2020; World Health Organization (WHO): Geneva, Switzerland, 2013.
- Migration & Integration. Statistisches Jahrbuch. Zahlen Daten Indikatoren. Wien 2020; Statistik Austria: Vienna, Austria, 2020.
- Strategic Response Plan for the Measles Emergency in the WHO European Region, September 2019–December 2020; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2019.
- In Proceedings of the Eighth Meeting of the European Regional Verification Commission for Measles and Rubella Elimination (RVC), Warsaw, Poland, 12–14 June 2019; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2019. Available online: https://www.euro.who.int/en/health-topics/communicable-diseases/measles-and-rubella/publications/2019/8th-meeting-of-the-european-regional-verification-commission-for-measles-and-rubella-elimination-rvc-2019 (accessed on 14 December 2020).
- Measles and Rubella Laboratory Documents; World Health Organization (WHO): Vienna, Austria, 2018.
- Dubé, E.; Gagnon, D.; Macdonald, N.E. Strategies intended to address vaccine hesitancy: Review of published reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzmann, H.; Wiedermann, U. Mandatory vaccination: Suited to enhance vaccination coverage in Europe? Eurosurveillance 2019, 24, 1900376. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J. The state of vaccine confidence. Lancet 2018, 392, 2244–2246. [Google Scholar] [CrossRef]
- Muscat, M.; Ben Mamou, M.; Singh, S.; de Kat, C.; Jankovic, D.; Huseynov, S.; Deshevoi, S.; Datta, S.; O’Connor, P. Elimination of measles in the WHO European Region-challenges persist. Bundesgesundh. Gesundh. Gesundh. 2019, 62, 440–449. [Google Scholar] [CrossRef]
- Kasper, S.; Holzmann, H.; Aberle, S.W.; Wassermann-Neuhold, M.; Gschiel, H.; Feenstra, O.; Allerberger, F.; Schmid, D. Measles outbreak in Styria, Austria, March-May 2009. Eurosurveillance 2009, 14, 19347. [Google Scholar]
- Paulke-Korinek, M. Schulimpfungen; Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentenschutz: Vienna, Austria, 2019. (In Germany) [Google Scholar]
- Commission Decision of 30 April 2009 Amending Decision 2002/253/EC Laying down Case Definitions for Reporting Communicable Diseases to the Community Network under Decision No 2119/98/EC of the European Parliament and of the Council. In Official Journal of the European Union; European Union: Brussels, Belgium, 2009.
- Manual for the Diagnosis of Measles and Rubella Infection, 2nd ed.; World Health Organization (WHO): Geneva, Switzerland, 2007.
- Measles. In Annual Epidemiological Report for 2019; European Center for Disease Prevention and Control (ECDC): Stockholm, Sweden, 2020.
- Schmid, D.; Holzmann, H.; Schwarz, K.; Kasper, S.; Kuo, H.-W.; Aberle, S.W.; Redlberger-Fritz, M.; Hautmann, W.; Santibanez, S.; Mankertz, A.; et al. Measles outbreak linked to a minority group in Austria, 2008. Epidemiol. Infect. 2009, 138, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Fournet, N.; Mollema, L.; Ruijs, W.L.; Harmsen, I.A.; Keck, F.; Durand, J.Y.; Cunha, M.P.; Wamsiedel, M.; Reis, R.; French, J.; et al. Under-vaccinated groups in Europe and their beliefs, attitudes and reasons for non-vaccination; two systematic reviews. BMC Public Health 2018, 18, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Miko, D.; Costache, C.; Neculicioiu, V. Qualitative Assessment of Vaccine Hesitancy in Romania. Medicina 2019, 55, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjipanayis, A.; Van Esso, D.; Del Torso, S.; Dornbusch, H.J.; Michailidou, K.; Minicuci, N.; Pancheva, R.; Mujkic, A.; Geitmann, K.; Syridou, G.; et al. Vaccine confidence among parents: Large scale study in eighteen European countries. Vaccine 2020, 38, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Global Measles and Rubella Strategic Plan 2012–2020; World Health Organization (WHO): Geneva, Switzerland, 2012.
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [Green Version]
- Arendt, F.; Scherr, S. Investigating an Issue–Attention–Action Cycle: A Case Study on the Chronology of Media Attention, Public Attention, and Actual Vaccination Behavior during the 2019 Measles Outbreak in Austria. J. Health Commun. 2019, 24, 654–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giese, H.; Neth, H.; Moussaïd, M.; Betsch, C.; Gaissmaier, W. The echo in flu-vaccination echo chambers: Selective attention trumps social influence. Vaccine 2020, 38, 2070–2076. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; Macdonald, N.; Bocquier, A.; Peretti-Watel, P.; Verger, P. Underlying factors impacting vaccine hesitancy in high income countries: A review of qualitative studies. Expert Rev. Vaccines 2018, 17, 989–1004. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Alstyne, J.A.M.-V.; Nowak, G.J.; Aikin, A.L. What is ‘confidence’ and what could affect it? A qualitative study of mothers who are hesitant about vaccines. Vaccine 2018, 36, 6464–6472. [Google Scholar] [CrossRef]
- Vanderslott, S. Exploring the meaning of pro-vaccine activism across two countries. Soc. Sci. Med. 2019, 222, 59–66. [Google Scholar] [CrossRef]
- Musa, S.; Skrijelj, V.; Kulo, A.; Habersaat, K.B.; Smjecanin, M.; Primorac, E.; Becirovic, D.; Jackson, C. Identifying barriers and drivers to vaccination: A qualitative interview study with health workers in the Federation of Bosnia and Herzegovina. Vaccine 2020, 38, 1906–1914. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henszel, L.; Kanitz, E.E.; Grisold, A.; Holzmann, H.; Aberle, S.W.; Schmid, D. Vaccination Status and Attitude among Measles Cluster Cases in Austria, 2019. Int. J. Environ. Res. Public Health 2020, 17, 9377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249377
Henszel L, Kanitz EE, Grisold A, Holzmann H, Aberle SW, Schmid D. Vaccination Status and Attitude among Measles Cluster Cases in Austria, 2019. International Journal of Environmental Research and Public Health. 2020; 17(24):9377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249377
Chicago/Turabian StyleHenszel, Lukasz, Elisabeth E. Kanitz, Andrea Grisold, Heidemarie Holzmann, Stephan W. Aberle, and Daniela Schmid. 2020. "Vaccination Status and Attitude among Measles Cluster Cases in Austria, 2019" International Journal of Environmental Research and Public Health 17, no. 24: 9377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249377