Malaria Case Fatality Rate among Children under Five in Burkina Faso: An Assessment of the Spatiotemporal Trends Following the Implementation of Control Programs

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings
2.2. Data Sources
2.2.1. Malaria Case Fatality Data
2.2.2. Malaria Control Programs Data
2.2.3. Control Variables
2.3. Statistical Analysis of Malaria CFR
2.3.1. Estimating District-Level Interventions Coverage
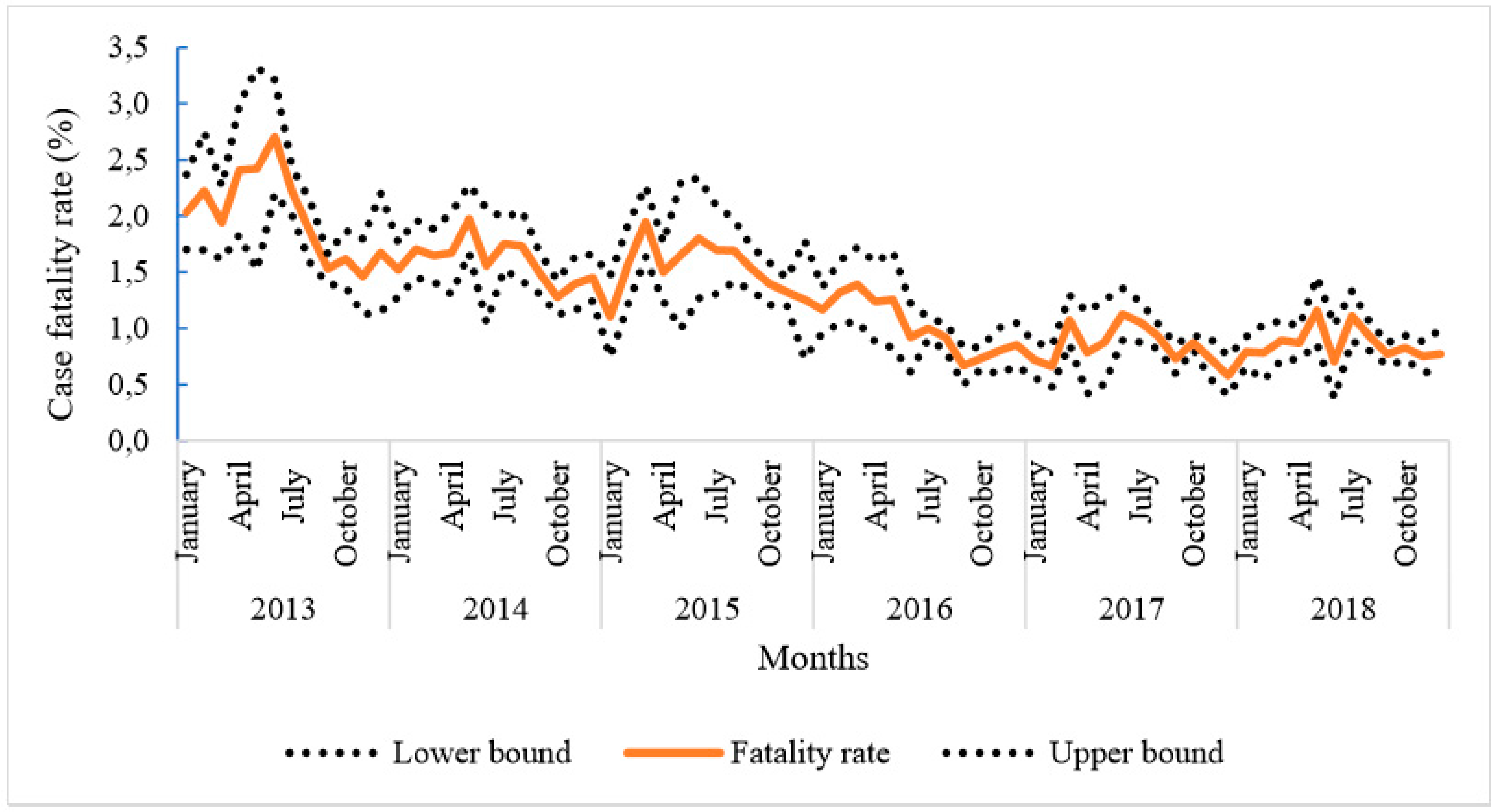
2.3.2. Descriptive Analysis of Temporal Trends
2.3.3. Spatiotemporal Modelling
2.3.4. Ethical Considerations
3. Results
3.1. Summary of Crude Estimates of Severe Malaria Case Fatality Rate in Children under Five
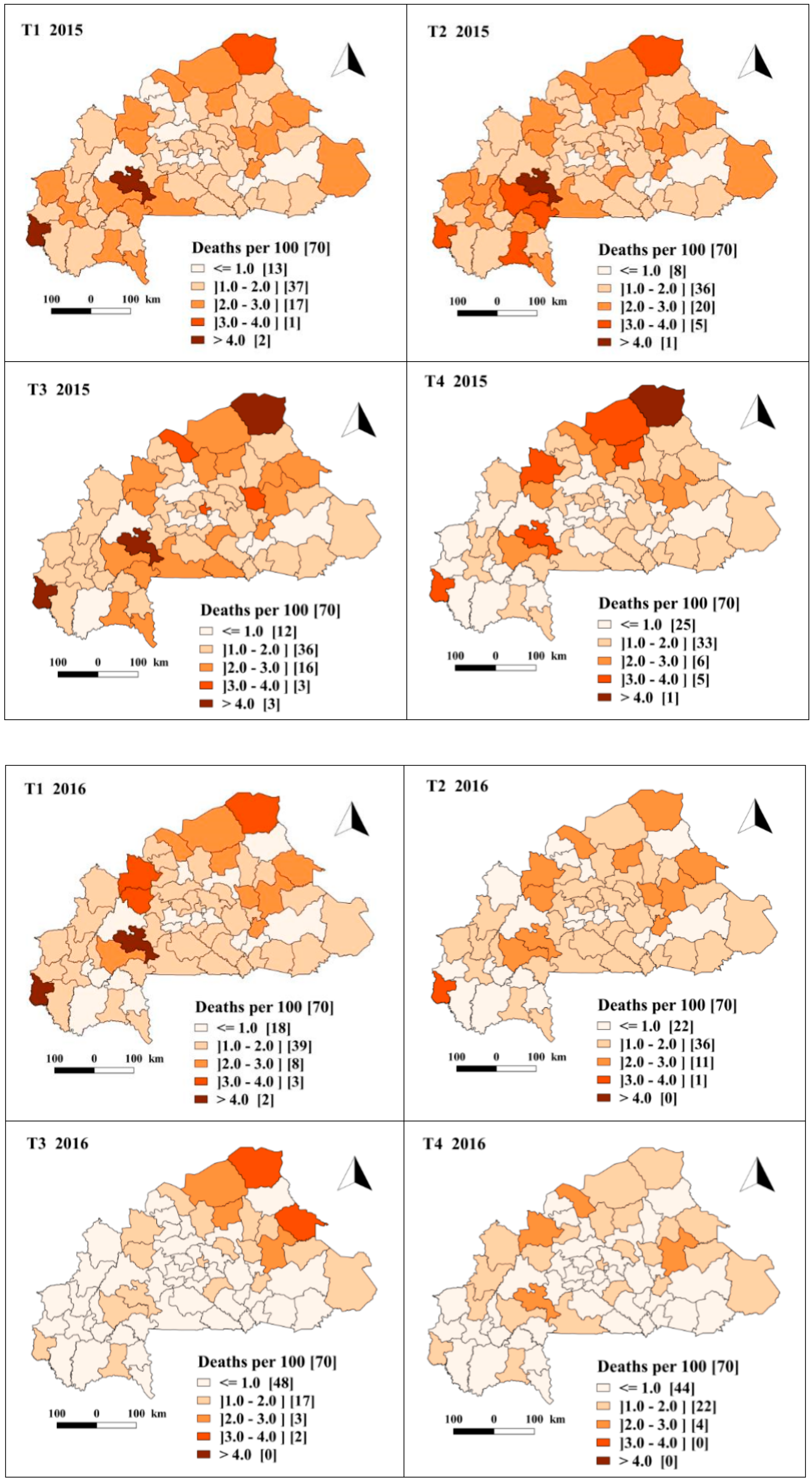
3.2. Spatio-Temporal Dynamics of Crude and Predicted Rate of Malaria Case Fatality Rate by Quarter and by District
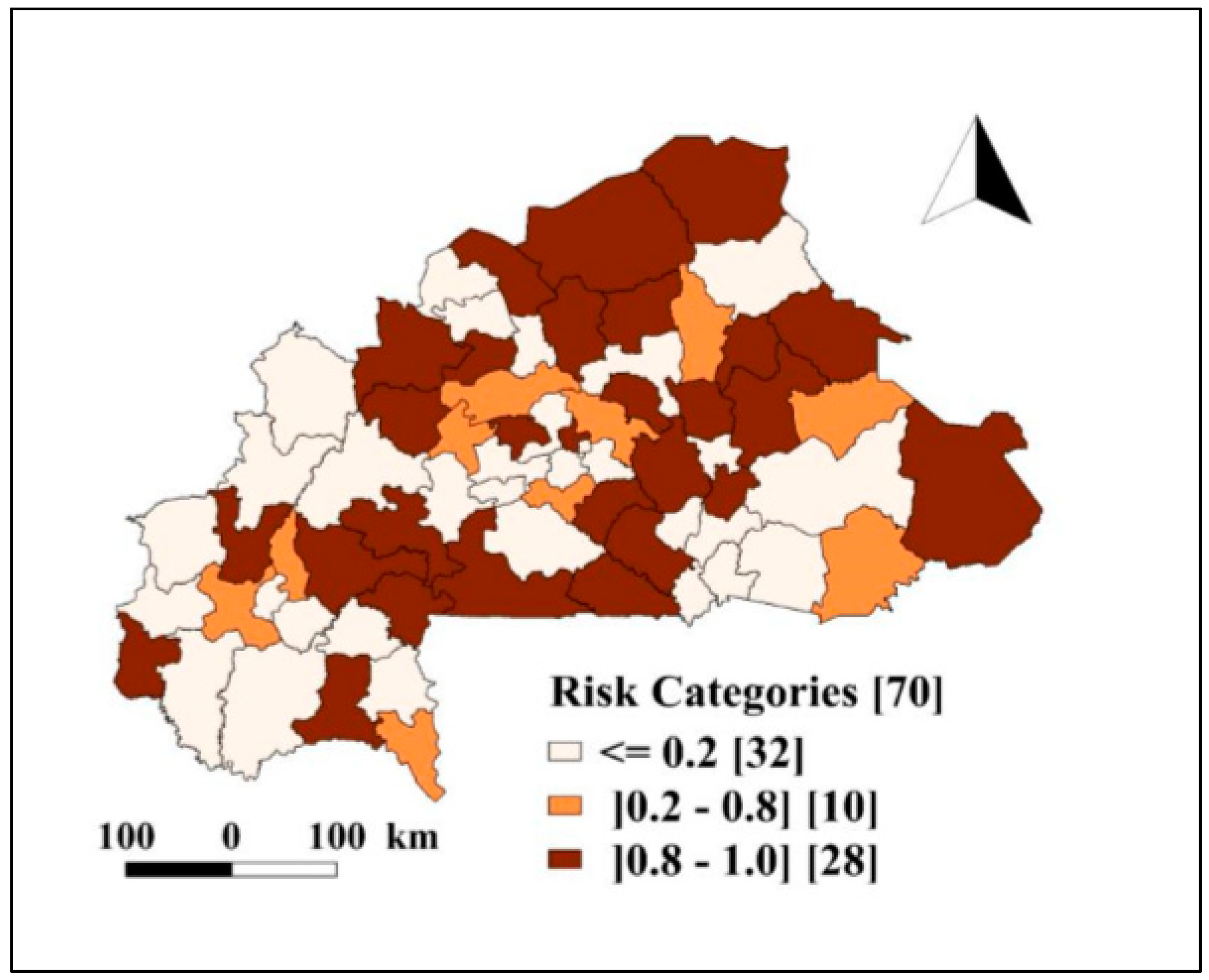
3.3. Spatial Pattern of Risk of Death Due to Severe Malaria among Children under Five
3.4. Association between Health Programs and Malaria Case Fatality Rate
4. Discussion
5. Conclusions
6. Research Data and Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BCI | Bayesian credible intervals |
| DIC | Deviance information criterion |
| DHIS2 | District Health Information System |
| INLA | Integrated Nested Laplace Approximation |
| mCFR | malaria case fatality risk |
| RDT | Rapid Diagnostic Test |
Appendix A1. Estimating District-Level Interventions Coverage




Appendix A2. Choice of ZIP Model or ZNIB for Modelling
References
- World Health Organization. World Malaria Report 2019. Available online: https://www.who.int/publications-detail/world-malaria-report-2019 (accessed on 21 November 2018).
- Rowe, A.K.; Rowe, S.Y.; Snow, R.W.; Korenromp, E.L.; Schellenberg, J.R.; Stein, C.; Nahlen, B.L.; Bryce, J.; Black, R.E.; Steketee, R.W. The burden of malaria mortality among African children in the year 2000. Int. J. Epidemiol. 2006, 35, 691–704. [Google Scholar] [CrossRef] [Green Version]
- Walker, K. A review of control methods for African malaria vectors. Environ. Health Proj. 2002, 2, 618–627. [Google Scholar]
- Ministère de la Santé. Annuaire Statistique 2018. Available online: http://www.cns.bf/IMG/pdf/annuaire_ms_2018.pdf (accessed on 21 September 2019).
- Ministère de la Santé. Plan Stratégique National de Lutte Contre le Paludisme du Burkina Faso 2016–2020. Available online: http://onsp-sante.bf/sites/default/files/publications/166/PSN%20%20%20%20%202016-2020_Paludisme_20_02_2017.pdf (accessed on 21 October 2019).
- Chuma, J.; Okungu, V.; Molyneux, C. Barriers to prompt and effective malaria treatment among the poorest population in Kenya. Malar. J. 2010, 9, 144. [Google Scholar] [CrossRef] [Green Version]
- Halwindi, H.; Siziya, S.; Magnussen, P.; Olsen, A. Factors perceived by caretakers as barriers to health care for under-five children in Mazabuka District, Zambia. Int. Sch. Res. Not. 2013, 2013, 905836. [Google Scholar] [CrossRef]
- Sieleunou, I.; Betsi, E.; Kouontchou, J.; Nguela, A.T.; Yumo, H.A. Removing the user fees for the under-fives’ simple malaria treatment in Cameroon effect on the health services utilization. J. Community Med. Health Educ. 2015, 5, 383. [Google Scholar] [CrossRef] [Green Version]
- Chuma, J.; Musimbi, J.; Okungu, V.; Goodman, C.; Molyneux, C. Reducing user fees for primary health care in Kenya: Policy on paper or policy in practice? Int. J. Equity Health 2009, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Lagarde, M.; Palmer, N. The impact of user fees on health service utilization in low- and middle-income countries: How strong is the evidence? Bull. World Health Organ. 2008, 86, 839–848. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, B.; Harper, S.; Kaufman, J.S.; Bergevin, Y. Removing user fees for facility-based delivery services: A difference-in-differences evaluation from ten sub-Saharan African countries. Health Policy Plan. 2015, 30, 432–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atchessi, N.; Ridde, V.; Zunzunegui, M.V. User fees exemptions alone are not enough to increase indigent use of healthcare services. Health Policy Plan. 2016, 31, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Heinmüller, R.; Dembélé, Y.A.; Jouquet, G.; Haddad, S.; Ridde, V. Free healthcare provision with an NGO or by the Malian government. Impact on health center attendance by children under five. Field Actions Sci. Rep. 2013. Available online: http://journals.openedition.org/factsreports/1731 (accessed on 21 September 2019).
- Nyonator, F.; Kutzin, J. Health for some? The effects of user fees in the Volta Region of Ghana. Health Policy Plan. 1999, 14, 329–341. [Google Scholar] [CrossRef] [Green Version]
- Penfold, S.; Harrison, E.; Bell, J.; Fitzmaurice, A. Evaluation of the delivery fee exemption policy in ghana: Population estimates of changes in delivery service utilization in two regions. Ghana Med. J. 2007, 41, 100–109. [Google Scholar]
- Ponsar, F.; Van Herp, M.; Zachariah, R.; Gerard, S.; Philips, M.; Jouquet, G. Abolishing user fees for children and pregnant women trebled uptake of malaria-related interventions in Kangaba, Mali. Health Policy Plan. 2011, 26 (Suppl 2), ii72–ii83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organisation International. Décret 2016-311_PRES/PM/MS/MATDSI/MINEFID Portant Gratuité de Soins au Profit des Femmes et des Enfants de Moins de Cinq ans Vivant au Burkina Faso. JO N°22.du 02 juin 2016. Available online: http://www.ilo.org/dyn/natlex/docs/ELECTRONIC/104122/126889/F331618513/BFA-104122.pdf (accessed on 21 September 2019).
- Ministère de la Santé. Annuaire Statistique 2016. Available online: http://www.cns.bf/IMG/pdf/annuaire_2016_ms_signe.pdf (accessed on 21 September 2019).
- Ministère de la Santé. Annuaire Statistique 2017. Available online: http://www.cns.bf/IMG/pdf/annuaire_ms_2017.pdf (accessed on 21 September 2019).
- Alegana, V.A.; Atkinson, P.M.; Lourenco, C.; Ruktanonchai, N.W.; Bosco, C.; Erbach-Schoenberg, E.Z.; Didier, B.; Pindolia, D.; Menach, A.L.; Katokele, S.; et al. Advances in mapping malaria for elimination: Fine resolution modelling of Plasmodium falciparum incidence. Sci. Rep. 2016, 6, 29628. [Google Scholar] [CrossRef] [PubMed]
- Ouedraogo, M.; Samadoulougou, S.; Rouamba, T.; Hien, H.; Sawadogo, J.E.M.; Tinto, H.; Alegana, V.A.; Speybroeck, N.; Kirakoya-Samadoulougou, F. Spatial distribution and determinants of asymptomatic malaria risk among children under 5 years in 24 districts in Burkina Faso. Malar. J. 2018, 17, 460. [Google Scholar] [CrossRef] [PubMed]
- Samadoulougou, S.; Maheu-Giroux, M.; Kirakoya-Samadoulougou, F.; De Keukeleire, M.; Castro, M.C.; Robert, A. Multilevel and geo-statistical modeling of malaria risk in children of Burkina Faso. Parasites Vectors 2014, 7, 350. [Google Scholar] [CrossRef] [Green Version]
- Ssempiira, J.; Kissa, J.; Nambuusi, B.; Kyozira, C.; Rutazaana, D.; Mukooyo, E.; Opigo, J.; Makumbi, F.; Kasasa, S.; Vounatsou, P. The effect of case management and vector-control interventions on space-time patterns of malaria incidence in Uganda. Malar. J. 2018, 17, 162. [Google Scholar] [CrossRef]
- Besag, J.; York, J.; Mollié, A. Bayesian image restoration, with two applications in spatial statistics. Ann. Inst. Stat. Math. 1991, 43, 1–20. [Google Scholar] [CrossRef]
- Stern, H. Inference for extremes in disease mapping. In Disease Mapping and Risk Assessment for Public Health; Lawson, A.B., Biggeri, A., Bohning, D., Lesaffre, E., Viel, J.F., Bertollini, R., Eds.; John Wiley & Son: Hoboken, NJ, USA, 1999; pp. 63–84. [Google Scholar]
- Ouedraogo, M.; Rouamba, T.; Samadoulougou, S.; Kirakoya-Samadoulougou, F. Effect of Free Healthcare Policy for Children under Five Years Old on the Incidence of Reported Malaria Cases in Burkina Faso by Bayesian Modelling: “Not only the Ears but also the Head of the Hippopotamus”. Int. J. Environ. Res. Public Health 2020, 17, 417. [Google Scholar] [CrossRef] [Green Version]
- Rouamba, T.; Samadoulougou, S.; Tinto, H.; Alegana, V.A.; Kirakoya-Samadoulougou, F. Bayesian Spatiotemporal Modeling of Routinely Collected Data to Assess the Effect of Health Programs in Malaria Incidence During Pregnancy in Burkina Faso. Sci. Rep. 2020, 10, 2618. [Google Scholar] [CrossRef] [Green Version]
- Rouamba, T.; Samadoulougou, S.; Tinto, H.; Alegana, V.A.; Kirakoya-Samadoulougou, F. Severe-malaria infection and its outcomes among pregnant women in Burkina Faso health-districts: Hierarchical Bayesian space-time models applied to routinely-collected data from 2013 to 2018. Spat. Spatio-Temporal Epidemiol. 2020, 33, 100333. [Google Scholar] [CrossRef]
- Institut National de la Statistique et de la Démographie. Projection Démographique de 2007–2020. 2009. Available online: http://www.cns.bf/IMG/pdf/projections_demographiques_sous_nationales.pdf (accessed on 21 September 2019).
- Ministère de la Santé. Carte_Sanitaire_2010. Available online: http://www.cns.bf/IMG/pdf/carte_sanitaire_2010.pdf (accessed on 21 September 2019).
- Ministère de la Santé. Plan National de Développement Sanitaire. 2011, pp. 3–22. Available online: https://www.uhc2030.org/fileadmin/uploads/ihp/Documents/Country_Pages/Burkina_Faso/Burkina_Faso_National_Health_Strategy_2011-2020_French.pdf (accessed on 21 September 2019).
- Institut national de la Statistique et de la Démographie. Enquête Multisectorielle Continue sur les Conditions de vie des Ménages. 2014. Available online: http://www.insd.bf/n/contenu/enquetes_recensements/Enq_EMC/Profil_de_pauvrete_et_d_inegalite_en_2014.pdf (accessed on 21 October 2019).
- Institut National de la Statistique et de la Démographie. Enqête Démographique et de Santé et à Indicateurs Multiples (EDSBF-MICS IV) 2010. 2012. Available online: https://dhsprogram.com/pubs/pdf/FR256/FR256.pdf (accessed on 21 October 2019).
- Institut National de la Statistique et de la Démographie. Rapport de L’enquête Nationale sur les Indicateurs du Paludisme 2017–2018. Available online: http://www.insd.bf/n/contenu/enquetes_recensements/enquete_palu/EIPBF_2018.pdf (accessed on 21 October 2019).
- Ministère de la Santé. Entrepôt de Données Sanitaires du Burkina Faso -Endos-BF, Burkina Faso 2013. Available online: https://burkina.dhis2.org/dhis/dhis-web-commons/security/login.action2013 (accessed on 21 October 2019).
- Ministère de la Santé. Rapport D’évaluation du Système de Gestion et de la Qualité des Données de Routine du SNIS; Direction Générale des Etudes et des Statistique Sectorielle: Ouagadougou, Burkina Faso, 2018. [Google Scholar]
- Institut national de la Statistique et de la Démographie. Rapport de L’enquête Nationale sur les Indicateurs du Paludisme. 2014. Available online: http://www.cns.bf/IMG/pdf/mis19.pdf (accessed on 21 November 2019).
- Ministère de la Santé/Direction Générale des Etudes et des Statistiques Sectorielles. Enquête Nationale sur les Prestations des Services de Santé et la Qualité des Données Sanitaires. 2012. Available online: http://apps.who.int/healthinfo/systems/datacatalog/index.php/catalog/50/reports (accessed on 21 November 2019).
- Rytter, M.J.; Kolte, L.; Briend, A.; Friis, H.; Christensen, V.B. The immune system in children with malnutrition--a systematic review. PLoS ONE 2014, 9, e105017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chotsiri, P.; Denoeud-Ndam, L.; Baudin, E.; Guindo, O.; Diawara, H.; Attaher, O.; Smit, M.; Guerin, P.J.; Doumbo, O.K.; Wiesner, L.; et al. Severe Acute Malnutrition Results in Lower Lumefantrine Exposure in Children Treated With Artemether-Lumefantrine for Uncomplicated Malaria. Clin. Pharmacol. Ther. 2019, 106, 1299–1309. [Google Scholar] [CrossRef] [PubMed]
- Rice, A.L.; Sacco, L.; Hyder, A.; Black, R.E. Malnutrition as an underlying cause of childhood deaths associated with infectious diseases in developing countries. Bull. World Health Organ. 2000, 78, 1207–1221. [Google Scholar] [PubMed]
- UNHCR. Acute Malnutrition Threshold. UNHCR Emergency Handbook 2020. Available online: https://emergency.unhcr.org/entry/32604/acute-malnutrition-threshold (accessed on 22 January 2020).
- Ministère de la Santé. Annuaire Statistique 2013. Available online: http://www.cns.bf/IMG/pdf/annuaire_sante_2013.pdf (accessed on 21 November 2019).
- Ministère de la Santé. Annuaire Statistique 2014. Available online: http://www.cns.bf/IMG/pdf/annuaire_2014_du_ms.pdf (accessed on 21 November 2019).
- Ministère de la Santé. Annuaire Statistique 2015. Available online: http://www.cns.bf/IMG/pdf/annuaire_ms_2015_signe.pdf (accessed on 21 November 2019).
- Nkollo, B.; Claude, W. (Eds.) La nécessité d’une Gestion Optimale des Ressources Humaines. In Proceedings of the Conférence Régionale sur la Crise des Ressources Humaines en Santé en Afrique Subsaharienne, Douala, Cameroon, June 2007; Available online: https://www.who.int/workforcealliance/Cameroun.pdf (accessed on 21 November 2019).
- Ministère de la Santé. Métadonnées des Indicateurs du Système National D’information Sanitaire (SNIS). 2015. Available online: http://www.cns.bf/IMG/Metadonnees/Meta_donnees_SNIS.pdf (accessed on 21 November 2019).
- McCullagh, P.; Nelder, J. Generalized Linear Models; Monographs on Statistics and Applied Probability 37; Chapman and Hall: London, UK, 1989. [Google Scholar]
- Lawson, A.B. Bayesian Disease Mapping: Hierarchical Modeling in Spatial Epidemiology; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Gelman, A. Prior distributions for variance parameters in hierarchical models (comment on article by Browne and Draper). Math. Stat. Online 2006, 1, 515–534. [Google Scholar] [CrossRef]
- Richardson, S.; Thomson, A.; Best, N.; Elliott, P. Interpreting posterior relative risk estimates in disease-mapping studies. Environ. Health Perspect. 2004, 112, 1016–1025. [Google Scholar] [CrossRef]
- Quantum Gis, Development Team. QGIS Geographic Information System, Version 2.18. 2017. Available online: https://qgis.org/en/site/forusers/download.html (accessed on 21 October 2019).
- Dolan, C.B.; BenYishay, A.; Grépin, K.A.; Tanner, J.C.; Kimmel, A.D.; Wheeler, D.C.; McCord, G.C. The impact of an insecticide treated bednet campaign on all-cause child mortality: A geospatial impact evaluation from the Democratic Republic of Congo. PLoS ONE 2019, 14, e0212890. [Google Scholar] [CrossRef]
- Valle, D.; Millar, J.; Amratia, P. Spatial heterogeneity can undermine the effectiveness of country-wide test and treat policy for malaria: A case study from Burkina Faso. Malar. J. 2016, 15, 513. [Google Scholar] [CrossRef] [Green Version]
- Gething, P.W.; Casey, D.C.; Weiss, D.J.; Bisanzio, D.; Bhatt, S.; Cameron, E.; Battle, K.E.; Dalrymple, U.; Rozier, J.; Rao, P.C.; et al. Mapping Plasmodium falciparum Mortality in Africa between 1990 and 2015. N. Engl. J. Med. 2016, 375, 2435–2445. [Google Scholar] [CrossRef] [Green Version]
- Zurovac, D.; Githinji, S.; Memusi, D.; Kigen, S.; Machini, B.; Muturi, A.; Otieno, G.; Snow, R.W.; Nyandigisi, A. Major improvements in the quality of malaria case-management under the “test and treat” policy in Kenya. PLoS ONE 2014, 9, e92782. [Google Scholar] [CrossRef]
- O’Meara, W.P.; Mangeni, J.N.; Steketee, R.; Greenwood, B. Changes in the burden of malaria in sub-Saharan Africa. Lancet Infect. Dis. 2010, 10, 545–555. [Google Scholar] [CrossRef]
- Fatungase, K.O.; Amoran, O.E.; Alausa, K.O. The effect of health education intervention on the home management of malaria among the caregivers of children aged under 5 years in Ogun State, Nigeria. Eur. J. Med. Res. 2012, 17, 11. [Google Scholar] [CrossRef] [Green Version]
- Kenangalem, E.; Poespoprodjo, J.R.; Douglas, N.M.; Burdam, F.H.; Gdeumana, K.; Chalfein, F.; Prayoga; Thio, F.; Devine, A.; Martfurt, J.; et al. Malaria morbidity and mortality following introduction of a universal policy of artemisinin-based treatment for malaria in Papua, Indonesia: A longitudinal surveillance study. PLoS Med. 2019, 16, e1002815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkwenti, H.E.; Ngowe, M.N.; Fokam, P.; Fonyuy, J.N.; Atanga, S.N.; Nkfusai, N.C.; Yankam, B.M.; Tsoka-Gwegweni, J.M.; Cumber, S.N. The effect of subsidized malaria treatment among under-five children in the Buea Health District, Cameroon. Pan Afr. Med. J. 2019, 33, 152. [Google Scholar] [CrossRef] [PubMed]
- Ridde, V.; Robert, E.; Meessen, B. A literature review of the disruptive effects of user fee exemption policies on health systems. BMC Public Health 2012, 12, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faye, O.; Correa, J.; Camara, B.; Dieng, T.; Dieng, Y.; Gaye, O.; Bah, I.B.; N’Dir, O.; Fall, M.; Diallo, S. Malaria lethality in Dakar pediatric environment: Study of risk factors. Med. Trop. 1998, 58, 361–364. [Google Scholar]
- Newton, C.R.; Taylor, T.E.; Whitten, R.O. Pathophysiology of fatal falciparum malaria in African children. Am. J. Trop. Med. Hyg. 1998, 58, 673–683. [Google Scholar] [CrossRef]
- Idro, R.; Marsh, K.; John, C.C.; Newton, C.R.J. Cerebral Malaria: Mechanisms of Brain Injury and Strategies for Improved Neurocognitive Outcome. Pediatric Res. 2010, 68, 267–274. [Google Scholar] [CrossRef]
- Sypniewska, P.; Duda, J.F.; Locatelli, I.; Althaus, C.R.; Althaus, F.; Genton, B. Clinical and laboratory predictors of death in African children with features of severe malaria: A systematic review and meta-analysis. BMC Med. 2017, 15, 147. [Google Scholar] [CrossRef] [Green Version]
- Conroy, A.L.; Hawkes, M.; Elphinstone, R.E.; Morgan, C.; Hermann, L.; Barker, K.R.; Namasopo, S.; Opoka, R.O.; John, C.C.; Liles, W.C.; et al. Acute Kidney Injury Is Common in Pediatric Severe Malaria and Is Associated with Increased Mortality. Open Forum Infect. Dis. 2016, 3, ofw046. [Google Scholar] [CrossRef] [Green Version]
- Berkley, J.; Mwarumba, S.; Bramham, K.; Lowe, B.; Marsh, K. Bacteraemia complicating severe malaria in children. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 283–286. [Google Scholar] [CrossRef] [Green Version]
- Church, J.; Maitland, K. Invasive bacterial co-infection in African children with Plasmodium falciparum malaria: A systematic review. BMC Med. 2014, 12, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagbo, G.G.; Alihonou, F.; Alao, M.J.; Tohodjèdé, Y.; Zohoun, L.; Bognon, G.; Agossou, J.; Noudamadjo, A.; Orou-Guidou, A. The Determinants of Fatal Outcomes during Severe Malaria in Children at the HKM University Teaching Hospital of Cotonou-Benin. J. Pediatrics 2017, 7, 245. [Google Scholar] [CrossRef] [Green Version]
- Camara, B.; Diagne, N.; Faye, P.; Fall, M.; Ndiaye, J.; Ba, M.; Sow, H.D. Critères de gravité et facteurs pronostiques du paludisme chez l’enfant à Dakar. Med. Mal. Infect. 2011, 41, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Pasvol, G. The treatment of complicated and severe malaria. Br. Med. Bull. 2005, 75, 29–47. [Google Scholar] [CrossRef] [Green Version]
- Mutombo, A.M.; Mukuku, O.; Tshibanda, K.N.; Swana, E.K.; Mukomena, E.; Ngwej, D.T.; Luboya, O.N.; Kakoma, J.B.; Wembonyama, S.O.; Geertruyden, J.P.V.; et al. Severe malaria and death risk factors among children under 5 years at Jason Sendwe Hospital in Democratic Republic of Congo. Pan Afr. Med. J. 2018, 29, 1–8. [Google Scholar] [CrossRef]
- Win Han, O.; Gold, L.; Moore, K.; Agius, P.A.; Fowkes, F.J.I. The impact of community-delivered models of malaria control and elimination: A systematic review. Malar. J. 2019, 18, 269. [Google Scholar] [CrossRef]
- Health Organization World. Global Technical Strategy for Malaria 2016–2030; Global Malaria Programme: Geneva, Switzerland, 2015; Available online: https://www.who.int/malaria/publications/atoz/9789241564991/en/ (accessed on 21 September 2019).
- Ministère de la Santé. Organigramme 2016. Available online: http://ilo.org/dyn/natlex/docs/ELECTRONIC/104132/126909/F1133913732/BFA-104132.pdf (accessed on 21 October 2019).
- Van Den Broeck, J.; Eeckels, R.; Vuylsteke, J. Influence of nutritional status on child mortality in rural Zaire. Lancet 1993, 341, 1491–1495. [Google Scholar] [CrossRef]
- Monjour, L.; Palminteri, R.; Froment, A.; Renault, T.; Alfred, C.; Gentilini, M.; Gouba, E. Is cell-mediated immune response related to nutritional state, but unaffected by concomitant malarial infection? Ann. Trop. Med. Parasitol. 1982, 76, 575–577. [Google Scholar] [CrossRef]
- Genton, B.; al-Yaman, F.; Alpers, M.P.; Mokela, D. Indicators of fatal outcome in paediatric cerebral malaria: A study of 134 comatose Papua New Guinean children. Int. J. Epidemiol. 1997, 26, 670–676. [Google Scholar] [CrossRef]
- Renaudin, P. Evaluation de l’état nutritionnel de l’enfant de moins de 5 ans à Moundou, Tchad: Relations avec la morbidité et la mortalité hospitalières. Med. Trop. 1997, 57, 49–54. [Google Scholar] [CrossRef]
- Hughes, S.; Kelly, P. Interactions of malnutrition and immune impairment, with specific reference to immunity against parasites. Parasite Immunol. 2006, 28, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Bourke, C.D.; Berkley, J.A.; Prendergast, A.J. Immune Dysfunction as a Cause and Consequence of Malnutrition. Trends Immunol. 2016, 37, 386–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, A.H. Nutritional modulation of malaria morbidity and mortality. J. Infect. Dis. 2000, 182 (Suppl. 1), S37–S53. [Google Scholar] [CrossRef]
- Murray, M.J.; Murray, A.B.; Murray, N.J.; Murray, M.B. Diet and cerebral malaria: The effect of famine and refeeding. Am. J. Clin. Nutr. 1978, 31, 57–61. [Google Scholar] [CrossRef]
- Murray, M.J.; Murray, A.B.; Murray, M.B.; Murray, C.J. Somali food shelters in the Ogaden famine and their impact on health. Lancet 1976, 1, 1283–1285. [Google Scholar] [CrossRef]
- Murray, M.J.; Murray, N.J.; Murray, A.B.; Murray, M.B. Refeeding-malaria and hyperferraemia. Lancet 1975, 1, 653–654. [Google Scholar] [CrossRef]
- Nacher, M.; Singhasivanon, P.; Treeprasertsuk, S.; Vannaphan, S.; Traore, B.; Looareesuwan, S.; Gay, F. Intestinal helminths and malnutrition are independently associated with protection from cerebral malaria in Thailand. Ann. Trop. Med. Parasitol. 2002, 96, 5–13. [Google Scholar] [CrossRef]
- Ferreira, E.; Alexandre, M.A.; Salinas, J.L.; de Siqueira, A.M.; Benzecry, S.G.; de Lacerda, M.V.; Monteiro, W.M. Association between anthropometry-based nutritional status and malaria: A systematic review of observational studies. Malar. J. 2015, 14, 346. [Google Scholar] [CrossRef] [Green Version]
- Mockenhaupt, F.P.; Ehrhardt, S.; Burkhardt, J.; Bosomtwe, S.Y.; Laryea, S.; Anemana, S.D.; Otchwemah, R.N.; Cramer, J.P.; Dietz, E.; Gellert, S.; et al. Manifestation and outcome of severe malaria in children in northern Ghana. Am. J. Trop. Med. Hyg. 2004, 71, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Orimadegun, A.E.; Fawole, O.; Okereke, J.O.; Akinbami, F.O.; Sodeinde, O. Increasing burden of childhood severe malaria in a Nigerian tertiary hospital: Implication for control. J. Trop. Pediatrics 2007, 53, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Von Seidlein, L.; Olaosebikan, R.; Hendriksen, I.C.; Lee, S.J.; Adedoyin, O.T.; Agbenyega, T.; Nguah, S.B.; Bojang, K.; Deen, J.L.; Evans, J.; et al. Predicting the clinical outcome of severe falciparum malaria in african children: Findings from a large randomized trial. Clin. Infect. Dis. 2012, 54, 1080–1090. [Google Scholar] [CrossRef]
- Olumese, P.E.; Sodeinde, O.; Ademowo, O.G.; Walker, O. Protein energy malnutrition and cerebral malaria in Nigerian children. J. Trop. Pediatrics 1997, 43, 217–219. [Google Scholar] [CrossRef]
- Kendjo, E.; Agbenyega, T.; Bojang, K.; Newton, C.R.; Bouyou-Akotet, M.; Pedross, F.; Kombila, M.; Helbok, R.; Kremsner, P.G. Mortality patterns and site heterogeneity of severe malaria in African children. PLoS ONE 2013, 8, e58686. [Google Scholar] [CrossRef]
- Jenkins, R.; Omollo, R.; Ongecha, M.; Sifuna, P.; Othieno, C.; Ongeri, L.; Kingora, J.; Ogutu, B. Prevalence of malaria parasites in adults and its determinants in malaria endemic area of Kisumu County, Kenya. Malar. J. 2015, 14, 263. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictor | Adjusted IRR (95% BCI) |
|---|---|
| Free of charge health care | |
| No | 1 |
| Yes | 0.47 (0.38, 0.58) |
| Availability of mRDT a | 0.54 (0.47, 0.62) |
| Availability of treatment a | 0.50 (0.41, 0.61) |
| Use ACT for treatment a | 0.54 (0.47, 0.62) |
| Global acute malnutrition | |
| <10% | 1 |
| ≥10% | 1.06 (0.99, 1.13) |
| Distance (km) b | |
| <5 | 1 |
| ≥5 | 1.12(1.03, 1.22) |
| Population nurse ratio | |
| <5000 | 1 |
| ≥5000 | 1.07 (0.99, 1.15) |
| Spatial variance | Mean [95% BCI] |
| Non-structural Variance | 1.036 (1.035, 1.037) |
| Structural Variance | 1.028 (1.027, 1.029) |
| Temporal variance | Mean [95% BCI] |
| Structural variance | 1.209 (1.063, 1.955) |
| Interaction variance | 1.170 (1.169, 1.172) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouédraogo, M.; Kangoye, D.T.; Samadoulougou, S.; Rouamba, T.; Donnen, P.; Kirakoya-Samadoulougou, F. Malaria Case Fatality Rate among Children under Five in Burkina Faso: An Assessment of the Spatiotemporal Trends Following the Implementation of Control Programs. Int. J. Environ. Res. Public Health 2020, 17, 1840. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061840
Ouédraogo M, Kangoye DT, Samadoulougou S, Rouamba T, Donnen P, Kirakoya-Samadoulougou F. Malaria Case Fatality Rate among Children under Five in Burkina Faso: An Assessment of the Spatiotemporal Trends Following the Implementation of Control Programs. International Journal of Environmental Research and Public Health. 2020; 17(6):1840. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061840
Chicago/Turabian StyleOuédraogo, Mady, David Tiga Kangoye, Sékou Samadoulougou, Toussaint Rouamba, Philippe Donnen, and Fati Kirakoya-Samadoulougou. 2020. "Malaria Case Fatality Rate among Children under Five in Burkina Faso: An Assessment of the Spatiotemporal Trends Following the Implementation of Control Programs" International Journal of Environmental Research and Public Health 17, no. 6: 1840. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061840