Prenatal Manganese Exposure and Long-Term Neuropsychological Development at 4 Years of Age in a Population-Based Birth Cohort

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
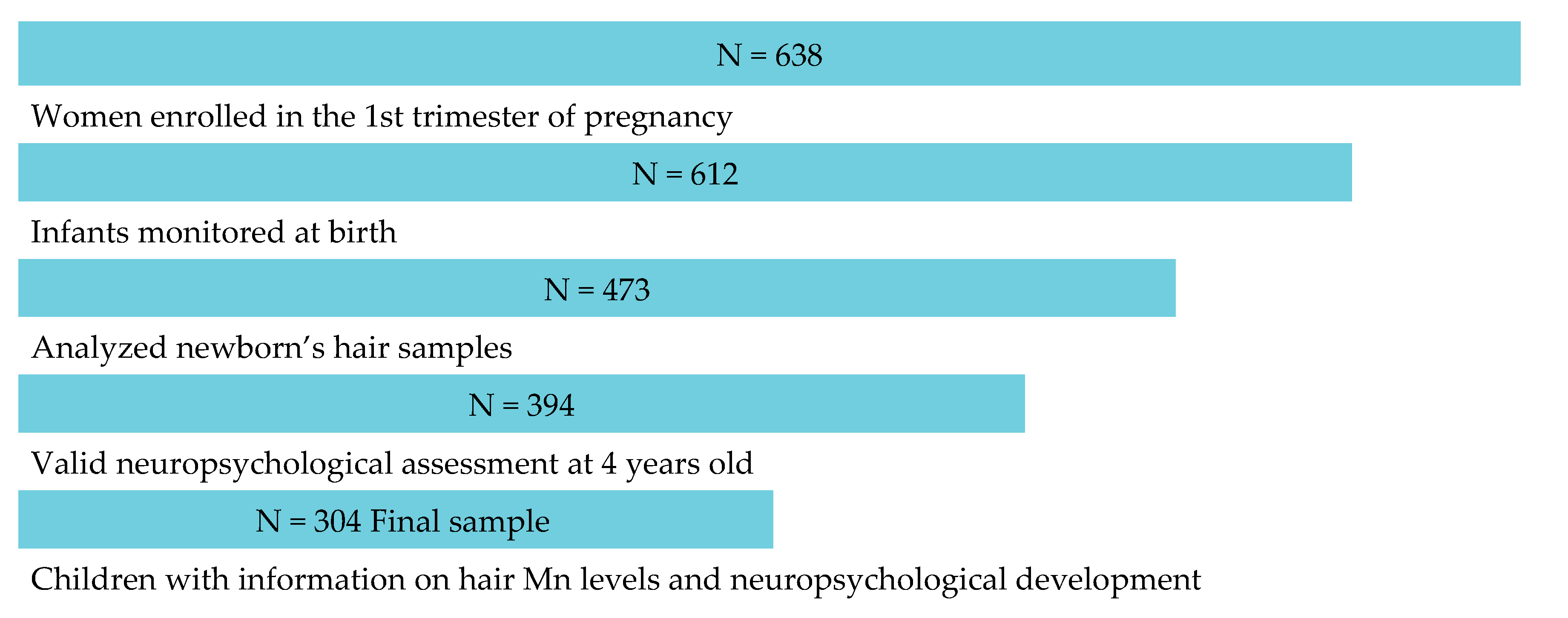
2.1. Study Design and Participants
2.2. Manganese in Hair
2.3. Children’s Neuropsychological Development
2.4. Potential Confounding or Predictor Variables
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chung, S.E.; Cheong, H.K.; Ha, E.H.; Kim, B.N.; Ha, M.; Kim, Y.; Hong, Y.C.; Park, H.; Oh, S.Y. Maternal Blood Manganese and Early Neurodevelopment: The Mothers and Children’s Environmental Health (MOCEH) Study. Environ. Health Perspect. 2015, 123, 717–722. [Google Scholar] [CrossRef] [Green Version]
- Wood, R.J. Manganese and birth outcome. Nutr. Rev. 2009, 67, 416–420. [Google Scholar] [CrossRef]
- Zota, A.R.; Ettinger, A.S.; Bouchard, M.; Amarasiriwardena, C.J.; Schwartz, J.; Hu, H.; Wright, R.O. Maternal blood manganese levels and infant birth weight. Epidemiology 2009, 20, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Mistry, H.D.; Williams, P.J. The importance of antioxidant micronutrients in pregnancy. Oxid. Med. Cell Longev. 2011, 2011, 841749. [Google Scholar] [CrossRef] [Green Version]
- Grandjean, P.; Landrigan, P.J. Neurobehavioural effects of developmental toxicity. Lancet Neurol. 2014, 13, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Haynes, E.N.; Sucharew, H.; Kuhnell, P.; Alden, J.; Barnas, M.; Wright, R.O.; Parsons, P.J.; Aldous, K.M.; Praamsma, M.L.; Beidler, C.; et al. Manganese Exposure and Neurocognitive Outcomes in Rural School-Age Children: The Communities Actively Researching Exposure Study (Ohio, USA). Environ. Health Perspect. 2015, 123, 1066–1071. [Google Scholar] [CrossRef]
- Nadaska, A.G.; Lesny, J.; Michalik, I. Environmental aspect of manganese chemistry. Hung. J. Sci. 2010, 100702, 1–16. [Google Scholar]
- ATSDR. Toxicological Profile for Manganese. U.S. Department of Health and Human Services, Public Health Service, ATSDR, Atlanta, GA. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp151.pdf (accessed on 6 June 2019).
- Bouchard, M.; Laforest, F.; Vandelac, L.; Bellinger, D.; Mergler, D. Hair manganese and hyperactive behaviors: Pilot study of school-age children exposed through tap water. Environ. Health Perspect. 2007, 115, 122–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, C.F.; Menezes-Filho, J.A.; de Matos, V.P.; Bessa, J.R.; Coelho-Santos, J.; Viana, G.F.; Argollo, N.; Abreu, N. Elevated airborne manganese and low executive function in school-aged children in Brazil. Neurotoxicology 2014, 45, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.; Wasserman, G.A.; Liu, X.; Ahmed, E.; Parvez, F.; Slavkovich, V.; Levy, D.; Mey, J.; van Geen, A.; Graziano, J.H.; et al. Manganese exposure from drinking water and children’s academic achievement. Neurotoxicology 2012, 33, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Agustín, R.; Rodríguez-Agudelo, Y.; Schilmann, A.; Solís-Vivanco, R.; Montes, S.; Riojas-Rodríguez, H.; Cortez-Lugo, M.; Ríos, C. Effect of environmental manganese exposure on verbal learning and memory in Mexican children. Environ. Res. 2013, 121, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Gulson, B.; Mizon, K.; Taylor, A.; Korsch, M.; Stauber, J.; Davis, J.M.; Louie, H.; Wu, M.; Swan, H. Changes in manganese and lead in the environment and young children associated with the introduction of methylcyclopentadienyl manganese tricarbonyl in gasoline—Preliminary results. Environ. Res. 2006, 100, 100–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunier, R.B.; Arora, M.; Jerrett, M.; Bradman, A.; Harley, K.G.; Mora, A.M.; Kogut, K.; Hubbard, A.; Austin, C.; Holland, N.; et al. Manganese in teeth and neurodevelopment in young Mexican-American children. Environ. Res. 2015, 142, 688–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora, A.M.; Arora, M.; Harley, K.G.; Kogut, K.; Parra, K.; Hernández-Bonilla, D.; Gunier, R.B.; Bradman, A.; Smith, D.R.; Eskenazi, B. Prenatal and postnatal manganese teeth levels and neurodevelopment at 7, 9, and 10.5 years in the CHAMACOS cohort. Environ. Int. 2015, 84, 39–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, G.A.; Liu, X.; Parvez, F.; Ahsan, H.; Levy, D.; Factor-Litvak, P.; Kline, J.; van Geen, A.; Slavkovich, V.; Lolacono, N.J.; et al. Water manganese exposure and children’s intellectual function in Araihazar, Bangladesh. Environ. Health Perspect. 2006, 114, 124–129. [Google Scholar] [CrossRef] [Green Version]
- Freeland-Graves, J.H.; Mousa, T.Y.; Kim, S. International variability in diet and requirements of manganese: Causes and consequences. J. Trace Elem. Med. Biol. 2016, 38, 24–32. [Google Scholar] [CrossRef]
- Koivistoinen, P. (Ed.) Mineral element composition of Finnish foods: N, K, Ca, Mg, P, S, Fe, Cu, Mn, Zn, Mo, Co, Ni, Cr, F, Se, Si, Rb, Al, B, Br, Hg, As, Cd, Pb, and ash. In Acta Agriculturae Scandinavica Supplementum 22; Scandinavian Association of Agricultural Scientists and the Royal Swedish Academy of Agriculture and Forestry: Stockholm, Sweden, 1980. [Google Scholar]
- Irizar, A.; Gil, F.; Lertxundi, A.; Martín-Domingo, M.C.; Urbieta, N.; Molinuevo, A.; Ibarluzea, J.; Basterrechea, M.; Aurrekoetxea, J.J.; Jiménez-Zabala, A.; et al. Manganese levels in newborns’ hair by maternal sociodemographic, dietary and environmental factors. Environ. Res. 2019, 170, 92–100. [Google Scholar] [CrossRef]
- Mena, I.; Horiuchi, K.; Lopez, G. Factors enhancing entrance of manganese into brain: Iron deficiency and age. J. Nucl. Med. 1974, 15, 516. [Google Scholar]
- Aschner, M. Manganese: Brain transport and emerging research needs. Environ. Health Perspect. 2000, 108 (Suppl. 3), S429–S432. [Google Scholar]
- U.S. EPA. Report on the 2015 U.S. Environmental Protection Agency (EPA) International Decontamination Research and Development Conference; Environmental Protection Agency: Washington, DC, USA, 2015. [Google Scholar]
- Leonhard, M.J.; Chang, E.T.; Loccisano, A.E.; Garry, M.R. A systematic literature review of epidemiologic studies of developmental manganese exposure and neurodevelopmental outcomes. Toxicology 2019, 420, 46–65. [Google Scholar] [CrossRef]
- Menezes-Filho, J.A.; Novaes, C.D.O.; Moreira, J.C.; Sarcinelli, P.N.; Mergler, D. Elevated manganese and cognitive performance in school-aged children and their mothers. Environ. Res. 2011, 111, 156–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchard, M.F.; Sauvé, S.; Barbeau, B.; Legrand, M.; Brodeur, M.È.; Bouffard, T.; Limoges, E.; Bellinger, D.C.; Mergler, D. Intellectual impairment in school-age children exposed to manganese from drinking water. Environ. Health Perspect. 2011, 119, 138–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, R.O.; Amarasiriwardena, C.; Woolf, A.D.; Jim, R.; Bellinger, D.C. Neuropsychological correlates of hair arsenic, manganese, and cadmium levels in school-age children residing near a hazardous waste site. Neurotoxicology 2006, 27, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Riojas-Rodríguez, H.; Solís-Vivanco, R.; Schilmann, A.; Montes, S.; Rodríguez, S.; Ríos, C.; Rodríguez-Agudelo, Y. Intellectual function in Mexican children living in a mining area and environmentally exposed to manganese. Environ. Health Perspect. 2010, 118, 1465–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oulhote, Y.; Mergler, D.; Barbeau, B.; Bellinger, D.C.; Bouffard, T.; Brodeur, M.È.; Saint-Amour, D.; Legrand, M.; Sauvé, S.; Bouchard, M.F. Neurobehavioral function in school-age children exposed to manganese in drinking water. Environ. Health Perspect. 2014, 122, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Rink, S.M.; Ardoino, G.; Queirolo, E.I.; Cicariello, D.; Mañay, N.; Kordas, K. Associations between hair manganese levels and cognitive, language, and motor development in preschool children from Montevideo, Uruguay. Arch. Environ. Occup. Health 2014, 69, 46–54. [Google Scholar] [CrossRef]
- Coetzee, D.J.; McGovern, P.M.; Rao, R.; Harnack, L.J.; Georgieff, M.K.; Stepanov, I. Measuring the impact of manganese exposure on children’s neurodevelopment: Advances and research gaps in biomarker-based approaches. Environ. Health 2016, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.C.; Chen, Y.C.; Su, F.C.; Lin, C.M.; Liao, H.F.; Hwang, Y.H.; Hsieh, W.S.; Jeng, S.F.; Su, Y.N.; Chen, P.C. In utero exposure to environmental lead and manganese and neurodevelopment at 2 years of age. Environ. Res. 2013, 123, 52–57. [Google Scholar] [CrossRef]
- Takser, L.; Mergler, D.; Hellier, G.; Sahuquillo, J.; Huel, G. Manganese, monoamine metabolite levels at birth, and child psychomotor development. Neurotoxicology 2003, 24, 667–674. [Google Scholar] [CrossRef]
- Rahman, S.M.; Kippler, M.; Tofail, F.; Bölte, S.; Derakhshani Hamadani, J.; Vahter, M. Manganese in Drinking Water and Cognitive Abilities and Behavior at 10 Years of Age: A Prospective Cohort Study. Environ. Health Perspect. 2017, 125, 057003. [Google Scholar] [CrossRef]
- Lucchini, R.G.; Guazzetti, S.; Zoni, S.; Donna, F.; Peter, S.; Zacco, A.; Salmistraro, M.; Bontempi, E.; Zimmerman, N.J.; Smith, D.R. Tremor, olfactory and motor changes in Italian adolescents exposed to historical ferro-manganese emission. Neurotoxicology 2012, 33, 687–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guxens, M.; Ballester, F.; Espada, M.; Fernández, M.F.; Grimalt, J.O.; Ibarluzea, J.; Olea, N.; Rebagliato, M.; Tardón, A.; Torrent, M.; et al. Cohort Profile: The INMA—INfancia y Medio Ambiente—(Environment and Childhood) Project. Int. J. Epidemiol. 2012, 41, 930–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil, F.; Hernández, A.F. Toxicological importance of human biomonitoring of metallic and metalloid elements in different biological samples. Food Chem. Toxicol. 2015, 80, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Molina-Villlalba, I.; Lacasaña, M.; Rodriguez-Barranco, M.; Hernandez, A.; Gonzalez-Alzaga, B.; Aguilar-Garduño, C.; Gil, F. Biomonitoring of arsenic, cadmium, lead, manganese and mercury in urine and hair of children living near mining and industrial areas. Chemosphere 2015, 24, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Olmedo, P.; Pla, A.; Hernández, A.F.; López-Guarnido, O.; Rodrigo, L.; Gil, F. Validation of a method to quantify chromium, cadmium, manganese, nickel and lead in human whole blood, urine, saliva and hair samples by electrothermal atomic absorption spectrometry. Anal. Chim. Acta 2010, 659, 60–67. [Google Scholar] [CrossRef]
- McCarthy, D. MSCA. Escalas McCarthy de Aptitudesy Psicomotricidad para Niños; TEA Ediciones: Madrid, Spain, 2009. [Google Scholar]
- Andiarena, A.; Balluerka, N.; Gorostiaga, A.; Ibarluzea, J. Neuropsychological Assessment at Preschool Age: Adaptation and Validation of the McCarthy Scales of Children’s Abilities to 4 Year-old Basque-speaking Children. Span. J. Psychol. 2017, 20, E49. [Google Scholar] [CrossRef]
- Julvez, J.; Forns, M.; Ribas-Fitό, N.; Torrent, M.; Sunyer, J. Attention behavior and hyperactivity and concurrent neurocognitive and social competence functioning in 4-year-olds from two population-based birth cohorts. Eur. Psychiatry 2011, 26, 381–389. [Google Scholar] [CrossRef]
- Arija, V.; Hernández-Martínez, C.; Tous, M.; Canals, J.; Guxens, M.; Fernández-Barrés, S.; Ibarluzea, J.; Babarro, I.; Soler-Blasco, R.; Llop, S.; et al. Association of Iron Status and Intake During Pregnancy with Neuropsychological Outcomes in Children Aged 7 Years: The Prospective Birth Cohort Infancia y Medio Ambiente (INMA) Study. Nutrients 2019, 11, 2999. [Google Scholar] [CrossRef] [Green Version]
- Lertxundi, A.; Martinez, M.D.; Ayerdi, M.; Alvarez, J.; Ibarluzea, J.M. Air quality assessment in urban areas of Gipuzkoa (Spain). Gac. Sanit. 2010, 24, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Velasco, D.; Sánchez de Miguel, M.; Egurza, M.; Arranz, E.; Aranbarri, A.; Fano, E.; Ibarluzea, J. Family context assessment in a public health study. Gac. Sanit. 2014, 28, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Barreto, F.B.; Sánchez de Miguel, M.; Ibarluzea, J.; Andiarena, A.; Arranz, E. Family context and cognitive development in early childhood: A longitudinal study. Intelligence 2017, 65, 11–22. [Google Scholar] [CrossRef]
- Erikson, K.M.; Thompson, K.; Aschner, J.; Aschner, M. Manganese neurotoxicity: A focus on the neonate. Pharmacol. Ther. 2007, 113, 369–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soler-Blasco, R.; Murcia, M.; Lozano, M.; González-Safont, L.; Amorós, R.; Ibarluzea, J.; Broberg, K.; Irizar, A.; Lopez-Espinosa, M.J.; Lertxundi, N.; et al. Prenatal manganese exposure and effects on neuropsychological development in early childhood in the INMA cohort. Int. J. Hygiene Environ. Health 2020, 224, 113443. [Google Scholar] [CrossRef]
- Eastman, R.R.; Jursa, T.P.; Benedetti, C.; Lucchini, R.G.; Smith, D.R. Hair as a biomarker of environmental manganese exposure. Environ. Sci. Technol. 2013, 47, 1629–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora, A.M.; Córdoba, L.; Cano, J.C.; Hernandez-Bonilla, D.; Pardo, L.; Schnaas, L.; Smith, D.R.; Menezes-Filho, J.A.; Mergler, D.; Lindh, C.H.; et al. Prenatal Mancozeb Exposure, Excess Manganese, and Neurodevelopment at 1 Year of Age in the Infants’ Environmental Health (ISA) Study. Environ. Health Perspect. 2018, 126, 057007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llop, S.; Lopez-Espinosa, M.J.; Rebagliato, M.; Ballester, F. Gender differences in the neurotoxicity of metals in children. Toxicology 2013, 311, 3–12. [Google Scholar] [CrossRef]
- Arranz Freijo, E.B.; Olabarrieta Artetxe, F.; Manzano Fernández, A.; Martín Ayala, J.L.; Galende Pérez, N. Etxadi-Gangoiti scale: A proposal to evaluate the family contexts of two-year-old children. Early Child Dev. Care 2014, 184, 933–948. [Google Scholar] [CrossRef]
- Boucher, O.; Julvez, J.; Guxens, M.; Arranz, E.; Ibarluzea, J.; Sánchez de Miguel, M.; Fernández-Somoano, A.; Tardon, A.; Rebagliato, M.; Garcia-Esteban, R.; et al. Association between breastfeeding duration and cognitive development, autistic traits and ADHD symptoms: A multicenter study in Spain. Pediatr. Res. 2017, 81, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Do Nascimento, S.N.; Barth, A.; Göethel, G.; Baierle, M.; Charao, M.F.; Brucker, N.; Moro, A.M.; Bubols, G.B.; Sobreira, J.S.; Sauer, E.; et al. Cognitive deficits and ALA-D-inhibition in children exposed to multiple metals. Environ. Res. 2015, 136, 387–395. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N (%) | Mean (sd) | Number of Missing Data | ||
|---|---|---|---|---|
| Maternal characteristics | ||||
| Age | 31.67 (3.3) | 0(0%) | ||
| Educational level | Primary | 38 (12.5%) | 1 (0.33%) | |
| Secondary | 120 (39.47%) | |||
| University | 145 (47.7%) | |||
| Body mass index, kg/m2 | Underweight (<18.5) | 13 (4.28%) | 0 (0%) | |
| Normal weight (>18.5–25) | 231 (75.99%) | |||
| Over weight (26–30) | 45 (14.8%) | |||
| Obese (≥30) | 15 (4.93%) | |||
| Parity | 0 | 167 (54.93%) | 0 (0%) | |
| ≥1 | 116 (45.07%) | |||
| Alcohol consumedin pregnancy | No | 271 (89.10%) | 2 (0.66%) | |
| Yes | 21 (6.91%) | |||
| Smoking in pregnancy | No | 266 (87.5%) | 7 (2.3%) | |
| Yes | 31 (10.20%) | |||
| Ferritin level (μg/L) | 34.54 (26.11) | 1 (0.33%) | ||
| PM2.5 in pregnancy (unit) | 16.98 (2.43) | 22 (7.24%) | ||
| Child characteristics | ||||
| Sex | Male | 153 (50.33%) | 0 (0%) | |
| Female | 151 (49.67%) | |||
| Low birth weight (<2500 g) | No | 292 (96.05%) | 1 (0.33%) | |
| Yes | 11 (3.62%) | |||
| Season of birth | Winter | 87 (28.62%) | 0 (0%) | |
| Autumn | 50 (16.45%) | |||
| Spring | 88 (28.95%) | |||
| Summer | 79 (25.99%) | |||
| Sibling order | First | 169 (55.59%) | 0 (0%) | |
| Other | 135 (44.41%) | |||
| Preterm (<37 weeks) | No | 294 (96.71%) | ||
| Yes | 8 (2.63%) | |||
| Breastfed (weeks) | 29.98 (20.20) | 12 (3.95%) | ||
| Nursery (14 months) | No | 150 (49.34%) | 13 (4.28%) | |
| Yes | 141 (46.38%) | |||
| Passive smoking (14 months) | No | 262 (86.18%) | 0(0%) | |
| Yes | 42 (13.82%) | |||
| Etxadi-Gangoiti Scale (at 2 years) | 73.71 (9.78) | 46 (15.13%) | ||
| Age at assessment (at 4 years) | 4.48 (0.12) | 3 (0.99%) | ||
| Beta (CI 95%) | ||||||||
|---|---|---|---|---|---|---|---|---|
| For a 1−Point Increase in Mn Levels | R2 | AIC | Tertile 1 [0.0065–0.2316] | Tertile 2 (0.2316–0.4093] | Tertile 3 (0.4093–2.1658] | p for Trend | ||
| General cognitive | Model 1 | −1.05 (−6.72, 4.62) | 0.011 | 2272.542 | 1 (Ref.) | 0.18 (−4.26, 4.61) | −0.48 (−4.97, 4.01) | 0.834 |
| Model 2 | 0.36 (−5.23, 5.95) | 0.144 | 2128.497 | 1 (Ref.) | 0.53 (−3.85, 4.9) | 0.12 (−4.29, 4.54) | 0.954 | |
| Verbal | Model 1 | −1.78 (−7.45, 3.88) | 0.014 | 2271.846 | 1 (Ref.) | 0.86 (−3.58, 5.29) | 0.48 (−4.01, 4.97) | 0.833 |
| Model 2 | −0.93 (−6.71, 4.85) | 0.100 | 2145.329 | 1 (Ref.) | 1.58 (−2.94, 6.1) | 0.74 (−3.82, 5.3) | 0.744 | |
| Perceptive−manip. | Model 1 | 0.77 (−4.75, 6.28) | 0.016 | 2257.169 | 1 (Ref.) | −0.41 (−4.72, 3.9) | −0.48 (−4.84, 3.89) | 0.829 |
| Model 2 | 2.24 (−3.27, 7.76) | 0.120 | 2121.771 | 1 (Ref.) | −0.57 (−4.9, 3.75) | 0.23 (−4.13, 4.6) | 0.919 | |
| Quantitative | Model 1 | −2.21 (−7.88, 3.47) | 0.009 | 2272.823 | 1 (Ref.) | −0.56 (−5, 3.88) | −1.07 (−5.57, 3.42) | 0.638 |
| Model 2 | −0.43 (−5.92, 5.06) | 0.160 | 2119.094 | 1 (Ref.) | −0.11 (−4.41, 4.19) | −0.09 (−4.43, 4.24) | 0.966 | |
| Memory | Model 1 | −1.3 (−7.19, 4.58) | 0.006 | 2292.962 | 1 (Ref.) | 1.26 (−3.35, 5.86) | 0.83 (−3.83, 5.49) | 0.726 |
| Model 2 | −0.39 (−6.16, 5.38) | 0.132 | 2144.533 | 1 (Ref.) | 1.68 (−2.83, 6.19) | 1.23 (−3.32, 5.78) | 0.591 | |
| Executive function | Model 1 | −1.43 (−7.05, 4.2) | 0.014 | 2267.655 | 1 (Ref.) | −0.23 (−4.63, 4.17) | −0.27 (−4.73, 4.18) | 0.904 |
| Model 2 | 0.1 (−5.46, 5.65) | 0.120 | 2125.193 | 1 (Ref.) | 0.57 (−3.78, 4.92) | 0.61 (−3.78, 4.99) | 0.784 | |
| Motor global | Model 1 | 0.33 (−5.18, 5.84) | 0.023 | 2256.665 | 1 (Ref.) | 0.26 (−4.05, 4.57) | −0.16 (−4.52, 4.2) | 0.943 |
| Model 2 | 1.9 (−3.74, 7.55) | 0.060 | 2133.311 | 1 (Ref.) | 0.58 (−3.84, 5.01) | 1.12 (−3.34, 5.57) | 0.621 | |
| Gross motor | Model 1 | 3.25 (−2.44, 8.93) | 0.038 | 2273.539 | 1 (Ref.) | 2.21 (−2.23, 6.66) | 2.24 (−2.26, 6.74) | 0.326 |
| Model 2 | 3.57 (−2.1, 9.23) | 0.097 | 2135.314 | 1 (Ref.) | 3.39 (−1.03, 7.81) | 3.42 (−1.04, 7.87) | 0.130 | |
| Fine motor | Model 1 | −2.99 (−8.36, 2.37) | 0.013 | 2241.805 | 1 (Ref.) | −1.98 (−6.17, 2.21) | −2.66 (−6.9, 1.59) | 0.218 |
| Model 2 | −0.94 (−6.23, 4.36) | 0.135 | 2100.425 | 1 (Ref.) | −2.76 (−6.89, 1.38) | −1.98 (−6.14, 2.19) | 0.346 | |
| Beta (CI 95%) | ||||||
|---|---|---|---|---|---|---|
| Fora 1 Point Increase in Mn Levels | Tertile 1 [0.0065–0.2316] | Tertile 2 (0.2316–0.4093] | Tertile 3 (0.4093–2.1658] | p for Trend | ||
| General cognitive | Boys | 0.01 (−7.63, 7.65) | 1 (Ref.) | −0.76 (−7.59, 6.08) | 1.17 (−5.43, 7.77) | 0.727 |
| Girls | 4.56 (−4.01, 13.14) | 1 (Ref.) | 1.32 (−4.39, 7.03) | 1.77 (−4.2, 7.75) | 0.551 | |
| Verbal | Boys | −1.53 (−9.47, 6.42) | 1 (Ref.) | 1.61 (−5.49, 8.71) | 3.01 (−3.85, 9.87) | 0.384 |
| Girls | 2.68 (−6.35, 11.71) | 1 (Ref.) | 1.14 (−4.86, 7.14) | 0.65 (−5.63, 6.93) | 0.826 | |
| Perceptive−manip. | Boys | 3.86 (−3.85, 11.58) | 1 (Ref.) | −2.7 (−9.61, 4.21) | 0.48 (−6.19, 7.16) | 0.892 |
| Girls | 2.9 (−5.53, 11.33) | 1 (Ref.) | 0.86 (−4.74, 6.46) | 1.76 (−4.1, 7.62) | 0.552 | |
| Quantitative | Boys | −3.53 (−10.66, 3.59) | 1 (Ref.) | −2.15 (−8.54, 4.24) | −2.66 (−8.83, 3.51) | 0.392 |
| Girls | 5.82 (−3.06, 14.69) | 1 (Ref.) | 1.8 (−4.08, 7.69) | 4.33 (−1.83, 10.49) | 0.166 | |
| Memory | Boys | −1.1 (−8.35, 6.14) | 1 (Ref.) | 0.96 (−5.52, 7.43) | 2.56 (−3.69, 8.82) | 0.417 |
| Girls | 4.09 (−5.54, 13.72) | 1 (Ref.) | 1.84 (−4.56, 8.25) | 2.37 (−4.32, 9.07) | 0.475 | |
| Executive function | Boys | −2.73 (−10.62, 5.16) | 1 (Ref.) | −1.93 (−9.01, 5.15) | −1.11 (−7.95, 5.72) | 0.745 |
| Girls | 6.12 (−2.08, 14.31) | 1 (Ref.) | 2.34 (−3.1, 7.79) | 4.1 (−1.6, 9.79) | 0.153 | |
| Motor global | Boys | 4.06 (−3.61, 11.73) | 1 (Ref.) | −0.27 (−7.16, 6.62) | 2.03 (−4.62, 8.68) | 0.547 |
| Girls | 0.05 (−8.56, 8.67) | 1 (Ref.) | 2.18 (−3.52, 7.88) | 2.29 (−3.67, 8.26) | 0.436 | |
| Gross motor | Boys | 4.05 (−3.85, 11.96) | 1 (Ref.) | 3.24 (−3.83, 10.31) | 3.98 (−2.85, 10.81) | 0.248 |
| Girls | 2.3 (−6, 10.59) | 1 (Ref.) | 5.15 (−0.27, 10.58) | 4.53 (−1.14, 10.21) | 0.105 | |
| Fine motor | Boys | 1.82 (−5.46, 9.1) | 1 (Ref.) | −3.9 (−10.39, 2.59) | −1.19 (−7.46, 5.07) | 0.702 |
| Girls | −2.39 (−10.78, 5.99) | 1 (Ref.) | −2.22 (−7.78, 3.34) | −1.39 (−7.21, 4.43) | 0.617 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andiarena, A.; Irizar, A.; Molinuevo, A.; Urbieta, N.; Babarro, I.; Subiza-Pérez, M.; Santa-Marina, L.; Ibarluzea, J.; Lertxundi, A. Prenatal Manganese Exposure and Long-Term Neuropsychological Development at 4 Years of Age in a Population-Based Birth Cohort. Int. J. Environ. Res. Public Health 2020, 17, 1665. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051665
Andiarena A, Irizar A, Molinuevo A, Urbieta N, Babarro I, Subiza-Pérez M, Santa-Marina L, Ibarluzea J, Lertxundi A. Prenatal Manganese Exposure and Long-Term Neuropsychological Development at 4 Years of Age in a Population-Based Birth Cohort. International Journal of Environmental Research and Public Health. 2020; 17(5):1665. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051665
Chicago/Turabian StyleAndiarena, Ainara, Amaia Irizar, Amaia Molinuevo, Nerea Urbieta, Izaro Babarro, Mikel Subiza-Pérez, Loreto Santa-Marina, Jesús Ibarluzea, and Aitana Lertxundi. 2020. "Prenatal Manganese Exposure and Long-Term Neuropsychological Development at 4 Years of Age in a Population-Based Birth Cohort" International Journal of Environmental Research and Public Health 17, no. 5: 1665. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051665