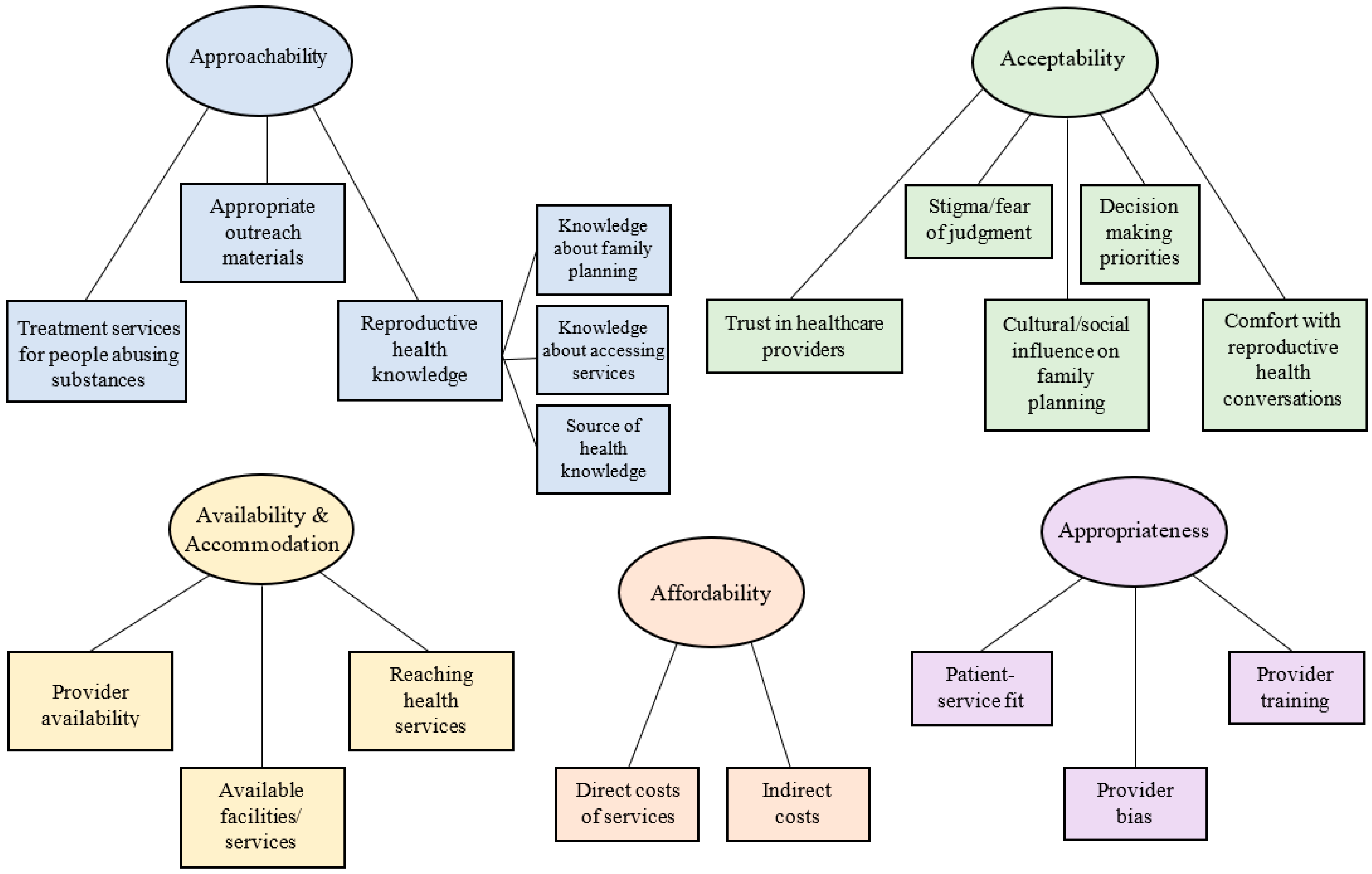
Our findings, which are discussed below, are categorized into the five overarching themes that represent the aspects of healthcare access conceptualized by Levesque, Harris, and Russell (2013) [
4], as well as subthemes that emerged within each of these overarching categories. A graphic representation of these findings is shown in a thematic map in
Figure 1, and a description of the a priori themes alongside the subthemes we identified are shown in
Table 1.
The five overarching themes (approachability/ability to perceive the need for care; acceptability/ability to seek care; availability and accommodation/ability to reach care; affordability/ability to pay for care; and appropriateness/ability to engage in care), which are described in detail below, are distinct from one another, although they also contain overlapping elements. For example, while the availability/accommodation and affordability themes both refer to transportation as a potential barrier to care, the affordability theme refers specifically to the ability to afford the costs of care, including expenses related to transportation to care while the availability/accommodation theme refers specifically to being able to be physically present at a health facility, where convenience and availability of services are largely the barriers to care.
3.1. Approachability
The approachability theme referred to community members’ ability to perceive the need for health services and to identify that such services exist and can impact people’s health. Quotes coded as approachability mentioned transparency of information, provider outreach activities, screening procedures, or patient health literacy or expectations as issues that stakeholders believed would prevent Appalachian people in their own communities from being able to perceive the need for healthcare and therefore be able to approach family planning services. These issues related to community members being able to identify that a form of service exists and is important for their health.
3.1.1. Treatment Services for People Abusing Substances
The treatment services for people abusing substances subtheme captured stakeholder comments about Appalachian people who abuse substances, particularly opioids, being able to perceive the need for family planning and substance abuse treatment services. One participant mentioned that community members who need substance abuse treatment may not know what services to pursue if they were to get pregnant, stating that it is necessary to ask patients if they “have a plan for addiction recovery if [they] do become pregnant, because there’s different options…Is there a plan with it, and do they seek [treatment] options throughout the plan?”
Another participant commented that sometimes treatment services for people using substances focus almost solely on drug treatment, while other services, including contraception, are an afterthought, which can lead to unplanned pregnancies, especially in circumstances when community members may be trading sex for drugs or money. This participant stated:
Like that pattern of the drug-seeking being the primary focus and birth control is not an issue. And sometimes that means I get high, and I had sex, and end up pregnant or sometimes I had sex to get my drugs, then I end up pregnant.
Participants also discussed the impact of NAS in the Appalachian region, commenting on the importance of spreading information to help educate the public and prevent NAS cases. One participant stated, “there’s a huge awareness piece right now in the [blank] County area about reducing neonatal abstinence syndrome, the impact of neonatal abstinence syndrome.” Similarly, another stakeholder commented, “I think this region [in Appalachia], in particular, is really becoming very aware about neonatal abstinence syndrome in correlation to substance use and family planning. A lot of people are trying to help with NAS in a variety of different ways.” These quotes demonstrate that stakeholders in Appalachia have identified a lack of information as an issue related to high NAS rates and are working to provide information to this community, which would allow community members to perceive the need for certain family planning and/or substance use services.
3.1.2. Appropriate Outreach Materials
Stakeholders also discussed the importance of healthcare providers disseminating appropriate reproductive health outreach materials to the community, in order to help them perceive the need for contraception and family planning care. Specifically, participants commented on the importance of outreach materials matching the reading and health literacy level of the community members they are trying to reach. One participant described working with a health literacy team to ensure that outreach materials were appropriate, stating:
I know for a lot of patient education materials I’ve had to create, we have connected with our health literacy team, and we realized that we were writing education materials at a college reading level, and they helped us change wording around to get it closer to that target 6th-grade reading level.
Another participant reiterated this comment, describing the importance of ensuring that “the material provided to [community members] for educational purposes [is] understandable to them.”
Participants also connected this issue to community members in need of both substance use and family planning services, describing the need to assess whether a “written handout for education, was…understandable as it relates to [both] addiction and carrying a pregnancy. The risks, benefits of going to something like Subutex. [Do] they feel like they got good information to make decisions, and understand?”
3.1.3. Reproductive Health Knowledge
Many participants described how a lack of reproductive health knowledge can be a barrier to Appalachian community members’ ability to perceive the need for health services. The stakeholders explained that knowledge about family planning, knowledge about accessing health services, and the source of health information are all important aspects of reproductive health knowledge. As shown in the quotes below, the stakeholders described how, in order to perceive the need for healthcare and the effectiveness of health services, Appalachian community members need to understand the concept of family planning and the purpose of reproductive health services and be able to identify how to access such services. Additionally, the source and frequency of exposure to this information are important, because different sources have different perceived authority and motives, which may impact a community member’s ability to accurately perceive the need for services.
Knowledge about Family Planning
Participants explained that, in order to understand Appalachian community members’ ability to perceive the need for health services, it is important to begin by understanding what the term “family planning” means to these community members. For example, several participants commented that the meaning of the term “family planning” may not be clear to all Appalachian community members, with one participant stating:
I don’t think a lot of people even know what family planning is or the definition of that, cause that’s not language they hear or [were] taught in school or at home. So you know, what we consider family planning, I don’t think would ever come across their mind as family planning.
Other participants extended this comment to community members who may fail to realize that family planning means more than birth control, with one participant stating:
When students do speak about it to me, or even just people in general in the community, it’s usually just birth control. That’s all I hear about, the birth control aspect. And it’s not saying not wanting to get pregnant, it’s just always just birth control. They don’t talk about safe sex, they don’t talk about STD testing or all these different things that they could receive at a family planning clinic or at a Planned Parenthood; they just think birth control or abortion, automatically.
Participants also shared stories about their own experiences and those of other Appalachian people. One stakeholder shared that they had worked with 18- and 19-year old college women who:
…didn’t know basic health, reproductive health…they don’t even know….that birth control can be used for more than just preventing pregnancy…I had several girls that did not realize that birth control can be used to help with medical conditions related to reproductive health.
These quotes emphasize the need for community members to learn about reproductive health and family planning and understand that it encompasses multiple options in order to perceive the need for these health services.
Knowledge about Accessing Services
The stakeholders also identified knowledge about accessing health services as an important factor in community members’ ability to perceive the need for healthcare. One participant commented that it is important to better understand whether people “know where to go to…access family planning [services].” Another participant built on this comment as it pertains to accessing abortion care, questioning whether Appalachian community members:
…even know where to go [for abortions]? Do they even know there [are] two forms? There’s the surgical, and then there’s the abortion pill. Cause now, people really confuse…Plan B with the abortion pill. They tend to go to Walmart and [try] get [the abortion pill] over the counter, and it’s like no. That’s not the way it works.
3.2. Acceptability
The acceptability theme referred to community members’ ability to seek or pursue healthcare. Quotes categorized under this theme mentioned personal or community values, social norms, culture, or gender as issues that kept people from seeking healthcare services. These issues related to cultural and social factors that determined Appalachian community members’ ability to accept aspects of health services and service providers, such that they choose to pursue healthcare.
3.2.1. Trust in Healthcare Providers
The trust in healthcare providers subtheme captured information about how trust or lack of trust in healthcare providers may influence a community members’ ability to seek care. This issue is related to provider outreach regarding the types of services they provide, community members’ comfortability discussing health issues with a provider, and the confidentiality of services. The stakeholders reported that without these pieces present, community members may lack trust in their providers, which can influence peoples’ ability to seek family planning services. One participant reported that community members have trouble opening up to healthcare providers whom they do not trust because they fear getting a lecture. That participant stated:
I think people don’t feel like they can trust their provider…they’re always gonna get that lecture. They’re always gonna get that talk, you know. ‘Why [are] you sexually active?,’ ‘Why [are] you doing this?,’ Or, ‘why [are] you doing that?’ So just that level of trust.
Another participant commented on issues of trust that arise in small, rural communities, where community members may avoid acknowledging their health issues out of fear that their healthcare provider will not keep their treatment confidential. This stakeholder commented that research with this population should ask community members:
…‘do you have any providers that you trust in your community?’ And, ‘do you trust the confidentiality of those services?’ Because there are a lot of small communities around here, and [people might wonder,] ‘if I go to the health department is everybody going to know I have hep C?’
Participants also discussed trust in healthcare providers as it pertained to the intersection of family planning and substance use issues, noting that some Appalachian community members fear that providers may betray their trust by reporting their substance use during pregnancy to authorities. One participant stated:
…there’s a lot of fear around talking about pregnancy and drug use together. What that could mean for themselves, and if they’re going to be in danger. And I think it’s pretty similar to other areas of, you hear anything about pregnancy or reproductive health and drug use together, and you get nervous. I think there’s a lot of fear around this.
Community stakeholders noted that such a lack of trust in healthcare providers can keep members of their community who use substances from understanding and seeking care related to pregnancy.
3.2.2. Stigma/Fear of Judgment
The stigma/fear of judgment subtheme captured participants’ comments related to barriers to Appalachian community members seeking care because of the stigmatized nature of their health concerns, which can lead to a fear of being judged by healthcare providers or others in the community. Participants discussed stigma in Appalachia related to sex and reproductive health topics, with one participant stating:
I think a problem with this area is people choose not to go [to the doctor] because they feel like they’re really judged because they’re going and asking those [reproductive health] questions, then they know they’re gonna get a very judgmental body language back. Or just an answer back that is not an answer they need.
Participants felt that fear of discussing stigmatized health topics with a healthcare provider prevented Appalachian community members from seeking care.
The stakeholders also discussed the stigmatized nature of opioid use, especially among pregnant community members. For these people, seeking care may be especially frightening because they fear both provider judgment and possible legal action. One participant stated:
One of the biggest issues, especially, with the opioid recovery, is…them not coming in for initial family planning, but also when they do discover that they’re pregnant, not seeking treatment because they’ll have to take a drug test. Then what happens from that? Will they be in trouble, or will they be judged, or what happens?
Similarly, another participant described people in the community “[delaying] care because of fear for judgment during a pregnancy while being a substance…user” and allowing that fear to keep people from going “to the doctor to get prenatal care.”
3.2.3. Cultural/Social Influence on Family Planning
The cultural and social influence on family planning subtheme captures the influence of Appalachian culture and social norms as barriers to Appalachian community members seeking care. In particular, participants discussed religion and “conservative” or “narrow” norms as things that often keep Appalachian community members from seeking family planning services, particularly related to “what women are allowed to do sexually.” One participant stated:
I’ve heard people in the region talk about their fear of using methods to avoid getting pregnant [because of] religious [reasons]. Religion can keep you, a lot of people can think it’s sinful almost to use birth control or something like that, there’s some intersection there.
Participants also discussed social norms around childbearing, which can lead women to feel pressure to have children. One participant stated, “people [may] feel pressured to avoid using contraceptives from their significant other or family members to start a family.” Similarly, participants added that when a partner or family member pressures someone to start a family, that person may avoid seeking care because they do not want their family to know that they are using contraceptives. In addition to issues of confidentiality and trust, this point highlights the importance of, as one participant put it, contraceptive methods that “you [can] hide…from your family or your partner.”
3.2.4. Decision-Making Priorities
The decision-making priorities subtheme captures issues related to what Appalachian community members consider important when making family planning decisions, as these priorities inform their desire and ability to seek health services. As one stakeholder put it:
I think one other thing to consider, especially, is that I think we in this community are so focused sometimes on effectiveness, we forget even maybe about our own experiences with contraception. And we consider lots of things, how will it make my skin look? Or, how it will control menstrual cycles, or how it feels, things like that.
Participants discussed the many benefits and side effects of various contraceptives, pointing out that people have different needs and priorities. Community members’ individual priorities are influenced by the culture they live in and greatly impact their care-seeking. As such, participants suggested that it would be helpful to have Appalachian community members rank their “top priorities for reproductive healthcare and family planning” or report what they “consider when choosing…contraception.” One participant noted, “You might really be surprised at what comes up to the top. I’m sure effectiveness will, but I’m betting it won’t be the only one.”
3.2.5. Comfort with Reproductive Health Conversations
The comfort with reproductive health conversations subtheme describes the ways that Appalachian community members’ ability to seek or pursue family planning services is related to, and often limited by, their levels of comfort discussing these topics, thereby limiting family planning access by limiting the acceptability of these health services. This issue is linked to culture and norms, which impact community members’ values, their perceptions of their needs and the services being offered, and their comfort with seeking health services. Participants discussed how, because of community norms and values, some Appalachian community members may not be comfortable approaching a healthcare provider to discuss family planning or reproductive health.
In discussing this topic, the stakeholders offered several suggestions about how to help community members reach health services despite norms that may make them uncomfortable seeking care. One participant mentioned a successful program in which mothers and daughters attend together and receive reproductive health information. This participant stated:
…[the parents] really enjoy having someone else to do the conversation for them. Cause then if the daughters do too, they feel it’s more comfortable. And it opens [the] door where now they are able to ask those questions and see to it.
Additionally, participants discussed how telehealth and virtual health services can help uncomfortable community members receive care. One participant mentioned that people may be more comfortable using “the internet to explore resources,” and another participant discussed how these resources may be especially helpful for young community members, stating:
They might be more comfortable with that, especially with your mid-20s, mid-30s audience. If they could just go online, college-age kids can talk to that instead of going to their local health department. They might be willing to ask more personal questions or seek birth control after that. Or seek testing after that.
Participants discussed Appalachian community member’s overall lack of comfort with reproductive health and family planning topics, suggesting ways that community programs and online resources might be used to increase community members’ comfort and help them access health services. Overall, stakeholders acknowledged that the acceptability of health services is limited in Appalachia when community members are unable to seek or pursue family planning services because their culture, norms, or values create discomfort with reproductive health conversations.
3.3. Availability and Accommodation
The availability and accommodation theme referred to community members’ ability to reach healthcare services. Quotes coded as availability and accommodation denoted the physical existence of health resources, the geographic location of health services, hours of opening and appointment availability, or the availability of transportation as issues that prevented Appalachian community members from being able to physically reach family planning and substance use services in a timely manner.
3.3.1. Provider Availability
The provider availability subtheme captured participants’ descriptions of community members’ inability to reach services because of a lack of reproductive healthcare providers, many of whom work limited hours in a given community. One participant expressed this point, stating:
One of the things that we have seen here in our rural communities, is access to our providers. While we might have an OBGYN in every county, they’re only in that one county on Monday or let’s say Wednesday, from 10 to 2, and they don’t start taking appointments until Monday, two days beforehand. A lot of times people can’t get in to receive access.
Participants discussed how this issue is related to state-level “budget cuts for family planning,” which vary based on the state and subregion and can lead to “dropping time for [a] provider,” such that a county may have a single provider who “just comes in once a month.” To this point, participants described patients being “stuck sitting in a waiting room waiting for hours to be seen” because of a lack of access to appropriate reproductive healthcare providers. Participants discussed how these issues are especially problematic in rural areas, where “most of the…abortion clinics have been shut down…even when there were more clinics available, they’re hardly ever in a rural area.” Again, the stakeholders suggested that the use of remote or online health services could help community members in some circumstances bypass the provider shortage and access healthcare.
3.3.2. Available Facilities/Services
Similar to the issue of provider availability, participants reported that a lack of available facilities and services prevents many Appalachian community members from reaching reproductive health and substance abuse treatment services. One participant discussed this problem, stating:
One of the biggest problems we face with that, is we don’t have a lot of [substance abuse] recovery facilities outside of [the larger counties]. So, when you get into the rural communities, we have support groups, but we don’t have medical staff. We don’t have the recovery facility that we can connect with, where we could implement the [family planning] program, so we’re looking at how we can further the program in the rural communities.
Similarly, the stakeholders described a lack of available family planning facilities and services, particularly in conservative, rural communities. One participant stated that the nearest abortion clinic is “four and a half hours away from us, and you know you can’t put a brick and mortar clinic here. God knows you can’t do that close to a Southern Baptist around here.” Another participant discussed the influence of policies which impact the availability of family planning services and make reaching healthcare services more difficult, stating that it is:
…important to think about how people might have to cross state lines, and then what state laws also affect their access to family planning, or how their insurance factors into where they have to go, based on if their closest clinic might be across state lines, or if they have to travel further to still use state Medicaid or something like that.
3.3.3. Reaching Health Services
In addition to issues with provider and service availability, the stakeholders reported that Appalachian community members may have trouble reaching reproductive health and substance use services. This subtheme refers to barriers to reaching these services that are related to how far away appropriate services are and a lack of reliable and accessible transportation to reach those services. Participants discussed the difficulty of reaching reproductive healthcare when affordable services are located far away, with one participant stating:
…because when you’re looking at Appalachia, you are looking very much at rural areas where it’s not right across the road, necessarily, to get to a healthcare provider. When you are looking at affordable options, how far are you, or what distance are you to a healthcare provider, whether it be a health department or free, or affordable services.
Another participant described how difficult it is for pregnant women in their community, especially those who use substances, to reach care, stating:
…the local hospital stopped delivering babies. Women could be seen for prenatal care, and then they had to travel at least 45 min to over an hour, depending on where they lived, to actually deliver in a hospital…for high risk, they had to travel [even farther]. Some women, particularly those women with addiction issues, don’t have transportation. They didn’t have cars. They didn’t have resources.
Similarly, the stakeholders discussed various transportation options and the barriers to each for Appalachian community members. They argued for the importance of understanding community members’ access to transportation, with one participant stating, “I think finding out about people’s transportation, and the access that they have is important. Because, especially in our area, we don’t have [an] alternative.” Participants mentioned taxi and ambulance services as possible “transportation options for people without cars, or without money for gas,” but acknowledged the cost of these options and the difficulty of accessing them, with one participant acknowledging that arranging transportation can be challenging by stating that there are “always catches to how you can request [transportation services], and what [exactly] you can request.”
3.4. Affordability
The affordability theme referred to community members’ ability to pay for reproductive health and substance use services. Quotes coded as affordability denoted direct and indirect costs, including opportunity costs, or the lack of appropriate income, social capital, lack of health insurance coverage, or responsibility for co-insurance payments as factors that prevented community members from being able to pay for reproductive health and substance abuse treatment services. These issues related to Appalachian community members’ economic capacity to use time and/or resources on healthcare.
3.4.1. Direct Costs of Services
The direct costs of services subtheme captured participants’ descriptions of Appalachian community members having difficulty affording reproductive health and substance abuse recovery services because of a lack of affordable options, low incomes, or a lack of health insurance. One participant noted affordability as a problem, stating, “financial questions, I think are the thing that consistently comes up for that region.”
Participants specifically mentioned the importance of asking community members, “Can you afford contraception?” because they frequently encounter this barrier to care among people in their area. Another participant mentioned that unplanned pregnancies in the Appalachian region often occur because community members have “no insurance.” Additionally, participants discussed cost as a barrier to abortion services, describing policy barriers that prevent federal or state funds from covering these health services. The stakeholders also described the power of abortion funds (i.e., charitable organizations that provide financial aid to help people pay for unaffordable abortions [
41]) to help community members afford abortion care, with one participant describing the importance of assessing whether Appalachian community members “know if they do qualify for [abortion] funds,” following up that some agencies in the area address affordability of abortion services by “screen[ing] everybody for funding for their abortions.”
3.4.2. Indirect Costs
In addition to direct costs of health services, there are indirect costs associated with reproductive healthcare and substance use treatment, including paying for transportation to health facilities and pharmacies. Participants stated that “the cost of transportation” can prevent Appalachian community members from seeking healthcare. They also noted that healthcare options are often scarce for community members with limited transportation resources while people with financial resources have the luxury of choosing from multiple healthcare options. Along this line, one participant stated, “You have that option if you have the means to go there [to access services that are far away] and get that.” Additionally, participants described working with community members whose lack of resources led them to risk their reproductive health in order to afford transportation to health services and to meet other basic needs, as sex was one of the only resources that they had access to. As one participant stated:
A lot of the women that I worked with who were experiencing homelessness and had issues with addiction, also used sex as a currency. To get drugs, to get a place to stay, to get a ride to the clinic, whatever the case may be.
3.5. Appropriateness
The appropriateness theme referred to community members’ ability to engage in healthcare services. Quotes coded as appropriateness mentioned the technical and interpersonal quality of healthcare, the adequacy of care, care coordination and continuity, lacking feelings of empowerment, or the type of information provided to community members as issues that prevented people from being able to engage with reproductive health and substance use services. These issues related to the fit between the services being provided and Appalachian community members’ needs as well as the level to which patients are involved in decision making and treatment decisions.
3.5.1. Patient-Service Fit
The patient-service fit subtheme captured Appalachian community members’ ability to engage with healthcare providers and the services they provide. Patient-service fit can become a barrier to people’s ability to engage when providers misunderstand or ignore the needs of the communities they serve. For example, participants discussed how providers in Appalachia often do not understand the needs of gender and sexual minorities, reporting that “for transgender men and gender non-conforming folks, …their identity [may have] prevented them from being able to access contraception.” In this example, there is a mismatch between the family planning needs of gender minority patients and the available services, leading to an inability for these patients to engage in appropriate health services.
Participants also focused on the needs of Appalachian community members who use substances but also need reproductive health and family planning services. They mentioned that healthcare providers may fail to acknowledge or address these needs with their patients, thereby preventing community members from engaging in necessary healthcare. One participant discussed the importance of medical professionals addressing substance use with pregnant patients “when they do engage in those kinds of behaviors when they’re pregnant, whether it be opioid use or smoking, or drinking, or tobacco usage of any kind.” Participants also discussed a similar problem in which healthcare providers may offer either reproductive health or substance use recovery services but are ill-equipped to provide both services. The stakeholders noted the inappropriateness of this service gap, especially in the context of the opioid crisis. As one participant stated:
We [in our community] have a program…helping lower the incidences of neonatal abstinence syndrome. And what we learned in the research was the recovery facilities had provided very little information to women who were seeking help through the recovery facilities, to talk about preventing pregnancy. In fact, we actually had several homes tell us that, that was outside of their wheelhouse. And we were like, ‘How can that be outside of your wheelhouse?’ If you’re not telling women how to prevent an unintended pregnancy, and they’re coming up pregnant, and there’s all these pieces that go along with it. And I said, ‘What do you do when they do when they do come to you and they’re pregnant?’ They’re like, ‘Oh, we kick them out of our program.’ And I’m like, ‘What?!’ It’s kind of crazy.
3.5.2. Provider Bias
The provider bias subtheme captured stakeholder descriptions of Appalachian community members’ inability to engage adequately with reproductive healthcare or substance use services when providers do not involve patients in decision making and treatment decisions and instead limit patient autonomy by making assumptions about or even coercing patients into participating or not participating in certain health services. Participants discussed this issue as often related to social norms, providers’ personal values and expectations, and misinformation among providers. One participant discussed their experience with healthcare providers who believe that long-acting reversible contraception (LARC), such as an intrauterine devices (IUD), is the most appropriate family planning service for certain groups of people, regardless of patient desire for this contraceptive method. As this participant stated:
I think it’s much more related to what their [providers’] values are. Sometimes you will have providers that are really committed to wanting to provide good access to all people, regardless of substance use or not. And then you have other providers who maybe will identify and say things like, ‘You know what? [They are a] drug addict, [so] I’m going to push IUDs.’ I’ve heard providers say that. Or, ‘[For] people that are in poverty, I’m going to push IUDs, because I don’t want them to have more kids.’ I don’t think it’s necessarily what their job description is, as much as what their values are. If they’re having a high…[degree of] values against those people, that might affect access.
This participant described certain populations (e.g., people who abuse substances, people living in poverty) that healthcare providers may coerce into using LARCs because they consider these to be populations for which reproduction is undesirable.
Many participants also described healthcare providers “refusing to provide” abortion services as well as other family planning services, such as birth control or emergency contraception, that “they would potentially consider an abortive agent.” As one participant stated, “it might be surprising to find out how many people [are] just actually being flat out denied something they went and asked for.” In addition to refusing to provide requested services, participants discussed healthcare providers in Appalachia who refuse to even mention certain services that they disagree with as potential options for their patients. As one participant stated, “They [healthcare providers] won’t even discuss that [abortion] as an option. They won’t even say you have that option.” Similarly, another participant stated, “there are some physicians that still believe contraception is abortion, so they don’t want to offer it to patients, and they won’t offer it to unmarried patients.”
Participants also described how reproductive healthcare providers sometimes allow their assumptions about their patients to drive which services they offer. In one example, a participant stated:
I have [an overweight] friend once who went to a gynecologist. And when she asked for birth control, the gynecologist looked at her and said, ‘why?’ And she’s like, ‘I’m not sure what you’re...what do you mean why? Because I’m sexually active.’ And the gynecologist actually responded and said, ‘You’re sexually active?’ Like [the gynecologist was] so shocked that a fat person could have sex. But that’s what we’re dealing with.
Here, in a particularly salient quote due to the high rates of obesity in the Appalachian region [
18], a provider allowed their own bias about the sexuality and reproductive health needs of an overweight patient to influence the health services offered to this patient, potentially compromising the patient’s ability to engage in appropriate health services. Thus, the provider bias subtheme refers to Appalachian community members’ inability to engage with health services when healthcare providers’ personal values or biases cause them to provide inappropriate or inadequate services.
3.5.3. Provider Training
The stakeholders also related Appalachian community members’ ability to engage in reproductive health and substance use services to the training and education that their healthcare providers had obtained, discussing how a lack of adequate “provider preparation” can prevent providers from being able to provide appropriate health services. Participants specifically related this issue to provider training about how to provide family planning services. One participant stated, “it seems like family planning is being handed to the primary care providers now, rather than the specialists or the family planning centers.” Participants discussed this as an issue particularly because primary care providers may not be adequately prepared to offer family planning services. As one participant stated, “There is little to no training that’s happening in general around contraceptive counseling…even in medical school.” Participants discussed their concern that ill-prepared healthcare providers were being expected to be primary family planning healthcare providers, which can lead to Appalachian patients receiving poor reproductive healthcare.
Additionally, participants described populations whose needs may not be covered in healthcare provider education, leading to community members who are unable to engage in appropriate healthcare because their providers are not adequately prepared to meet their needs. One example is healthcare providers who are not prepared to work with patients who are transgender. One participant discussed this issue, stating:
So, I’m pretty sure that she probably assumed at that point that [my transgender friend] was gay…I don’t think she knew how to react with her at that point. She’s transgender, she’s not gay. But still, I think it just makes things very complicated that she...I think it is an issue of preparation. Like are our providers really prepared?

 ,
, 



{kind=link}