Mobile Dental Delivery System: An Effective Protocol for Hygiene and Disinfection

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Maintenance Protocol
- Remove the reservoir and disinfect it by soaking (as well as its cap) in a solution of Aniosyme X3© (Anios) for 5 min, in a tray dedicated to reservoirs.
- Rinse this reservoir and its cap with bacteriologically controlled water (tap provided with a bacteria filter), dry it with medical air, close it with its cap, and package it in a sterile pouch in order to stock it in clean and dry conditions.
- Fill another clean and disinfected reservoir with sterile water and Calbenium© at a concentration of 2%. Put it in place in the MDDS.
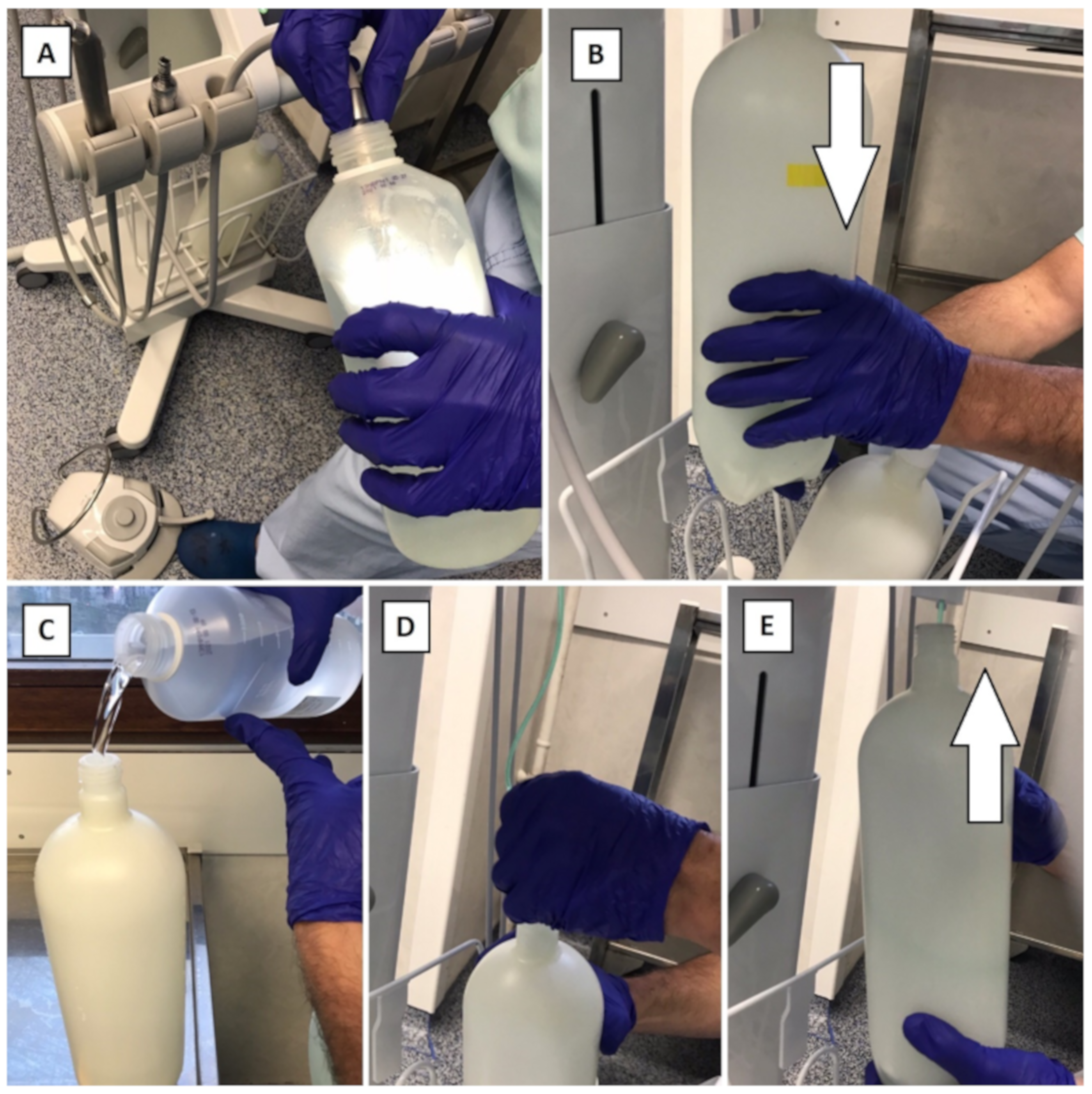
- Purge the air/water spray and the handpiece hoses for 1 min each in the suction can (Figure 3A).
- Leave for 5 min to act.
- During that time, remove the reservoir that contains the Calbenium© solution (which will not be used for the dental procedures), close it tight, and keep it for the next purges during the same session (Figure 3B).
- Put in place a reservoir, clean and disinfected, filled with sterile water (Figure 3C–E).
- Purge the air/water spray and the handpiece hoses in the suction can for 30 seconds each, to remove the Calbenium© from the DUWL.
- Clean and disinfect the surfaces using a detergent-disinfectant product.
- Remove the reservoir and disinfect it by soaking (as well as its cap) in a solution of Aniosyme X3© during 5 min, in a tray dedicated to reservoirs.
- Rinse this reservoir and its cap with bacteriologically controlled water (tap provided with a bacteria filter), dry it with medical air, close it with its cap, and package it in a sterile pouch to stock it in clean and dry conditions.
- Put in place the reservoir that contains the 2% Calbenium© solution.
- Purge the air/water spray and the handpiece hoses in the suction can for 30 seconds each, before disconnecting and treating dental handpieces (Figure 3A).
- Leave for 5 min to act.
- During that time, remove the reservoir that contains the Calbenium© solution (Figure 3B), which will not be used for the dental procedures, close it tight, and keep it for the next purges during the same session.
- Put a reservoir in place, clean and disinfected, filled with sterile water (Figure 3C–E).
- Purge the air/water spray and the handpiece hoses in the suction can for 30 s each, in order to remove the Calbenium© from the DUWL.
- Clean and disinfect the surfaces using a detergent-disinfectant product.
- Remove the reservoir and disinfect it by soaking (as well as its cap) in a solution of Aniosyme X3© for 5 min, in a tray dedicated to reservoirs.
- Rinse this reservoir and its cap with bacteriologically controlled water (tap provided with a bacteria filter), dry it with medical air, close it with its cap, and package it in a sterile pouch in order to stock it in clean and dry conditions.
- Put in place the reservoir that contains the 2% Calbenium© solution.
- Purge the air/water spray and the handpiece hoses in the suction can for 30 s each, before disconnecting and treating dental handpieces (Figure 3A).
- Leave for 5 min to act.
- Remove the reservoir that contains the Calbenium© solution (Figure 3B) and disinfect it by soaking (as well as its cap) in a solution of Aniosyme X3© for 5 min in a tray dedicated to reservoirs.
- Rinse this reservoir and its cap with bacteriologically controlled water (tap provided with a bacteria filter), dry it with medical air, close it with its cap, and package it in a sterile pouch in order to stock it in clean and dry conditions.
- Put a reservoir in place, clean, disinfected, and empty.
- Drain the DUWL with air for 30 s. Leave the reservoir in place.
- Clean and disinfect the surfaces using a detergent and a disinfectant.
2.2. Study Design
- -
- J0, after a first realization of the maintenance protocol (“Between each patient” part), and before the first effective use of the MDDS in patients.
- -
- J0 + 1 month, J0 + 3 months, J0 + 6 months, J0 + 12 months, and J0 + 24 months, to monitor the evolution of a potential contamination.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vashishtha, V.; Kote, S.; Basavaraj, P.; Singla, A.; Pandita, V.; Ravneet, K.M. Reach the unreached—A systematic review on mobile dental units. J. Clin. Diagn. Res. 2014, 8, 5–8. [Google Scholar] [CrossRef]
- Ganavadiya, R.; Chandrashekar, B.R.; Goel, P.; Honqal, S.G.; Jain, M. Mobile and portable dental services catering to the basic oral health needs of the underserved population in developing countries: A proposed model. Ann. Med. Health Sci. Res. 2014, 4, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Goel, P.; Goel, A.; Torwane, N.A. Cost-efficiency of indigenously fabricated mobile-portable dental unit in delivery of primary healthcare in rural India. J. Clin. Diagn. Res. 2014, 8, 6–9. [Google Scholar]
- Mortier, S.D.; Marlene, M.; Ahmed, B.; Pierre, P. Mobile health units-Methodological approach. Int. Comm. Red Cross 2006, 1, 27. [Google Scholar]
- Mulligan, R.; Seirawan, H.; Faust, S.; Habibian, M. Mobile dental clinic: An oral health care delivery model for underserved migrant children. J. Calif. Dent. Assoc. 2010, 38, 115–122. [Google Scholar] [PubMed]
- Dougherty, N. The dental patient with special needs: A review of indications for treatment under general anesthesia. Spec. Care Dent. 2009, 29, 17–20. [Google Scholar] [CrossRef]
- Savanheimo, N.; Sundberg, S.A.; Virtanen, J.I.; Vehkalahti, M.M. Dental care and treatments provided under general anaesthesia in the Helsinki Public Dental Service. BMC Oral Health 2012, 12, 45. [Google Scholar] [CrossRef] [Green Version]
- Park, J.S.; Anthonappa, R.P.; King, N.M.; McGrath, C. The family impact of dental general anaesthesia in children: A meta-analysis. Int. J. Paediatr. Dent. 2019, 29, 149–161. [Google Scholar] [CrossRef]
- Enever, G.R.; Nunn, J.H.; Sheehan, J.K. A comparison of post-operative morbidity following outpatient dental care under general anaesthesia in paediatric patients with and without disabilities. Int. J. Paediatr. Dent. 2000, 10, 120–125. [Google Scholar] [CrossRef]
- Jamjoom, M.M.; al-Malik, M.I.; Holt, R.D.; el-Nassry, A. Dental treatment under general anaesthesia at a hospital in Jeddah, Saudi Arabia. Int. J. Paediatr. Dent. 2001, 11, 110–116. [Google Scholar] [CrossRef]
- Jamieson, L.M.; Roberts-Thomson, K.F. Dental general anaesthetic trends among Australian children. BMC Oral Health 2006, 61, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loyola-Rodriguez, J.P.; Zavala-Alonso, V.; Gonzalez-Alvarez, C.L.; Juarez-Lopez, L.A.; Patiño-Marin, N.; Gonzalez, C.D. Dental treatment under general anesthesia in healthy and medically compromised/developmentally disabled children: A comparative study. J. Clin. Pediatric Dent. 2009, 34, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Attri, J.P.; Sharan, R.; Makkar, V.; Gupta, K.K.; Khetarpal, R.; Kataria, A.P. Conscious sedation: Emerging trends in pediatric dentistry. Anesth. Essays Res. 2017, 11, 277–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atan, S.; Ashely, P.; Gilthorpe, M.S.; Scheer, B.; Mason, C.; Roberts, G. Morbidity following dental treatment of children under intubation general anesthesia in a day-stay unit. Int. J. Paediatr. Dent. 2004, 14, 9–16. [Google Scholar] [CrossRef]
- Li, G.; Warner, M.; Lang, B.H.; Huang, L.; Sun, L.S. Epidemiology of anesthesia-related mortality in the United States, 1999-2005. Anesthesiology 2009, 110, 759–765. [Google Scholar] [CrossRef] [Green Version]
- North, S.; Davidson, L.E.; Blinkhorn, A.S.; Mackie, I.C. The effects of a long wait for children’s dental general anaesthesia. Int. J. Paediatr. Dent. 2007, 17, 105–109. [Google Scholar] [CrossRef]
- Boehmer, J.; Stoffels, J.A.; Van Rooij, I.A.; Heyboer, A. Complications due to the waiting period for dental treatment under general anaesthesia [article in dutch]. Ned. Tijdschr. Tandheelkd. 2007, 114, 69–75. [Google Scholar]
- Albadri, S.S.; Lee, S.; Lee, G.T.; Llewelyn, R.; Blinkhorn, A.S.; Mackie, I.C. The use of general anaesthesia for the extraction of children’s teeth. Results from two UK dental hospitals. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2006, 7, 110–115. [Google Scholar] [CrossRef]
- Lewis, C.W.; Nowak, A.J. Stretching the safety net too far waiting times for dental treatment. Pediatric Dent. 2002, 24, 6–10. [Google Scholar]
- Foster Page, L.A. Retrospective audit of Taranaki children undergoing dental care under general anaesthetic from 2001 to 2005. N. Z. Dent. J. 2009, 105, 8–12. [Google Scholar]
- Haubek, D.; Fugslang, M.; Poulsen, S.; Rølling, I. Dental treatment of children referred to general Anaesthesia—Association with country of origin and medical status. Int. J. Paediatr. Dent. 2006, 16, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.D.; Chidiac, R.H.; Rule, D.C. Dental treatment for children under general anaesthesia in day care facilities at a London dental hospital. Br. Dent. J. 1991, 170, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Laino, L.; Cicciù, >M; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Surgical Risk on Patients with Coagulopathies: Guidelines on Hemophiliac Patients for Oro-Maxillofacial Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Offner, D.; Deboscker, S.; Belotti, L.; Brisset, L.; Lavigne, T.; Musset, A.M. Elaboration et évaluation d’un protocole d’entretien des units et fauteuils dentaire (ADEC® et Planmeca®) aux Hôpitaux Universitaires de Strasbourg. Hygiènes 2013, 21, 21–28. [Google Scholar]
- Offner, D.; Musset, A.M. Hygiene management of dental units: Speaking about patients’ safety. Rev. Odontostomatol. 2018, 47, 158–171. [Google Scholar]
- Offner, D.; Iltis, L.; Bertrand, A.; Musset, A.M. L’hygiène des tuyaux d’aspiration de l’unit dentaire, étude comparative de l’impact de leur structure et entretien. Inf. Dent. 2015, 18, 12–17. [Google Scholar]
- Ricci, M.L.; Fontana, S.; Pinci, F.; Fiumana, E.; Pedna, M.F.; Farolfi, P.; Sabattini, M.A.B.; Scaturro, M. Pneumonia associated with a dental unit waterline. Lancet 2012, 379, 684. [Google Scholar] [CrossRef]
- Smith, G.; Smith, A. Microbial contamination of used dental handpieces. Am. J. Infect. Control 2014, 42, 1019–1021. [Google Scholar] [CrossRef]
- Coleman, D.C.; O’Donnell, M.J.; Shore, A.C.; Russell, R.J. Biofilm problems in dental unit water systems and its practical control. J. Appl. Microbiol. 2008, 106, 1424–1437. [Google Scholar] [CrossRef]
- Offner, D.; Fioretti, F.; Musset, A.M. Contamination of dental unit waterlines: Assessment of three continuous water disinfection systems. BDJ Open 2016, 2, 16007. [Google Scholar] [CrossRef]
- Offner, D.; Brisset, L.; Musset, A.M. Evaluation of the mechanical cleaning efficacy of dental handpieces. J. Hosp. Infect. 2018. [Google Scholar] [CrossRef] [PubMed]
- Nikaeen, M.; Hatamzadeh, M.; Sabzevari, Z.; Zareh, O. Microbial quality of water in dental unit waterlines. J. Res. Med. Sci. 2009, 14, 297–300. [Google Scholar] [PubMed]
- French Society for the History of Dentistry (SFHAD). Histoire de L’aménagement Opératoire du Cabinet Dentaire. L’instrumentation: Les “Outils à Dents” des Nécessaires de Biennais. L’énigme du Nécessaire Dentaire de L’empereur de la Fondation Napoléon. Available online: https://www.biusante.parisdescartes.fr/sfhad/cab_txt03x7.htm (accessed on 20 February 2020).
- French Society for the History of Dentistry (SFHAD). Histoire de L’aménagement Opératoire du Cabinet Dentaire. Les Années 1960. Les Pionniers du Travail en Posture Assise. Malençon, Comhaire: Le Renouveau de L’esprit Créatif Européen. Les Recherches de L’ecole Américaine: Le Réaménagement de L’agencement Opératoire. Available online: https://www.biusante.parisdescartes.fr/sfhad/cab_txt23.htm (accessed on 20 February 2020).
- Iwai, T.; Goto, T.; Matsui, Y.; Tohnai, I. Endoscopic removal of throat-packing gauze swallowed during general anesthesia. J. Craniofac. Surg. 2012, 23, 1547–1549. [Google Scholar] [CrossRef] [Green Version]
- European Council. Council directive 98/83/EC of 3 November 1998 on the quality of water intended for human consumption. Off. J. Eur. Commun. 1998, L330, 32–54. [Google Scholar]
- ISO 6222. In Water Quality—Enumeration of Culturable Micro-Organisms—Colony Count by Inoculation in a Nutrient Agar Culture Medium; International Standard Organization: Geneva, Switzerland, 1999.
- ISO 9308-1. In Water Quality—Enumeration of Escherichia Coli and Coliform Bacteria—Part 1: Membrane Filtration Method for Waters with Low Bacterial Background Flora; International Standard Organization: Geneva, Switzerland, 2014.
- ISO 16266. In Water Quality—Detection and Enumeration of Pseudomonas Aeruginosa—Method by Membrane Filtration; International Standard Organization: Geneva, Switzerland, 2006.
- Petti, S.; Moroni, C.; Messano, G.A.; Polimeni, A. Detection of oral streptococci in dental unit water lines after therapy with air turbine handpiece: Biological fluid retraction more frequent than expected. Future Microbiol. 2013, 8, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Statement on Dental Unit Waterlines. American Dental Association. Last Updated: 20 March 2019. Available online: https://www.ada.org/en/member-center/oral-health-topics/dental-unit-waterlines (accessed on 20 February 2020).
- Barbeau, J.; Gauthier, C.; Payment, P. Biofilms, infectious agents, and dental unit waterlines: A review. Can. J. Microbiol. 1998, 44, 1019–1028. [Google Scholar] [CrossRef]
- Wirthlin, M.R.; Marshall, G.W., Jr.; Rowland, R.W. Formation and decontamination of biofilms in dental unit waterlines. J. Periodontol. 2003, 74, 1595–1609. [Google Scholar] [CrossRef]
- Pawar, A.; Garg, S.; Mehta, S.; Dang, R. Breaking the Chain of Infection: Dental Unit Water Quality Control. J. Clin. Diagn. Res. 2016, 10, ZC80–ZC84. [Google Scholar] [CrossRef]
- Alkhulaifi, M.M.; Alotaibi, D.H.; Alajlan, H.; Binshoail, T. Assessment of nosocomial bacterial contamination in dental unit waterlines: Impact of flushing. Saudi Dent. J. 2020, 32, 68–73. [Google Scholar] [CrossRef]
- Wirthlin, M.R.; Roth, M. Dental unit waterline contamination: A review of research and findings from a clinic setting. Compend. Contin. Educ. Dent. 2015, 36, 216–219. [Google Scholar]
- Fiorillo, L. We Do Not Eat Alone: Formation and Maturation of the Oral Microbiota. Biology 2020, 9, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Microorganisms Sought | Volume Analyzed | Maximum Storage Duration before Analysis Recommended (h) | Maximum Storage Duration before Analysis Accepted (h) | Storage Temperature (°C) before Analysis | Samples Seeding Conditions | Standard |
|---|---|---|---|---|---|---|
| Viable aerobic MO at 22°C | 1 mL | 8 | 12 | 5 ± 3 | 72 h at 22 °C on agar PCA by inclusion | ISO 6222 [37] |
| viable aerobic MO at 37°C | 1 mL | 8 | 12 | 5 ± 3 | 48 h at 36 °C on agar PCA by inclusion | ISO 6222 [37] |
| Coliform bacteria and Escherichia coli | 100 mL | 8 | 18 | 5 ± 3 | 24 h at 36 °C on agar TTC by membrane filtration, 2nd inspection after 48 h | ISO 9308-1 [38] |
| Pseudomonas aeruginosa | 100 mL | 8 | 12 | 5 ± 3 or ambient (≤25) | 48 h at 36 °C on cetrimide agar by membrane filtration | ISO 16266 [39] |
| Microorganisms Sought | J0 | J0 + 1 Month | J0 + 3 Months | J0 + 6 Months | J0 + 12 Months | J0 + 24 Months | Target Level |
|---|---|---|---|---|---|---|---|
| Viable aerobic MO at 22 °C | <1 | <1 | <1 | <1 | <1 | <1 | ≤100 cfu/mL |
| Viable aerobic MO at 37 °C | <1 | <1 | <1 | <1 | <1 | <1 | ≤10 cfu/mL |
| Coliform bacteria and E. coli | <1 | <1 | <1 | <1 | <1 | <1 | <1 cfu/100mL |
| Pseudomonas aeruginosa | <1 | <1 | <1 | <1 | <1 | <1 | <1 cfu/100mL |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Offner, D.; Fernandez De Grado, G.; Strub, M.; Belotti, L.; Deboscker, S.; Musset, A.-M. Mobile Dental Delivery System: An Effective Protocol for Hygiene and Disinfection. Int. J. Environ. Res. Public Health 2020, 17, 1603. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051603
Offner D, Fernandez De Grado G, Strub M, Belotti L, Deboscker S, Musset A-M. Mobile Dental Delivery System: An Effective Protocol for Hygiene and Disinfection. International Journal of Environmental Research and Public Health. 2020; 17(5):1603. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051603
Chicago/Turabian StyleOffner, Damien, Gabriel Fernandez De Grado, Marion Strub, Laure Belotti, Stéphanie Deboscker, and Anne-Marie Musset. 2020. "Mobile Dental Delivery System: An Effective Protocol for Hygiene and Disinfection" International Journal of Environmental Research and Public Health 17, no. 5: 1603. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051603