Association of Economic Status and Mortality in Patients with Acute Respiratory Distress Syndrome

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Data Source
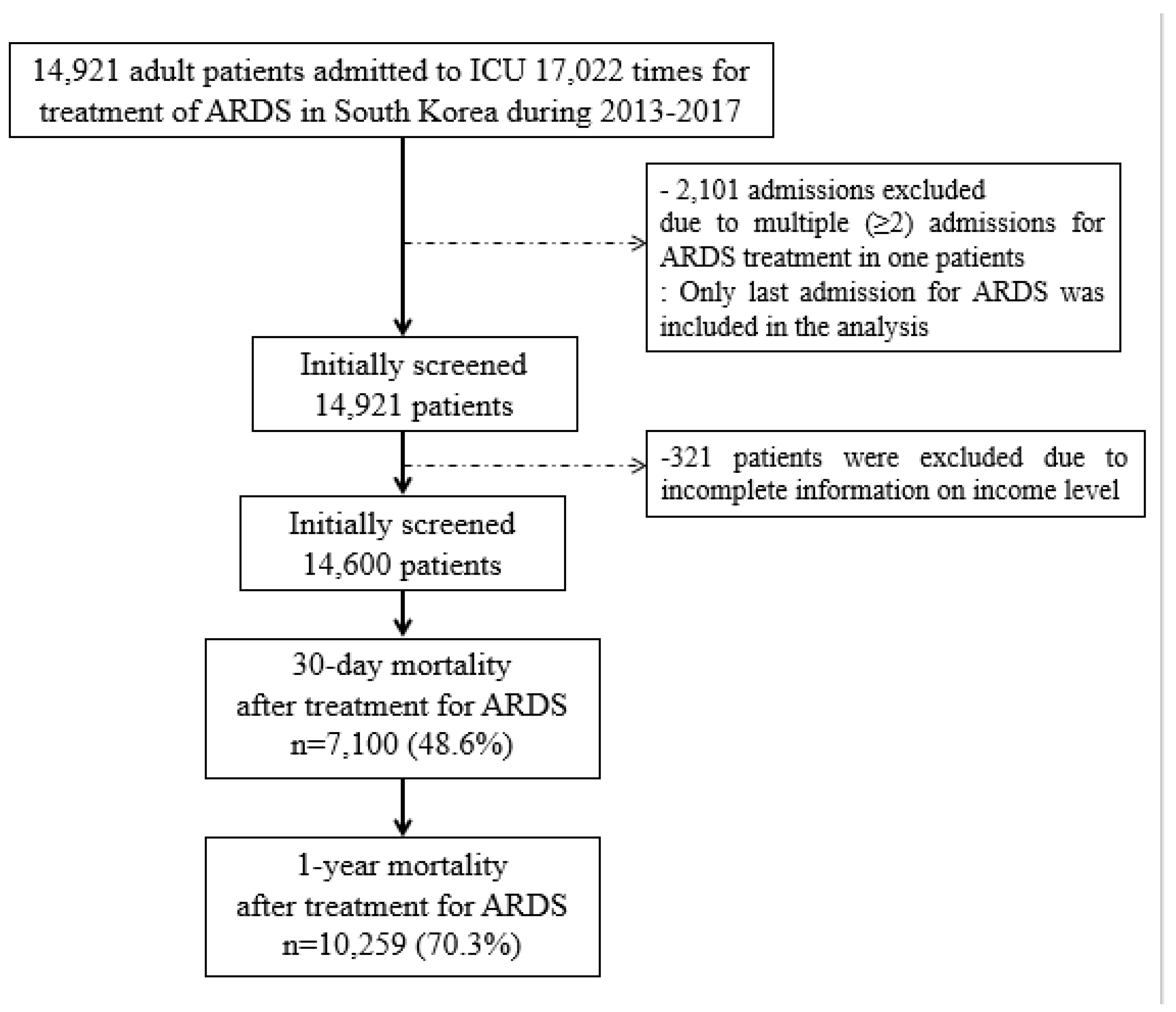
2.3. Study Population
2.4. Income Level as An Independent Variable
2.5. Study Endpoint
2.6. Confounders
2.7. Statistical Analysis
3. Results
3.1. Patients
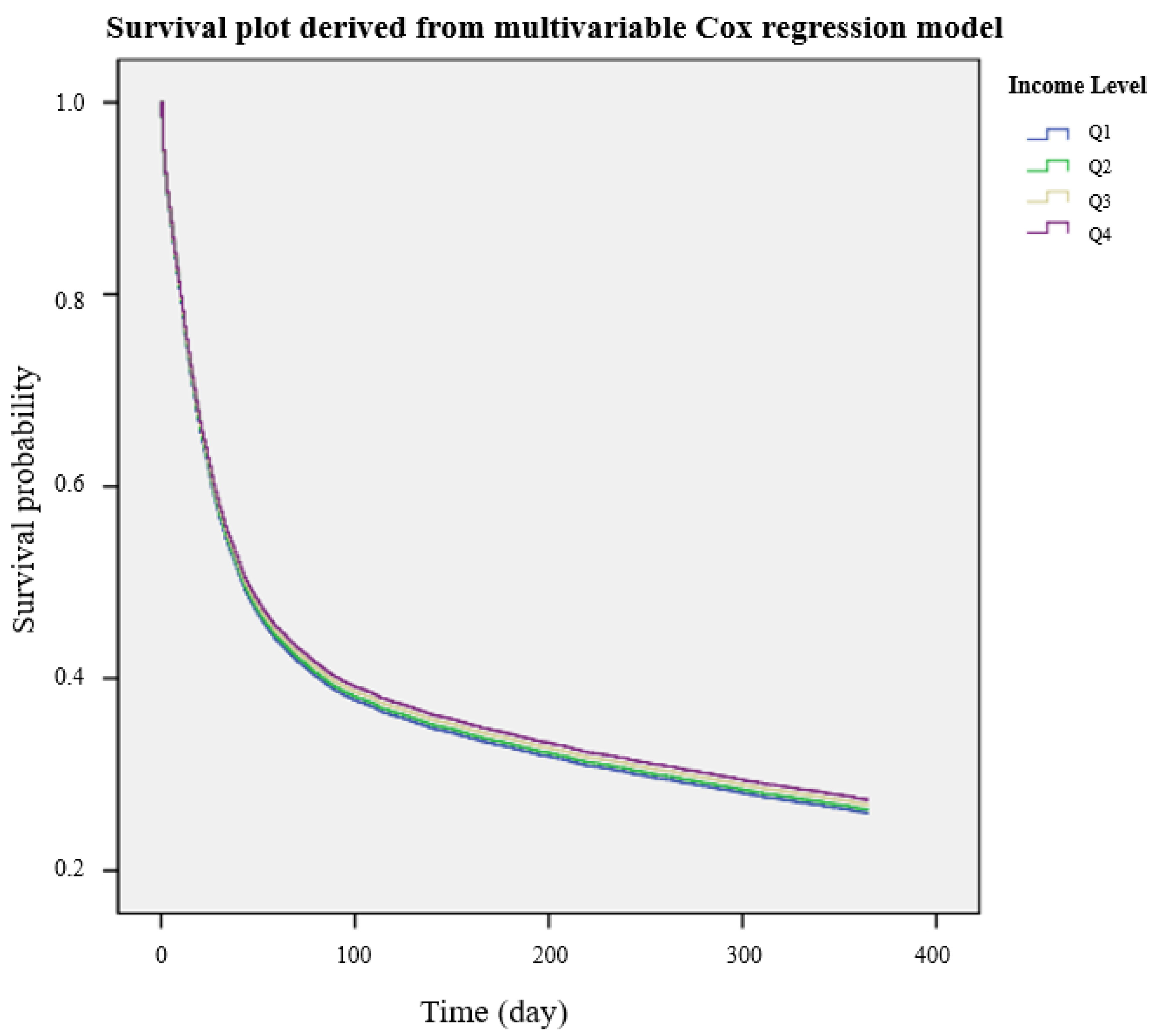
3.2. Survival Analysis According to Income Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. Acute respiratory distress in adults. Lancet 1967, 2, 319–323. [Google Scholar] [CrossRef]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R. The american-european consensus conference on ards. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am. J. Respir. Crit. Care Med. 1994, 149, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Maca, J.; Jor, O.; Holub, M.; Sklienka, P.; Bursa, F.; Burda, M.; Janout, V.; Sevcik, P. Past and present ards mortality rates: A systematic review. Respir. Care 2017, 62, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adhikari, N.K.; Fowler, R.A.; Bhagwanjee, S.; Rubenfeld, G.D. Critical care and the global burden of critical illness in adults. Lancet 2010, 376, 1339–1346. [Google Scholar] [CrossRef]
- Riviello, E.D.; Kiviri, W.; Twagirumugabe, T.; Mueller, A.; Banner-Goodspeed, V.M.; Officer, L.; Novack, V.; Mutumwinka, M.; Talmor, D.S.; Fowler, R.A. Hospital incidence and outcomes of the acute respiratory distress syndrome using the kigali modification of the berlin definition. Am. J. Respir. Crit. Care Med. 2016, 193, 52–59. [Google Scholar] [CrossRef]
- Marti, J.; Hall, P.; Hamilton, P.; Lamb, S.; McCabe, C.; Lall, R.; Darbyshire, J.; Young, D.; Hulme, C. One-year resource utilisation, costs and quality of life in patients with acute respiratory distress syndrome (ards): Secondary analysis of a randomised controlled trial. J. Intensive Care 2016, 4, 56. [Google Scholar] [CrossRef] [Green Version]
- Oh, T.K.; Jo, J.; Jeon, Y.-T.; Song, I. Impact of socioeconomic status on 30-day and 1-year mortalities after intensive care unit admission in south korea: A retrospective cohort study. Acute Crit. Care 2018, 33, 230–237. [Google Scholar] [CrossRef]
- Schnegelsberg, A.; Mackenhauer, J.; Nibro, H.L.; Dreyer, P.; Koch, K.; Kirkegaard, H. Impact of socioeconomic status on mortality and unplanned readmission in septic intensive care unit patients. Acta Anaesthesiol. Scand. 2016, 60, 465–475. [Google Scholar] [CrossRef]
- Sinharoy, A.; Mitra, S.; Mondal, P. Socioeconomic and environmental predictors of asthma-related mortality. J. Environ. Public Health 2018, 2018, 9389570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schechter, M.S.; Shelton, B.J.; Margolis, P.A.; Fitzsimmons, S.C. The association of socioeconomic status with outcomes in cystic fibrosis patients in the united states. Am. J. Respir. Crit. Care Med. 2001, 163, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Bime, C.; Poongkunran, C.; Borgstrom, M.; Natt, B.; Desai, H.; Parthasarathy, S.; Garcia, J.G. Racial differences in mortality from severe acute respiratory failure in the united states, 2008–2012. Ann. Am. Thorac. Soc. 2016, 13, 2184–2189. [Google Scholar] [CrossRef] [PubMed]
- Laffey, J.G.; Madotto, F.; Bellani, G.; Pham, T.; Fan, E.; Brochard, L.; Amin, P.; Arabi, Y.; Bajwa, E.K.; Bruhn, A.; et al. Geo-economic variations in epidemiology, patterns of care, and outcomes in patients with acute respiratory distress syndrome: Insights from the lung safe prospective cohort study. Lancet Respir. Med. 2017, 5, 627–638. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S. Thirty years of national health insurance in south korea: Lessons for achieving universal health care coverage. Health Policy Plan. 2009, 24, 63–71. [Google Scholar] [CrossRef]
- Cha, J.K.; Oh, T.K.; Song, I.A. Impacts of financial coverage on long-term outcome of intensive care unit survivors in south korea. Yonsei Med. J. 2019, 60, 976–983. [Google Scholar] [CrossRef]
- Howard, A.E.; Courtney-Shapiro, C.; Kelso, L.A.; Goltz, M.; Morris, P.E. Comparison of 3 methods of detecting acute respiratory distress syndrome: Clinical screening, chart review, and diagnostic coding. Am. J. Crit. Care 2004, 13, 59–64. [Google Scholar] [CrossRef]
- Kumar, G.; Taneja, A.; Majumdar, T.; Jacobs, E.R.; Whittle, J.; Nanchal, R.; Milwaukee Initiative in Critical Care Outcomes Research (MICCOR) Group of Investigators. The association of lacking insurance with outcomes of severe sepsis: Retrospective analysis of an administrative database. Crit. Care Med. 2014, 42, 583–591. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, J.M.; Lu, B.; Ali, N.A.; Levine, D.A.; Aberegg, S.K.; Lemeshow, S. Insurance type and sepsis-associated hospitalizations and sepsis-associated mortality among us adults: A retrospective cohort study. Crit. Care 2011, 15, R130. [Google Scholar] [CrossRef] [Green Version]
- Herridge, M.S.; Cheung, A.M.; Tansey, C.M.; Matte-Martyn, A.; Diaz-Granados, N.; Al-Saidi, F.; Cooper, A.B.; Guest, C.B.; Mazer, C.D.; Mehta, S.; et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N. Engl. J. Med. 2003, 348, 683–693. [Google Scholar] [CrossRef] [Green Version]
- Herridge, M.S.; Tansey, C.M.; Matte, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional disability 5 years after acute respiratory distress syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herridge, M.S.; Chu, L.M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J.O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; et al. The recover program: Disability risk groups and 1-year outcome after 7 or more days of mechanical ventilation. Am. J. Respir. Crit. Care Med. 2016, 194, 831–844. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, B.B.; Huang, M.; Dinglas, V.D.; Colantuoni, E.; Von Wachter, T.M.; Hopkins, R.O.; Needham, D.M.; National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome Network. Joblessness and lost earnings after acute respiratory distress syndrome in a 1-year national multicenter study. Am. J. Respir. Crit. Care Med. 2017, 196, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, B.B.; Sepulveda, K.A.; Chong, A.; Lord, R.K.; Dinglas, V.D.; Mendez-Tellez, P.A.; Shanholtz, C.; Colantuoni, E.; Von Wachter, T.M.; Pronovost, P.J.; et al. Return to work and lost earnings after acute respiratory distress syndrome: A 5-year prospective, longitudinal study of long-term survivors. Thorax 2018, 73, 125–133. [Google Scholar] [CrossRef]
- Fowler, R.A.; Noyahr, L.A.; Thornton, J.D.; Pinto, R.; Kahn, J.M.; Adhikari, N.K.; Dodek, P.M.; Khan, N.A.; Kalb, T.; Hill, A.; et al. An official american thoracic society systematic review: The association between health insurance status and access, care delivery, and outcomes for patients who are critically ill. Am. J. Respir. Crit. Care Med. 2010, 181, 1003–1011. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Total (14,600), n (%) | Mean (SD) | |
|---|---|---|---|
| Age, year | 69.8 (15.3) | ||
| Gender, male | 9065 (62.1) | ||
| Residence at diagnosis | |||
| Capital city, Seoul | 2402 (16.5) | ||
| Other metropolitan city a | 3334 (22.8) | ||
| Others | 8864 (60.7) | ||
| Income level at diagnosis | |||
| Q1 | 2449 (16.8) | ||
| Q2 | 2732 (18.7) | ||
| Q3 | 4199 (28.8) | ||
| Q4 | 5220 (35.8) | ||
| Length of hospital stay, day | 16.2 (15.0) | ||
| Duration of treatment, day | 18.4 (17.1) | ||
| ECMO use for treatment | 681 (4.7) | ||
| Comorbidities before diagnosis | |||
| Hypertension | 9735 (66.7) | ||
| Coronary artery disease | 4403 (30.2) | ||
| Diabetes mellitus | 6500 (44.5) | ||
| Cerebrovascular disease | 5044 (34.5) | ||
| Lung cancer | 1125 (7.7) | ||
| Chronic kidney disease | 1434 (9.8) | ||
| Dyslipidemia | 8021 (54.9) | ||
| Anemia | 2733 (18.7) | ||
| COPD | 3819 (26.2) | ||
| Asthma | 1809 (12.4) | ||
| Arrhythmia | 1017 (7.0) | ||
| Liver cirrhosis | 408 (2.8) | ||
| Diagnosis per year | |||
| 2013 | 1978 (13.5) | ||
| 2014 | 2089 (14.3) | ||
| 2015 | 2065 (14.1) | ||
| 2016 | 2289 (15.7) | ||
| 2017 | 6179 (42.3) | ||
| Variable | 30-Day Mortality | p | 1-Year Mortality | p | |
|---|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | ||||
| Income level at ARDS diagnosis | |||||
| Q1 | 1 | 1 | |||
| Q2 | 1.02 (0.94, 1.10) | 0.719 | 0.99 (0.93, 1.06) | 0.762 | |
| Q3 | 1.00 (0.93, 1.08) | 0.946 | 0.98 (0.92, 1.04) | 0.420 | |
| Q4 | 0.98 (0.91, 1.05) | 0.542 | 0.96 (0.91, 1.02) | 0.189 | |
| Age, year | 1.02 (1.01, 1.02) | <0.001 | 1.02 (1.01, 1.02) | <0.001 | |
| Gender, male | 1.00 (0.95, 1.05) | 0.895 | 1.03 (0.99, 1.07) | 0.167 | |
| Residence at diagnosis | |||||
| Capital city, Seoul | 1 | 1 | |||
| Other metropolitan city | 1.18 (1.09, 1.27) | <0.001 | 1.12 (1.06, 1.20) | <0.001 | |
| Others | 1.11 (1.04, 1.19) | 0.002 | 1.04 (0.98, 1.09) | 0.211 | |
| ECMO use for treatment | 1.30 (1.16, 1.45) | <0.001 | 1.38 (1.25, 1.52) | <0.001 | |
| Comorbidity before diagnosis | |||||
| Hypertension | 0.92 (0.87, 0.97) | 0.004 | 0.93 (0.89, 0.97) | 0.002 | |
| Coronary artery disease | 0.97 (0.92, 1.03) | 0.285 | 0.95 (0.91, 1.00) | 0.029 | |
| Diabetes mellitus | 0.99 (0.94, 1.04) | 0.687 | 0.98 (0.94, 1.02) | 0.397 | |
| Cerebrovascular disease | 0.89 (0.84, 0.94) | <0.001 | 0.93 (0.89, 0.97) | 0.002 | |
| Lung cancer | 0.99 (0.91, 1.08) | 0.799 | 1.09 (1.02, 1.17) | 0.017 | |
| Chronic kidney disease | 0.80 (0.73, 0.87) | <0.001 | 0.84 (0.78, 0.90) | <0.001 | |
| Dyslipidemia | 1.06 (1.00, 1.12) | 0.039 | 1.07 (1.02, 1.12) | 0.004 | |
| Anemia | 0.94 (0.88, 1.00) | 0.050 | 0.95 (0.87, 1.03) | 0.182 | |
| COPD | 0.76 (0.71, 0.80) | <0.001 | 0.77 (0.74, 0.81) | <0.001 | |
| Asthma | 0.98 (0.90, 1.06) | 0.539 | 0.96 (0.90, 1.02) | 0.194 | |
| Arrhythmia | 0.95 (0.86, 1.05) | 0.332 | 0.95 (0.87, 1.03) | 0.182 | |
| Liver cirrhosis | 1.17 (1.01, 1.34) | 0.034 | 1.17 (1.04, 1.31) | 0.010 | |
| Diagnosis per year | |||||
| 2013 | 1 | 1 | |||
| 2014 | 0.86 (0.80, 0.93) | <0.001 | 0.84 (0.78, 0.89) | <0.001 | |
| 2015 | 0.84 (0.78, 0.91) | <0.001 | 0.76 (0.72, 0.82) | <0.001 | |
| 2016 | 0.79 (0.73, 0.85) | <0.001 | 0.70 (0.66, 0.75) | <0.001 | |
| 2017 | 0.25 (0.23, 0.27) | <0.001 | 0.16 (0.15, 0.18) | <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.K.; Song, I.-A.; Lee, J.H. Association of Economic Status and Mortality in Patients with Acute Respiratory Distress Syndrome. Int. J. Environ. Res. Public Health 2020, 17, 1815. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061815
Oh TK, Song I-A, Lee JH. Association of Economic Status and Mortality in Patients with Acute Respiratory Distress Syndrome. International Journal of Environmental Research and Public Health. 2020; 17(6):1815. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061815
Chicago/Turabian StyleOh, Tak Kyu, In-Ae Song, and Jae Ho Lee. 2020. "Association of Economic Status and Mortality in Patients with Acute Respiratory Distress Syndrome" International Journal of Environmental Research and Public Health 17, no. 6: 1815. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061815