A Systematic Literature Review of Factors Affecting the Timing of Menarche: The Potential for Climate Change to Impact Women’s Health


Abstract
:
1. Introduction
2. Materials and Methods
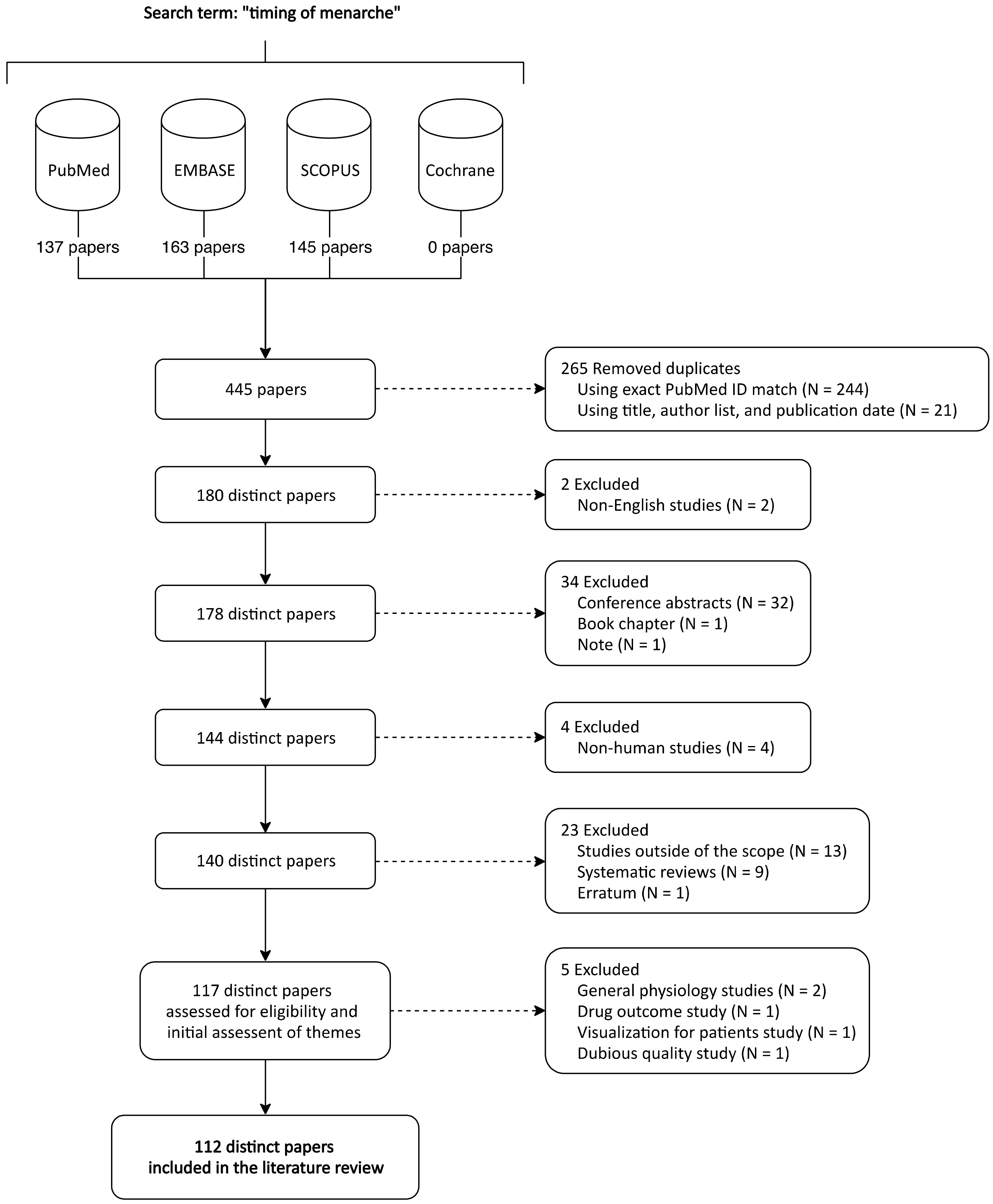
2.1. Systematic Review of Literature
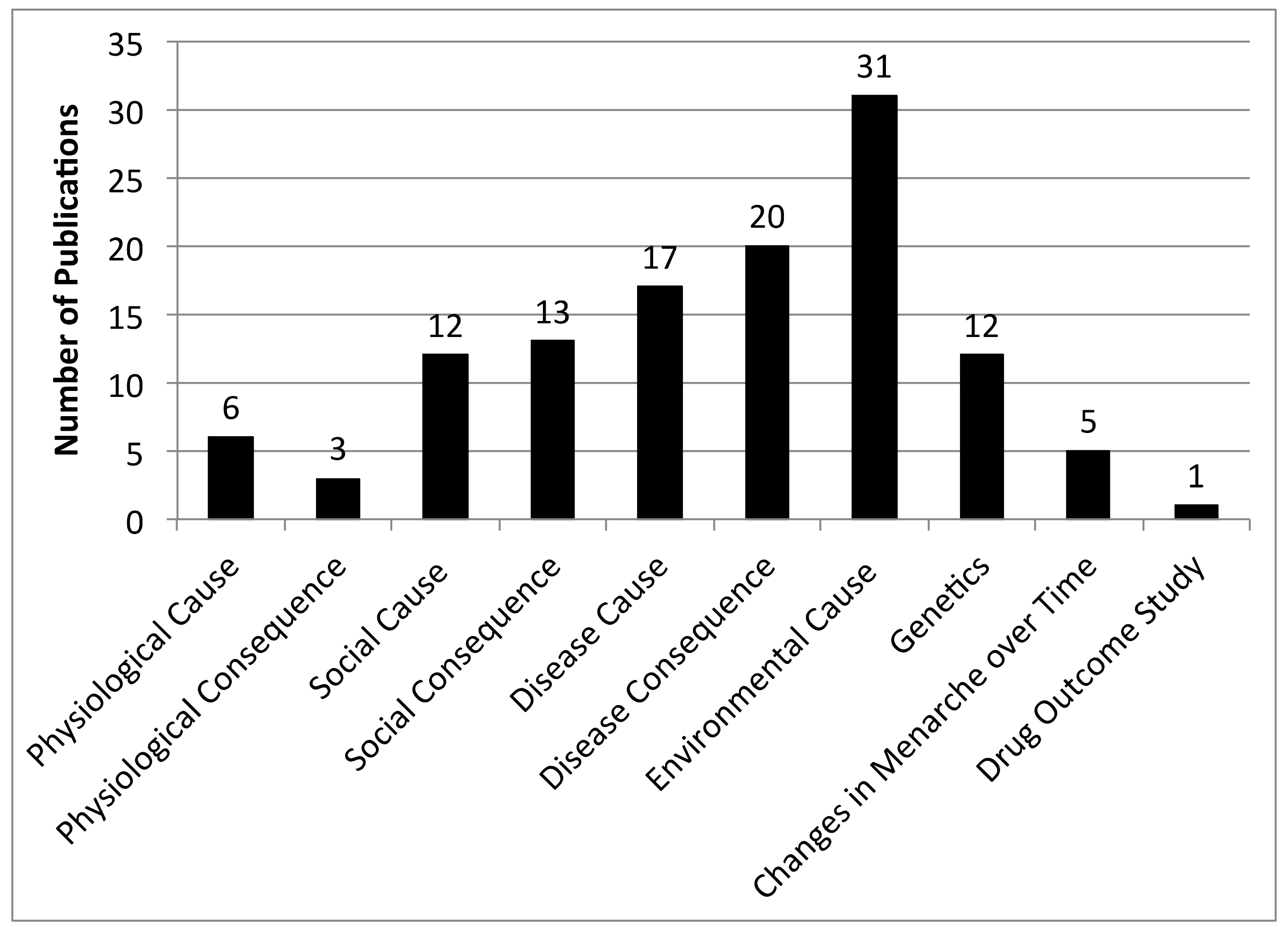
2.2. Identification of Themes
3. Results
3.1. Systematic Review of Literature
3.2. Themes Identified as Important for Understanding a Woman’s Timing of Menarche
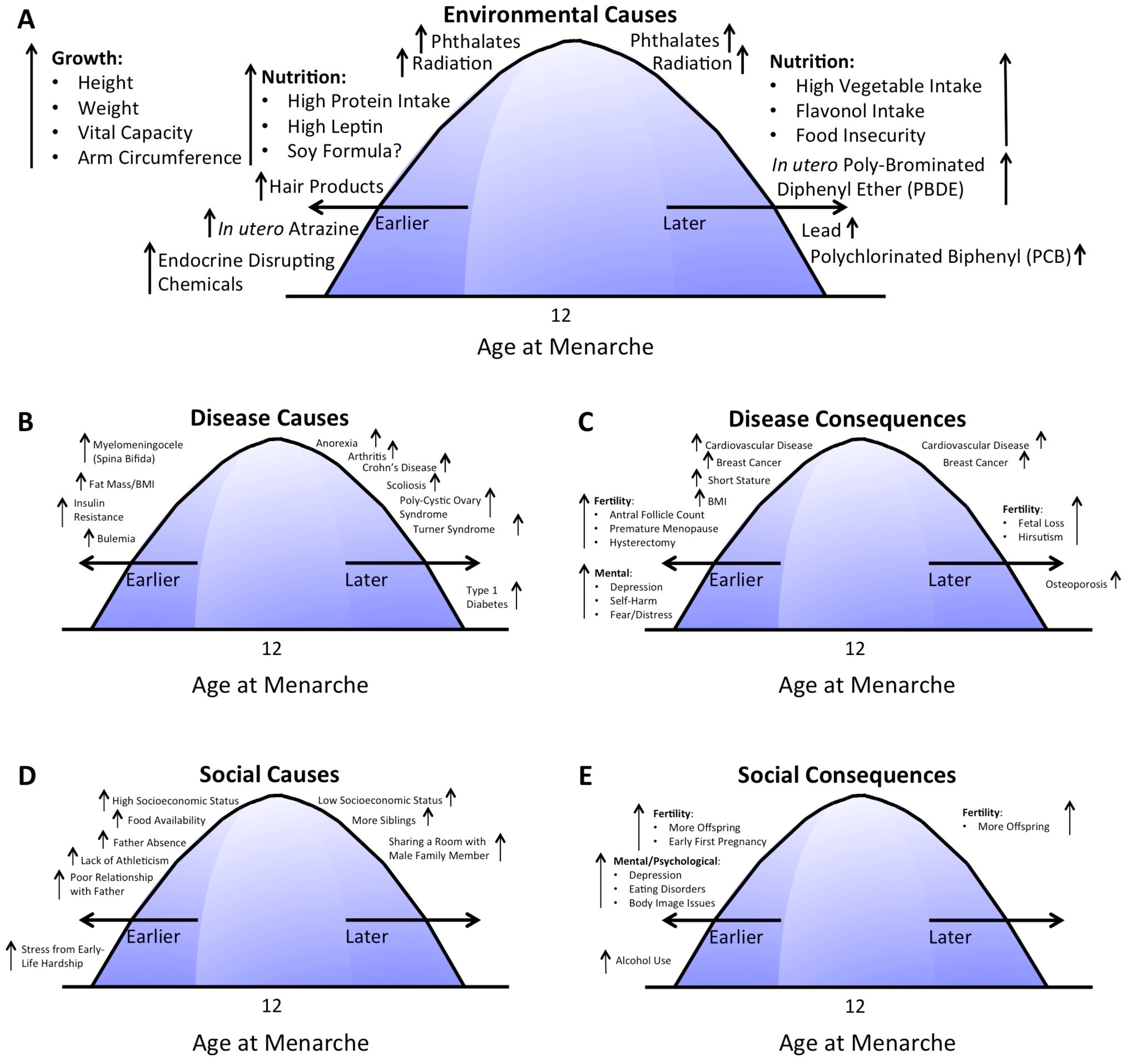
3.2.1. Environmental Causes
Growth/Nutrition
Toxins and Pollutants
3.2.2. Disease Causes and Consequences
Diseases that Affect Timing of Menarche (Causes)
Diseases that Result from Perturbations in Timing of Menarche (Consequences)
3.2.3. Social Causes and Consequences
Social Factors that Affect Timing of Menarche (Causes)
Social Factors that Result from Perturbations in Timing of Menarche (Consequences)
3.2.4. Genetics and Other Factors
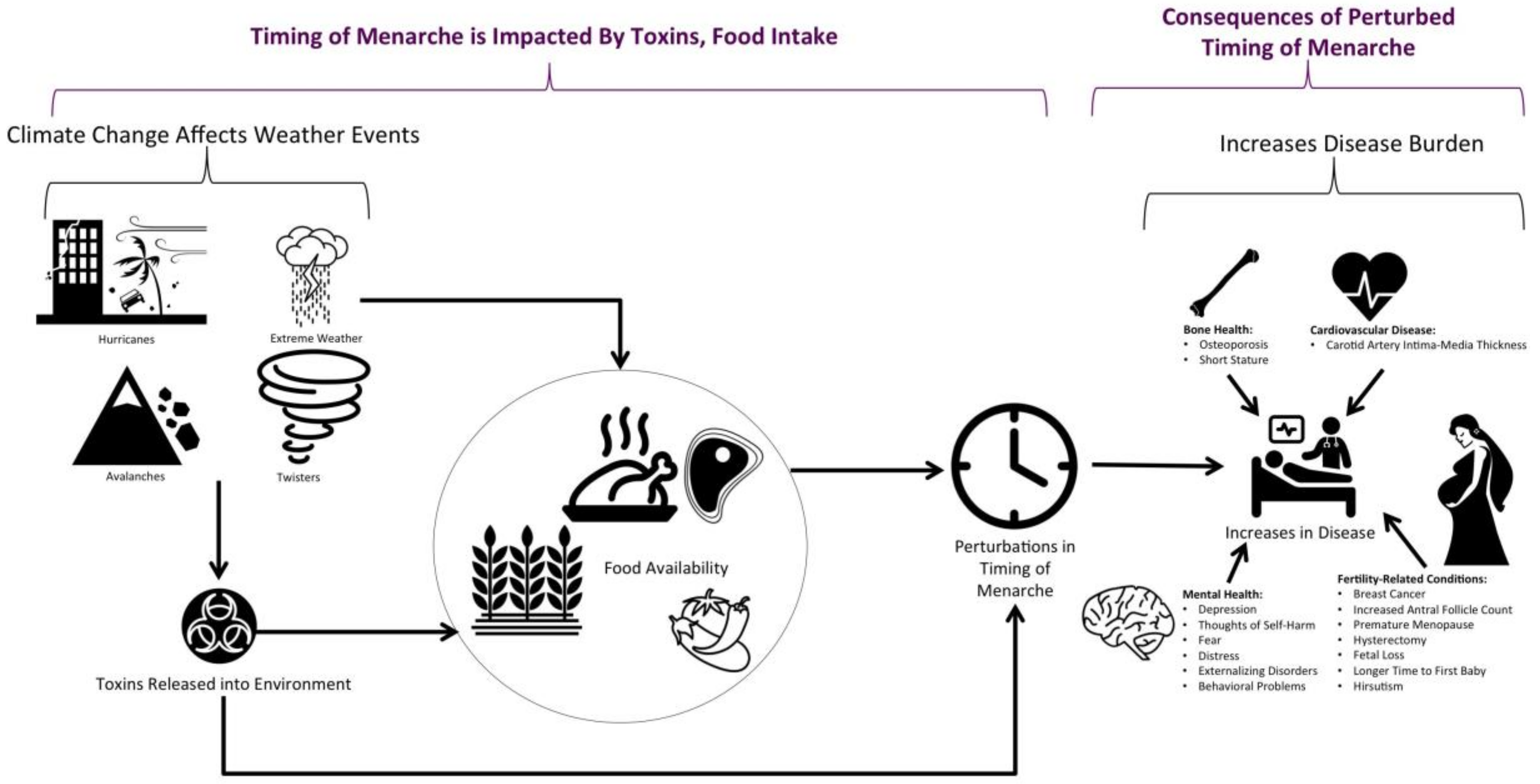
3.3. Potential for Climate Change to Impact Timing of Menarche
4. Discussion
4.1. Impact of Crops and Crop Production on Timing of Menarche
4.2. Overview of Climate Change
4.3. Impact of Climate Change on Pollutant Release and Timing of Menarche
4.4. Potential for Climate Change to Alter Weather Events and Food/Crop Availability
4.5. Limitations of Studies in This Review
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sommer, M.; Sutherland, C.; Chandra-Mouli, V. Putting menarche and girls into the global population health agenda. Reprod. Health 2015, 12, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natsuaki, M.N.; Leve, L.D.; Mendle, J. Going through the rites of passage: Timing and transition of menarche, childhood sexual abuse, and anxiety symptoms in girls. J. Youth Adolesc. 2011, 40, 1357–1370. [Google Scholar] [CrossRef] [Green Version]
- Šaffa, G.; Kubicka, A.M.; Hromada, M.; Kramer, K.L. Is the timing of menarche correlated with mortality and fertility rates? PLoS ONE 2019, 14, e0215462. [Google Scholar] [CrossRef]
- Nagai, N.; Matsumoto, K.; Mino, T.; Takeuchi, H.; Takeda, S. The secular trends in the menarcheal age and the maximum growth age in height for Japanese schoolgirls. Wakayama Med. Rep. 1980, 23, 41–45. [Google Scholar]
- Finlay, F.O.; Jones, R.; Coleman, J. Is puberty getting earlier? The views of doctors and teachers. Child Care Health Dev. 2002, 28, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J. Secular trends in growth. Proc. Nutr. Soc. 2000, 59, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, J.H.; Lim, S.W.; Song, B.S.; Seo, J.; Lee, J.A.; Kim, D.H.; Lim, J.S. Age at menarche in the Korean female: Secular trends and relationship to adulthood body mass index. Ann. Pediatr. Endocrinol. Metab. 2013, 18, 60–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.H.; Kim, S.H.; Oh, M.; Lee, K.W.; Park, M.J. Age at menarche in Korean adolescents: Trends and influencing factors. Reprod. Health 2016, 13, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabanes, A.; Ascunce, N.; Vidal, E.; Ederra, M.; Barcos, A.; Erdozain, N.; Lope, V.; Pollan, M. Decline in age at menarche among Spanish women born from 1925 to 1962. BMC Public Health 2009, 9, 449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, N.; Kiang, M.V.; Kosheleva, A.; Waterman, P.D.; Chen, J.T.; Beckfield, J. Age at menarche: 50-year socioeconomic trends among US-born black and white women. Am. J. Public Health 2015, 105, 388–397. [Google Scholar] [CrossRef]
- Song, Y.; Ma, J.; Wang, H.J.; Wang, Z.; Hu, P.; Zhang, B.; Agardh, A. Trends of age at menarche and association with body mass index in chinese school-aged girls, 1985–2010. J. Pediatr. 2014, 165, 1172–1177. [Google Scholar] [CrossRef] [Green Version]
- Morris, D.H.; Jones, M.E.; Schoemaker, M.J.; Ashworth, A.; Swerdlow, A.J. Secular trends in age at menarche in women in the UK born 1908-93: Results from the Breakthrough Generations Study. Paediatr. Perinat. Epidemiol. 2011, 25, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Rigon, F.; Bianchin, L.; Bernasconi, S.; Bona, G.; Bozzola, M.; Buzi, F.; Cicognani, A.; De Sanctis, C.; De Sanctis, V.; Radetti, G.; et al. Update on Age at Menarche in Italy: Toward the Leveling Off of the Secular Trend. J. Adolesc. Health 2010, 46d, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Thomas, F.; Renaud, F.; Benefice, E.; De Meeüs, T.; Guegan, J.-F. International variability of ages at menarche and menopause: Patterns and main determinants. Hum. Biol. 2001, 73, 271–290. [Google Scholar] [CrossRef] [PubMed]
- Demerath, E.W.; Towne, B.; Chumlea, W.C.; Sun, S.S.; Czerwinski, S.A.; Remsberg, K.E.; Siervogel, R.M. Recent decline in age at menarche: The Fels Longitudinal Study. Am. J. Hum. Biol. 2004, 16, 453–457. [Google Scholar] [CrossRef]
- Hermanussen, M.; Lehmann, A.; Scheffler, C. Psychosocial pressure and menarche: A review of historic evidence for social amenorrhea. Obstetr. Gynecol. Sur. 2012, 67, 237–241. [Google Scholar] [CrossRef]
- Salsberry, P.J.; Reagan, P.B.; Pajer, K. Growth differences by age of menarche in African American and White girls. Nurs. Res. 2009, 58, 382. [Google Scholar] [CrossRef]
- Sohn, K. The influence of climate on age at menarche: Augmented with the influence of ancestry. HOMO-J. Comp. Hum. Biol. 2016, 67, 328–336. [Google Scholar] [CrossRef]
- Saar, E.; Shalev, C.; Dalal, I.; Sod-Moriah, U.A. Age at menarche: The influence of environmental conditions. Int. J. Biometeorol. 1988, 32, 33–35. [Google Scholar] [CrossRef]
- Jansen, E.C.; Herrán, O.F.; Fleischer, N.L.; Mondul, A.M.; Villamor, E. Age at menarche in relation to prenatal rainy season exposure and altitude of residence: Results from a nationally representative survey in a tropical country. J. Dev. Orig. Health Dis. 2017, 8, 188–195. [Google Scholar] [CrossRef]
- Boland, M.R. A model investigating environmental factors that play a role in female fecundity or birth rate. PLoS ONE 2018, 13, e0207932. [Google Scholar] [CrossRef] [PubMed]
- Crowley, T.J. Causes of climate change over the past 1000 years. Science 2000, 289, 270–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panofsky, H.A. Theories of Climate Change. Weatherwise 1956, 9, 183–204. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Adlassnig, K.-P.; Blobel, B.; Mantas, J. Medical Informatics in a United and Healthy Europe: Proceedings of MIE 2009; IOS Press: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Paterson, W.; McNeill, E.; Young, D.; Donaldson, M. Auxological outcome and time to menarche following long-acting goserelin therapy in girls with central precocious or early puberty. Clin. Endocrinol. 2004, 61, 626–634. [Google Scholar] [CrossRef]
- Magarey, A.; Boulton, T.; Chatterton, B.; Schultz, C.; Nordin, B.; Cockington, R. Bone growth from 11 to 17 years: Relationship to growth, gender and changes with pubertal status including timing of menarche. Acta Paediatr. 1999, 88, 139–146. [Google Scholar] [CrossRef]
- Frey, S.; Balu, S.; Greusing, S.; Rothen, N.; Cajochen, C. Consequences of the timing of menarche on female adolescent sleep phase preference. PLoS ONE 2009, 4, e5217. [Google Scholar] [CrossRef] [Green Version]
- Bandini, L.G.; Must, A.; Naumova, E.N.; Anderson, S.E.; Caprio, S.; Spadano-Gasbarro, J.L.; Dietz, W.H. Change in leptin, body composition and other hormones around menarche–a visual representation. Acta Paediatr. 2008, 97, 1454–1459. [Google Scholar] [CrossRef]
- Kanazawa, S. An association between women’s physical attractiveness and the length of their reproductive career in a prospectively longitudinal nationally representative sample. Am. J. Hum. Biol. 2019, 31, e23256. [Google Scholar] [CrossRef]
- Wang, Z.; Dang, S.; Xing, Y.; Li, Q.; Yan, H. Correlation of body mass index levels with menarche in adolescent girls in Shaanxi, China: A cross sectional study. BMC Women’s Health 2016, 16, 61. [Google Scholar] [CrossRef]
- Ohsawa, S.; Ji, C.Y.; Kasai, N. Age at menarche and comparison of the growth and performance of pre-and post-menarcheal girls in China. Am. J. Hum. Biol. 1997, 9, 205–212. [Google Scholar] [CrossRef]
- Delgado, H.L.; Hurtado, E.; Valverde, V. Physical growth, age at menarche and age at first union in rural Guatemala. Ecol. Food Nutr. 1985, 16, 127–133. [Google Scholar] [CrossRef]
- Kirchengast, S.; Göstl, A. Body composition characteristics during puberty in girls and boys from Eastern Austria. Int. J. Anthropol. 2006, 21, 45–54. [Google Scholar] [CrossRef]
- Krzyżanowska, M.; Mascie-Taylor, C.N.; Thalabard, J.-C. Biosocial correlates of age at menarche in a British cohort. Ann. Hum. Biol. 2016, 43, 235–240. [Google Scholar] [CrossRef]
- Gunther, A.L.; Karaolis-Danckert, N.; Kroke, A.; Remer, T.; Buyken, A.E. Dietary protein intake throughout childhood is associated with the timing of puberty. J. Nutr. 2009, 140, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.; Badenhop, N.; Skugor, M.; Klisovic, D.; Landoll, J.; Matkovic, V. The Onset of Menarche Is Inversely Related to Serum Leptin Level. Proc. Faseb J. 1997, 11, 1016. [Google Scholar]
- Matkovic, V.; Ilich, J.Z.; Skugor, M.; Badenhop, N.E.; Goel, P.; Clairmont, A.; Klisovic, D.; Nahhas, R.W.; Landoll, J.D. Leptin is inversely related to age at menarche in human females. J. Clin. Endocrinol. Metab. 1997, 82, 3239–3245. [Google Scholar] [CrossRef]
- Adgent, M.A.; Daniels, J.L.; Rogan, W.J.; Adair, L.; Edwards, L.J.; Westreich, D.; Maisonet, M.; Marcus, M. Early-life soy exposure and age at menarche. Paediatr. Perinat. Epidemiol. 2012, 26, 163–175. [Google Scholar] [CrossRef] [Green Version]
- Segovia-Siapco, G.; Pribis, P.; Messina, M.; Oda, K.; Sabaté, J. Is soy intake related to age at onset of menarche? A cross-sectional study among adolescents with a wide range of soy food consumption. Nutr. J. 2014, 13, 54. [Google Scholar] [CrossRef] [Green Version]
- Mervish, N.A.; Teitelbaum, S.L.; Pajak, A.; Windham, G.C.; Pinney, S.M.; Kushi, L.H.; Biro, F.M.; Wolff, M.S. Peripubertal dietary flavonol and lignan intake and age at menarche in a longitudinal cohort of girls. Pediatr. Res. 2017, 82, 201. [Google Scholar] [CrossRef] [Green Version]
- Belachew, T.; Hadley, C.; Lindstrom, D.; Getachew, Y.; Duchateau, L.; Kolsteren, P. Food insecurity and age at menarche among adolescent girls in Jimma Zone Southwest Ethiopia: A longitudinal study. Reprod. Biol. Endocrinol. 2011, 9, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, H.L.; Raubenheimer, D.; Steinbeck, K.; Baur, L.; Garnett, S. New insights into the association of mid-childhood macronutrient intake to pubertal development in adolescence using nutritional geometry. Br. J. Nutr. 2019, 122, 274–283. [Google Scholar] [CrossRef]
- Zhu, K.; Zhang, Q.; Foo, L.H.; Trube, A.; Ma, G.; Hu, X.; Du, X.; Cowell, C.T.; Fraser, D.R.; Greenfield, H. Growth, bone mass, and vitamin D status of Chinese adolescent girls 3 y after withdrawal of milk supplementation. Am. J. Clin. Nutr. 2006, 83, 714–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, A.M.; Willekens, F.J.; Baqui, A.H.; Van Ginneken, J.K.; Hutter, I. Association between age at menarche and early-life nutritional status in rural Bangladesh. J. Biosoc. Sci. 2008, 40, 223–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, I.d.S.; De Stavola, B.L.; Mann, V.; Kuh, D.; Hardy, R.; Wadsworth, M.E. Prenatal factors, childhood growth trajectories and age at menarche. Int. J. Epidemiol. 2002, 31, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Blell, M.; Pollard, T.M.; Pearce, M.S. Predictors of age at menarche in the Newcastle Thousand Families Study. J. Biosoc. Sci. 2008, 40, 563–575. [Google Scholar] [CrossRef] [Green Version]
- Hayes, P.; Tan, T.X. Timing of menarche in girls adopted from China: A cohort study. Child Care Health Dev. 2016, 42, 859–862. [Google Scholar] [CrossRef]
- Davies, M.J. Evidence for effects of weight on reproduction in women. Reprod. Biomed. Online 2006, 12, 552–561. [Google Scholar] [CrossRef]
- Denham, M.; Schell, L.M.; Deane, G.; Gallo, M.V.; Ravenscroft, J.; DeCaprio, A.P. Relationship of lead, mercury, mirex, dichlorodiphenyldichloroethylene, hexachlorobenzene, and polychlorinated biphenyls to timing of menarche among Akwesasne Mohawk girls. Pediatrics 2005, 115, e127–e134. [Google Scholar] [CrossRef] [Green Version]
- Den Hond, E.; Dhooge, W.; Bruckers, L.; Schoeters, G.; Nelen, V.; Van De Mieroop, E.; Koppen, G.; Bilau, M.; Schroijen, C.; Keune, H. Internal exposure to pollutants and sexual maturation in Flemish adolescents. J. Exp. Sci. Environ. Epidemiol. 2011, 21, 224. [Google Scholar] [CrossRef] [Green Version]
- Harley, K.G.; Rauch, S.A.; Chevrier, J.; Kogut, K.; Parra, K.L.; Trujillo, C.; Lustig, R.H.; Greenspan, L.C.; Sjödin, A.; Bradman, A. Association of prenatal and childhood PBDE exposure with timing of puberty in boys and girls. Environ. Int. 2017, 100, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Núñez, Z.; Barrett, E.S.; Szamreta, E.A.; Shapses, S.A.; Qin, B.; Lin, Y.; Zarbl, H.; Buckley, B.; Bandera, E.V. Urinary mycoestrogens and age and height at menarche in New Jersey girls. Environ. Health 2019, 18, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binder, A.M.; Corvalan, C.; Calafat, A.M.; Ye, X.; Mericq, V.; Pereira, A.; Michels, K.B. Childhood and adolescent phenol and phthalate exposure and the age of menarche in Latina girls. Environ. Health 2018, 17, 32. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Friedman, D.L.; Yasui, Y.; Whitton, J.A.; Stovall, M.; Robison, L.L.; Sklar, C.A. Timing of menarche among survivors of childhood acute lymphoblastic leukemia: A report from the Childhood Cancer Survivor Study. Pediatr. Blood Cancer 2008, 50, 854–858. [Google Scholar] [CrossRef]
- Armstrong, G.T.; Whitton, J.A.; Gajjar, A.; Kun, L.E.; Chow, E.J.; Stovall, M.; Leisenring, W.; Robison, L.L.; Sklar, C.A. Abnormal timing of menarche in survivors of central nervous system tumors: A report from the Childhood Cancer Survivor Study. Cancer 2009, 115, 2562–2570. [Google Scholar] [CrossRef] [Green Version]
- Clayton, P.E.; Shalet, S.M.; Price, D.A.; Jones, P.M. Ovarian function following chemotherapy for childhood brain tumours. Med. Pediatr. Oncol. 1989, 17, 92–96. [Google Scholar] [CrossRef]
- McDougall, J.A.; Sakata, R.; Sugiyama, H.; Grant, E.; Davis, S.; Nishi, N.; Soda, M.; Shimizu, Y.; Tatsukawa, Y.; Kasagi, F. Timing of menarche and first birth in relation to risk of breast cancer in A-bomb survivors. Cancer Epidemiol. Prev. Biomark. 2010, 19, 1746–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, J.A.; Tehranifar, P.; Flom, J.D.; Terry, M.B.; James-Todd, T. Hair product use, age at menarche and mammographic breast density in multiethnic urban women. Environ. Health 2018, 17, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namulanda, G.; Taylor, E.; Maisonet, M.; Barr, D.B.; Flanders, W.D.; Olson, D.; Qualters, J.R.; Vena, J.; Northstone, K.; Naeher, L. In utero exposure to atrazine analytes and early menarche in the Avon Longitudinal Study of Parents and Children Cohort. Environ. Res. 2017, 156, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Namulanda, G.; Maisonet, M.; Taylor, E.; Flanders, W.D.; Olson, D.; Sjodin, A.; Qualters, J.R.; Vena, J.; Northstone, K.; Naeher, L. In utero exposure to organochlorine pesticides and early menarche in the Avon Longitudinal Study of Parents and Children. Environ. Int. 2016, 94, 467–472. [Google Scholar] [CrossRef] [Green Version]
- Furman, L.; Mortimer, J.C. Menarche and menstrual function in patients with myelomeningocele. Dev. Med. Child Neurol. 1994, 36, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Gavela-Pérez, T.; Garcés, C.; Navarro-Sánchez, P.; López Villanueva, L.; Soriano-Guillén, L. Earlier menarcheal age in S panish girls is related with an increase in body mass index between pre-pubertal school age and adolescence. Pediatr. Obes. 2015, 10, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Pereira, K.; Pugliese, B.; Guimarães, M.; Gama, M. Pubertal development in children diagnosed with diabetes mellitus type 1 before puberty. J. Pediatr. Adolesc. Gynecol. 2015, 28, 66–71. [Google Scholar] [CrossRef]
- Bratke, H.; Bruserud, I.S.; Brannsether, B.; Aßmus, J.; Bjerknes, R.; Roelants, M.; Júlíusson, P.B. Timing of menarche in Norwegian girls: Associations with body mass index, waist circumference and skinfold thickness. BMC Pediatr. 2017, 17, 138. [Google Scholar] [CrossRef]
- Liu, M.; He, Y.; Jiang, B.; Wu, L.; Wang, J.; Yang, S.; Wang, Y.; Li, X. Association between reproductive variables and metabolic syndrome in chinese community elderly women. Arch. Gerontol. Geriatr. 2016, 63, 78–84. [Google Scholar] [CrossRef]
- Slyper, A.H. The pubertal timing controversy in the USA, and a review of possible causative factors for the advance in timing of onset of puberty. Clin. Endocrinol. 2006, 65, 1–8. [Google Scholar] [CrossRef]
- Ruuska, J.; Kaltiala-Heino, R.; Koivisto, A.-M.; Rantanen, P. Puberty, sexual development and eating disorders in adolescent outpatients. Eur. Child Adolesc. Psychiatr. 2003, 12, 214–220. [Google Scholar] [CrossRef]
- Sørensen, K.; Juul, A.; Christensen, K.; Skytthe, A.; Scheike, T.; Kold Jensen, T. Birth size and age at menarche: A twin perspective. Hum. Reprod. 2013, 28, 2865–2871. [Google Scholar] [CrossRef] [Green Version]
- James, E.; Wood, C.L.; Nair, H.; Williams, T.C. Preterm birth and the timing of puberty: A systematic review. BMC Pediatr. 2018, 18, 3. [Google Scholar] [CrossRef] [Green Version]
- Shim, Y.S.; Park, H.K.; Yang, S.; Hwang, I.T. Age at menarche and adult height in girls born small for gestational age. Ann. Pediatr. Endocrinol. Metab. 2013, 18, 76. [Google Scholar] [CrossRef] [Green Version]
- Völkl, T.M.; Öhl, L.; Rauh, M.; Schöfl, C.; Dörr, H.G. Adrenarche and puberty in children with classic congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Horm. Res. Padiatr. 2011, 76, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Sloboda, D.M.; Hart, R.; Doherty, D.A.; Pennell, C.E.; Hickey, M. Age at menarche: Influences of prenatal and postnatal growth. J. Clin. Endocrinol. Metab. 2007, 92, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; de Zegher, F.; Garnett, S.P.; Baur, L.A.; Cowell, C.T. Opposing influences of prenatal and postnatal growth on the timing of menarche. J. Clin. Endocrinol. Metab. 2006, 91, 4369–4373. [Google Scholar] [CrossRef]
- Winterer, J.; Cutler, G.B.J.; Loriaux, D.L. Caloric balance, brain to body ratio, and the timing of menarche. Med. Hypotheses 1984, 15, 87–91. [Google Scholar] [CrossRef]
- Rozé, C.; Doyen, C.; Le Heuzey, M.F.; Armoogum, P.; Mouren, M.C.; Léger, J. Predictors of late menarche and adult height in children with anorexia nervosa. Clin. Endocrinol. 2007, 67, 462–467. [Google Scholar] [CrossRef]
- Mao, S.-H.; Jiang, J.; Sun, X.; Zhao, Q.; Qian, B.-P.; Liu, Z.; Shu, H.; Qiu, Y. Timing of menarche in Chinese girls with and without adolescent idiopathic scoliosis: Current results and review of the literature. Eur. Spine J. 2011, 20, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Folsom, L.J.; Slaven, J.E.; Nabhan, Z.M.; Eugster, E.A. Characterization of spontaneous and induced puberty in girls with Turner Syndrome. Endocr. Pract. 2017, 23, 768–774. [Google Scholar] [CrossRef] [Green Version]
- Sadrzadeh, S.; Klip, W.; Broekmans, F.; Schats, R.; Willemsen, W.; Burger, C.; Van Leeuwen, F.; Lambalk, C. Birth weight and age at menarche in patients with polycystic ovary syndrome or diminished ovarian reserve, in a retrospective cohort. Hum. Reprod. 2003, 18, 2225–2230. [Google Scholar] [CrossRef] [Green Version]
- Fraser, P.A.; Hoch, S.; Erlandson, D.; Partridge, R.; Jackson, J.M. The timing of menarche in juvenile rheumatoid arthritis. J. Adolesc. Health Care 1988, 9, 483–487. [Google Scholar] [CrossRef]
- Rusconi, R.; Corona, F.; Grassi, A.; Carnelli, V. Age at menarche in juvenile rheumatoid arthritis. J. Pediatr. Endocrinol. Metab. JPEM 2003, 16, 285–288. [Google Scholar]
- Gupta, N.; Lustig, R.H.; Kohn, M.A.; Vittinghoff, E. Menarche in pediatric patients with Crohn’s disease. Dig. Dis. Sci. 2012, 57, 2975–2981. [Google Scholar] [CrossRef] [PubMed]
- Chevalley, T.; Rizzoli, R.; Hans, D.; Ferrari, S.; Bonjour, J.-P. Interaction between calcium intake and menarcheal age on bone mass gain: An eight-year follow-up study from prepuberty to postmenarche. J. Clin. Endocrinol. Metab. 2005, 90, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varea, C.; Bernis, C.; Elizondo, S. Physiological maturation, reproductive patterns, and female fecundability in a traditional Moroccan population (Amizmiz, Marrakech). Am. J. Hum. Biol. 1993, 5, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Jahanfar, S.; Lye, M.-S.; Krishnarajah, I.S. Genetic and environmental effects on age at menarche, and its relationship with reproductive health in twins. Indian J. Hum. Genet. 2013, 19, 245. [Google Scholar]
- Ibánez, L.; Ferrer, A.; Marcos, M.V.; Hierro, F.R.; de Zegher, F. Early puberty: Rapid progression and reduced final height in girls with low birth weight. Pediatrics 2000, 106, e72. [Google Scholar] [CrossRef] [Green Version]
- Schuh, S.M.; Kadie, J.; Rosen, M.P.; Sternfeld, B.; Pera, R.A.R.; Cedars, M.I. Links between age at menarche, antral follicle count, and body mass index in African American and European American women. Fertil. Steril. 2019, 111, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Mishra, G.D.; Pandeya, N.; Dobson, A.J.; Chung, H.-F.; Anderson, D.; Kuh, D.; Sandin, S.; Giles, G.G.; Bruinsma, F.; Hayashi, K. Early menarche, nulliparity and the risk for premature and early natural menopause. Hum. Reprod. 2017, 32, 679–686. [Google Scholar] [CrossRef]
- Cooper, R.; Hardy, R.; Kuh, D. Timing of menarche, childbearing and hysterectomy risk. Maturitas 2008, 61, 317–322. [Google Scholar] [CrossRef]
- Sequeira, M.-E.; Lewis, S.J.; Bonilla, C.; Smith, G.D.; Joinson, C. Association of timing of menarche with depressive symptoms and depression in adolescence: Mendelian randomisation study. Br. J. Psychiatr. 2017, 210, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Roberts, E.; Fraser, A.; Gunnell, D.; Joinson, C.; Mars, B. Timing of menarche and self-harm in adolescence and adulthood: A population-based cohort study. Psychol. Med. 2019, 28, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Platt, J.M.; Colich, N.L.; McLaughlin, K.A.; Gary, D.; Keyes, K.M. Transdiagnostic psychiatric disorder risk associated with early age of menarche: A latent modeling approach. Compr. Psychiatr. 2017, 79, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, J.L.; Van Hulle, C.; D’Onofrio, B.; Rathouz, P.; Beasley, W.; Johnson, A.; Waldman, I.; Lahey, B.B. Behavior problems and timing of menarche: A developmental longitudinal biometrical analysis using the NLSY-Children data. Behav. Genet. 2015, 45, 51–70. [Google Scholar] [CrossRef] [PubMed]
- Ley, S.H.; Li, Y.; Tobias, D.K.; Manson, J.E.; Rosner, B.; Hu, F.B.; Rexrode, K.M. Duration of reproductive life span, age at menarche, and age at menopause are associated with risk of cardiovascular disease in women. J. Am. Heart Assoc. 2017, 6, e006713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhuiyan, A.R.; Srinivasan, S.R.; Chen, W.; Fernandez, C.; Xu, J.-H.; Berenson, G.S. Timing of menarche related to carotid artery intima-media thickness in black and white young adult women: The Bogalusa Heart Study. Ann. Epidemiol. 2015, 25, 414–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.J.; Cook-Wiens, G.; Johnson, B.D.; Braunstein, G.D.; Berga, S.L.; Stanczyk, F.Z.; Pepine, C.J.; Bairey Merz, C.N.; Shufelt, C.L. Age at Menarche and Risk of Cardiovascular Disease Outcomes: Findings from the National Heart Lung and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation. J. Am. Heart Assoc. 2019, 8, e012406. [Google Scholar] [CrossRef] [PubMed]
- Li, C.I.; Malone, K.E.; Daling, J.R.; Potter, J.D.; Bernstein, L.; Marchbanks, P.A.; Strom, B.L.; Simon, M.S.; Press, M.F.; Ursin, G. Timing of menarche and first full-term birth in relation to breast cancer risk. Am. J. Epidemiol. 2007, 167, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Colditz, G.A.; Frazier, A.L. Models of breast cancer show that risk is set by events of early life: Prevention efforts must shift focus. Cancer Epidemiol. Prev. Biomark. 1995, 4, 567–571. [Google Scholar]
- Braithwaite, D.; Moore, D.H.; Lustig, R.H.; Epel, E.S.; Ong, K.K.; Rehkopf, D.H.; Wang, M.C.; Miller, S.M.; Hiatt, R.A. Socioeconomic status in relation to early menarche among black and white girls. Cancer Causes Control 2009, 20, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Minami, Y.; Nishino, Y.; Kawai, M.; Tada, H.; Kanemura, S.; Miyashita, M.; Ishida, T.; Kakugawa, Y. Reproductive history and breast cancer survival: A prospective patient cohort study in Japan. Breast Cancer 2019, 26, 687–702. [Google Scholar] [CrossRef]
- Bielicki, T.; Welon, Z. Growth data as indicators of social inequalities: The case of Poland. Am. J. Phys. Anthropol. 1982, 25, 153–167. [Google Scholar] [CrossRef]
- Bogaert, A.F. Menarche and father absence in a national probability sample. J. Biosoc. Sci. 2008, 40, 623–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maestripieri, D.; Roney, J.R.; DeBias, N.; Durante, K.M.; Spaepen, G.M. Father absence, menarche and interest in infants among adolescent girls. Dev. Sci. 2004, 7, 560–566. [Google Scholar] [CrossRef]
- Culpin, I.; Heron, J.; Araya, R.; Melotti, R.; Lewis, G.; Joinson, C. Father absence and timing of menarche in adolescent girls from a UK cohort: The mediating role of maternal depression and major financial problems. J. Adolesc. 2014, 37, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Culpin, I.; Heron, J.; Araya, R.; Joinson, C. Early childhood father absence and depressive symptoms in adolescent girls from a UK cohort: The mediating role of early menarche. J. Abnorm. Child Psychol. 2015, 43, 921–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Yu, T.; Chen, Q.; Wellings, K.; Oniffrey, T.M.; Ma, J.; Huang, L.; Fan, S.; Ma, L.; Li, R. Early menarche and its relationship to paternal migrant work among middle-school-aged students in China. J. Biosoc. Sci. 2020, 52, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Sung, S.; Simpson, J.A.; Griskevicius, V.; Kuo, S.I.-C.; Schlomer, G.L.; Belsky, J. Secure infant-mother attachment buffers the effect of early-life stress on age of menarche. Psychol. Sci. 2016, 27, 667–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clancy, K.B.; Klein, L.D.; Ziomkiewicz, A.; Nenko, I.; Jasienska, G.; Bribiescas, R.G. Relationships between biomarkers of inflammation, ovarian steroids, and age at menarche in a rural Polish sample. Am. J. Hum. Biol. 2013, 25, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Koziel, S.; Chakraborty, R.; Bose, K. Sibling composition and household room sharing are associated with menarcheal status among rural Bengalee girls of West Bengal, India. Hum. Biol. 2013, 85, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Malina, R. Menarche in atheletes: A synthesis and hypothesis. Ann. Hum. Biol. 1983, 10, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M. Physical activity and training: Effects on stature and the adolescent growth spurt. Med. Sci. Sports Exerc. 1994, 26, 759–766. [Google Scholar] [CrossRef]
- Lee, E.-Y.; Pabayo, R.; Kawachi, I. Timing of spermarche and menarche are associated with physical activity and sedentary behavior among Korean adolescents. Osong Public Health Res. Perspect. 2016, 7, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udry, J.R. Age at menarche, at first intercourse, and at first pregnancy. J. Biosoc. Sci. 1979, 11, 433–441. [Google Scholar] [CrossRef]
- Jokela, M.; Kivimäki, M.; Elovainio, M.; Viikari, J.; Raitakari, O.T.; Keltikangas-Järvinen, L. Body mass index in adolescence and number of children in adulthood. Epidemiology 2007, 18, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Joinson, C.; Heron, J.; Araya, R.; Lewis, G. Early menarche and depressive symptoms from adolescence to young adulthood in a UK cohort. J. Am. Acad. Child Adolesc. Psychiatr. 2013, 52, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Joinson, C.; Heron, J.; Lewis, G.; Croudace, T.; Araya, R. Timing of menarche and depressive symptoms in adolescent girls from a UK cohort. Br. J. Psychiatr. 2011, 198, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Striegel-Moore, R.H.; McMahon, R.P.; Biro, F.M.; Schreiber, G.; Crawford, P.B.; Voorhees, C. Exploring the relationship between timing of menarche and eating disorder symptoms in black and white adolescent girls. Int. J. Eat. Dis. 2001, 30, 421–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruble, D.N.; Brooks-Gunn, J. The experience of menarche. Child Dev. 1982, 53, 1557–1566. [Google Scholar] [CrossRef]
- Hayward, C.; Gotlib, I.H.; Schraedley, P.K.; Litt, I.F. Ethnic differences in the association between pubertal status and symptoms of depression in adolescent girls. J. Adolesc. Health 1999, 25, 143–149. [Google Scholar] [CrossRef]
- Joinson, C.; Heron, J.; Araya, R.; Paus, T.; Croudace, T.; Rubin, C.; Marcus, M.; Lewis, G. Association between pubertal development and depressive symptoms in girls from a UK cohort. Psychol. Med. 2012, 42, 2579–2589. [Google Scholar] [CrossRef]
- Rierdan, J.; Koff, E. Timing of menarche and initial menstrual experience. J. Youth Adolesc. 1985, 14, 237–244. [Google Scholar] [CrossRef]
- Deardorff, J.; Gonzales, N.A.; Christopher, F.S.; Roosa, M.W.; Millsap, R.E. Early puberty and adolescent pregnancy: The influence of alcohol use. Pediatrics 2005, 116, 1451–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asadullah, M.N.; Wahhaj, Z. Early marriage, social networks and the transmission of norms. Economica 2016, 86, 801–831. [Google Scholar] [CrossRef] [Green Version]
- Towne, B.; Czerwinski, S.A.; Demerath, E.W.; Blangero, J.; Roche, A.F.; Siervogel, R.M. Heritability of age at menarche in girls from the Fels Longitudinal Study. Am. J. Phys. Anthropol. 2005, 128, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Hartge, P. Genetics of reproductive lifespan. Nat. Genet. 2009, 41, 637–638. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.M.; Eaves, L.J.; Heath, A.C.; Martin, N.G. Estimating genetic influences on the age-at-menarche: A survival analysis approach. Am. J. Med. Genet. 1991, 39, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Chumlea, C.; Stepick, C.D.; Lopez, F.G. Age of menarche in Oaxaca, Mexico, schoolgirls, with comparative data for other areas of Mexico. Ann. Hum. Biol. 1977, 4, 551–558. [Google Scholar] [CrossRef]
- Xita, N.; Tsatsoulis, A.; Stavrou, I.; Georgiou, I. Association of SHBG gene polymorphism with menarche. Mol. Hum. Reprod. 2005, 11, 459–462. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-Z.; Shin, A.; Lee, Y.-S.; Kim, S.-Y.; Kim, Y.; Lee, E.-S. Polymorphisms in adiposity-related genes are associated with age at menarche and menopause in breast cancer patients and healthy women. Hum. Reprod. 2012, 27, 2193–2200. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Zhang, B.; Choi, J.-Y.; Gao, Y.-T.; Li, H.; Lu, W.; Long, J.; Kang, D.; Xiang, Y.-B.; Wen, W. Age at menarche and age at natural menopause in East Asian women: A genome-wide association study. Age 2016, 38, 513–523. [Google Scholar] [CrossRef] [Green Version]
- Tempfer, C.B.; Riener, E.-K.; Keck, C.; Grimm, C.; Heinze, G.; Huber, J.C.; Gitsch, G.; Hefler, L.A. Polymorphisms associated with thrombophilia and vascular homeostasis and the timing of menarche and menopause in 728 white women. Menopause 2005, 12, 325–330. [Google Scholar] [CrossRef]
- Grimm, C.; Tempfer, C.B.; Walch, K.; Reinthaller, A.; Tomovski, C.; Huber, J.C.; Leodolter, S.; Hefler, L.A. The influence of a Vitamin D receptor gene polymorphism on the timing of female reproductive functions in humans. Maturitas 2005, 51, 135–139. [Google Scholar] [CrossRef]
- Cerne, J.-Z.; Pohar-Perme, M.; Cerkovnik, P.; Gersak, K.; Novakovic, S. Age at menarche and menopause is not associated with two common genetic variants in the methylenetetrahydrofolate reductase (MTHFR) gene. Eur. J. Contracept. Reprod. Health Care 2011, 16, 241–247. [Google Scholar] [CrossRef]
- Nanao, K.; Hasegawa, Y. Polymorphisms at the 5’end of the human gonadotropin-releasing hormone receptor gene are not associated with the timing of menarche in Japanese girls. Eur. J. Endocrinol. 2000, 143, 555–556. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Lu, Y.; Recker, R.R.; Deng, H.-W.; Dvornyk, V. Association analyses suggest multiple interaction effects of the methylenetetrahydrofolate reductase polymorphisms on timing of menarche and natural menopause in white women. Menopause 2010, 17, 185. [Google Scholar] [CrossRef] [Green Version]
- Day, F.R.; Thompson, D.J.; Helgason, H.; Chasman, D.I.; Finucane, H.; Sulem, P.; Ruth, K.S.; Whalen, S.; Sarkar, A.K.; Albrecht, E. Genomic analyses identify hundreds of variants associated with age at menarche and support a role for puberty timing in cancer risk. Nat. Genet. 2017, 49, 834. [Google Scholar] [CrossRef]
- Group, E.C.W. Nutrition and reproduction in women. Hum. Reprod. Update 2006, 12, 193–207. [Google Scholar] [CrossRef]
- Frisch, R.E. Body fat, puberty and fertility. Biol. Rev. 1984, 59, 161–188. [Google Scholar] [CrossRef] [PubMed]
- Lassek, W.D.; Gaulin, S.J. Brief communication: Menarche is related to fat distribution. Am. J. Phys. Anthropol. 2007, 133, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Merzenich, H.; Boeing, H.; Wahrendorf, J. Dietary fat and sports activity as determinants for age at menarche. Am. J. Epidemiol. 1993, 138, 217–224. [Google Scholar] [CrossRef]
- Hernandez, M.I.; Unanue, N.; Gaete, X.; Cassorla, F.; Codner, E. Age of menarche and its relationship with body mass index and socioeconomic status. Rev. Méd. Chile 2007, 135, 1429–1436. [Google Scholar]
- Freedman, D.S.; Khan, L.K.; Serdula, M.K.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. Relation of age at menarche to race, time period, and anthropometric dimensions the Bogalusa Heart Study. Pediatrics 2002, 110, e43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkey, C.S.; Gardner, J.D.; Lindsay Frazier, A.; Colditz, G.A. Relation of Childhood Diet and Body Size to Menarche and Adolescent Growth in Girls. Am. J. Epidemiol. 2000, 152, 446–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavarro, J.; Villamor, E.; Narvaez, J.; Hoyos, A. Socio-demographic predictors of age at menarche in a group of Colombian university women. Ann. Hum. Biol. 2004, 31, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.P. Reproductive Function in the Ballet Dancer. In The Menstrual Cycle and Its Disorders; Springer: Berlin/Heidelberg, Germany, 1989; pp. 161–170. [Google Scholar] [CrossRef]
- Frisch, R.E.; Wyshak, G.; Vincent, L. Delayed menarche and amenorrhea in ballet dancers. N. Engl. J. Med. 1980, 303, 17–19. [Google Scholar] [CrossRef] [Green Version]
- Cumming, D.C.; Wheeler, G.D.; Harber, V.J. Physical activity, nutrition, and reproduction. Ann. N.Y. Acad. Sci. 1994, 709, 55–76. [Google Scholar] [CrossRef]
- Warren, M.P. The Effects of Exercise on Pubertal Progression and Reproductive Function in Girls*. J. Clin. Endocrinol. Metab. 1980, 51, 1150–1157. [Google Scholar] [CrossRef]
- Baxter-Jones, A.D.G.; Helms, P.; Baines-Preece, J.; Preece, M. Menarche in intensively trained gymnasts, swimmers and tennis players. Ann. Hum. Biol. 1994, 21, 407–415. [Google Scholar] [CrossRef]
- Gopalan, C.; Naidu, A.N. Nutrition and fertility. Lancet 1972, 1077–1079. [Google Scholar] [CrossRef]
- Groos, A.D.; Smith, T.A. Age at menarche and associated nutritional status variables in Karimui and Daribi census divisions of Simbu Province. Papua N. Guin. Med. J. 1992, 35, 84–94. [Google Scholar]
- Elias, S.G.; van Noord, P.A.; Peeters, P.H.; den Tonkelaar, I.; Kaaks, R.; Grobbee, D.E. Menstruation during and after caloric restriction: The 1944–1945 Dutch famine. Fertil. Steril. 2007, 88, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Bleiberg, F.M.; Brun, T.A.; Goihman, S.; Gouba, E. Duration of activities and energy expenditure of female farmers in dry and rainy seasons in Upper-Volta. Br. J. Nutr. 1980, 43, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Bantje, H.F.W. Female stress and birth seasonality in tanzania. J. Biosoc. Sci. 1988, 20, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Pagezy, H. Seasonal hunger, as experienced by the oto and the twa of a ntomba village in the equatorial forest (lake tumba, zaire). Ecol. Food Nutr. 1982, 12, 139–153. [Google Scholar] [CrossRef]
- Leslie, P.W.; Fry, P.H. Extreme seasonality of births among nomadic Turkana pastoralists. Am. J. Phys. Anthropol. 1989, 79, 103–115. [Google Scholar] [CrossRef]
- Ellison, P.T.; Peacock, N.R.; Lager, C. Ecology and ovarian function among Lese women of the Ituri forest, Zaire. Am. J. Phys. Anthropol. 1989, 78, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.C.; Jenike, M.R.; Ellison, P.T.; Bentley, G.R. The ecology of birth seasonality among agriculturalists in central africa. J. Biosoc. Sci. 1992, 24, 393–412. [Google Scholar] [CrossRef]
- Kolata, G.B. !Kung Hunter-Gatherers: Feminism, Diet, and Birth Control. Science 1974, 185, 932–934. [Google Scholar] [CrossRef]
- Pennington, R. Did Food Increase Fertility? Evaluation of !Kung and Herero History. Hum. Biol. 1992, 64, 497–521. [Google Scholar]
- Bentley, G.R. Hunter-gatherer energetics and fertility: A reassessment of the! Kung San. Hum. Ecol. 1985, 13, 79–109. [Google Scholar] [CrossRef]
- Panter-Brick, C.; Lotstein, D.S.; Ellison, P.T. Seasonality of reproductive function and weight loss in rural Nepali women. Hum. Reprod. 1993, 8, 684–690. [Google Scholar] [CrossRef]
- Matchock, R.L.; Susman, E.J.; Brown, F.M. Seasonal rhythms of menarche in the United States: Correlates to menarcheal age, birth age, and birth month. Womens Health Issues 2004, 14, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Gueresi, P. Monthly distribution of menarche in three provinces of north Italy. Ann. Hum. Biol. 1997, 24, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Brundtland, G.H.; Liestøl, K. Seasonal variations in menarche in Oslo. Ann. Hum. Biol. 1982, 9, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Chompootaweep, S.; Tankeyoon, M.; Poomsuwan, P.; Yamarat, K.; Dusitsin, N. Age at menarche in Thai girls. Ann. Hum. Biol. 1997, 24, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Miura, T.; Nakamura, I.; Nonaka, K.; Shimura, M. Correlation between month of menarche and month of birth. Arch. Gynecol. 1987, 240, 195–200. [Google Scholar] [CrossRef]
- Gille, S.T. Warming of the Southern Ocean since the 1950s. Science 2002, 295, 1275–1277. [Google Scholar] [CrossRef] [Green Version]
- Wijffels, S.; Roemmich, D.; Monselesan, D.; Church, J.; Gilson, J. Ocean temperatures chronicle the ongoing warming of Earth. Nat. Clim. Chang. 2016, 6, 116–118. [Google Scholar] [CrossRef]
- Beaubien, E.; Freeland, H. Spring phenology trends in Alberta, Canada: Links to ocean temperature. Int. J. Biometeorol. 2000, 44, 53–59. [Google Scholar] [CrossRef]
- Byrne, M.P.; O’Gorman, P.A. Trends in continental temperature and humidity directly linked to ocean warming. Proc. Natl. Acad. Sci. USA 2018, 115, 4863–4868. [Google Scholar] [CrossRef] [Green Version]
- Bender, M.A.; Knutson, T.R.; Tuleya, R.E.; Sirutis, J.J.; Vecchi, G.A.; Garner, S.T.; Held, I.M. Modeled impact of anthropogenic warming on the frequency of intense Atlantic hurricanes. Science 2010, 327, 454–458. [Google Scholar] [CrossRef] [Green Version]
- Malet, J.-P.; Durand, Y.; Remaître, A.; Maquaire, O.; Etchevers, P.; Guyomarc’h, G.; Déqué, M.; Van Beek, L. Assessing the Influence of Climate Change on the Activity of Landslides in the Ubaye Valley. In Landslides and Climate Change–Challenges and Solutions; Taylor and Francis: London, UK, 2007; pp. 195–205. [Google Scholar]
- Crozier, M.J. Deciphering the effect of climate change on landslide activity: A review. Geomorphology 2010, 124, 260–267. [Google Scholar] [CrossRef]
- Wilson, J.F. Health and the environment after Hurricane Katrina. Ann. Int. Med. 2006, 144, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Kassotis, C.D.; Iwanowicz, L.R.; Akob, D.M.; Cozzarelli, I.M.; Mumford, A.C.; Orem, W.H.; Nagel, S.C. Endocrine disrupting activities of surface water associated with a West Virginia oil and gas industry wastewater disposal site. Sci. Total Environ. 2016, 557, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Mouritsen, A.; Aksglaede, L.; Sørensen, K.; Mogensen, S.S.; Leffers, H.; Main, K.; Frederiksen, H.; Andersson, A.M.; Skakkebaek, N.; Juul, A. Hypothesis: Exposure to endocrine-disrupting chemicals may interfere with timing of puberty. Int. J. Androl. 2010, 33, 346–359. [Google Scholar] [CrossRef]
- ter Schure, A.F.H.; Larsson, P. Polybrominated diphenyl ethers in precipitation in Southern Sweden (Skåne, Lund). Atmos. Environ. 2002, 36, 4015–4022. [Google Scholar] [CrossRef]
- Rahman, F.; Langford, K.H.; Scrimshaw, M.D.; Lester, J.N. Polybrominated diphenyl ether (PBDE) flame retardants. Sci. Total Environ. 2001, 275, 1–17. [Google Scholar] [CrossRef]
- Schneider, A.R.; Porter, E.T.; Baker, J.E. Polychlorinated Biphenyl Release from Resuspended Hudson River Sediment. Environ. Sci. Technol. 2007, 41, 1097–1103. [Google Scholar] [CrossRef]
- Balluz, L.; Moll, D.; Diaz Martinez, M.G.; Merida Colindres, J.E.; Malilay, J. Environmental pesticide exposure in Honduras following hurricane Mitch. Bull. World Health Organ. 2001, 79, 288–295. [Google Scholar]
- Nelson, G.C.; Rosegrant, M.W.; Koo, J.; Robertson, R.; Sulser, T.; Zhu, T.; Ringler, C.; Msangi, S.; Palazzo, A.; Batka, M. Climate Change: Impact on Agriculture and Costs of Adaptation; International Food Policy Research Institute: Washington, DC, USA, 2009; Volume 21. [Google Scholar]
- Nelson, G.C.; Rosegrant, M.W.; Palazzo, A.; Gray, I.; Ingersoll, C.; Robertson, R.; Tokgoz, S.; Zhu, T.; Sulser, T.B.; Ringler, C. Food Security, Farming, And Climate Change To 2050: Scenarios, Results, Policy Options; International Food Policy Research Institute: Washington, DC, USA, 2010; Volume 172. [Google Scholar]
- Okonya, J.S.; Syndikus, K.; Kroschel, J. Farmers’ perception of and coping strategies to climate change: Evidence from six Agro-Ecological zones of Uganda. J. Agric. Sci. 2013, 5, 252. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, T.; Von Braun, J. Climate change impacts on global food security. Science 2013, 341, 508–513. [Google Scholar] [CrossRef]
- Vermeulen, S.J.; Campbell, B.M.; Ingram, J.S.I. Climate Change and Food Systems. Ann. Rev. Environ. Resour. 2012, 37, 195–222. [Google Scholar] [CrossRef] [Green Version]
- Schmidhuber, J.; Tubiello, F.N. Global food security under climate change. Proc. Natl. Acad. Sci. USA 2007, 104, 19703–19708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, J.F. The impact of climate change on smallholder and subsistence agriculture. Proc. Natl. Acad. Sci. USA 2007, 104, 19680–19685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Bank. Poverty Overview. Understanding Poverty. 2019. Available online: https://www.worldbank.org/en/topic/poverty/overview (accessed on 19 January 2020).
- Singh-Peterson, L.; Shoebridge, A.; Lawrence, G. Food pricing, extreme weather and the rural/urban divide: A case study of northern nsw, Australia. J. Food Secur. 2013, 1, 42–48. [Google Scholar]
- Newsham, A.J.; Thomas, D.S.G. Knowing, farming and climate change adaptation in North-Central Namibia. Glob. Environ. Chang. 2011, 21, 761–770. [Google Scholar] [CrossRef] [Green Version]
- Sivakumar, M.V. Impacts of Natural Disasters in Agriculture, Rangeland and Forestry: An Overview. In Natural Disasters and Extreme Events in Agriculture; Springer: Berlin/Heidelberg, Germany, 2005; pp. 1–22. [Google Scholar]
- El-Khouri, B.M.; Mellner, C. Symptom development and timing of menarche: A longitudinal study. Int. J. Methods Psychiatr. Res. 2004, 13, 40–53. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Early or Late Menarche | Reference |
|---|---|---|
| Disease Causes for Perturbations in Age at Menarche | ||
| Myelomingocele (a type of spina bifida) | Early | [62] |
| Fat mass | Early | [63] |
| Inverse association with BMI (i.e., heavier BMI - earlier menarche) | Early | [64,65] |
| Metabolic syndrome | Early | [66] |
| Insulin resistance | Early | [67] |
| Not Associated with Age at Menarche | ||
| Birth weight | NA | [69] |
| Pre-term birth | NA | [70] |
| Small for gestational age | NA | [71] |
| Congenital adrenal hyperplasia | NA | [72] |
| Type 1 diabetes | Late | [64] |
| Anorexia | Late | [76] |
| Scoliosis | Late | [77] |
| Turner syndrome (one X chromosome) | Late | [78] |
| Polycystic ovarian syndrome (PCOS) | Late | [79] |
| Juvenile rheumatoid arthritis | Late | [80,81] |
| Crohn’s disease | Late | [82] |
| Disease Consequences of Perturbations in Age at Menarche (i.e., resulting from delay or early menarche) | ||
| Short stature | Early | [86] |
| Elevated BMI | Early | [87] |
| Mental Health Conditions: | ||
| Depression | Early | [90] |
| Thoughts of self-harm (but not suicidal) | Early | [91] |
| Fear | Early | [92] |
| Distress | Early | [92] |
| Externalizing disorders | Early | [92] |
| Behavioral problems | Early | [93] |
| Cardiovascular disease: | Early | [94,95,96] |
| Carotid artery intima-media thickness | Early | [95] |
| Fertility-Related Conditions: | ||
| Increased Antral follicle count (typically a sign of increased fertility) | Early | [87] |
| Premature menopause | Early | [88] |
| Hysterectomy | Early | [89] |
| Breast Cancer | Early | [97,98,100] |
| Fertility-Related Conditions: | ||
| Breast Cancer | Late | [100] |
| Fetal loss | Late | [84] |
| Longer time to first baby | Late | [84] |
| Hirsutism (excessive body hair growth) | Late | [85] |
| Bone Health Conditions: | ||
| Osteoporosis | Late | [83] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canelón, S.P.; Boland, M.R. A Systematic Literature Review of Factors Affecting the Timing of Menarche: The Potential for Climate Change to Impact Women’s Health. Int. J. Environ. Res. Public Health 2020, 17, 1703. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051703
Canelón SP, Boland MR. A Systematic Literature Review of Factors Affecting the Timing of Menarche: The Potential for Climate Change to Impact Women’s Health. International Journal of Environmental Research and Public Health. 2020; 17(5):1703. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051703
Chicago/Turabian StyleCanelón, Silvia P., and Mary Regina Boland. 2020. "A Systematic Literature Review of Factors Affecting the Timing of Menarche: The Potential for Climate Change to Impact Women’s Health" International Journal of Environmental Research and Public Health 17, no. 5: 1703. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051703