Initial COVID-19 Outbreak: An Epidemiological and Socioeconomic Case Review of Iran


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Country’s Overview and Results
3.1. Case Presentation
3.1.1. Demographic, Economic, Geographic, Political, and Climatic Characteristics of Iran
3.1.2. Healthcare System
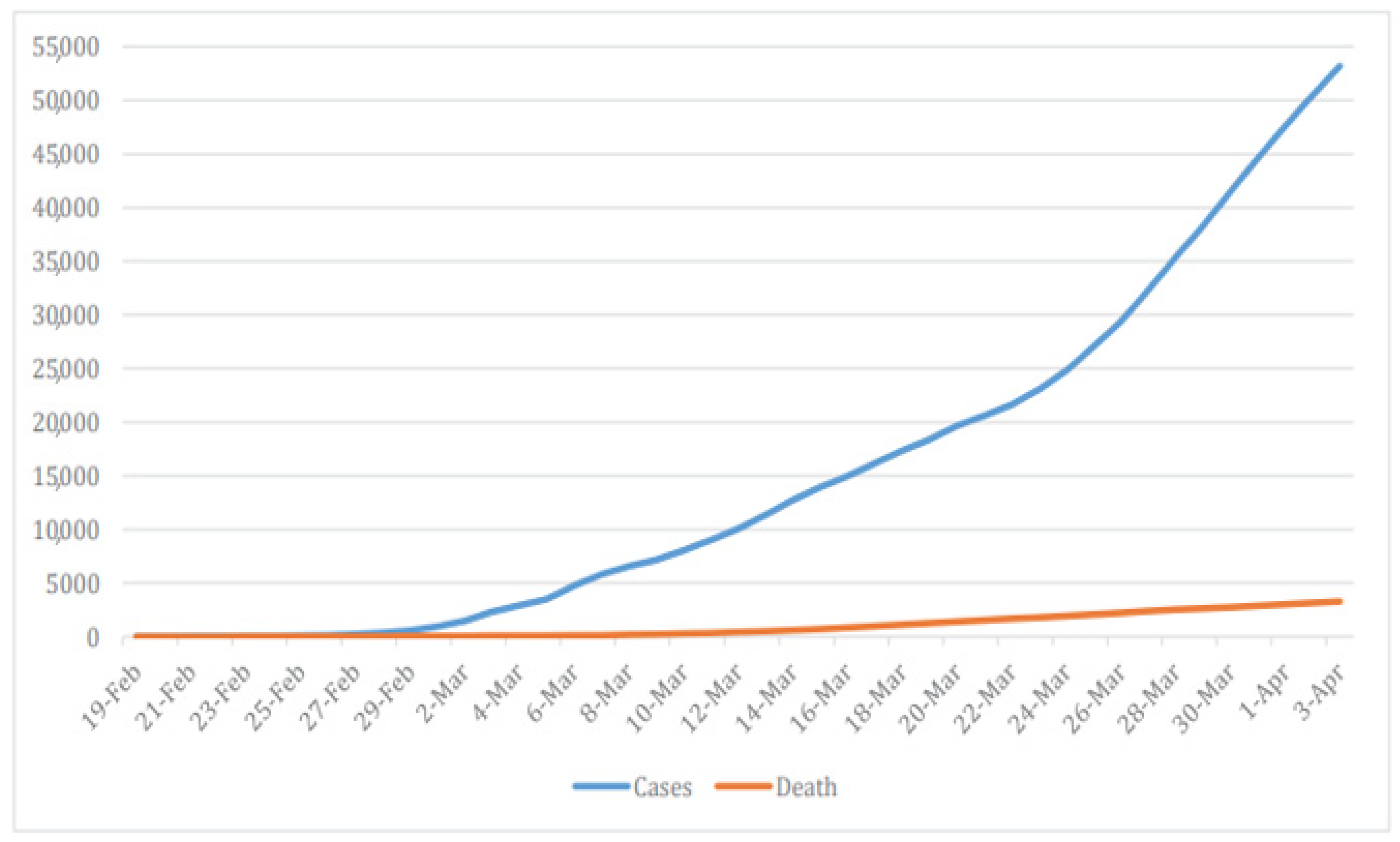
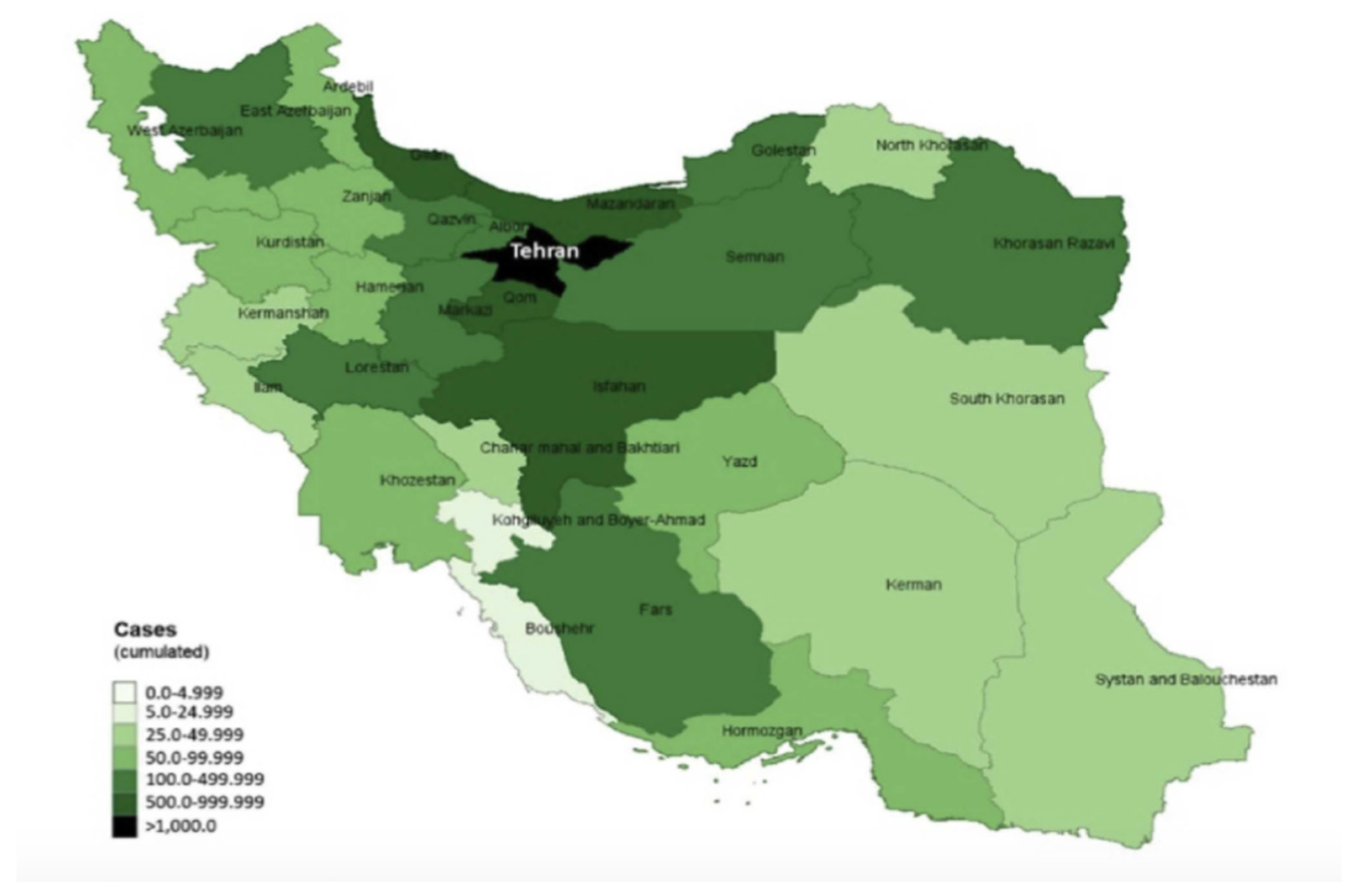
3.1.3. Epidemiological Situation of Iran Regarding COVID-19
3.2. Management and Outcome
3.2.1. Non-Pharmaceutical Measures
3.2.2. Political and Social Issues
3.2.3. Economic Impact
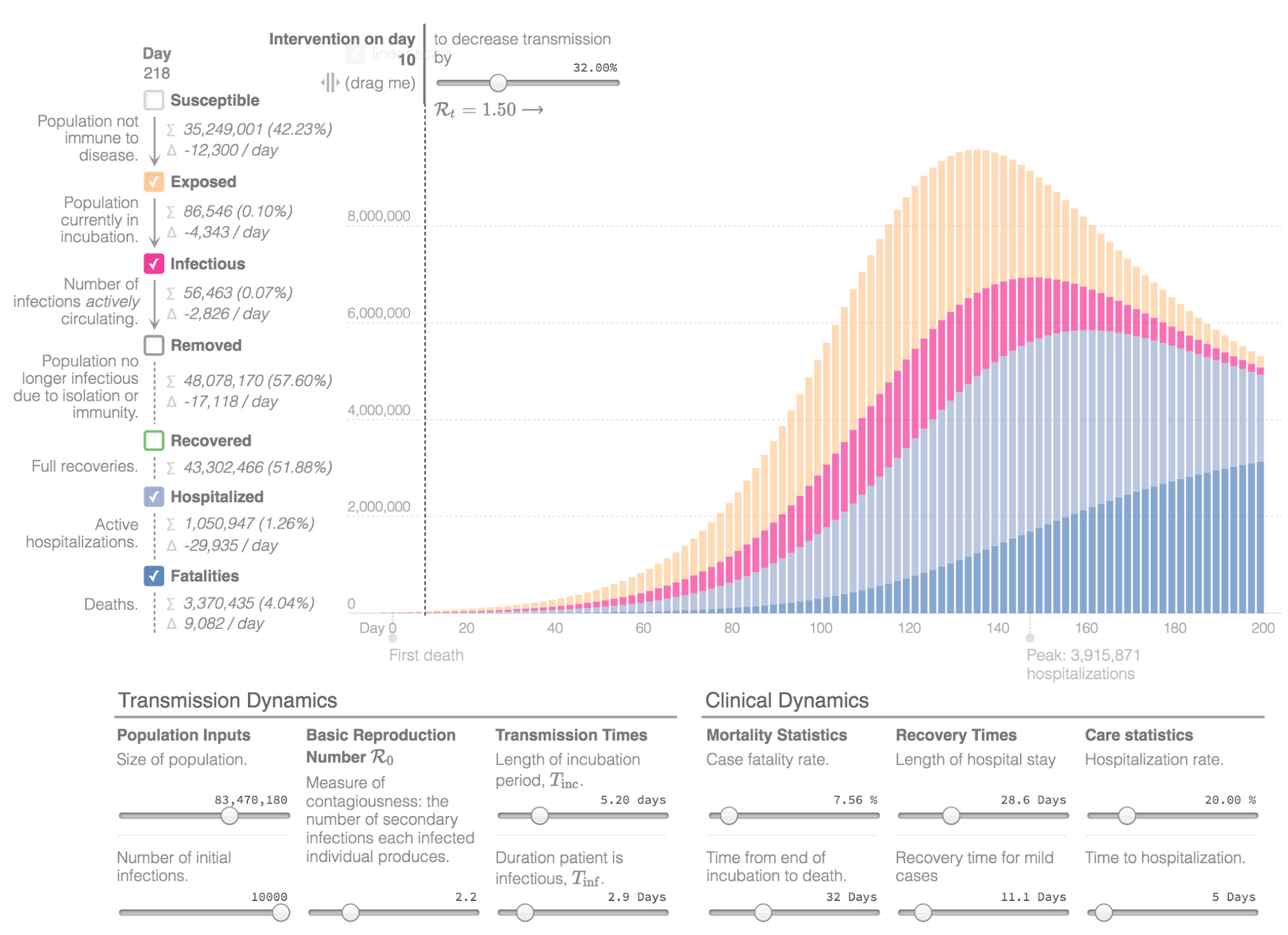
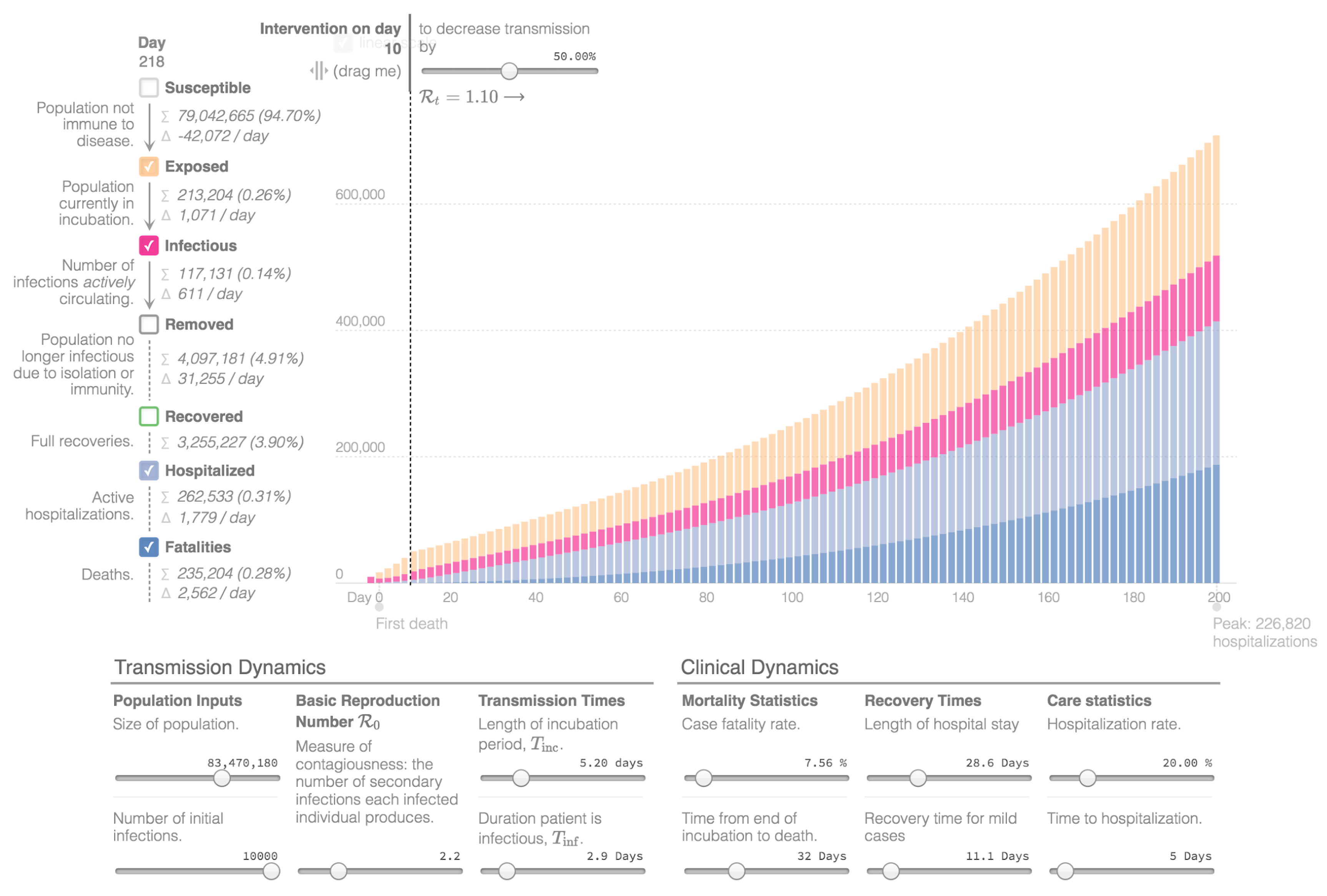
3.2.4. Mathematical Modeling Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lu, H.; Stratton, C.W.; Tang, Y.-W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.M.; Adams, M.J.; Carstens, E.B.; Lefkowitz, E.J. Virus Taxonomy: Ninth Report of the International Committee on Taxonomy of Viruses; Elsevier: Amsterdam, The Netherlands, 2012; pp. 486–487. [Google Scholar]
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-11-march-2020 (accessed on 25 October 2020).
- Raoofi, A.; Takian, A.; Sari, A.A.; Olyaeemanesh, A.; Haghighi, H.; Aarabi, M. COVID-19 Pandemic and comparative health policy learning in Iran. Arch. Iran. Med. 2020, 23, 220–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iran International Exclusive. WHO Report Shows Regime of Iran Covered up the Coronavirus Outbreak. Available online: https://iranintl.com/en/world/exclusive-who-report-shows-regime-iran-covered-coronavirus-outbreak (accessed on 4 May 2020).
- Arab-Mazar, Z.; Sah, R.; Rabaan, A.A.; Dhama, K.; Rodriguez-Morales, A.J. Mapping the incidence of the COVID-19 hotspot in Iran – Implications for Travellers. Travel Med. Infect. Dis. 2020, 34, 101630. [Google Scholar] [CrossRef]
- Goh, G. Epidemic Calculator. 2020. Available online: https://gabgoh.github.io/COVID/index.html?fbclid=IwAR1U6uu-iTfyJ3gWQvYi8Bli3406AuR3MK2NQV-b31Iu4SRsmE-QnSRwHTU (accessed on 12 March 2020).
- IMUNA Education Through Simulation. Iran, Islamic Republic of, Country Profiles. Available online: https://imuna.org/resources/country-profiles/iran-islamic-republic/ (accessed on 12 March 2020).
- United Nations. Data Country Profiles. Iran (Islamic Republic of). Available online: http://data.un.org/en/iso/ir.html (accessed on 12 March 2020).
- United Nations Department of Economic and Social Affairs. Iran, Revision of World Population Prospects. 2019. Available online: https://population.un.org/wpp/ (accessed on 12 March 2020).
- World Data. The Climate in Iran. Available online: https://www.worlddata.info/asia/iran/climate.php (accessed on 13 March 2020).
- World Intellectual Property Organisation. Constitution of the Islamic Republic of Iran. 1989. Available online: https://wipolex.wipo.int/en/text/332330 (accessed on 13 March 2020).
- Avery, P.W.; Afary, J. Iran—Relief, Britannica. Available online: https://www.britannica.com/place/Iran/Relief (accessed on 10 March 2020).
- World Bank. Islamic Republic of Iran. 2018. Available online: https://www.worldbank.org/en/country/iran/overview (accessed on 12 March 2020).
- Mehrdad, R. Health system in Iran. JMAJ 2009, 52, 69–73. [Google Scholar]
- Letafat, M.; Beyranvand, T.; Aryankhesal, A.; Behzadifar, M.; Behzadifar, M. Universal Health Coverage (UHC) in Iran. Iran. J. Public Heal. 2018, 47, 1061–1062. [Google Scholar]
- Esmailzadeh, H.; Rajabi, F.; Rostamigooran, N.; Majdzadeh, R. Iran Health System Reform Plan Methodology. Iran. J. Public Health 2013, 42 (Suppl. 1), 13–17. [Google Scholar]
- Abolhallaje, M.; Mousavi, S.M.; Anjomshoa, M.; Nasiri, A.B.; Seyedin, H.; Sadeghifar, J.; Aryankhesal, A.; Vasokolaei, G.R.; Nasiri, M.B. Assessing health inequalities in Iran: A focus on the distribution of health care facilities. Glob. J. Health Sci. 2014, 6, 285–291. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Strategic Partnership for International Health Regulations (2005) and Health Security (SPH)—Iran’s Health Security Status. Available online: https://extranet.who.int/sph/recipient/iran-islamic-republic#ihrsar (accessed on 10 March 2020).
- Ministry of Health and Medical Education. Daily Situation Report on Coronavirus Disease (COVID-19) in Iran. Available online: http://corona.behdasht.gov.ir/files/site1/files/Factsheet_12-0109-En.pdf (accessed on 28 March 2020).
- World Bank. Population of Iran. 2019. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=IR (accessed on 12 March 2020).
- John Hopkins University of Medicine. Coronavirus COVID-19 Global Cases Interactive Dashboard. 2020. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 28 March 2020).
- Rogg, I. Coronavirus Iran: Iran Cannot Stop the Spread of the Coronavirus, Neue Zuercher Zeitung. Available online: https://www.nzz.ch/international/coronavirus-iran-ausbreitung-schwer-einzudaemmen-ld.1547156 (accessed on 19 March 2020).
- BBC News. Iran Reports Leap in Death Toll. Available online: https://www.bbc.com/news/world-middle-east-51801968 (accessed on 9 March 2020).
- World Population Review. Population of Cities in Iran (2020). Available online: https://worldpopulationreview.com/countries/cities/iran (accessed on 12 March 2020).
- Abdi, M. Coronavirus disease 2019 (COVID-19) outbreak in Iran: Actions and problems. Infect. Control Hosp. Epidemiol. 2020, 41, 754–755. [Google Scholar] [CrossRef] [Green Version]
- Reuters. Iran’s Coronavirus Death Toll Reaches 2757-Health Official. Available online: https://www.reuters.com/article/health-coronavirus-iran-idUSD5N2BI04O (accessed on 30 March 2020).
- Yjc. Announcement of Trends and Epidemiological Models of Coronavirus. Available online: https://bit.ly/3dF9D1Z (accessed on 28 March 2020).
- Tuite, A.R.; Bogoch, I.I.; Sherbo, R.; Watts, A.; Fisman, D.; Khan, K. Estimation of Coronavirus disease 2019 (COVID-19) burden and potential for international dissemination of infection from Iran. Ann. Intern. Med. 2020, 172, 699–701. [Google Scholar] [CrossRef] [Green Version]
- Reuters; Farge, E. WHO to Start Coronavirus Testing in Rebel Syria; Iran Raises Efforts, Official Says. Available online: https://uk.reuters.com/article/uk-health-coronavirus-mideast/who-to-start-coronavirus-testing-in-rebel-syria-iran-raises-efforts-official-says-idUKKBN2133O0 (accessed on 24 March 2020).
- Iraninti. Hospitals in Iran Refuse to Record COVID19 as the Cause of Death. Available online: https://iranintl.com/en/iran/hospitals-iran-refuse-record-covid19-cause-death (accessed on 18 March 2020).
- Worldometers. COVID-19 Outbreak in Iran—Data Visualisation. 2020. Available online: https://www.worldometers.info/coronavirus/country/%C4%B1ran (accessed on 8 November 2020).
- The Central Bank of Iran. “تمهیدات مراقبتی ویژه “مشتریان بانک ها” به منظور مقابله با ویروس کرونا”. Available online: https://cbi.ir/showitem/19952.aspx (accessed on 10 March 2020).
- Radio Farda. اعطای مرخصی به ۷۰ هزار زندانی برای جلوگیری از شیوع کرونا. Available online: https://www.radiofarda.com/a/30477520.html (accessed on 9 March 2020).
- Tehran Times. Google Play Removes Iranian App INTENDED to curb COVID-19. Available online: https://www.tehrantimes.com/news/446237/Google-Play-removes-Iranian-app-intended-to-curb-COVID-19 (accessed on 17 March 2020).
- Official Website of the President of the Islamic Republic of Iran. Available online: http://www.president.ir (accessed on 21 March 2020).
- Iranian Students’ News Agency (ISNA). Available online: https://www.isna.ir/news (accessed on 21 March 2020).
- Kaffashi, A.; Jahani, F. Nowruz travelers and the COVID-19 pandemic in Iran. Infect. Control. Hosp. Epidemiol. 2020, 41, 1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iran Press News Agency, Firefighters Disinfect Tehran Streets, Passways with Latest Heavy Equipment. Available online: https://iranpress.com/content/19618 (accessed on 11 March 2020).
- BBC News. Coronavirus: Iran Bans Internal Travel to Avert ‘Second Wave’. Available online: https://www.bbc.com/news/world-middle-east-52039298 (accessed on 25 March 2020).
- BBC News. Iran’s Cities Will Be Quarantined. Available online: https://www.bbc.com/persian/iran-52045576 (accessed on 26 March 2020).
- Bedrosian, S.R.; Young, C.E.; Smith, L.A.; Cox, J.D.; Manning, C.; Pechta, L.; Telfer, J.L.; Gaines-McCollom, M.; Harben, K.; Holmes, W.; et al. Lessons of risk communication and health promotion—West Africa and United States. MMWR Suppl. 2016, 65, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- New York Times. Iran Plane Crash Covered. Available online: https://www.nytimes.com/2020/01/26/world/middleeast/iran-plane-crash-coverup.html (accessed on 4 April 2020).
- Alimardani, M.; Elswah, M. Trust, religion, and politics: Coronavirus misinformation in Iran. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Salehi-Isfahani, D. The Coronavirus is Iran’s Perfect Storm. Foreign Affairs, 18 March 2020. [Google Scholar]
- BBC News. MSF in Iran Has Stopped. Available online: https://www.bbc.com/persian/iran-52016338 (accessed on 24 March 2020).
- Parhizi, A. Le Nouveau Coronavirus Rouvre le Débat Entre Sciences et Religion en Iran. L’Orient Le Jour. 2020. Available online: https://www.lorientlejour.com/article/1208719/le-nouveau-coronavirus-rouvre-le-debat-entre-science-et-religion-en-iran.html (accessed on 3 March 2020).
- ABC News. As Iranian New Year Begins, Fear of New Wave of Coronavirus Cases Emerges. Available online: https://abcnews.go.com/International/iranian-year-begins-fear-wave-coronavirus-cases-emerges/story?id=69722197 (accessed on 21 March 2020).
- Ghanbari, B. On forecasting the spread of the COVID-19 in Iran: The second wave. Chaos Solit. Fract. 2020, 140, 110176. [Google Scholar] [CrossRef] [PubMed]
- Zareipour, M.; Kalejahi, J.N. The role of social participation in controlling and preventing of coronavirus 2019 disease in Iran. Open Access Maced. J. Med Sci. 2020, 8, 134–136. [Google Scholar] [CrossRef]
- New York Times. Coronavirus Fears Reverberate Across Global Economy. Available online: https://www.nytimes.com/2020/02/28/business/economy/coronavirus-economy.html (accessed on 28 February 2020).
- Bloomberg. Coronavirus Will Hammer Iran’s Economy. Available online: https://www.bloomberg.com/opinion/articles/2020-02-25/coronavirus-will-hammer-iran-s-economy (accessed on 25 February 2020).
- Iris. Entre Sanctions Américaines et Pandémie de COVID-19, où en Est l’Iran? Available online: https://www.iris-france.org/145440-entre-sanctions-americaines-et-pandemie-de-covid-19-ou-en-est-liran/ (accessed on 20 March 2020).
- Takian, A.; Raoofi, A.; Kazempour-Ardebili, S. COVID-19 battle during the toughest sanctions against Iran. Lancet 2020, 395, 1035–1036. [Google Scholar] [CrossRef]
- Aloosh, M.; Salavati, A.; Aloosh, A. Economic sanctions threaten population health: The case of Iran. Public Health 2019, 169, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Keogh-Brown, M.R.; Smith, R.D. The economic impact of SARS: How does the reality match the predictions? Health Policy 2008, 88, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Lebni, J.Y.; Abbas, J.; Moradi, F.; Salahshoor, M.R.; Chaboksavar, F.; Irandoost, S.F.; Nezhaddadgar, N.; Ziapour, A. How the COVID-19 pandemic effected economic, social, political, and cultural factors: A lesson from Iran. Int. J. Soc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Yezli, S.; Khan, A. COVID-19 social distancing in the Kingdom of Saudi Arabia: Bold measures in the face of political, economic, social and religious challenges. Travel Med. Infect. Dis. 2020, 37, 101692. [Google Scholar] [CrossRef]
- World Health Organisation. China Joint Mission, Report on Coronavirus Disease. 2019. Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 24 February 2020).
- Kucharski, A.J.; Russel, T.W.; Diamond, C.; Liu, Y.; CMMID COVID-19 Working Group. Early Dynamics of Transmission and Control of COVID-19 in Wuhan. Center of Mathematical Modelling of Infectious Diseases Repository. Available online: https://cmmid.github.io/topics/covid19/wuhan-early-dynamics.html (accessed on 26 February 2020).
- Ebrahhimneja, H. Les épidémies et l’évolution de la médecine dans l’Iran du XIXe siècle. Med. Secoli 1999, 11, 167–196. [Google Scholar]
- Venkatesan, P. COVID-19 in Iran: Round 2. Lancet Infect. Dis. 2020, 20, 784. [Google Scholar] [CrossRef]
- Postel-Vinay, N.; Chemardin, J. La communication sur le SRAS: Un outil essentiel de santé publique. Rev. Mal. Respir. 2004, 21, 1061–1065. [Google Scholar] [CrossRef]
- Blundell, R.; Costa, D.; Joyce, M. COVID-19 and inequalities. Fisc. Stud. 2020, 41, 291–319. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blandenier, E.; Habibi, Z.; Kousi, T.; Sestito, P.; Flahault, A.; Rozanova, L. Initial COVID-19 Outbreak: An Epidemiological and Socioeconomic Case Review of Iran. Int. J. Environ. Res. Public Health 2020, 17, 9593. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249593
Blandenier E, Habibi Z, Kousi T, Sestito P, Flahault A, Rozanova L. Initial COVID-19 Outbreak: An Epidemiological and Socioeconomic Case Review of Iran. International Journal of Environmental Research and Public Health. 2020; 17(24):9593. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249593
Chicago/Turabian StyleBlandenier, Elise, Zahra Habibi, Timokleia Kousi, Paolo Sestito, Antoine Flahault, and Liudmila Rozanova. 2020. "Initial COVID-19 Outbreak: An Epidemiological and Socioeconomic Case Review of Iran" International Journal of Environmental Research and Public Health 17, no. 24: 9593. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249593