Development and Investigation of a Wearable Aid for a Load Carriage Task


Abstract
:1. Introduction
2. Materials and Methods
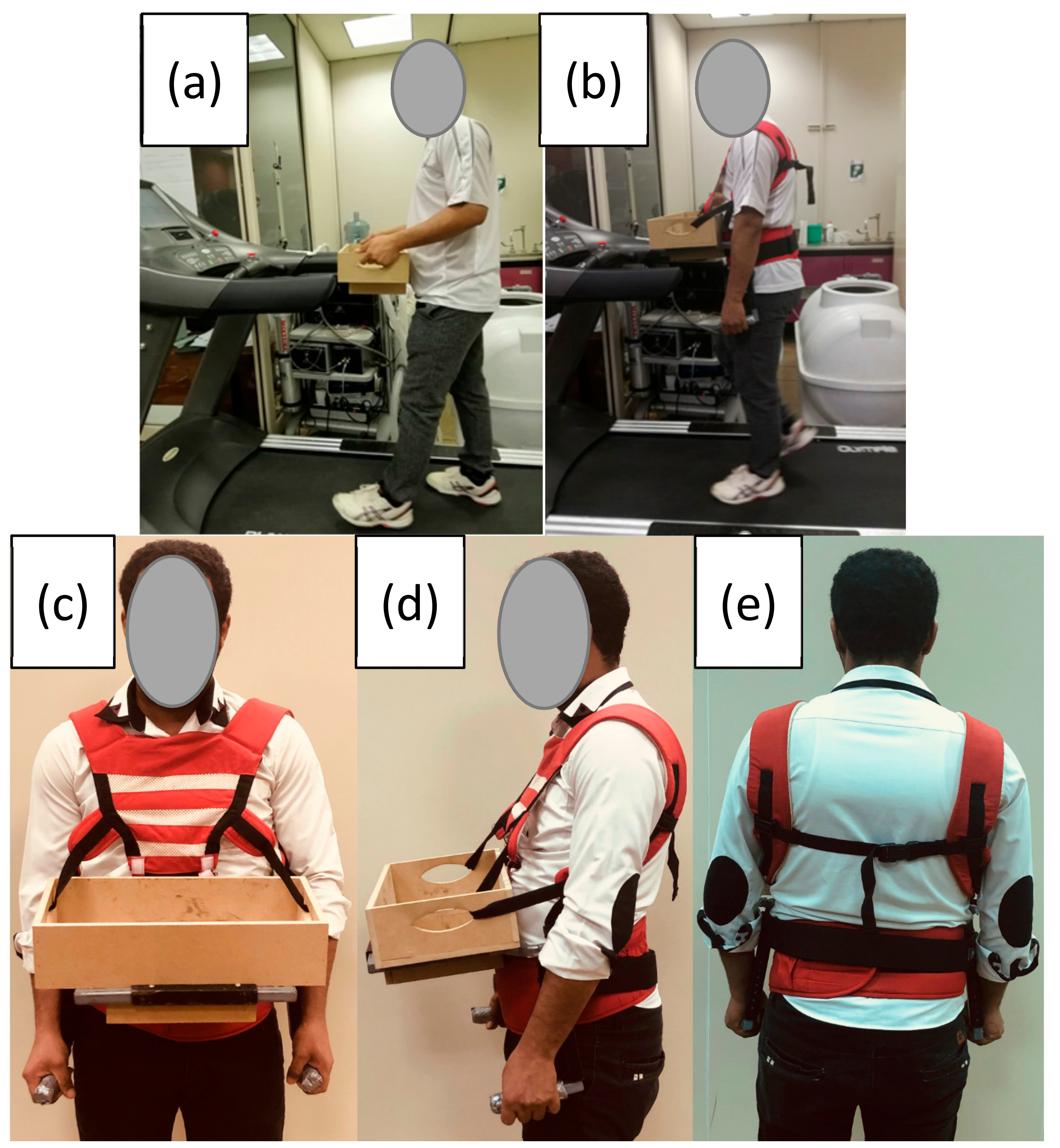
2.1. The Aid Design Requirements and Development
2.2. Participants
2.3. Task Description
2.4. Independent Variables
2.5. Procedures and Data Collection
2.6. Dependent Variables
2.7. Statistical Analysis of Data
3. Results
3.1. Median Loading Metrics (50th Percentile nEMG)
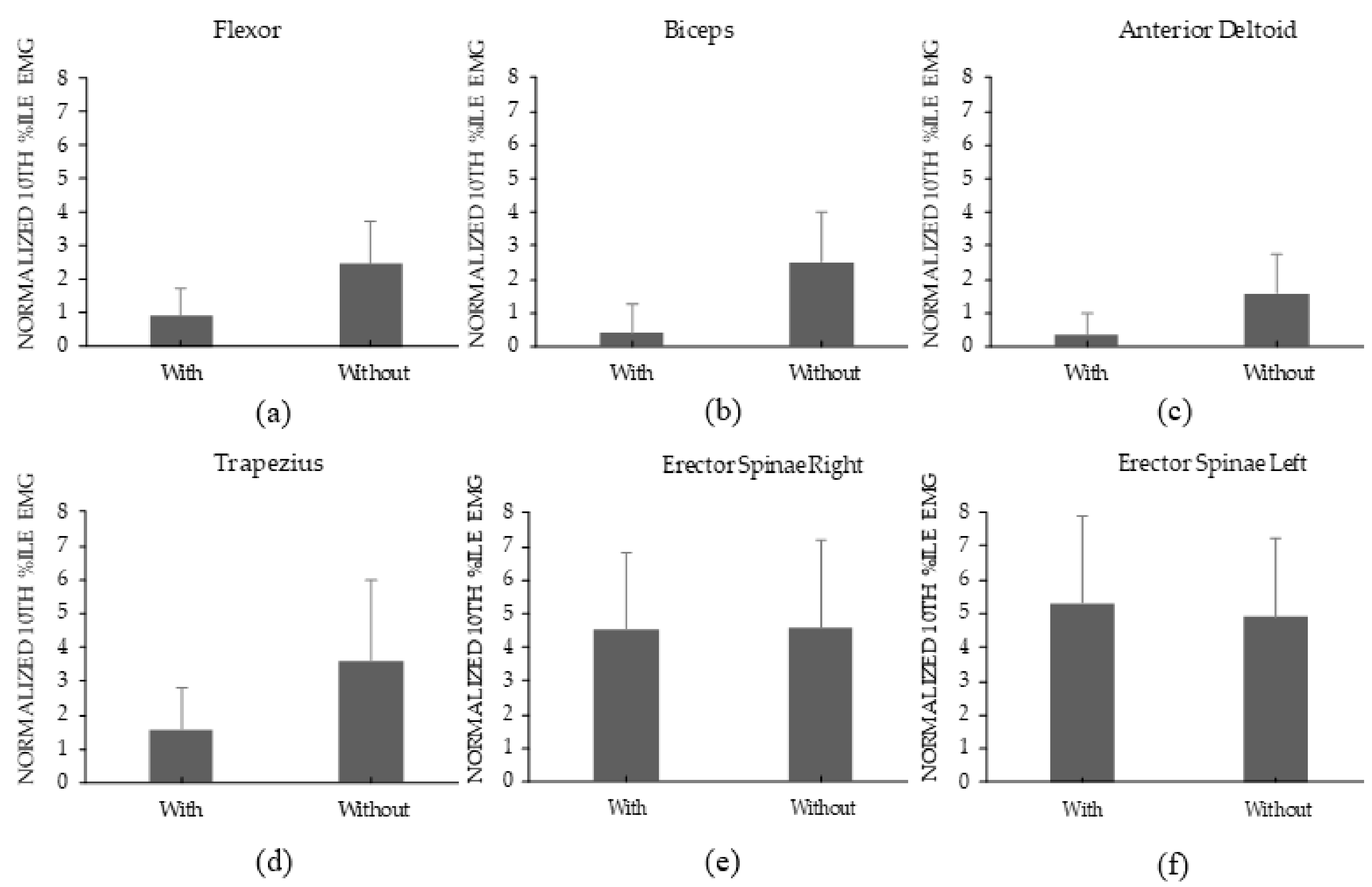
3.2. Static Loading Metrics (10th Percentile nEMG)
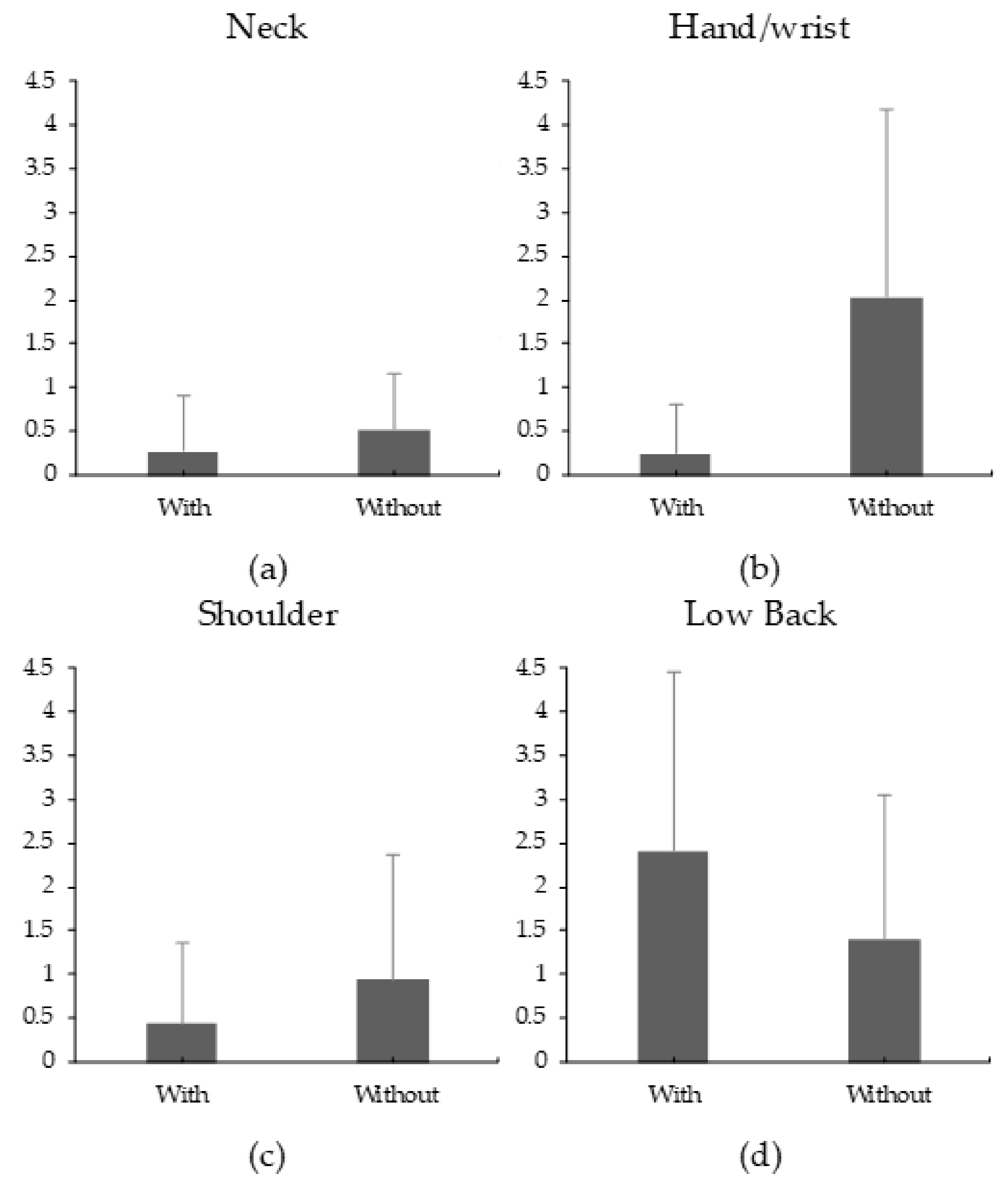
3.3. Rating of Perceived Discomfort
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rajesh, R. Manual Material Handling: A Classification Scheme. Procedia Technol. 2016, 24, 568–575. [Google Scholar] [CrossRef]
- Texas Department of Insurance. Manual Material Handling. Int. J. Sci. Res. 2009, 2, 153–154. [Google Scholar]
- Huysamen, K.; de Looze, M.; Bosch, T.; Ortiz, J.; Toxiri, S.; O’Sullivan, L.W. Assessment of an Active Industrial Exoskeleton to Aid Dynamic Lifting and Lowering Manual Handling Tasks. Appl. Ergon. 2018, 68, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Kram, R. Carrying Loads with Springy Poles. J. Appl. Physiol. 1991, 71, 1119–1122. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.K. Dibble Sticks, Donkey, and Diesels. Machines in Crop Production; International Rice Research Institute: Metro Manila, Philippines, USA, 1990. [Google Scholar]
- Lahiri, S.; Tempesti, T.; Gangopadhyay, S. Is There an Economic Case for Training Intervention in the Manual Material Handling Sector of Developing Countries? J. Occup. Environ. Med. 2016, 58, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Yentes, J.; Rosen, A.; Grindstaff, T.L. An Investigation in Muscle Activation during Load Carrying. Ph.D. Thesis, University of Nebraska-Lincoln, Lincoln, NE, USA, April 2017. [Google Scholar]
- Ciriello, V.M.; Snook, S.H.; Hashemi, L.; Cotnam, J. Distributions of Manual Materials Handling Task Parameters. Int. J. Ind. Ergon. 1999, 24, 379–388. [Google Scholar] [CrossRef]
- Jaenen, S. Identification of Common Military Tasks. Optimizing Operational Physical Fitness. 2009, 8, 1–6. [Google Scholar]
- Golriz, S.; Walker, B. Can Load Carriage System Weight, Design and Placement Affect Pain and Discomfort? A Systematic Review. J. Back Musculoskelet. Rehabil. 2011, 24, 1–16. [Google Scholar] [CrossRef] [Green Version]
- van Vuuren, B.J.; Becker, P.J.; van Heerden, H.J.; Zinzen, E.; Meeusen, R. Lower Back Problems and Occupational Risk Factors in a South African Steel Industry. Am. J. Ind. Med. 2005, 47, 451–457. [Google Scholar] [CrossRef]
- Meislin, R.J.; Sperling, J.W.; Stitik, T.P. Persistent Shoulder Pain: Epidemiology, Pathophysiology, and Diagnosis. Am. J. Orthop. (Belle Mead NJ) 2005, 34 (Suppl. 12), 5–9. [Google Scholar]
- Davis, M.A.; Onega, T.; Weeks, W.B.; Lurie, J.D. Where the United States Spends Its Spine Dollars. Spine (Phila. Pa 1976) 2012, 37, 1693–1701. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A Systematic Review of the Global Prevalence of Low Back Pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, T.; Jacklyn, G.; Orchard, J.; Passmore, E.; Vos, T.; Freedman, G.; Lim, S.; Punnett, L. The Global Burden of Occupationally Related Low Back Pain: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Coyte, P.C.; Asche, C.V.; Croxford, R.; Chan, B. The Economic Cost of Musculoskeletal Disorders in Canada. Am. Coll. Rheumatol. 1998, 11, 315–325. [Google Scholar] [CrossRef]
- Health and Safety Statistics. Annual Report for Great Britain 2013/14; Health and Safety Executive: London, UK, 2013.
- Gillette, J.C.; Stevermer, C.A.; Meardon, S.A.; Derrick, T.R.; Schwab, C.V. Upper Extremity and Lower Back Moments during Carrying Tasks in Farm Children. J. Appl. Biomech. 2009, 25, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.H.; Yeh, Y.C. Effects of Carrying Handles, Postures, Materials and Distances on Carrying Capability. Int. J. Occup. Saf. Ergon. 2015, 21, 250–255. [Google Scholar] [CrossRef]
- Meyers, J.M.; Miles, J.A.; Faucett, J.; Janowitz, I.; Tejeda, D.G.; Weber, E.; Smith, R.; Garcia, L. Priority Risk Factors for Back Injury in Agricultural Field Work: Vineyard Ergonomics. J. Agromed. 2001, 8, 39–54. [Google Scholar] [CrossRef]
- Schertzer, E.; Riemer, R. Metabolic Rate of Carrying Added Mass: A Function of Walking Speed, Carried Mass and Mass Location. Appl. Ergon. 2014, 45, 1422–1432. [Google Scholar] [CrossRef]
- Wu, S.-P.; Chen, C.-C. Psychophysical Determination of Load Carrying Capacity for a 1-h Work Period by Chinese Males. Ergonomics 2001, 44, 1008–1023. [Google Scholar] [CrossRef]
- Wu, S.P. Psychophysically Determined 1-h Load Carrying Capacity of Chinese Females. Int. J. Ind. Ergon. 2006, 36, 891–899. [Google Scholar] [CrossRef]
- Legg, S.J.; Mahanty, A. Comparison of Five Modes of Carrying a Load Close to the Trunk. Ergonomics 1985, 28, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M.; Neumann, D.A. The Effects of Load Placement on the EMG Activity of the Low Back Muscles during Load Carrying by Men and Women. Ergonomics 1987, 30, 1413–1423. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.D.; Mendel, E.; Marras, W.S. Carrying and Spine Loading. Ergonomics 2013, 56, 1722–1732. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.M.; Meador, K.A.; McClure, L.R.; Makrozahopoulos, D.; Brooks, D.J.; Mirka, G.A. A Biomechanical Analysis of Anterior Load Carriage. Ergonomics 2007, 50, 2104–2117. [Google Scholar] [CrossRef] [PubMed]
- Muslim, K.; Nussbaum, M.A. The Effects of a Simple Intervention on Exposures to Low Back Pain Risk Factors during Traditional Posterior Load Carriage. Appl. Ergon. 2017, 59, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Smallman, C.L.W.; Graham, R.B.; Stevenson, J.M. The Effect of an On-Body Assistive Device on Transverse Plane Trunk Coordination during a Load Carriage Task. J. Biomech. 2013, 46, 2688–2694. [Google Scholar] [CrossRef] [PubMed]
- Gregorczyk, K.N.; Hasselquist, L.; Schiffman, J.M.; Bensel, C.K.; Obusek, J.P.; Gutekunst, D.J. Effects of a Lower-Body Exoskeleton Device on Metabolic Cost and Gait Biomechanics during Load Carriage. Ergonomics 2010, 53, 1263–1275. [Google Scholar] [CrossRef]
- Muslim, K.; Nussbaum, M.A. Traditional Posterior Load Carriage: Effects of Load Mass and Size on Torso Kinematics, Kinetics, Muscle Activity and Movement Stability. Ergonomics 2016, 59, 99–111. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.G.; Sun, S.Q.; Goonetilleke, R.S.; Chow, D.H.K. Effect of an On-Hip Load-Carrying Belt on Physiological and Perceptual Responses during Bimanual Anterior Load Carriage. Appl. Ergon. 2016, 55, 133–137. [Google Scholar] [CrossRef]
- Kudryk, I.A. A Biomechanical Analysis of a Specialized Load Carriage Technique and the Development of an Assistive Load Carriage Device. Master’s Thesis, Queen’s University, Kingston, ON, Canada, 2008. [Google Scholar]
- Van de Putte, M.; Hagemeister, N.; St-Onge, N.; Parent, G.; de Guise, J.A. Habituation to Treadmill Walking. Biomed. Mater. Eng. 2006, 16, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeni, J.A.; Higginson, J.S. Gait Parameters and Stride-to-Stride Variability during Familiarization to Walking on a Split-Belt Treadmill. Clin. Biomech. 2010, 25, 383–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G.A. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Sood, D.; Nussbaum, M.A.; Hager, K. Fatigue during Prolonged Intermittent Overhead Work: Reliability of Measures and Effects of Working Height. Ergonomics 2007, 50, 497–513. [Google Scholar] [CrossRef]
- Alabdulkarim, S.; Nussbaum, M.A.; Rashedi, E.; Kim, S.; Agnew, M.; Gardner, R. Impact of Task Design on Task Performance and Injury Risk: Case Study of a Simulated Drilling Task. Ergonomics 2017, 60, 851–866. [Google Scholar] [CrossRef]
- Rashedi, E.; Kim, S.; Nussbaum, M.A.; Agnew, M.J. Ergonomic Evaluation of a Wearable Assistive Device for Overhead Work. Ergonomics 2014, 57, 1864–1874. [Google Scholar] [CrossRef]
- Alabdulkarim, S.; Kim, S.; Nussbaum, M.A. Effects of exoskeleton design and precision requirements on physical demands and quality in a simulated overhead drilling task. Appl. Ergon. 2019, 80, 136–145. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European Recommendations for Surface Electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- De Luca, C.J. The use of surface electromyography in biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef] [Green Version]
- Huysamen, K.; Bosch, T.; de Looze, M.; Stadler, K.S.; Graf, E.; O’Sullivan, L.W. Evaluation of a Passive Exoskeleton for Static Upper Limb Activities. Appl. Ergon. 2018, 70, 148–155. [Google Scholar] [CrossRef]
- Jonsson, B. Measurement and Evaluation of Local Muscular Strain in the Shoulder during Constrained Work. J. Hum. Ergol. (Tokyo) 1982, 11, 73–88. [Google Scholar]
- Bosch, T.; van Eck, J.; Knitel, K.; de Looze, M. The effects of a passive exoskeleton on muscle activity, discomfort and endurance time in forward bending work. Appl. Ergon. 2016, 54, 212–217. [Google Scholar] [CrossRef]
- Kim, S.; Nussbaum, M.A.; Esfahani, M.I.M.; Alemi, M.M.; Jia, B.; Rashedi, E. Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part II–“Unexpected” effects on shoulder motion, balance, and spine loading. Appl. Ergon. 2018, 70, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Alabdulkarim, S.; Nussbaum, M.A. Influences of different exoskeleton designs and tool mass on physical demands and performance in a simulated overhead drilling task. Appl. Ergon. 2019, 74, 55–66. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | Mean (SD) |
|---|---|
| Age (year) | 34.63 (5.54) |
| Weight (kg) | 69.97 (7.85) |
| Height (cm) | 164.66 (4.89) |
| Waist Circumference (cm) | 91.81 (6.13) |
| Body Breadth (cm) | 49.34 (3.26) |
| Waist Height (cm) | 91.97 (3.66) |
| Knuckle Height (cm) | 70.74 (3.47) |
| Response | Trans. | Device | Load | Device Load |
|---|---|---|---|---|
| Flexor | <0.0001 (0.73) | 0.003 (0.18) | 0.21 (0.04) | |
| Biceps | <0.0001 (0.77) | 0.05 (0.08) | 0.18 (0.04) | |
| Anterior Deltoid | <0.0001 (0.70) | 0.004 (0.17) | 0.01 (0.13) | |
| Trapezius | <0.0001 (0.61) | <0.0001 (0.37) | 0.04 (0.09) | |
| Erector Sp. R | (Ln) | 0.79 (0.00) | <0.0001 (0.48) | 0.32 (0.02) |
| Erector Sp. L | 0.10 (0.06) | <0.0001 (0.44) | 0.91 (0.00) |
| Response | Trans. | Device | Load | Device Load |
|---|---|---|---|---|
| Flexor | <0.0001 (0.52) | 0.05 (0.09) | 0.63 (0.01) | |
| Biceps | (Ln) | <0.0001 (0.64) | 0.59 (0.01) | 0.96 (0.00) |
| Anterior Deltoid | <0.0001 (0.52) | 0.13 (0.05) | 0.08 (0.07) | |
| Trapezius | <0.0001 (0.53) | <0.0001 (0.30) | 0.12 (0.05) | |
| Erector Sp. R | 0.40 (0.02) | <0.0001 (0.45) | 0.15 (0.04) | |
| Erector Sp. L | 0.20 (0.04) | <0.0001 (0.39) | 0.09 (0.06) |
| RPD | Trans. | Device | Load | Device Load |
|---|---|---|---|---|
| Neck | Sqrt | 0.014 (0.126) | 0.039 (0.091) | 0.865 (0.001) |
| Shoulders | Sqrt | 0.025 (0.107) | 0.094 (0.061) | 0.702 (0.003) |
| Low Back | 0.012 (0.131) | 0.027 (0.104) | 0.419 (0.014) | |
| Hand/wrist | <0.0001 (0.383) | 0.170 (0.041) | 0.170 (0.040) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alabdulkarim, S.A.; Farhan, A.M.; Ramadan, M.Z. Development and Investigation of a Wearable Aid for a Load Carriage Task. Int. J. Environ. Res. Public Health 2020, 17, 749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030749
Alabdulkarim SA, Farhan AM, Ramadan MZ. Development and Investigation of a Wearable Aid for a Load Carriage Task. International Journal of Environmental Research and Public Health. 2020; 17(3):749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030749
Chicago/Turabian StyleAlabdulkarim, Saad A., Abdulsalam M. Farhan, and Mohamed Z. Ramadan. 2020. "Development and Investigation of a Wearable Aid for a Load Carriage Task" International Journal of Environmental Research and Public Health 17, no. 3: 749. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030749