Equipment Became Better in Backcountry Skiing—Did Severity of Injuries Decrease? An Analysis from the Swiss Alps


Abstract
:1. Introduction
2. Material & Methods
2.1. Analyzed Population
2.2. Data Preparation
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Burtscher, M.; Bachmann, O.; Hatzl, T.; Hotter, B.; Likar, R.; Philadelphy, M.; Nachbauer, W. Cardiopulmonary and metabolic responses in healthy elderly humans during a 1-week hiking programme at high altitude. Eur. J. Appl. Physiol. 2001, 84, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, M.; Gatterer, H.; Flatz, M.; Sommersacher, R.; Woldrich, T.; Ruedl, G.; Hotter, B.; Lee, A.; Nachbauer, W. Effects of modern ski equipment on the overall injury rate and the pattern of injury location in Alpine skiing. Clin. J. Sport Med. 2008, 18, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Moosimann, U. Haftung am Berg. Available online: https://have.ch/fileadmin/_migrated/content_uploads/01_Mosimann_Sicherheit_beim_Bergsport_Version_HAVE.pdf (accessed on 31 January 2020).
- Lamprecht, M.; Fischer, A.; Stamm, H.P. Sport Schweiz 2014: Sportaktivität und Sportinteresse der Schweizer Bevölkerung; Bundesamt für Sport—BASPO: Magglingen, Schweiz, 2014. [Google Scholar]
- Diaz, E.; Ruiz, F.; Hoyos, I.; Zubero, J.; Gravina, L.; Gil, J.; Irazusta, J.; Gil, S.M. Cell damage, antioxidant status, and cortisol levels related to nutrition in ski mountaineering during a two-day race. J. Sports Sci. Med. 2010, 9, 338–346. [Google Scholar] [PubMed]
- Durand, F.; Kippelen, P.; Ceugniet, F.; Gomez, V.R.; Desnot, P.; Poulain, M.; Préfaut, C. Undiagnosed exercise-induced bronchoconstriction in ski-mountaineers. Int. J. Sports Med. 2005, 26, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez Martín, M.; Romero Colás, S.; Calvo Martínez de Laguna, T.; Fernández Garcés, F.; Vicente González, J. Hematologic repercussions of physical exercise in the mountains. Sangre (Barc). 1989, 34, 267–270. [Google Scholar] [PubMed]
- Praz, C.; Léger, B.; Kayser, B. Energy expenditure of extreme competitive mountaineering skiing. Eur. J. Appl. Physiol. 2014, 114, 2201–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duc, S.; Cassirame, J.; Durand, F. Physiology of ski mountaineering racing. Int. J. Sports Med. 2011, 32, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Gross, M.; Lüthy, F.; Kroell, J.; Müller, E.; Hoppeler, H.; Vogt, M. Effects of eccentric cycle ergometry in alpine skiers. Int. J. Sports Med. 2010, 31. [Google Scholar] [CrossRef] [PubMed]
- Schwameder, H.; Schilcher, P.; Ring, S. Energetische Aspekte im Tourenskilauf mit unterschiedlichen Schuh-Bindungssystemen. Spectrume 2005, 1, 79–86. [Google Scholar]
- Tosi, P.; Leonardi, A.; Zerbini, L.; Rosponi, A.; Schena, F. Energy cost and efficiency of ski mountaineering. A laboratory study. J. Sports Med. Phys. Fitness 2010, 50, 400–406. [Google Scholar]
- Vogt, M.; Däpp, C.; Blatter, J.; Hoppeler, H. Training zur Optimierung der Dosierung exzentrischer Muskelaktivität. Schweizerische Zeitschrift für Sportmedizin und Sporttraumatologie 2003, 51, 188–191. [Google Scholar]
- Winkler, K.; Brehm, H.P.; Haltmeier, J. Bergsport Winter; SAC-Verlag: Bern, Schweiz, 2008. [Google Scholar]
- Winkler, K.; Brehm, H.P.; Haltmeier, J. Bergsport Sommer; SAC-Verlag: Bern, Schweiz, 2008. [Google Scholar]
- Munter, W. Drei mal drei Reduktionsmethode. Risikomanagement im Wintersport; Tappeiner Verlag: Bozen, Italy, 2017. [Google Scholar]
- Berghold, F.; Brugger, H.; Burtscher, M.; Domej, W.; Durrer, B.; Fischer, R.; Paal, P.; Schaffert, W.; Schobersberger, W.; Sumann, G. Alpin- und Höhenmedizin; Springer: Berlin, Germany, 2015. [Google Scholar]
- Bürki, C.N.; Bridenbaugh, S.A.; Reinhardt, J.; Stippich, C.; Kressig, R.W.; Blatow, M. Imaging gait analysis: An fMRI dual task study. Brain Behav. 2017, 7, e00724. [Google Scholar] [CrossRef] [PubMed]
- Senner, V.; Lehner, S.; Nusser, M.; Michel, F.I. Skiausrüstung und Knieverletzungen beim alpinen Skifahren im Freizeitsport. Eine Expertise zum gegenwärtigen Stand der Technik und deren Entwicklungspotenzial; BfU—Beratungsstelle für Unfallverhütung: Bern, Schweiz, 2014. [Google Scholar]
- Burtscher, M.; Faulhaber, M.; Kornexl, E.; Nachbauer, W. Kardiorespiratorische und metabolische Reaktionen beim Bergwandern und alpinen Skilauf. Wiener Medizinische Wochenschrift 2005, 155, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Schenk, K.; Faulhaber, M.; Gatterer, H.; Burtscher, M.; Ferrari, M. Ski mountaineering competition: Fit for it? Clin. J. Sport Med. 2011, 21. [Google Scholar] [CrossRef]
- Faulhaber, M.; Pocecco, E.; Niedermeier, M.; Ruedl, G.; Walter, D.; Sterr, R.; Ebner, H.; Schobersberger, W.; Burtscher, M. Fall-related accidents among hikers in the Austrian Alps: A 9-year retrospective study. BMJ Open Sport Exerc. Med. 2017, 3, e000304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gschwind, Y.J.; Bridenbaugh, A.S.; Kressig, R.W. Sturz im Alter. In Geriatrische Notfallversorgung: Strategien und Konzepte; Springer: Wien, Austria, 2013. [Google Scholar]
- Lacroix, A.; Kressig, R.W.; Mühlbauer, T.; Brügger, O.; Granacher, U. Wirksamkeit eines Trainingsprogramms zur Sturzprävention: Effekte eines «Best-Practice-Modells» auf intrinsiche Sturzrisikofaktoren bei gesunden älteren Personen; bfu–Beratungsstelle für Unfallverhütung: Bern, Switzerlan, 2016; bfu-Report 74. [Google Scholar] [CrossRef]
- Willick, S.E.; Wagner, G.; Ericson, D.; Josten, G.; Teramoto, M.; Davis, J. Helmet Use and Risk-Taking Behavior Among Skiers and Snowboarders. Clin. J. Sport Med. 2019, 29, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Mosimann, U. Deutlich mehr Unfälle—Bergnotfälle 2018. Alpen 2018, 19, 24–30. [Google Scholar]
- Posch, P.; Ruedl, G.; Eberle, R.; Burtscher, M. Self-Release of Ski Bindings: A Sex Comparison. Snow Sports Trauma and Safety. 2017. [Google Scholar] [CrossRef] [Green Version]
- Posch, M.; Burtscher, M.; Schranz, A.; Tecklenburg, K.; Kenneth, H.; Ruedl, G. Impact of lowering ski binding settings on the outcome of the self-release test of ski bindings among female recreational skiers. J. Sports Med. 2017, 8, 267–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popper, K.R. Logik der Forschung; Mohr Siebeck: Tübingen, Deutschland, 1969. [Google Scholar]
- Schlechtriemen, T.; Burghofer, K.; Lackner, C.K.; Altemeyer, K.H. Validierung des NACA-Score anhand objektivierbarer Parameter. Untersuchung an 104.962 Primäreinsätzen der Jahre 1999–2003 aus der Luftrettung. Notfall + Rettungsmedizin 2005, 8, 96–108. [Google Scholar] [CrossRef]
- Schendera, C.F.G. Datenmanagement und Datenanalyse mit dem SAS-System; Oldenburg: München, Deutschland, 2004. [Google Scholar]
- Schendera, C.F.G. Datenqualität mit SPSS; Oldenburg: München, Deutschland, 2007. [Google Scholar]
- Stier, W. Empirische Forschungsmethoden; Springer: Berlin, Deutschland, 1996. [Google Scholar]
- Arrow, K.J. Essays in the Theory of Risk-Bearing; North-Holland Pub: Amsterdam, North-Holland, 1970. [Google Scholar]
- Mitlgliederzahlen* des Schweizer Alpen-Club SAC von 1863 bis 2010 und Prognose bis 2020. Available online: https://de.statista.com/statistik/daten/studie/599199/umfrage/anzahl-der-mitglieder-des-schweizer-alpen-club-sac/ (accessed on 31 January 2020).
- Österreichisches Kuratorium für Alpine Sicherheit. Skitouren in Zahlen. 2019. Available online: https://www.alpinmesse.info/de/Skitouren-in-Zahlen/ (accessed on 31 January 2020).
- Bianchi, G.; Brügger, O. Unfallgeschehen beim Ski-und Snowboardfahren in der Schweiz: Unfallausmass, Risikoabschätzung und Entwicklung; BfU—Beratungsstelle für Unfallverhütung: Bern, Scheweiz, 2016. [Google Scholar]
- Lawinenprävention. Available online: https://www.slf.ch/fileadmin/user_upload/WSL/Publikationen/Sonderformate/pdf/20180914_Lawinenfolder_d_achtung_lawinen.pdf (accessed on 31 January 2020).
- Meteoswiss. Available online: https://www.meteoswiss.admin.ch/home/climate/the-climate-of-switzerland.html (accessed on 31 January 2020).



{kind=link}
{kind=link}
| Score | Description |
|---|---|
| NACA 0 | No injury or disease. For example wrong alarm call |
| NACA I | Minor disturbance. No medical intervention is required. For example, slight abrasion. |
| NACA II | Slight to moderate disturbance. Outpatient medical investigation, but usually no emergency medical measures are necessary. For example, fracture of a finger bone, moderate cuts, moderate dehydration. |
| NACA III | Moderate to severe but not life-threatening disorder. Stationary treatment required, often emergency medical measures on the site. For example, femur fracture, milder stroke, smoke inhalation. |
| NACA IV | Serious incident where rapid development into a life-threatening condition cannot be excluded. In the majority of cases, emergency medical care is required. For example, vertebral injury with neurological deficit, severe asthma attack; drug poisoning. |
| NACA V | Acute danger. For example, third grade skull or brain trauma, severe heart attack. |
| NACA VI | Respiratory and or cardiac arrest. |
| NACA VII | Death |
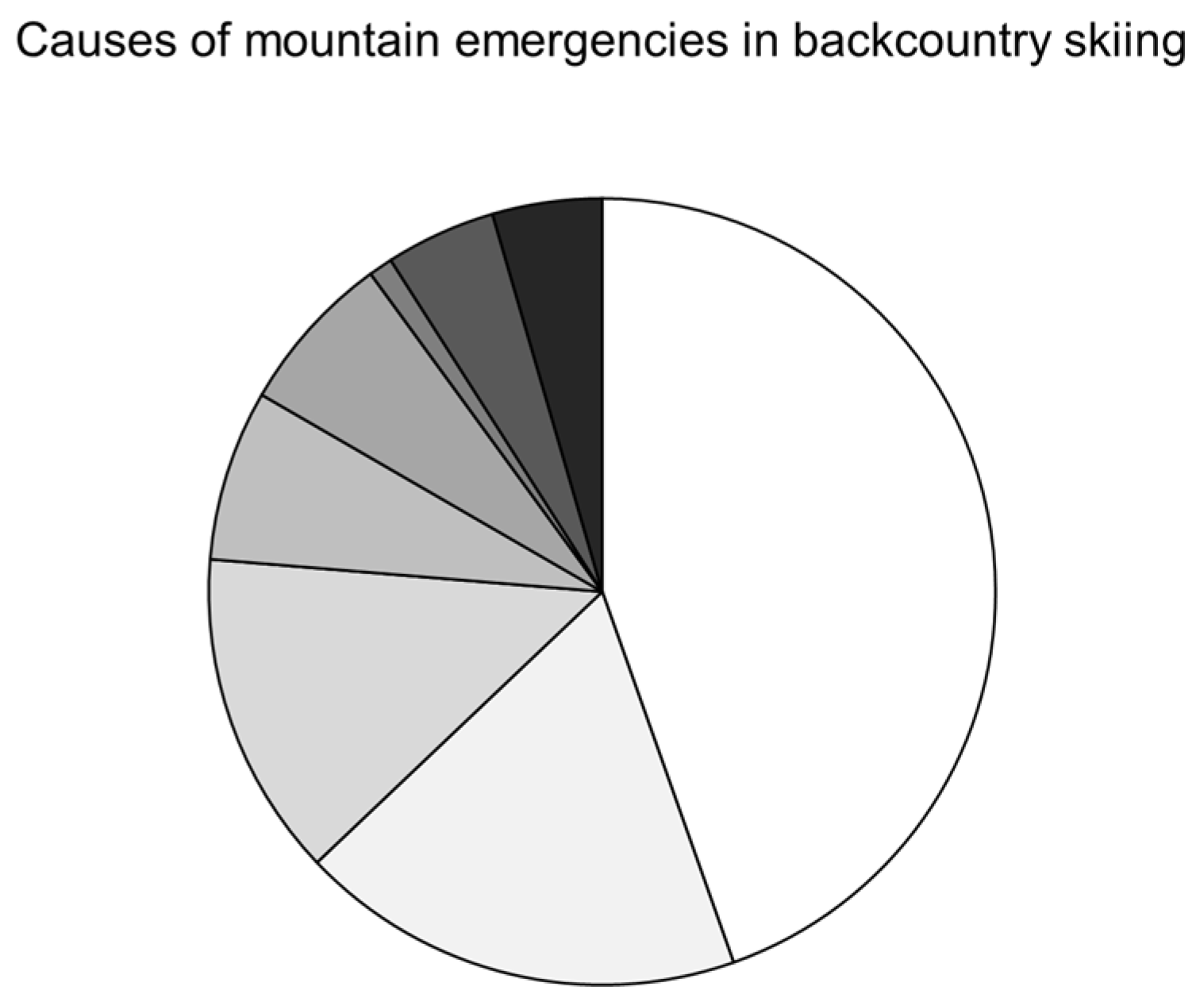
| All Events | Blocking | Losing Way | Illnesses | Falls | Avalanches | |
|---|---|---|---|---|---|---|
| 2009 | 258 | 30 | 33 | 15 | 110 | 46 |
| 2010 | 330 | 40 | 25 | 18 | 119 | 93 |
| 2011 | 281 | 35 | 26 | 21 | 110 | 55 |
| 2012 | 260 | 42 | 20 | 12 | 120 | 32 |
| 2013 | 349 | 54 | 22 | 26 | 140 | 78 |
| 2014 | 314 | 46 | 16 | 25 | 154 | 107 |
| 2015 | 320 | 31 | 25 | 23 | 138 | 67 |
| 2016 | 324 | 40 | 16 | 33 | 145 | 56 |
| 2017 | 281 | 27 | 4 | 19 | 150 | 36 |
| 2018 | 369 | 60 | 15 | 22 | 167 | 57 |
| Average per year | 309 ± 37 | 41 ± 11 | 20 ± 8 | 21 ± 6 | 135 ± 20 | 63 ± 24 |
| Coefficient of determination | 0.2486 | 0.0798 | 0.6494 | 0.2498 | 0.825 | 0.0151 |
| B-estimator | 6.15 | 0.0798 | −2.121 | 0.981 | 5.897 | −0.9758 |
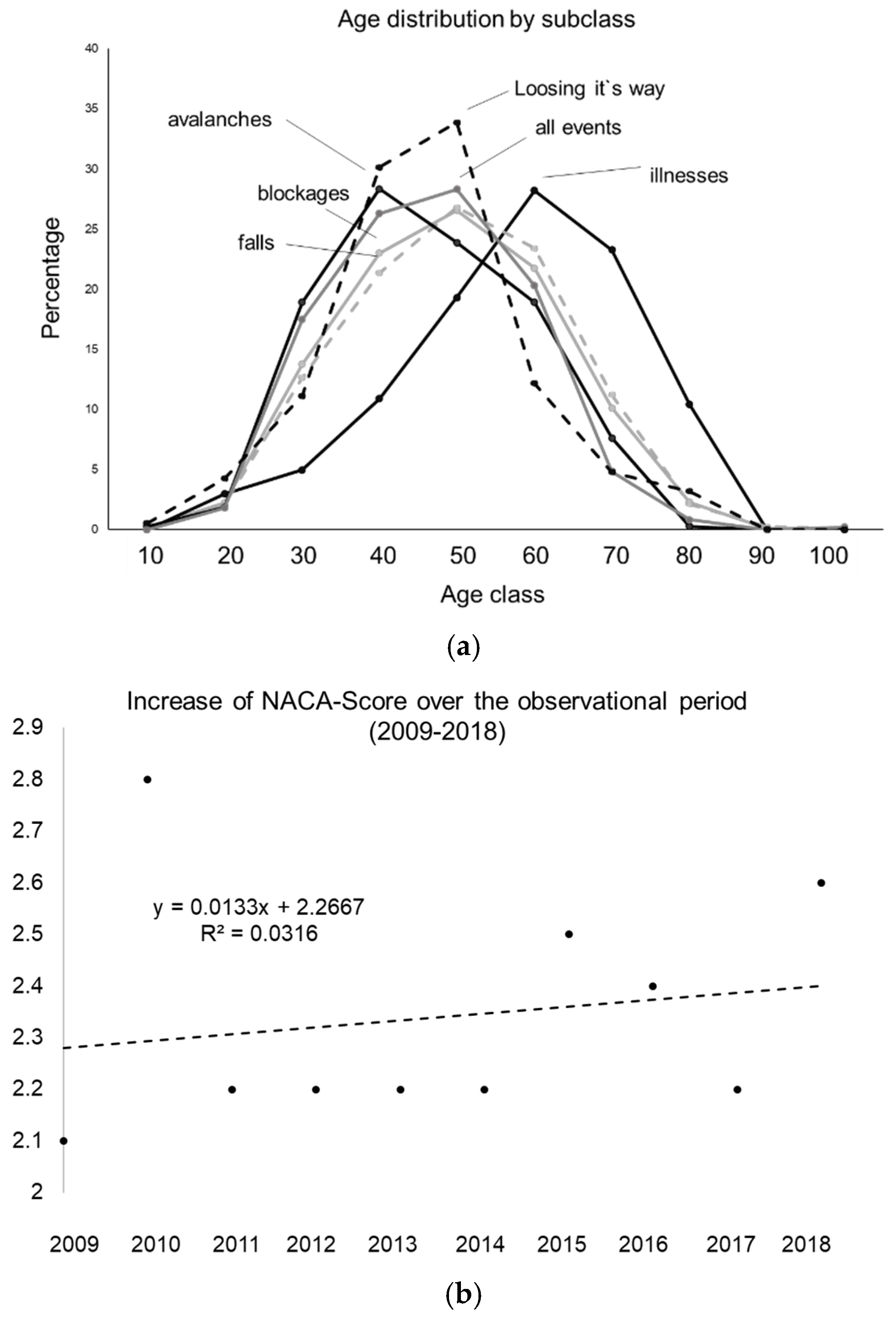
| All Events | Blocking | Falls | Loosing Way | Illnesses | Avalanches | |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| 2009 | 2.1 ± 1.8 | 0.1 ± 0.4 | 2.7 ± 1 | 0.1 ± 0.4 | 3.1 ± 1.5 | 2.6 ± 2.8 |
| 2010 | 2.8 ± 2.1 | 0.2 ± 0.5 | 2.6 ± 0.9 | 0.04 ± 0.2 | 4.2 ± 2.0 | 3.2 ± 2.8 |
| 2011 | 2.2 ± 2.1 | 0.1 ± 0.4 | 2.8 ± 1 | 0.7 ± 2 | 3.7 ± 2 | 3 ± 3 |
| 2012 | 2.2 ± 1.9 | 0.1 ± 2.1 | 2.6 ± 1.5 | 0.1 ± 0.2 | 3.8 ± 1.7 | 3.8 ± 3 |
| 2013 | 2.2 ± 1.8 | 0.1 ± 0.4 | 2.8 ± 0.8 | 0.3 ± 0.8 | 3.1 ± 1.7 | 2.9 ± 2.5 |
| 2014 | 2.2 ± 1.9 | 0.3 ± 1.1 | 2.9 ± 0.9 | 0.4 ± 1.8 | 3.3 ± 2.1 | 3.6 ± 2.4 |
| 2015 | 2.5 ± 2.0 | 0.3 ± 0.7 | 2.9 ± 1.0 | 0.6 ± 1.3 | 4.1 ± 1.9 | 3.4 ± 2.8 |
| 2016 | 2.4 ± 1.8 | 0.5 ± 0.9 | 2.8 ± 0.9 | 0 ± 0 | 3.7 ± 1.8 | 3 ± 2.7 |
| 2017 | 2.2 ± 1.6 | 0.1 ± 0.4 | 2.8 ± 1 | 0.3 ± 0.5 | 3.2 ± 1.1 | 2.6 ± 2.6 |
| 2018 | 2.6 ± 2.1 | 1.3 ± 2.4 | 3 ± 1.2 | 1 ± 1.1 | 4.3 ± 2.2 | 3.6 ± 2.4 |
| Effect sizes | 0.263 | 0.857 | 0.272 | 1.2 | 0.648 | 0.384 |
| Mean ± SD | 2.3 ± 0.2 | 0.3 ± 0.4 | 2.8 ± 0.1 | 0.3 ± 0.3 | 3.7 ± 0.5 | 3.2 ± 0.4 |
| Beta-estimator | 0.0133 | 0.079 | 0.0309 | 0.0486 | 0.0297 | 0.0261 |
| Coefficient of determination | 0.0316 | 0.403 | 0.529 | 0.2034 | 0.0386 | 0.035 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasser, B. Equipment Became Better in Backcountry Skiing—Did Severity of Injuries Decrease? An Analysis from the Swiss Alps. Int. J. Environ. Res. Public Health 2020, 17, 901. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030901
Gasser B. Equipment Became Better in Backcountry Skiing—Did Severity of Injuries Decrease? An Analysis from the Swiss Alps. International Journal of Environmental Research and Public Health. 2020; 17(3):901. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030901
Chicago/Turabian StyleGasser, Benedikt. 2020. "Equipment Became Better in Backcountry Skiing—Did Severity of Injuries Decrease? An Analysis from the Swiss Alps" International Journal of Environmental Research and Public Health 17, no. 3: 901. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030901