Evaluation of Health Information System (HIS) in The Surveillance of Dengue in Indonesia: Lessons from Case in Bandung, West Java


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Literature Review
2.1. Health Information System
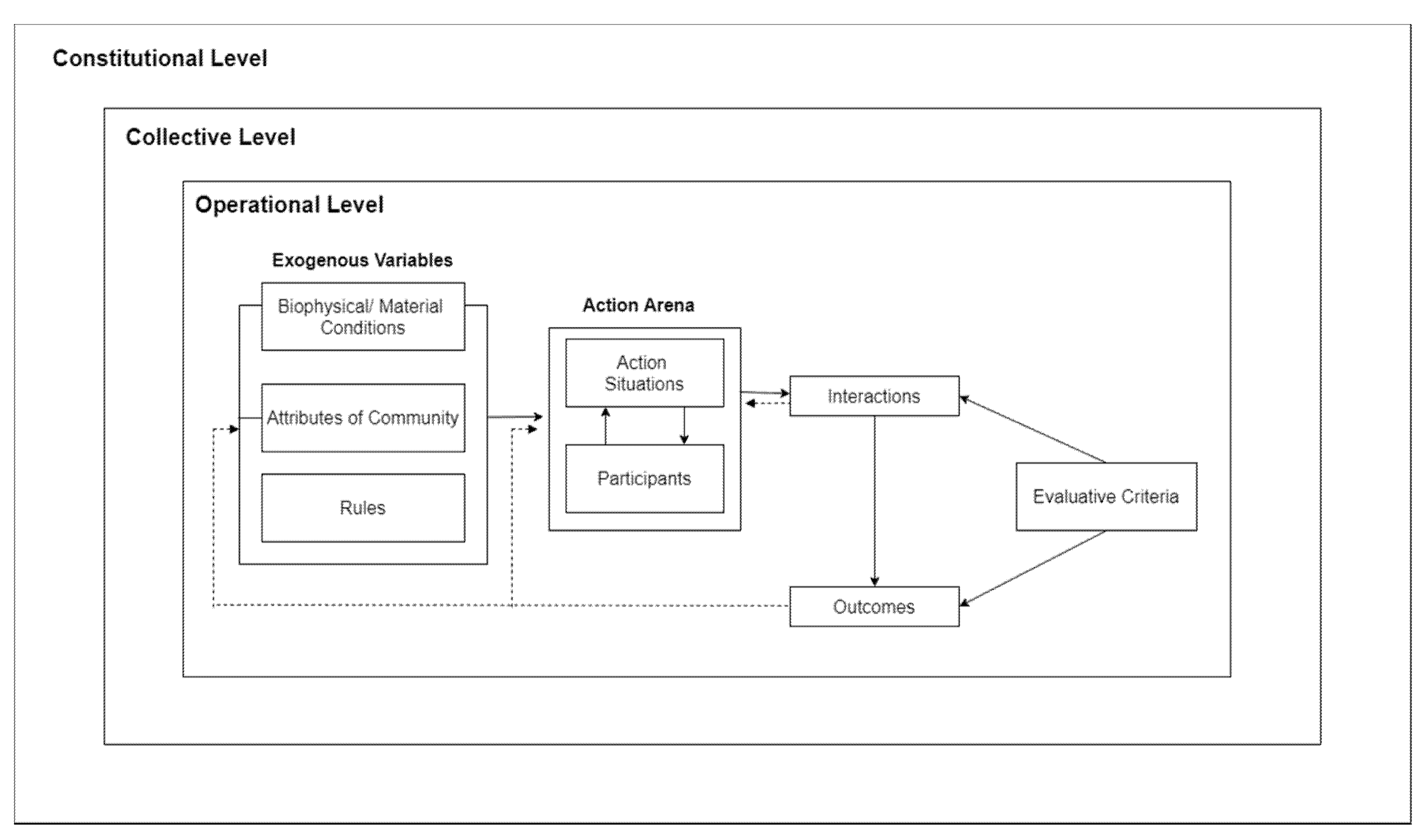
2.2. Evaluation Framework of HIS: Institutional Analysis and Development (IAD) Framework
3. Research Methods
3.1. Ethical Declaration
3.2. Study Area
3.3. Data Collection
3.4. Data Analysis
4. Results and Discussions
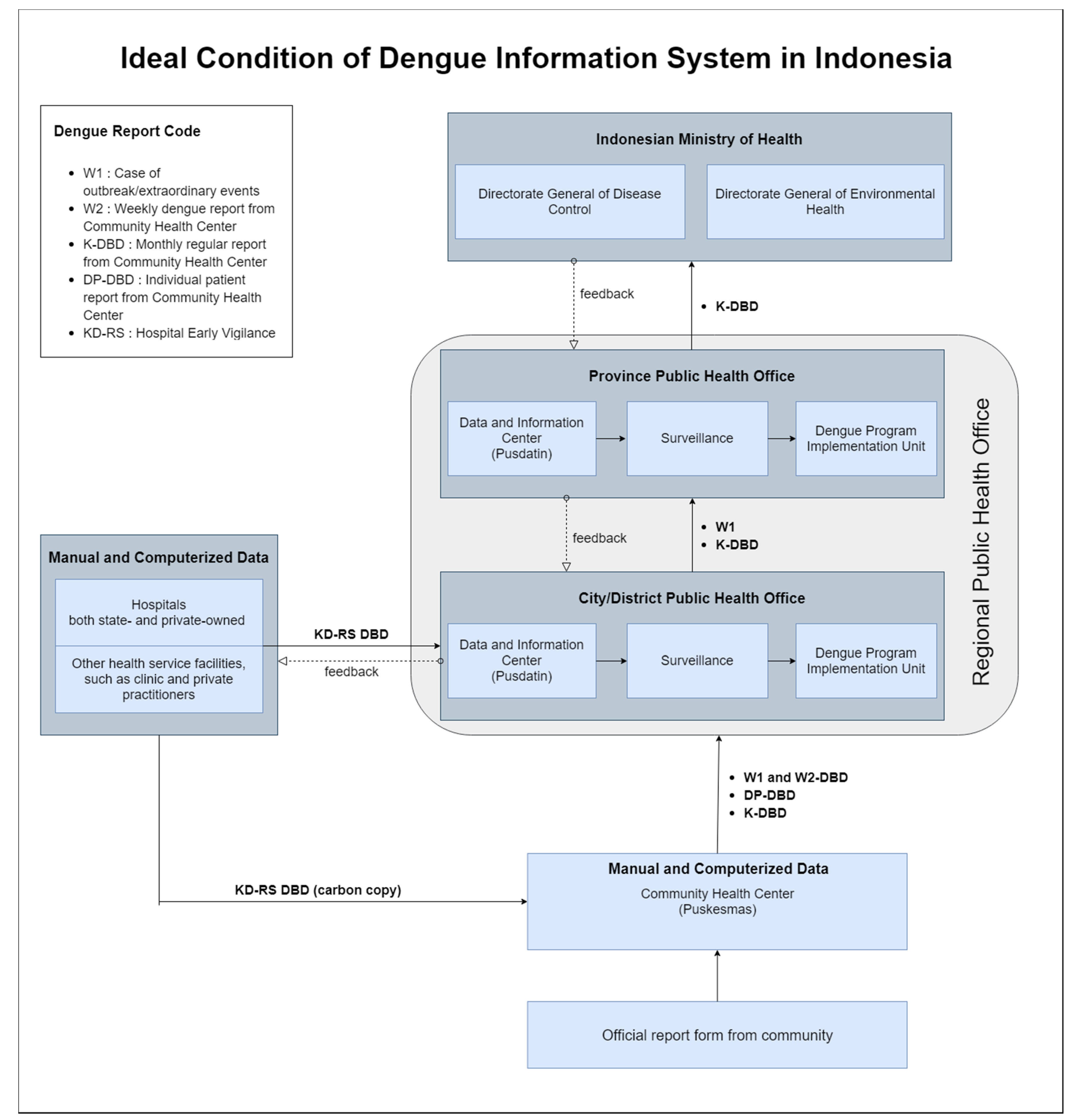
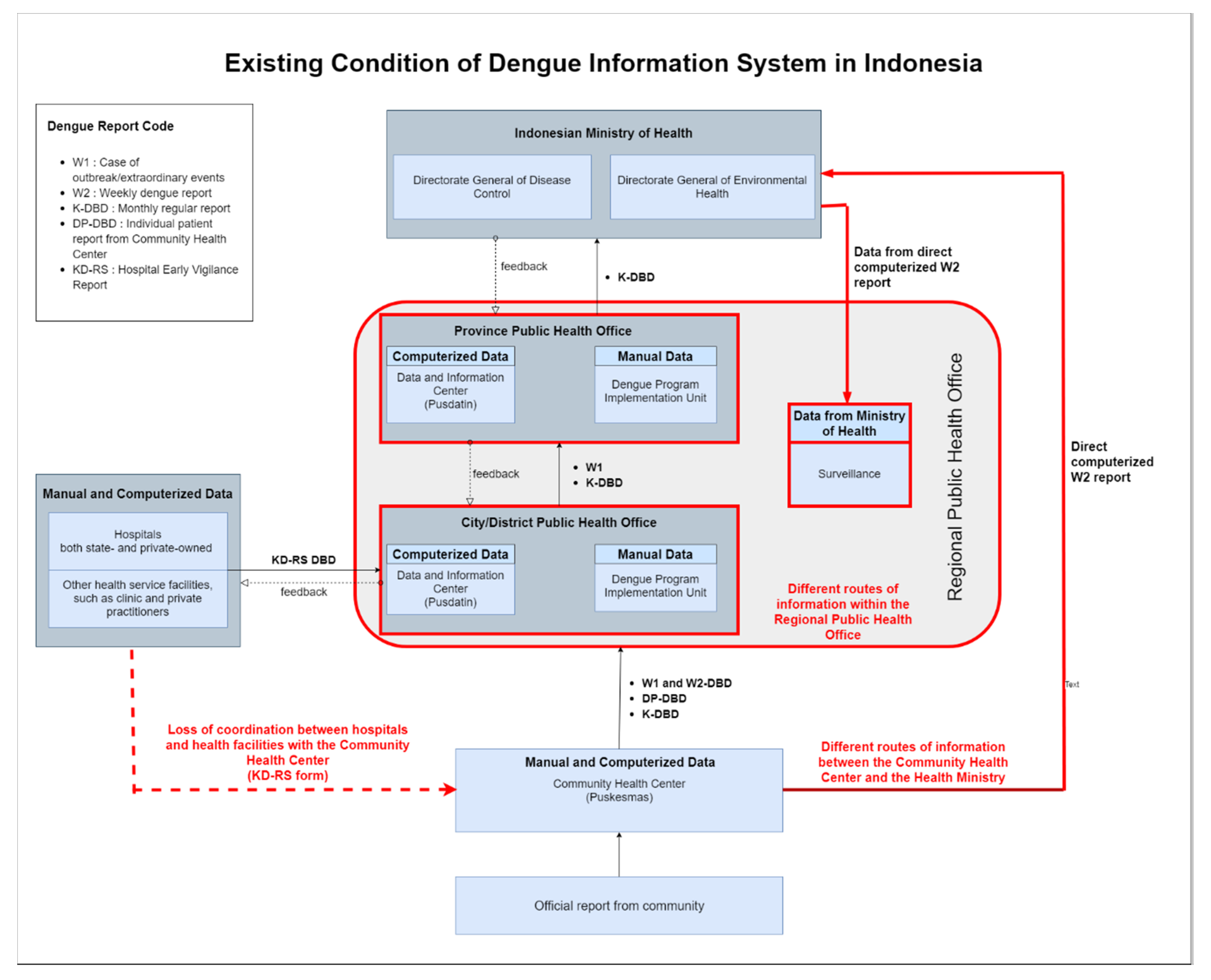
4.1. Material Condition: National Health Information System of Indonesia
- (1)
- W1 is a report that is created upon encountering dengue outbreak or extraordinary events;
- (2)
- W2 is a weekly epidemiological report that is consisted of several priority infectious diseases including dengue;
- (3)
- K-DBD is a routine monthly report of dengue case;
- (4)
- DP-DBD reports detailed record of individual dengue patients; and
- (5)
- KD-RS is reports made by hospitals and other health facilities such as clinic and private practitioners upon diagnosis of dengue among their patients
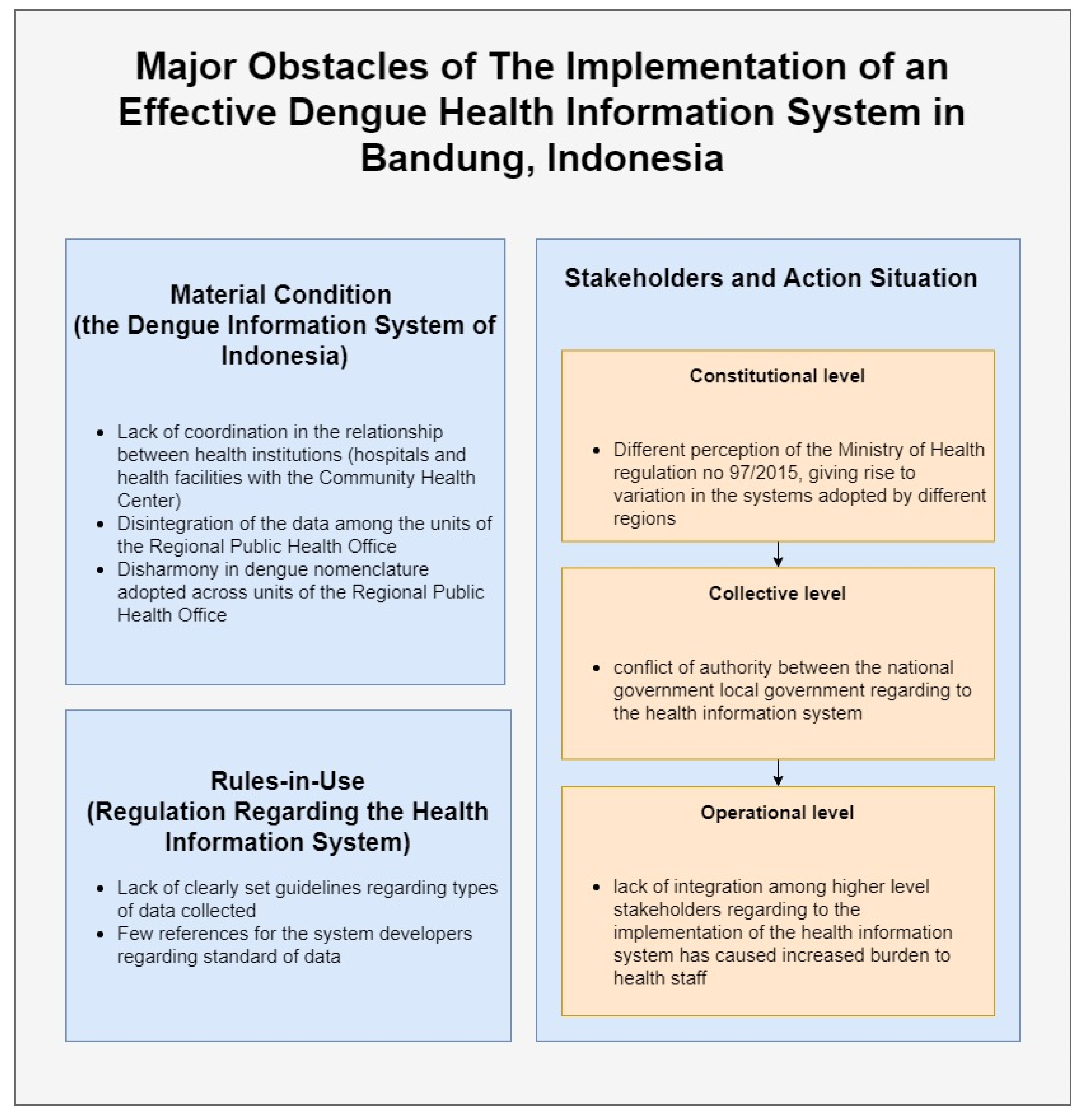
4.2. Rules-In-Use
4.3. Stakeholders and Action Situation
4.4. Recommendations for Reform
- (1)
- Insufficient government evaluation of the activities of health institutions and their compliance with regulations;
- (2)
- Unequal implementation of the health information system on the national and regional levels;
- (3)
- Lack of internal and external measures to monitor compliance with rules and a lack of consequences of defying them;
- (4)
- Low motivation and involvement of person-in-charge at the operational level.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Warkentien, T.; Pavlicek, R. Dengue Fever: Historical Perspective and the Global Response. J. Infect. Dis. Epidemiol. 2016, 2, 15. [Google Scholar] [CrossRef]
- Nadjib, M.; Setiawan, E.; Putri, S.; Nealon, J.; Beucher, S.; Hadinegoro, S.R.; Permanasari, V.Y.; Sari, K.; Wahyono, T.Y.M.; Kristin, E.; et al. Economic burden of dengue in Indonesia. PLoS Negl. Trop. Dis. 2019, 13, e0007038. [Google Scholar] [CrossRef] [Green Version]
- Haryanto, B. Indonesia Dengue Fever: Status, Vulnerability, and Challenges. In Current Topics in Tropical Emerging Diseases and Travel Medicine; IntechOpen: London, UK, 2018. [Google Scholar]
- Wahyono, T.Y.M.; Nealon, J.; Beucher, S.; Prayitno, A.; Moureau, A.; Nawawi, S.; Thabrany, H.; Nadjib, M. Indonesian dengue burden estimates: Review of evidence by an expert panel. Epidemiol. Infect. 2017, 145, 2324–2329. [Google Scholar] [CrossRef]
- Sulistyawati, S.; Dwi Astuti, F.; Rahmah Umniyati, S.; Tunggul Satoto, T.; Lazuardi, L.; Nilsson, M.; Rocklov, J.; Andersson, C.; Holmner, Å. Dengue Vector Control through Community Empowerment: Lessons Learned from a Community-Based Study in Yogyakarta, Indonesia. Int. J. Environ. Res. Public Health 2019, 16, 1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Information System. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=2ahUKEwjcvbeQo9flAhUXWCsKHf7_DZwQFjAAegQIABAC&url=https%3A%2F%2Fwww.who.int%2Fhealthinfo%2Fstatistics%2Ftoolkit_hss%2FEN_PDF_Toolkit_HSS_InformationSystems.pdf&usg=AOvVaw10i2ItGlASlaqIg7kUvpqL (accessed on 1 November 2019).
- Walsham, G. Health information systems in developing countries: Some reflections on information for action. Inf. Technol. Dev. 2020, 26, 194–200. [Google Scholar] [CrossRef]
- Roadmap Informasi Kesehatan Tahun 2011–2014. Available online: https://www.kemkes.go.id/download.php?file=download/pusdatin/lain-lain/roadmap-sik.pdf (accessed on 2 March 2020).
- Ali, M.; Park, J.-K.; von Seidlein, L.; Acosta, C.J.; Deen, J.L.; Clemens, J.D. Organizational aspects and implementation of data systems in large-scale epidemiological studies in less developed countries. BMC Public Health 2006, 6, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladwin, J.; Dixon, R.; Wilson, T. Implementing a new health management information system in Uganda. Health Policy Plan. 2003, 18, 214–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walt, G.; Gilson, L. Reforming the health sector in developing countries: The central role of policy analysis. Health Policy Plan. 1994, 9, 353–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braa, J.; Hanseth, A.; Heywood, A.; Mohammed, W.; Shaw, V. Developing Health Information Systems in Developing Countries: The Flexible Standards Strategy. MIS Q. 2007, 31, 381–402. [Google Scholar] [CrossRef] [Green Version]
- Abouzahr, C.; Boerma, T. Health information systems: The foundations of public health. Bull. World Health Organ. 2005, 83, 578–583. [Google Scholar] [PubMed]
- Nyamtema, A.S. Bridging the gaps in the Health Management Information System in the context of a changing health sector. BMC Med. Inform. Decis. Mak. 2010, 10, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaulagai, C.N.; Moyo, C.M.; Koot, J.; Moyo, H.B.; Sambakunsi, T.C.; Khunga, F.M.; Naphini, P.D. Design and implementation of a health management information system in Malawi: Issues, innovations and results. Health Policy Plan. 2005, 20, 375–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stylianides, A.; Mantas, J.; Roupa, Z.; Yamasaki, E.N. Development of an Evaluation Framework for Health Information Systems (DIPSA). Acta Inform. Med. 2018, 26, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Ammenwerth, E.; Brender, J.; Nykänen, P.; Prokosch, H.; Rigby, M.; Talmon, J. Visions and strategies to improve evaluation of health information systems. Int. J. Med. Inform. 2004, 73, 479–491. [Google Scholar] [CrossRef] [PubMed]
- Martinez, C. Barriers and challenges of implementing tobacco control policies in hospitals: Applying the institutional analysis and development framework to the Catalan Network of Smoke-Free Hospitals. Policy Politics Nurs. Pract. 2009, 10, 224–232. [Google Scholar] [CrossRef] [PubMed]
- An Institutional Framework for Policy Analysis and Design. Available online: https://www.semanticscholar.org/paper/An-Institutional-Framework-for-Policy-Analysis-and-Polski-Ostrom/ec8318779f3f04c6a88cb59cdb338d4d8cde3b85 (accessed on 10 February 2020).
- Whaley, L.; Weatherhead, E.K. An integrated approach to analyzing (adaptive) comanagement using the “politicized” IAD framework. Ecol. Soc. 2014, 19, 10. [Google Scholar] [CrossRef] [Green Version]
- Ostrom, E. Understanding Institutional Diversity; Princeton University Press: Princeton, NJ, USA, 2005. [Google Scholar]
- Nigussie, Z.; Tsunekawa, A.; Haregeweyn, N.; Adgo, E.; Cochrane, L.; Floquet, A.; Abele, S. Applying Ostrom’s institutional analysis and development framework to soil and water conservation activities in north-western Ethiopia. Land Use Policy 2018, 71, 1–10. [Google Scholar] [CrossRef]
- Hodgson, G.M. The evolution of institutions: An agenda for future theoretical research. Const. Political Econ. 2000, 13, 111–127. [Google Scholar] [CrossRef]
- Ostrom, E.; Garderner, R.; Walker, J. Rules, Games, and Common-Pool Resources. Michigan; The University of Michigan Press: Ann Arbor, MI, USA, 1994. [Google Scholar]
- Productive Inclusion of Smallholder Farmers in Brazil’s Biodiesel Value Chain: Programme Design, Institutional Incentives and Stakeholder Constraints. Available online: http://www.ipc-undp.org/pub/IPCWorkingPaper73.pdf (accessed on 10 February 2020).
- Komariah, N. Choosing Activity in Local Sectoral Programme Using Cost-Effectiveness Crlterla: Case Study the Eliminating Dengue Disease Activity in Bandung City. Ph.D Thesis, Institut Teknologi Bandung, Bandung, Indonesia, November 2006. [Google Scholar]
- Suganda, H. Jendela Bandung: Pengalaman Bersama Kompas; Penerbit Buku Kompas: Jakarta, Indonesia, 2007; pp. 4–6. [Google Scholar]
- Badan Pusat Statistik Kota Bandung. Bandung Dalam Angka 2018; Badan Pusat Statistik Kota Bandung: Bandung, Indonesia, 2018.
- BANDUNG: In Kota Bandung (West Java Province). Available online: https://www.citypopulation.de/php/indonesia-jawabarat.php?cityid=3273000000 (accessed on 4 November 2019).
- Jumlah Sarana Kesehatan di Kota Bandung Tahun 2017. Available online: http://data.bandung.go.id/dataset/jumlah-sarana-kesehatan-di-kota-bandung-tahun-2013/resource/d89bac3b-09fd-4e92-907a-19fdfecab777 (accessed on 10 February 2010).
- Kementerian Kesehatan, R.I. Pedoman Pencegahan Dan Pengendalian Demam Berdarah Dengue di Indonesia; Kementerian Kesehatan RI: Jakarta, Indonesia, 2017.
- Hapsari, R.B.; Riana, D.A.; Purwanto, E.; Kandel, N.; Setiawaty, V. Early Warning Alert and Response System (EWARS) in Indonesia: Highlight from the First Years of Implementation, 2009–2011. Health Sci. J. Indones. 2017, 8, 81–87. [Google Scholar] [CrossRef]
- Undang-Undang Republik Indonesia Nomor 36 Tahun 2009 Tentang Kesehatan. Available online: https://peraturan.bpk.go.id/Home/Details/38778/uu-no-36-tahun-2009 (accessed on 9 February 2020).
- Peraturan Presiden Republik Indonesia Nomor 47 Tahun 2009. Available online: https://kelembagaan.ristekdikti.go.id/wp-content/uploads/2017/01/nomor-47.pdf (accessed on 9 February 2020).
- Peraturan Menteri Kesehatan Republik Indonesia Nomor: 1144/MENKES/PER/VIII/2010. Available online: http://pusatkrisis.kemkes.go.id/peraturan-menteri-kesehatan-no1144menkesperviii2010 (accessed on 9 February 2020).
- Kedudukan, Tugas Dan Fungsi. Available online: https://pusdatin.kemkes.go.id/article/view/13010100003/tugas-dan-fungsi-pusdatin.html (accessed on 9 February 2020).
- Kementerian Kesehatan Republik Indonesia. Roadmap Sistem Informasi Kesehatan Tahun 2011–2014; Kementerian Kesehatan Republik Indonesia: Jakarta, Indonesia, 2012.
- Pusat Data Dan Informasi. Buletin Jendela Data Dan Informasi Kesehatan; Kementerian Kesehatan Republik Indonesia: Jakarta, Indonesia, 2016.
- Peraturan Menteri Kesehatan Republik Indonesia Nomor 97 Tahun 2015. Available online: https://pusdatin.kemkes.go.id/resources/download/pusdatin/lain-lain/PMK-No-97-Th-2015-ttg-Peta-Jalan-Sistem-Informasi-Kesehatan-Tahun-2015–2019.pdf (accessed on 9 February 2020).
- Rondo, T.V.M.; Peleal, F.J.O.; Maramis, F.R.R. Analysis of Implementation of Health Information System at Community Health Center of Southeast Minahasa Regency; Faculty of Public Health: Manado, Indonesia, 2013. [Google Scholar]
- Lippeveld, T.; Sauerborn, R.; Bodart, C.; World Health Organization. Design and Implementation of Health Information Systems; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Cucciniello, M.; Lapsley, I.; Nasi, G.; Pagliari, C. Understanding key factors affecting electronic medical record implementation: A sociotechnical approach. BMC Health Serv. Res. 2015, 15, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faridah, L.; Rinawan, F.R.; Fauziah, N.; Mayasari, W.; Dwiartama, A.; Watanabe, K. Evaluation of Health Information System (HIS) in The Surveillance of Dengue in Indonesia: Lessons from Case in Bandung, West Java. Int. J. Environ. Res. Public Health 2020, 17, 1795. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051795
Faridah L, Rinawan FR, Fauziah N, Mayasari W, Dwiartama A, Watanabe K. Evaluation of Health Information System (HIS) in The Surveillance of Dengue in Indonesia: Lessons from Case in Bandung, West Java. International Journal of Environmental Research and Public Health. 2020; 17(5):1795. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051795
Chicago/Turabian StyleFaridah, Lia, Fedri Ruluwedrata Rinawan, Nisa Fauziah, Wulan Mayasari, Angga Dwiartama, and Kozo Watanabe. 2020. "Evaluation of Health Information System (HIS) in The Surveillance of Dengue in Indonesia: Lessons from Case in Bandung, West Java" International Journal of Environmental Research and Public Health 17, no. 5: 1795. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051795