Predicting Hand Washing and Sleep Hygiene Behaviors among College Students: Test of an Integrated Social-Cognition Model

 , ,
, ,  and
and
Abstract
:1. Introduction
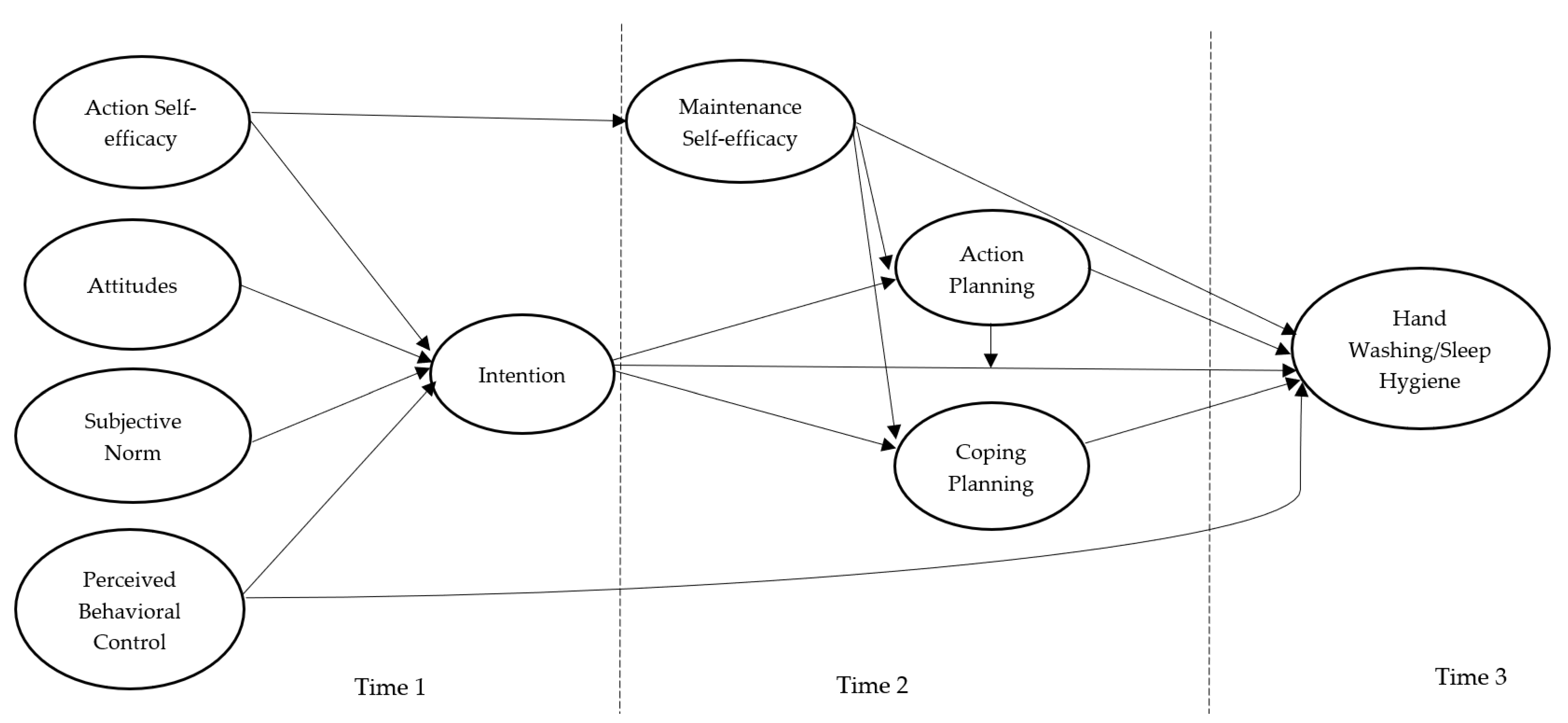
2. The Current Study and Hypotheses
3. Method
3.1. Participants and Procedure
3.2. Measures
3.3. Data Analysis
4. Results
4.1. Preliminary Analyses
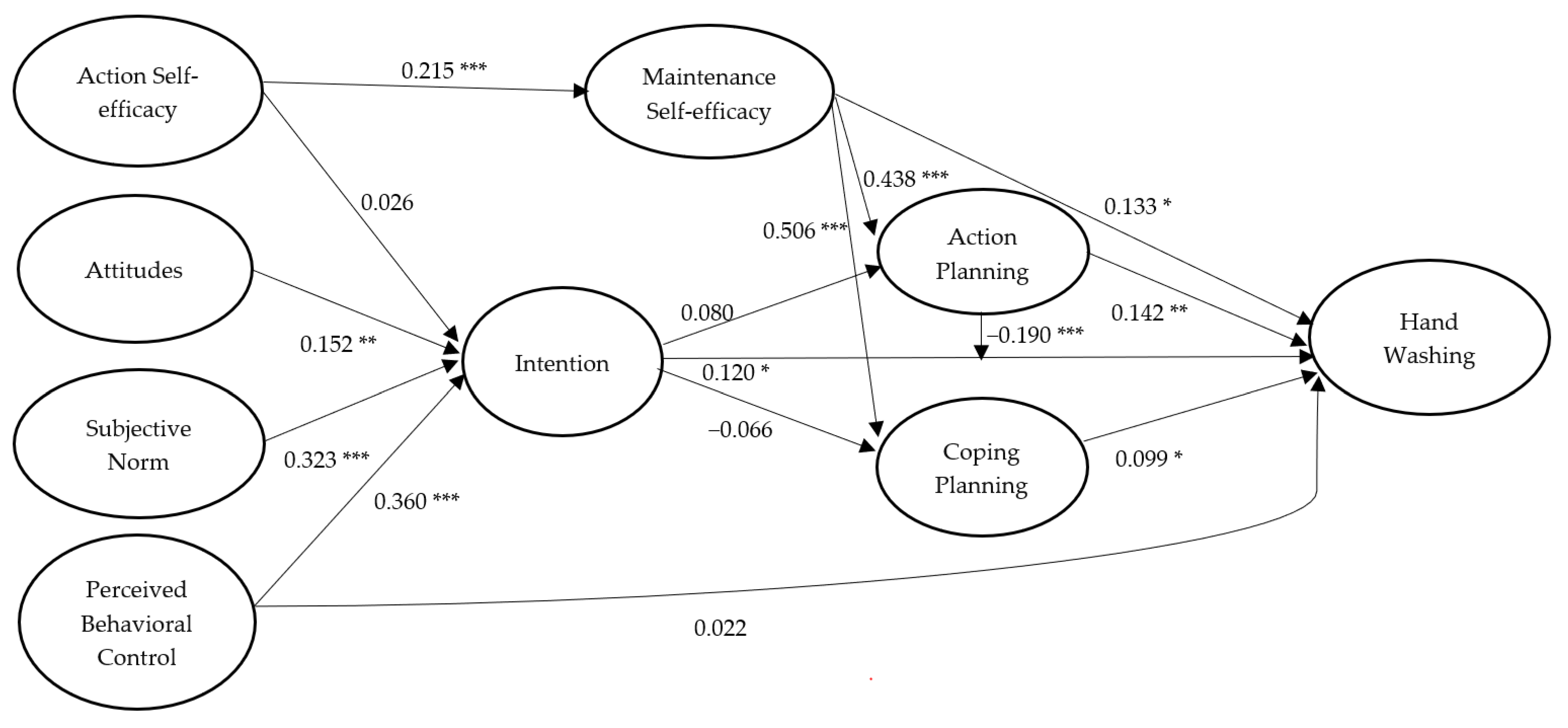
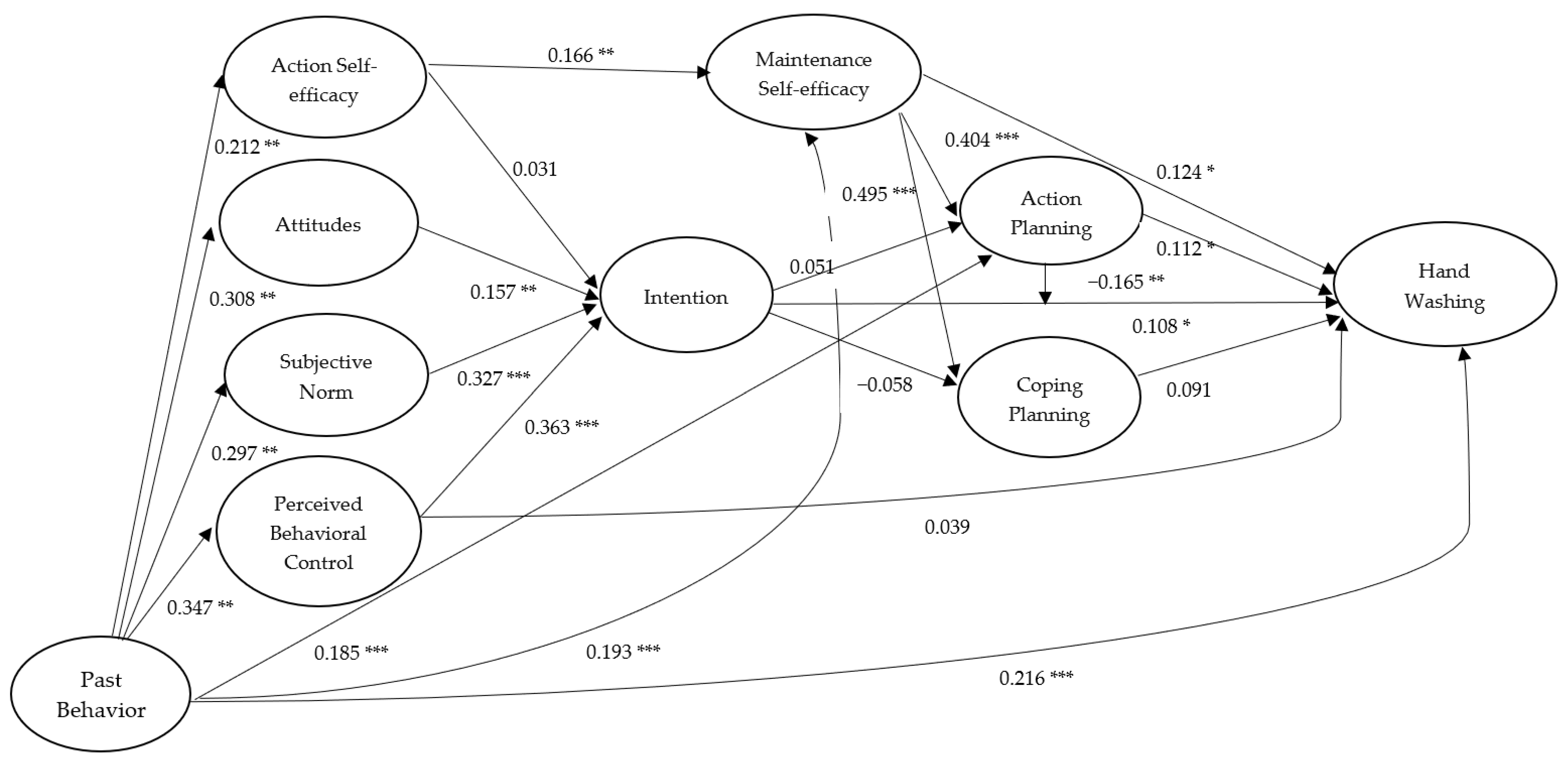
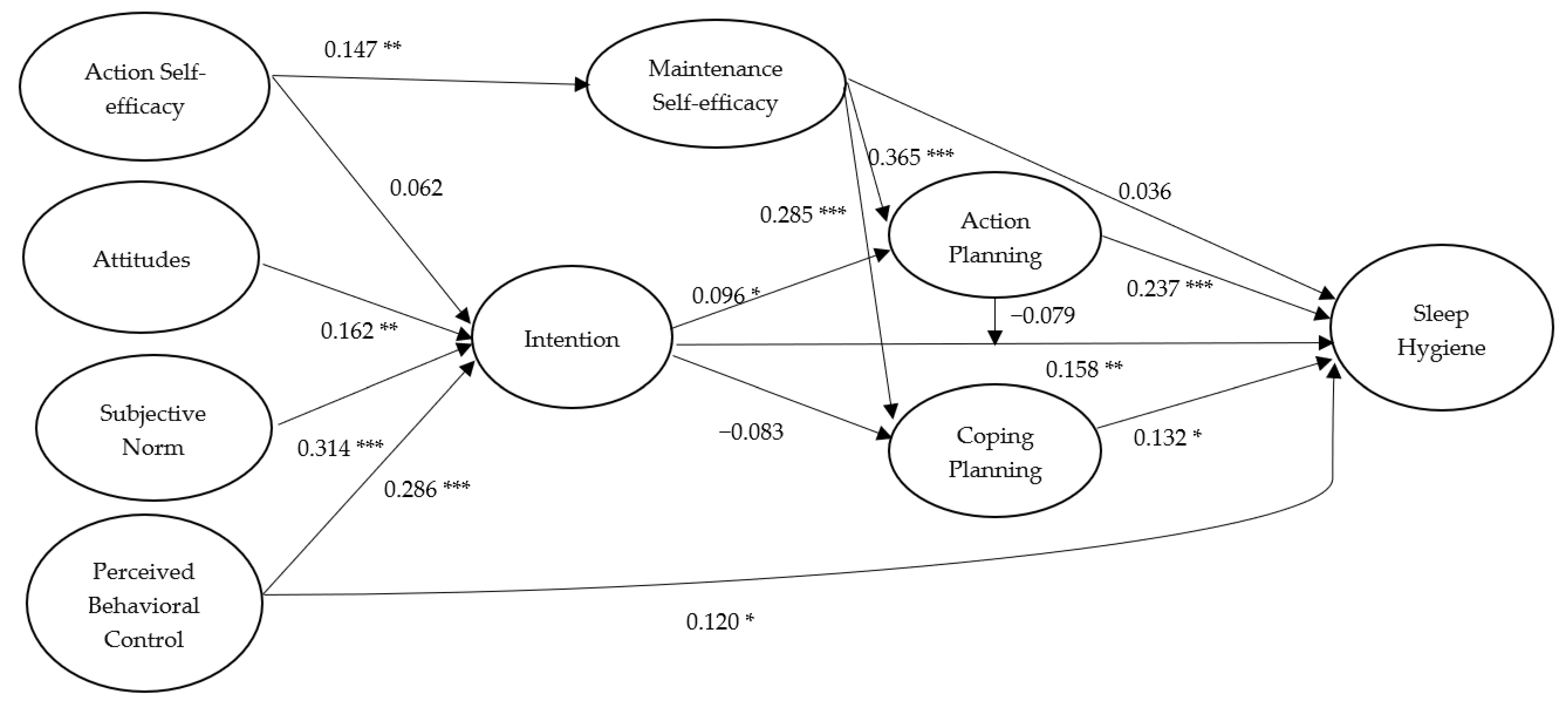
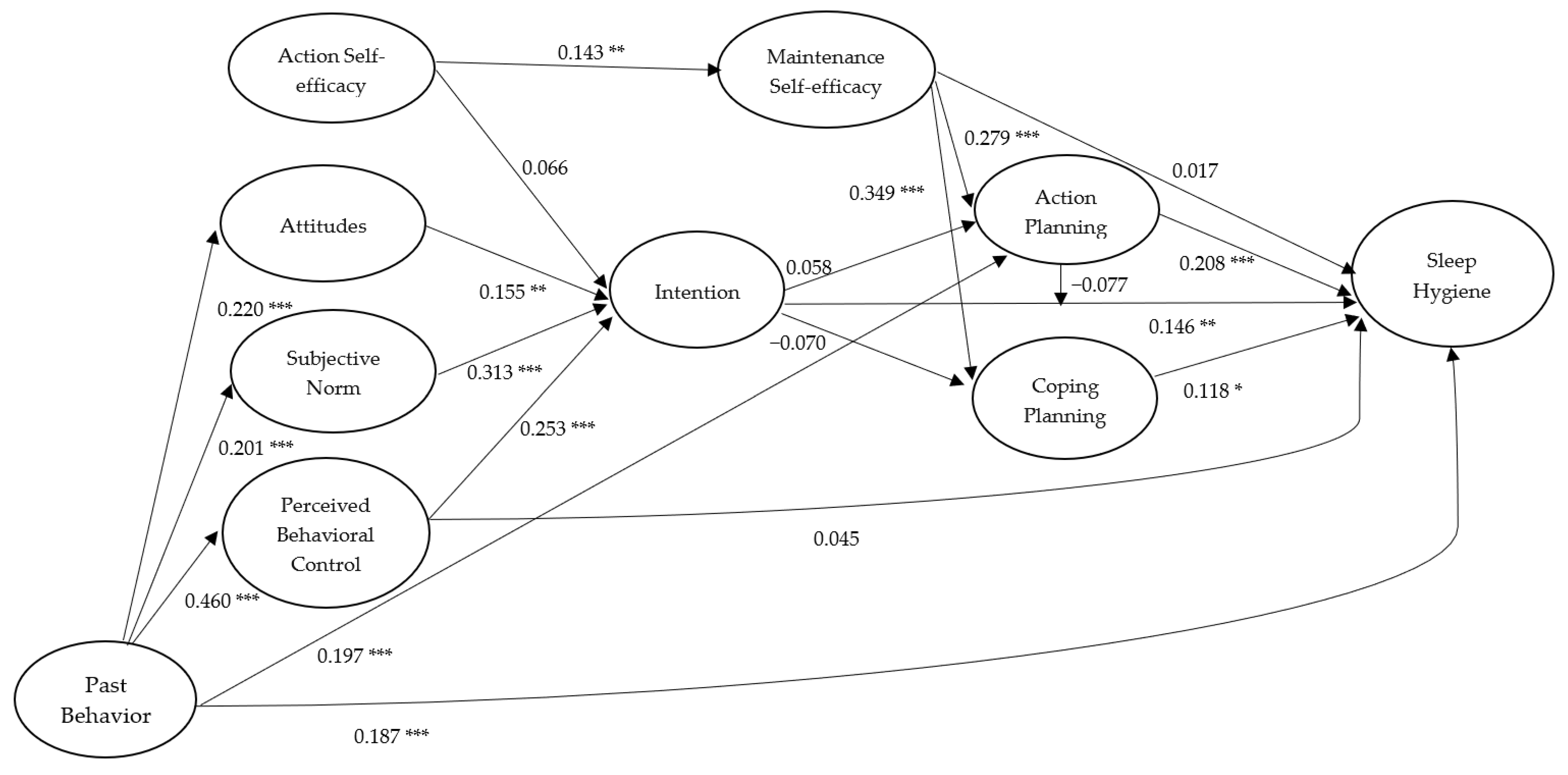
4.2. Model Effects
5. Discussion
6. Strengths and Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Raynor, D.A.; Levine, H. Associations between the five-factor model of personality and health behaviors among college students. J. Am. Coll. Health 2009, 58, 73–82. [Google Scholar] [CrossRef]
- Scott-Sheldon, L.A.J.; Carey, K.B.; Carey, M.P. Health behavior and college students: Does Greek affiliation matter? J. Behav. Med. 2007, 31, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Gardner, B.; de Bruijn, G.-J.; Lally, P. Habit, identity, and repetitive action: A prospective study of binge drinking in UK students. Br. J. Health Psychol. 2012, 17, 565–581. [Google Scholar] [CrossRef]
- Verplanken, B.; Sui, J. Habit and identity: Behavioral, cognitive, affective, and motivational facets of an integrated self. Front. Psychol. 2019, 10, 1504. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Social cognition models and health behaviour: A structured review. Psychol. Health 2000, 15, 173–189. [Google Scholar] [CrossRef] [Green Version]
- Hagger, M.S.; Hamilton, K. Changing behaviour using integrated theories. In The Handbook of Behavior Change; Hagger, M.S., Cameron, L., Hamilton, K., Hankonen, N., Lintunen, T., Eds.; Cambridge University Press: New York, NY, USA, 2020. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I.; Schmidt, P. Changing behaviour using the theory of planned behavior. In The Handbook of Behavior Change; Hagger, M.S., Cameron, L., Hamilton, K., Hankonen, N., Lintunen, T., Eds.; Cambridge University Press: New York, NY, USA, 2020. [Google Scholar]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Schwarzer, R.; Hamilton, K. Changing behaviour using the health action process approach. In The Handbook of Behavior Change; Hagger, M.S., Cameron, L., Hamilton, K., Hankonen, N., Lintunen, T., Eds.; Cambridge University Press: New York, NY, USA, 2020. [Google Scholar]
- Rabie, T.; Curtis, V. Handwashing and risk of respiratory infections: A quantitative systematic review. Trop. Med. Inter. Health 2006, 11, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.C.; Stocks, M.E.; Cumming, O.; Jeandron, A.; Higgins, J.P.; Wolf, J.; Prüss-Ustün, A.; Bonjour, S.; Hunter, P.R.; Fewtrell, L.; et al. Hygiene and health: Systematic review of handwashing practices worldwide and update of health effects. Trop. Med. Inter. Health 2014, 19, 906–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, V.; Cairncross, S. Effect of washing hands with soap on diarrhoea risk in the community: A systematic review. Lancet Infect. Dis. 2003, 3, 275–281. [Google Scholar] [CrossRef]
- Von Lengerke, T.; Lutze, B.; Krauth, C.; Lange, K.; Stahmeyer, J.T.; Chaberny, I.F. Promoting hand hygiene compliance: PSYGIENE—A cluster-randomized controlled trial of tailored interventions. Dtsch. Arztebl. Int. 2017, 114, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korniewicz, D.M.; El-Masri, M. Exploring the factors associated with hand hygiene compliance of nurses during routine clinical practice. Appl. Nurs. Res. 2010, 23, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Lhakhang, P.; Lippke, S.; Knoll, N.; Schwarzer, R. Evaluating brief motivational and self-regulatory hand hygiene interventions: A cross-over longitudinal design. BMC Public Health 2015, 15, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clayton, D.A.; Griffith, C.J. Efficacy of an extended theory of planned behaviour model for predicting caterers’ hand hygiene practices. Int. J. Environ. Health Res. 2008, 18, 83–98. [Google Scholar] [CrossRef]
- Mullan, B.A.; Wong, C.L. Hygienic food handling behaviours. An application of the Theory of Planned Behaviour. Appetite 2009, 52, 757–761. [Google Scholar] [CrossRef]
- Soon, J.M.; Baines, R.; Seaman, P. Meta-analysis of food safety training on hand hygiene knowledge and attitudes among food handlers. J. Food Prot. 2012, 75, 793–804. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.; Yardley, L.; Little, P. Development of an intervention to reduce transmission of respiratory infections and pandemic flu: Measuring and predicting hand-washing intentions. Psychol. Health Med. 2012, 17, 59–81. [Google Scholar] [CrossRef]
- Mariwah, S.; Hampshire, K.; Kasim, A. The impact of gender and physical environment on the handwashing behaviour of university students in Ghana. Trop. Med. Inter. Health 2012, 17, 447–454. [Google Scholar] [CrossRef]
- Mead, M.P.; Irish, L.A. Application of health behaviour theory to sleep health improvement. J. Sleep Res. 2019, e12950. [Google Scholar] [CrossRef]
- Thumma, J.; Aiello, A.E.; Foxman, B. The association between handwashing practices and illness symptoms among college students living in a university dormitory. Am. J. Infect. Control. 2009, 37, 70–72. [Google Scholar] [CrossRef]
- Buboltz Jr, W.; Jenkins, S.M.; Soper, B.; Woller, K.; Johnson, P.; Faes, T. Sleep habits and patterns of college students: An expanded study. J. Coll. Counsel. 2009, 12, 113–124. [Google Scholar] [CrossRef]
- Tsui, Y.Y.; Wing, Y.K. A study on the sleep patterns and problems of university business students in Hong Kong. J. Am. Coll. Health 2009, 58, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.M.; Adams, T.; Orr, C.; Quilter, L. Correlates of quality sleep and academic performance. Health Educ. 2008, 40, 82–89. [Google Scholar]
- Stepanski, E.J.; Wyatt, J.K. Use of sleep hygiene in the treatment of insomnia. Sleep Med. Rev. 2003, 7, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Irish, L.A.; Kline, C.E.; Gunn, H.E.; Buysse, D.J.; Hall, M.H. The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Med. Rev. 2015, 22, 23–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilcher, J.J.; Ginter, D.R.; Sadowsky, B. Sleep quality versus sleep quantity: Relationships between sleep and measures of health, well-being and sleepiness in college students. J. Psychosom. Res. 1997, 42, 583–596. [Google Scholar] [CrossRef]
- Mastin, D.F.; Bryson, J.; Corwyn, R. Assessment of sleep hygiene using the Sleep Hygiene Index. J. Behav. Med. 2006, 29, 223–227. [Google Scholar] [CrossRef]
- Kor, K.; Mullan, B.A. Sleep hygiene behaviours: An application of the theory of planned behaviour and the investigation of perceived autonomy support, past behaviour and response inhibition. Psychol. Health 2011, 26, 1208–1224. [Google Scholar] [CrossRef]
- Todd, J.; Mullan, B. The role of self-regulation in predicting sleep hygiene in university students. Psychol. Health Med. 2013, 18, 275–288. [Google Scholar] [CrossRef] [Green Version]
- Srigley, J.A.; Corace, K.; Hargadon, D.P.; Yu, D.; MacDonald, T.; Fabrigar, L.; Garber, G. Applying psychological frameworks of behaviour change to improve healthcare worker hand hygiene: A systematic review. J. Hosp. Infect. 2015, 91, 202–210. [Google Scholar] [CrossRef]
- Peach, H.D.; Gaultney, J.F.; Ruggiero, A.R. Direct and Indirect Associations of Sleep Knowledge and Attitudes with Objective and Subjective Sleep Duration and Quality via Sleep Hygiene. J. Prim. Prev. 2018, 39, 555–570. [Google Scholar] [CrossRef] [PubMed]
- Hagger, M.S.; Chan, D.K.; Protogerou, C.; Chatzisarantis, N.L. Using meta-analytic path analysis to test theoretical predictions in health behavior: An illustration based on meta-analyses of the theory of planned behavior. Prev. Med. 2016, 89, 154–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEachan, R.R.C.; Conner, M.; Taylor, N.J.; Lawton, R.J. Prospective prediction of health-related behaviours with the theory of planned behaviour: A meta-analysis. Health Psychol. Rev. 2011, 5, 97–144. [Google Scholar] [CrossRef]
- Jenner, E.A.; Watson, P.W.B.; Miller, L.; Jones, F.; Scott, G.M. Explaining hand hygiene practice: An extended application of the Theory of Planned Behaviour. Psychol. Health Med. 2002, 7, 311–326. [Google Scholar] [CrossRef]
- O’Boyle, C.A.; Henly, S.J.; Larson, E. Understanding adherence to hand hygiene recommendations: The theory of planned behavior. Am. J. Infect. Control. 2001, 29, 352–360. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Kim, K.M. Influencing factors on hand hygiene behavior of nursing students based on theory of planned behavior: A descriptive survey study. Nurse Educ. Today 2016, 36, 159–164. [Google Scholar] [CrossRef]
- Strong, C.; Lin, C.Y.; Jalilolghadr, S.; Updegraff, J.A.; Broström, A.; Pakpour, A.H. Sleep hygiene behaviours in Iranian adolescents: An application of the Theory of Planned Behavior. J. Sleep Res. 2018, 27, 23–31. [Google Scholar] [CrossRef]
- Knowlden, A.P.; Sharma, M.; Bernard, A.L. A theory of planned behavior research model for predicting the sleep intentions and behaviors of undergraduate college students. J. Prim. Prev. 2012, 33, 19–31. [Google Scholar] [CrossRef]
- Lao, H.C.; Tao, V.Y.; Wu, A.M. Theory of planned behaviour and healthy sleep of college students. Aust. J. Psychol. 2016, 68, 20–28. [Google Scholar] [CrossRef]
- Hagger, M.S.; Luszczynska, A. Implementation intention and action planning interventions in health contexts: State of the research and proposals for the way forward. Appl. Psychol. Health Well Being 2014, 6, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.-Q.; Zhang, R.; Schwarzer, R.; Hagger, M.S. A meta-analysis of the health action process approach. Health Psychol. 2019, 38, 623–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes Fernández, B.; Knoll, N.; Hamilton, K.; Schwarzer, R. Social-cognitive antecedents of hand washing: Action control bridges the planning–behaviour gap. Psychol. Health 2016, 31, 993–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, S.; Mullan, B. Predicting food hygiene. An investigation of social factors and past behaviour in an extended model of the Health Action Process Approach. Appetite 2010, 54, 126–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, K.; Ng, H.; Zhang, C.-Q.; Phipps, D.; Zhang, R. Social psychological predictors of sleep hygiene behaviors in Australian and Hong Kong university students. Int. J. Behav. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Nisbett, R.E.; Peng, K.; Choi, I.; Norenzayan, A. Culture and systems of thought: Holistic versus analytic cognition. Psychol. Rev. 2001, 108, 291–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gollwitzer, P.M.; Sheeran, P. Implementation intentions and goal achievement: A meta-analysis of effects and processes. Adv. Exp. Soc. Psychol. 2006, 38, 69–119. [Google Scholar]
- Zhang, C.-Q.; Wong, M.C.Y.; Zhang, R.; Hamilton, K.; Hagger, M.S. Adolescent sugar-sweetened beverage consumption: An extended Health Action Process Approach. Appetite 2019, 141, 104332. [Google Scholar] [CrossRef] [Green Version]
- Hagger, M.S.; Polet, J.; Lintunen, T. The reasoned action approach applied to health behavior: Role of past behavior and tests of some key moderators using meta-analytic structural equation modeling. Soc. Sci. Med. 2018, 213, 85–94. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Hand Hygiene: Why, How & When? Available online: https://www.who.int/gpsc/5may/Hand_Hygiene_Why_How_and_When_Brochure.pdf (accessed on 1 January 2020).
- National Sleep Foundation. Sleep Hygiene. Available online: https://www.sleepfoundation.org/articles/sleep-hygiene (accessed on 1 January 2020).
- Sniehotta, F.F.; Schwarzer, R.; Scholz, U.; Schuz, B. Action planning and coping planning for long-term lifestyle change: Theory and assessment. Eur. J. Soc. Psychol. 2005, 35, 565–576. [Google Scholar] [CrossRef]
- Kock, N. WarpPLS User Manual: Version 6.0. Available online: http://cits.tamiu.edu/WarpPLS/UserManual_v_6_0.pdf (accessed on 1 January 2020).
- Tenenhaus, M.; Vinzi, V.E.; Chatelin, Y.M.; Lauro, C. PLS path modeling. Compu. Sta. Data Analy. 2005, 48, 159–205. [Google Scholar] [CrossRef]
- Ajzen, I. Behavioral Interventions based on the Theory of Planned Behavior. Available online: http://people.umass.edu/aizen/pdf/tpb.intervention.pdf. (accessed on 1 January 2020).
- De Bruijn, G.J.; Rhodes, R.E.; van Osch, L. Does action planning moderate the intention-habit interaction in the exercise domain? A three-way interaction analysis investigation. J. Behav. Med. 2012, 35, 509–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Osch, L.; Beenackers, M.; Reubsaet, A.; Lechner, L.; Candel, M.; de Vries, H. Action planning as predictor of health protective and health risk behavior: An investigation of fruit and snack consumption. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagger, M.S. Habit and physical activity: Theoretical advances, practical implications, and agenda for future research. Psychol. Sport Exerc. 2019, 42, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, R.E.; Yao, C.A. Models accounting for intention-behavior discordance in the physical activity domain: A user’s guide, content overview, and review of current evidence. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, W.; Rünger, D. Psychology of habit. Annu. Rev. Psychol. 2016, 67, 289–314. [Google Scholar] [CrossRef] [Green Version]
- Ouellette, J.A.; Wood, W. Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior. Psychol. Bull. 1998, 124, 54–74. [Google Scholar] [CrossRef]
- Verplanken, B.; Orbell, S. Reflections on past behavior: A self-report index of habit strength. J. Appl. Soc. Psychol. 2003, 33, 1313–1330. [Google Scholar] [CrossRef]
- Van Bree, R.J.H.; van Stralen, M.M.; Mudde, A.N.; Bolman, C.; de Vries, H.; Lechner, L. Habit as mediator of the relationship between prior and later physical activity: A longitudinal study in older adults. Psychol. Sport Exerc. 2015, 19, 95–102. [Google Scholar] [CrossRef]
- Rothman, A.J.; Klein, W.M.P.; Sheeran, P. Moving from theoretical principles to intervention strategies: Applying the experimental medicine approach. In The Handbook of Behavior Change; Hagger, M.S., Cameron, L., Hamilton, K., Hankonen, N., Lintunen, T., Eds.; Cambridge University Press: New York, NY, USA, 2020. [Google Scholar]
- Hagger, M.S.; Cameron, L.D.; Hamilton, K.; Hankonen, N.; Lintunen, T. The science of behavior change: The road ahead. In The Handbook of Behavior Change; Hagger, M.S., Cameron, L., Hamilton, K., Hankonen, N., Lintunen, T., Eds.; Cambridge University Press: New York, NY, USA, 2020. [Google Scholar]
- Shiffman, S.; Stone, A.A. Introduction to the special section: Ecological momentary assessment in health psychology. Health Psychol. 1998, 17, 3–5. [Google Scholar] [CrossRef]
- Downs, D.S.; Hausenblas, H.A. Elicitation studies and the theory of planned behavior: A systematic review of exercise beliefs. Psychol. Sport Exerc. 2005, 6, 1–31. [Google Scholar] [CrossRef]
- Ajzen, I. Constructing a Theory of Planned Behavior Questionnaire. Available online: https://people.umass.edu/aizen/pdf/tpb.measurement.pdf (accessed on 1 January 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Attitudes T1 | 6.07 | 0.95 | 0.901 | |||||||||
| 2. Subjective norm T1 | 5.39 | 0.93 | 0.334 ** | 0.884 | ||||||||
| 3. PBC T1 | 5.55 | 0.89 | 0.353 ** | 0.476 ** | 0.861 | |||||||
| 4. Action SE T1 | 3.00 | 0.77 | 0.144 * | 0.205 ** | 0.250 ** | 0.873 | ||||||
| 5. Intention T1 | 5.76 | 0.84 | 0.373 ** | 0.544 ** | 0.542 ** | 0.212 ** | 0.841 | |||||
| 6. Hand washing T1 | 3.40 | 0.50 | 0.331 ** | 0.292 ** | 0.367 ** | 0.196 ** | 0.216 ** | 0.743 | ||||
| 7. Maintenance SE T2 | 2.90 | 0.53 | 0.121 * | 0.129 * | 0.173 ** | 0.175 ** | 0.204 ** | 0.128 * | 0.792 | |||
| 8. Action planning T2 | 2.85 | 0.53 | 0.123 * | 0.159 ** | 0.211 ** | 0.142 * | 0.126 * | 0.208 ** | 0.444 ** | 0.800 | ||
| 9. Coping planning T2 | 2.80 | 0.54 | 0.111 | 0.124 * | 0.133 * | 0.053 | 0.065 | 0.156 ** | 0.507 ** | 0.522 ** | 0.767 | |
| 10. Hand washing T3 | 3.30 | 0.58 | 0.216 ** | 0.165 ** | 0.159 ** | 0.071 | 0.204 ** | 0.312 ** | 0.280 ** | 0.272 ** | 0.272 ** | 0.826 |
| Variables | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Attitudes T1 | 5.19 | 0.90 | 0.812 | |||||||||
| 2. Subjective norm T1 | 5.26 | 0.84 | 0.145 * | 0.807 | ||||||||
| 3. PBC T1 | 4.91 | 10.01 | 0.158 * | 0.381 ** | 0.854 | |||||||
| 4. Action SE T1 | 2.67 | 0.65 | 0.141 * | 0.113 | 0.254 ** | 0.810 | ||||||
| 5. Intention T1 | 5.44 | 0.92 | 0.205 ** | 0.441 ** | 0.464 ** | 0.220 ** | 0.864 | |||||
| 6. Sleep hygiene T1 | 3.05 | 0.42 | 0.006 | 0.193 ** | 0.445 ** | 0.065 | 0.254 ** | 0.677 | ||||
| 7. Maintenance SE T2 | 2.83 | 0.53 | 0.043 | 0.196 ** | 0.252 ** | 0.135 * | 0.232 ** | 0.072 | 0.807 | |||
| 8. Action planning T2 | 2.74 | 0.51 | 0.085 | 0.081 | 0.237 ** | 0.182 ** | 0.124 * | 0.222 ** | 0.336 ** | 0.763 | ||
| 9. Coping planning T2 | 2.60 | 0.57 | −0.010 | 0.014 | 0.146* | 0.070 | 0.042 | 0.134 * | 0.282 ** | 0.249 ** | 0.762 | |
| 10. Sleep hygiene T3 | 3.06 | 0.44 | 0.181 ** | 0.201 ** | 0.270 ** | 0.092 | 0.255 ** | 0.327 ** | 0.151* | 0.267 ** | 0.071 | 0.746 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.-Q.; Fang, R.; Zhang, R.; Hagger, M.S.; Hamilton, K. Predicting Hand Washing and Sleep Hygiene Behaviors among College Students: Test of an Integrated Social-Cognition Model. Int. J. Environ. Res. Public Health 2020, 17, 1209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041209
Zhang C-Q, Fang R, Zhang R, Hagger MS, Hamilton K. Predicting Hand Washing and Sleep Hygiene Behaviors among College Students: Test of an Integrated Social-Cognition Model. International Journal of Environmental Research and Public Health. 2020; 17(4):1209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041209
Chicago/Turabian StyleZhang, Chun-Qing, Rongyu Fang, Ru Zhang, Martin S. Hagger, and Kyra Hamilton. 2020. "Predicting Hand Washing and Sleep Hygiene Behaviors among College Students: Test of an Integrated Social-Cognition Model" International Journal of Environmental Research and Public Health 17, no. 4: 1209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041209