The Influence of Mistreatment by Patients on Job Satisfaction and Turnover Intention among Chinese Nurses: A Three-Wave Survey

Abstract
:1. Introduction
2. Theoretical Review and Hypothesis Development
2.1. Mediating Role of Work Meaningfulness
2.2. Mediating Role of Emotional Dissonance
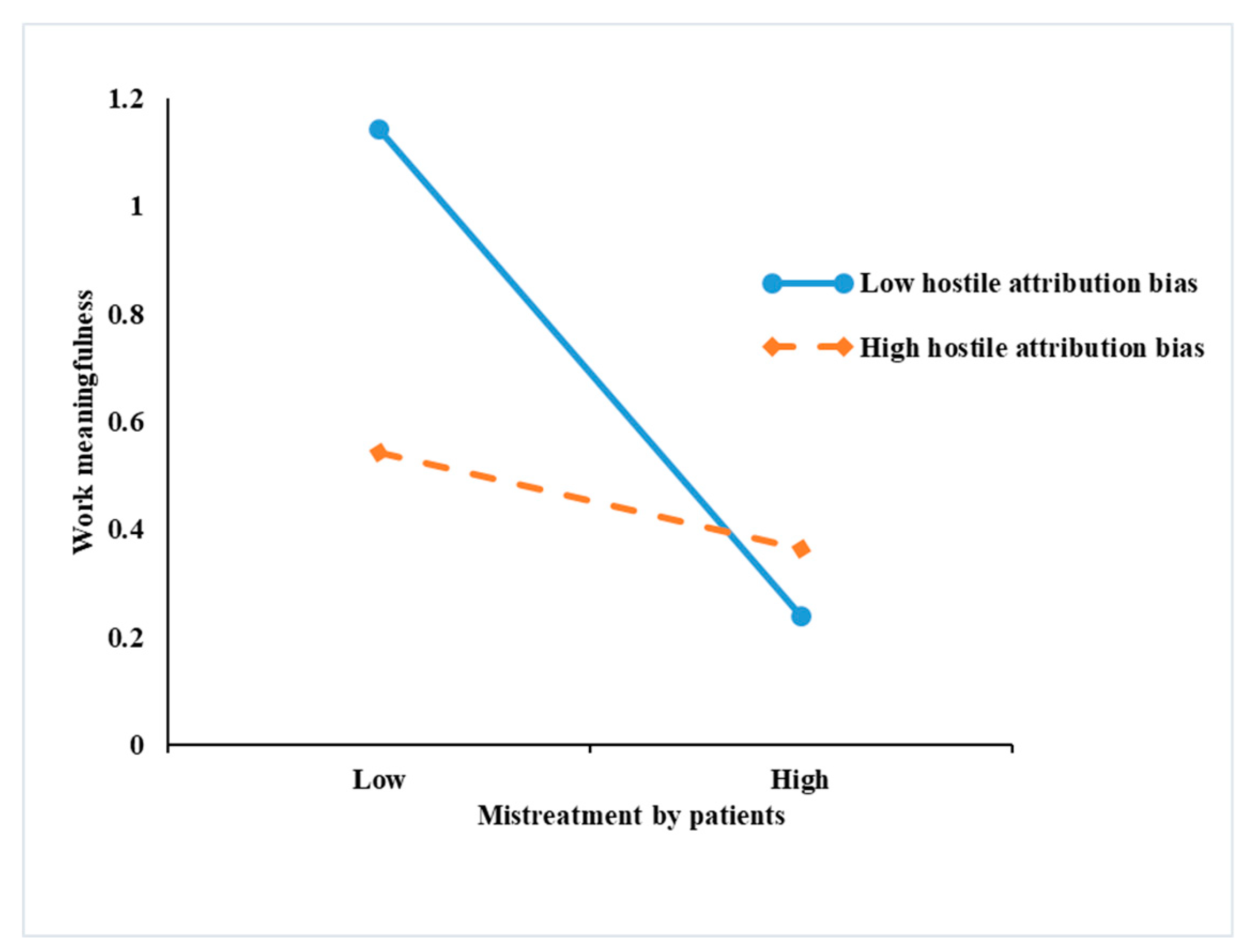
2.3. Moderating Role of Hostile Attribution Bias
3. Methods
3.1. Study Design and Participants
3.2. Measurement Scales
3.3. Data Analysis
4. Results
4.1. Descriptive Statistics Correlations
4.2. Confirmatory Factor Analyses
4.3. Hypothesis Testing
5. Discussion
5.1. Theoretical Contributions and Practical Implications
5.2. Limitations and Future Research Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Xinhua News Agency. Available online: http://www.xinhuanet.com/gongyi/2017-05/11/c_129601688_2.htm (accessed on 16 January 2020).
- Rupp, D.E.; Spencer, S. When customers lash out: The effects of customer interactional injustice on emotional labor and the mediating role of discrete emotions. J. Appl. Psychol. 2006, 91, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Karaeminogullari, A.; Erdogan, B.; Bauer, T.N. Biting the hand that heals: Mistreatment by patients and the well-being of healthcare workers. Pers. Rev. 2018, 47, 572–591. [Google Scholar] [CrossRef]
- Grandey, A.A.; Kern, J.H.; Frone, M.R. Verbal abuse from outsiders versus insiders: Comparing frequency, impact on emotional exhaustion, and the role of emotional labor. J. Occup. Health Psychol. 2007, 12, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, K.L.; Harris, L.C. When service failure is not service failure: An exploration of the forms and motives of “illegitimate” customer complaining. J. Serv. Mark. 2005, 19, 321–335. [Google Scholar] [CrossRef]
- Hershcovis, M.S.; Reich, T.C.; Parker, S.K.; Bozeman, J. The relationship between workplace aggression and target deviant behaviour: The moderating roles of power and task interdependence. Work Stress 2012, 26, 1–20. [Google Scholar] [CrossRef]
- Wang, M.; Liu, S.; Liao, H.; Gong, Y.; Kammeyer-Mueller, J.; Shi, J. Can’t get it out of my mind: Employee rumination after customer mistreatment and negative mood in the next morning. J. Appl. Psychol. 2013, 98, 989–1004. [Google Scholar] [CrossRef]
- Albashayreh, A.; Sabei, S.D.A.; AL-Rawajfah, O.M.; Al-Awaisi, H. Healthy work environments are critical for nurse job satisfaction: Implications for Oman. Int. Nurs. Rev. 2019, 66, 1–7. [Google Scholar] [CrossRef]
- Weiss, H.M.; Cropanzano, R. Affective Events Theory: A Theoretical Discussion of The Structure, Cause and Consequences of Affective Experiences at Work. Res. Organ. Behav. 1996, 18, 1–74. [Google Scholar]
- Hackman, J.R.; Oldham, G.R. Development of the job diagnostic survey. J. Appl. Psychol. 1975, 60, 159–170. [Google Scholar] [CrossRef] [Green Version]
- Rosso, B.D.; Dekas, K.H.; Wrzesniewski, A. On the meaning of work: A theoretical integration and review. Res. Organ. Behav. 2010, 30, 91–127. [Google Scholar] [CrossRef]
- Kahn, R.L.; Wolfe, D.M.; Quinn, R.P.; Snoek, J.D.; Rosenthal, R.A. Organizational Stress: Studies in Role Conflict and Ambiguity. Am. J. Sociol. 1965, 30, 620. [Google Scholar]
- Rafaeli, A.; Sutton, R.I. Expression of Emotion as Part of the Work Role. Acad. Manage. Rev. 1987, 12, 23–27. [Google Scholar] [CrossRef]
- Abraham, R. The impact of emotional dissonance on organizational commitment and intention to turnover. J. Psychol. 1999, 133, 441–455. [Google Scholar] [CrossRef] [PubMed]
- Back, C.-Y.; Hyun, D.-S.; Chang, S.-J. Association between Emotional Labor, Emotional Dissonance, Burnout and Turnover Intention in Clinical Nurses: A Multiple-Group Path Analysis across Job Satisfaction. J. Korean Acad. Nurs. 2017, 47, 770–780. [Google Scholar] [CrossRef] [Green Version]
- Bies, R.J. Interactional (in) justice: The sacred and the profane. Adv. Organ. Justice 2001, 3, 89–118. [Google Scholar]
- Dormann, C.; Zapf, D. Customer-related social stressors and burnout. J. Occup. Health Psychol. 2004, 9, 61–82. [Google Scholar] [CrossRef]
- Garcia, P.R.J.M.; Restubog, S.L.D.; Lu, V.N.; Amarnani, R.K.; Wang, L.; Capezio, A. Attributions of blame for customer mistreatment: Implications for employees’ service performance and customers’ negative word of mouth. J. Vocat. Behav. 2019, 110, 203–213. [Google Scholar] [CrossRef]
- Van Jaarsveld, D.D.; Walker, D.D.; Skarlicki, D.P. The role of job demands and emotional exhaustion in the relationship between customer and employee incivility. J. Manag. 2010, 36, 1486–1504. [Google Scholar] [CrossRef] [Green Version]
- Steger, M.F.; Dik, B.J.; Duffy, R.D. Measuring meaningful work: The work and meaning inventory (WAMI). J. Career Assess. 2012, 20, 322–337. [Google Scholar] [CrossRef] [Green Version]
- Martela, F.; Pessi, A.B. Significant work is about self-realization and broader purpose: Defining the key dimensions of meaningful work. Front. Psychol. 2018, 9, 363–377. [Google Scholar] [CrossRef]
- Yeoman, R. Conceptualising meaningful work as a fundamental human need. J. Bus. Ethics 2014, 125, 235–251. [Google Scholar] [CrossRef]
- Bailey, C.; Madden, A.; Alfes, K.; Shantz, A.; Soane, E. The mismanaged soul: Existential labor and the erosion of meaningful work. Hum. Resour. Manag. Rev. 2017, 27, 416–430. [Google Scholar] [CrossRef] [Green Version]
- Soane, E.; Shantz, A.; Alfes, K.; Truss, C.; Rees, C.; Gatenby, M. The Association of Meaningfulness, Well-Being, and Engagement with Absenteeism: A Moderated Mediation Model. Hum. Resour. Manage. 2013, 52, 441–456. [Google Scholar] [CrossRef] [Green Version]
- Demirtas, O.; Hannah, S.T.; Gok, K.; Arslan, A.; Capar, N. The moderated influence of ethical leadership, via meaningful work, on followers’ engagement, organizational identification, and envy. J. Bus. Ethics 2017, 145, 183–199. [Google Scholar] [CrossRef]
- Fagermoen, M.S. Professional identity: Values embedded in meaningful nursing practice. J. Adv. Nurs. 1997, 25, 434–441. [Google Scholar] [CrossRef]
- Grandey, A.; Foo, S.C.; Groth, M.; Goodwin, R.E. Free to be you and me: A climate of authenticity alleviates burnout from emotional labor. J. Occup. Health Psychol. 2012, 17, 1–14. [Google Scholar] [CrossRef]
- Geanellos, R. Sustaining well-being and enabling recovery: The therapeutic effect of nurse friendliness on clients and nursing environments. Contemp. Nurse 2005, 19, 242–252. [Google Scholar] [CrossRef]
- Daunt, K.L.; Harris, L.C. Linking employee and customer misbehaviour: The moderating role of past misdemeanours. J. Mark. Manag. 2014, 30, 221–244. [Google Scholar] [CrossRef]
- Qian, J.; Yang, F.; Wang, B.; Huang, C.; Song, B. When workplace ostracism leads to burnout: The roles of job self-determination and future time orientation. Int. J. Hum. Resour. Manag. 2017, 30, 1–17. [Google Scholar] [CrossRef]
- Diefendorff, J.M.; Gosserand, R.H. Understanding the emotional labor process: A control theory perspective. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2003, 24, 945–959. [Google Scholar] [CrossRef]
- McCance, A.S.; Nye, C.D.; Wang, L.; Jones, K.S.; Chiu, C. Alleviating the burden of emotional labor: The role of social sharing. J. Manag. 2013, 39, 392–415. [Google Scholar] [CrossRef] [Green Version]
- Locke, E.A. What is job satisfaction? Organ. Behav. Hum. Perform. 1969, 4, 309–336. [Google Scholar] [CrossRef]
- Martela, F.; Riekki, T.J. Autonomy, Competence, Relatedness, and Beneficence: A Multicultural Comparison of the Four Pathways to Meaningful Work. Front. Psychol. 2018, 9, 1157–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, C.L.; Taborda-Whitt, C.; Frazer, M.; Schellinger, S.; White, K.M.; Kaasovic, J.; Nelson, B.; Chant, A. A mixed methods study of emotional exhaustion: Energizing and depleting work within an innovative healthcare team. J. Interprof. Care 2017, 31, 714–724. [Google Scholar] [CrossRef] [PubMed]
- Lombas, A.S.; Esteban, M.Á. The confounding role of basic needs satisfaction between self-determined motivation and well-being. J. Happiness Stud. 2018, 19, 1305–1327. [Google Scholar] [CrossRef]
- Humphrey, S.E.; Nahrgang, J.D.; Morgeson, F.P. Integrating motivational, social, and contextual work design features: A meta-analytic summary and theoretical extension of the work design literature. J. Appl. Psychol. 2007, 92, 1332–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, S. Emotion at work: To what extent are we expressing, suppressing, or faking it? Eur. J. Work Organ. Psychol. 1999, 8, 347–369. [Google Scholar] [CrossRef]
- Grandey, A.A. Emotional regulation in the workplace: A new way to conceptualize emotional labor. J. Occup. Health Psychol. 2000, 5, 95–110. [Google Scholar] [CrossRef]
- Yang, J.; Diefendorff, J.M. The relations of daily counterproductive workplace behavior with emotions, situational antecedents, and personality moderators: A diary study in Hong Kong. Pers. Psychol. 2009, 62, 259–295. [Google Scholar] [CrossRef]
- Hur, W.-M.; Moon, T.W.; Han, S.-J. The effect of customer incivility on service employees’ customer orientation through double-mediation of surface acting and emotional exhaustion. J. Serv. Theory Pract. 2015, 25, 394–413. [Google Scholar] [CrossRef]
- Edwards, J.R. A cybernetic theory of stress, coping, and well-being in organizations. Acad. Manage. Rev. 1992, 17, 238–274. [Google Scholar] [CrossRef]
- Patrick, K.; Lavery, J.F. Burnout in nursing. Aust. J. Adv. Nurs. Q. Publ. R. Aust. Nurs. Fed. 2007, 24, 43–48. [Google Scholar]
- Garrosa, E.; Rainho, C.; Moreno-Jimenez, B.; Monteiro, M.J. The relationship between job stressors, hardy personality, coping resources and burnout in a sample of nurses: A correlational study at two time points. Int. J. Nurs. Stud. 2010, 47, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Mobley, W.H. Intermediate linkages in the relationship between job satisfaction and employee turnover. J. Appl. Psychol. 1977, 62, 237–240. [Google Scholar] [CrossRef]
- Hülsheger, U.R.; Schewe, A.F. On the costs and benefits of emotional labor: A meta-analysis of three decades of research. J. Occup. Health Psychol. 2011, 16, 361–389. [Google Scholar] [CrossRef]
- Applebaum, D.; Fowler, S.; Fiedler, N.; Osinubi, O.; Robson, M. The impact of environmental factors on nursing stress, job satisfaction, and turnover intention. J. Nurs. Adm. 2010, 40, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Grandey, A.A.; Tam, A.P.; Brauburger, A.L. Affective States and Traits in the Workplace: Diary and Survey Data from Young Workers. Motiv. Emot. 2002, 26, 31–55. [Google Scholar] [CrossRef]
- Han, S.J.; Bonn, M.A.; Cho, M. The relationship between customer incivility, restaurant frontline service employee burnout and turnover intention. Int. J. Hosp. Manag. 2016, 52, 97–106. [Google Scholar] [CrossRef]
- Jack, K.; Wibberley, C. The meaning of emotion work to student nurses: A Heideggerian analysis. Int. J. Nurs. Stud. 2014, 51, 900–907. [Google Scholar] [CrossRef]
- Matthews, B.A.; Norris, F.H. When Is Believing “Seeing”? Hostile Attribution Bias as a Function of Self-Reported Aggression 1. J. Appl. Soc. Psychol. 2002, 32, 1–31. [Google Scholar] [CrossRef]
- Wingrove, J.; Bond, A.J. Angry reactions to failure on a cooperative computer game: The effect of trait hostility, behavioural inhibition, and behavioural activation. Aggress. Behav. 1998, 24, 27–36. [Google Scholar] [CrossRef]
- Adams, S.H.; John, O.P. A Hostility Scale for the California Psychological Inventory: MMPI, Observer Q-Sort, and Big-Five Correlates. J. Pers. Assess. 1997, 69, 408–424. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.W.; Pondy, L.R. Toward an" intent" model of conflict management among principal parties. Hum. Relat. 1977, 30, 1089–1102. [Google Scholar] [CrossRef]
- Choi, J.N.; Sung, S.Y.; Lee, K.; Cho, D.-S. Balancing cognition and emotion: Innovation implementation as a function of cognitive appraisal and emotional reactions toward innovation. J. Organ. Behav. 2011, 32, 107–124. [Google Scholar] [CrossRef]
- Judge, T.A.; Scott, B.A.; Ilies, R. Hostility, Job Attitudes, and Workplace Deviance: Test of a Multilevel Model. J. Appl. Psychol. 2006, 91, 126–138. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.Z.; Zhang, H.; Chiu, R.K.; Kwan, H.K.; He, X. Hostile Attribution Bias and Negative Reciprocity Beliefs Exacerbate Incivility’s Effects on Interpersonal Deviance. J. Bus. Ethics 2013, 120, 189–199. [Google Scholar] [CrossRef]
- Hoobler, J.M.; Brass, D.J. Abusive supervision and family undermining as displaced aggression. J. Appl. Psychol. 2006, 91, 1125–1133. [Google Scholar] [CrossRef]
- Lyu, Y.; Zhu, H.; Zhong, H.-J.; Hu, L. Abusive supervision and customer-oriented organizational citizenship behavior: The roles of hostile attribution bias and work engagement. Int. J. Hosp. Manag. 2016, 53, 69–80. [Google Scholar] [CrossRef]
- Holtzworth-Munroe, A.; Anglin, K. The competency of responses given by maritally violent versus nonviolent men to problematic marital situations. Violence Vict. 1991, 6, 257–269. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; Organ, D.W. Self-reports in organizational research: Problems and prospects. J. Manag. 1986, 12, 531–544. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Schaffer, B.S.; Riordan, C.M. A review of cross-cultural methodologies for organizational research: A best-practices approach. Organ. Res. Methods 2003, 6, 169–215. [Google Scholar] [CrossRef] [Green Version]
- Cortina, L.M.; Magley, V.J.; Williams, J.H.; Langhout, R.D. Incivility in the workplace: Incidence and impact. J. Occup. Health Psychol. 2001, 6, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Duchon, D.; Plowman, D.A. Nurturing the spirit at work: Impact on work unit performance. Leadersh. Q. 2005, 16, 807–833. [Google Scholar] [CrossRef] [Green Version]
- Kumar Madupalli, R.; Poddar, A. Problematic customers and customer service employee retaliation. J. Serv. Mark. 2014, 28, 244–255. [Google Scholar] [CrossRef]
- Wright, T.A.; Cropanzano, R. Psychological well-being and job satisfaction as predictors of job performance. J. Occup. Health Psychol. 2000, 5, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Peus, C.; Weisweiler, S.; Frey, D. Transformational leadership, job satisfaction, and team performance: A multilevel mediation model of trust. Leadersh. Q. 2013, 24, 270–283. [Google Scholar] [CrossRef]
- Knudsen, H.K.; Ducharme, L.J.; Roman, P.M. Counselor emotional exhaustion and turnover intention in therapeutic communities. J. Subst. Abuse Treat. 2006, 31, 173–180. [Google Scholar] [CrossRef]
- Li, J.; Lambert, V.A. Workplace stressors, coping, demographics and job satisfaction in Chinese intensive care nurses. Nurs. Crit. Care 2008, 13, 12–24. [Google Scholar] [CrossRef]
- Emiroğlu, B.D.; Akova, O.; Tanrıverdi, H. The relationship between turnover intention and demographic factors in hotel businesses: A study at five star hotels in Istanbul. Procedia-Soc. Behav. Sci. 2015, 207, 385–397. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.-I.; Chang, H. Work climate perception and turnover intention among Korean hospital staff. Int. Nurs. Rev. 2009, 56, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Fit Indices in Covariance Structure Modeling: Sensitivity to Underparameterized Model Misspecification. Psychol Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Preacher, K.J.; Zyphur, M.J.; Zhang, Z. A general multilevel SEM framework for assessing multilevel mediation. Psychol. Methods 2010, 15, 209–233. [Google Scholar] [CrossRef] [Green Version]
- Baranik, L.E.; Wang, M.; Gong, Y.; Shi, J. Customer Mistreatment, Employee Health, and Job Performance: Cognitive Rumination and Social Sharing as Mediating Mechanisms. J. Manag. 2014, 43, 1971–1977. [Google Scholar] [CrossRef]
- Baik, D.; Zierler, B. RN Job Satisfaction and Retention After an Interprofessional Team Intervention. West. J. Nurs. Res. 2018, 41, 1–16. [Google Scholar] [CrossRef]
- Shao, R.; Skarlicki, D.P. Service employees’ reactions to mistreatment by customers: A comparison between North America and East Asia. Pers. Psychol. 2014, 67, 23–59. [Google Scholar] [CrossRef]
- Diefendorff, J.M.; Gabriel, A.S.; Nolan, M.T.; Yang, J. Emotion regulation in the context of customer mistreatment and felt affect: An event-based profile approach. J. Appl. Psychol. 2019, 104, 965–983. [Google Scholar] [CrossRef]
- Loi, R.; Xu, A.J.; Chow, C.W.; Kwok, J.M. Customer misbehavior and store managers’ work-to-family enrichment: The moderated mediation effect of work meaningfulness and organizational affective commitment. Hum. Resour. Manage. 2018, 57, 1039–1048. [Google Scholar] [CrossRef]
- Heider, F. The Psychology of Interpersonal Relations; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1958. [Google Scholar]
- Boafo, I.M. The effects of workplace respect and violence on nurses’ job satisfaction in Ghana: A cross-sectional survey. Hum. Resour. Health 2018, 16, 6. [Google Scholar] [CrossRef]
- Rayan, A.; Qurneh, A.; Elayyan, R.; Baker, O. Developing a policy for workplace violence against nurses and health care professionals in Jordan: A plan of action. Am. J. Public Health Res. 2016, 4, 47–55. [Google Scholar]
- Yagil, D.; Dayan, H. Justification of aggression against nurses: The effect of aggressor distress and nurse communication quality. J. Adv. Nurs. 2020, 76, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Goussinsky, R.; Livne, Y. Coping with interpersonal mistreatment: The role of emotion regulation strategies and supervisor support. J. Nurs. Manag. 2016, 24, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Agarwal, U.A.; Khatri, N. The relationships between perceived organizational support, affective commitment, psychological contract breach, organizational citizenship behaviour and work engagement. J. Adv. Nurs. 2016, 72, 2806–2817. [Google Scholar] [CrossRef] [PubMed]
- Chi, N.-W.; Yang, J.; Lin, C.-Y. Service workers’ chain reactions to daily customer mistreatment: Behavioral linkages, mechanisms, and boundary conditions. J. Occup. Health Psychol. 2018, 23, 58–70. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| M | S.D. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1.MP | 2.170 | 1.429 | ||||||||
| 2.WM | 5.114 | 1.139 | −0.172 ** | |||||||
| 3.JS | 5.042 | 1.154 | −0.118 ** | 0.642 ** | ||||||
| 4.ED | 3.455 | 1.348 | 0.430 ** | −0.135 ** | −0.110 ** | |||||
| 5.TI | 2.908 | 1.434 | 0.610 ** | −0.260 ** | −0.301 ** | 0.392 ** | ||||
| 6.HAB | 2.930 | 1.358 | 0.593 ** | −0.185 ** | −0.202 ** | 0.632 ** | 0.596 ** | |||
| 7.Gender | 1.746 | 0.436 | −0.129 ** | 0.046 | 0.050 | −0.039 | −0.146 ** | −0.073 | ||
| 8.Age | 30.887 | 7.311 | 0.070 | −0.072 | −0.056 | 0.094 * | 0.004 | 0.090 * | −0.139 ** | |
| 9.Tenure | 8.258 | 7.485 | 0.066 | −0.042 | −0.032 | 0.110 ** | −0.008 | 0.121 ** | −0.058 | 0.927 ** |
| Model | df | CFI | TLI | RMSEA | SRMR | |
|---|---|---|---|---|---|---|
| Six-factor model: MP, HAB, WM, JS, ED, TI | 279.726 | 89 | 0.985 | 0.979 | 0.057 | 0.027 |
| Five-factor model: MP + HAB, WM, JS, ED, TI | 2246.489 | 94 | 0.827 | 0.779 | 0.187 | 0.116 |
| Five-factor model: MP, HAB, WM + JS, ED, TI | 1017.690 | 94 | 0.926 | 0.905 | 0.122 | 0.052 |
| Five-factor model: MP, HAB, WM, JS, ED + TI | 1200.254 | 94 | 0.911 | 0.886 | 0.134 | 0.081 |
| One-factor model: MP + HAB + WM + JS + ED + TI | 7765.559 | 104 | 0.383 | 0.289 | 0.335 | 0.199 |
| Path | Estimates | S.E. | 95% CI | |
|---|---|---|---|---|
| Mediating effects | MP→WM→JS | −0.087 ** | 0.023 | [−0.135, −0.043] |
| MP→ED→TI | 0.067 ** | 0.020 | [0.032, 0.123] |
| Model | Mistreatment by Patients → Work Meaningfulness → Job Satisfaction | |||
|---|---|---|---|---|
| PMX | Direct Effect (PYX) | Indirect Effect (PYMPMX) | Total Effects (PYX + PYMPMX) | |
| High hostile attribution bias | −0.024 | 0.063 * | −0.013 | 0.050 |
| Low hostile attribution bias | −0.516 ** | −0.140 ** | −0.283 ** | −0.423 ** |
| The difference | 0.492 ** | 0.203 ** | 0.269 ** | 0.473 ** |
| Model | Mistreatment by Patients → Emotional Dissonance → Turnover Intention | |||
|---|---|---|---|---|
| PMX | Direct Effect (PYX) | Indirect Effect (PYMPMX) | Total Effects (PYX + PYMPMX) | |
| High hostile attribution bias | 0.091 * | 0.406 ** | 0.05 * | 0.455 ** |
| Low hostile attribution bias | −0.018 | 0.332 ** | −0.010 | 0.323 ** |
| The difference | 0.108 * | 0.073 | 0.059 * | 0.133 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, L.; Wei, X.; Li, Y.; Liu, B.; Xu, Z. The Influence of Mistreatment by Patients on Job Satisfaction and Turnover Intention among Chinese Nurses: A Three-Wave Survey. Int. J. Environ. Res. Public Health 2020, 17, 1256. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041256
Qi L, Wei X, Li Y, Liu B, Xu Z. The Influence of Mistreatment by Patients on Job Satisfaction and Turnover Intention among Chinese Nurses: A Three-Wave Survey. International Journal of Environmental Research and Public Health. 2020; 17(4):1256. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041256
Chicago/Turabian StyleQi, Lei, Xin Wei, Yuhan Li, Bing Liu, and Zikun Xu. 2020. "The Influence of Mistreatment by Patients on Job Satisfaction and Turnover Intention among Chinese Nurses: A Three-Wave Survey" International Journal of Environmental Research and Public Health 17, no. 4: 1256. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041256