The Risk of Depression in Patients with Pemphigus: A Nationwide Cohort Study in Taiwan


Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Subject Selection
2.3. Statistical Analysis
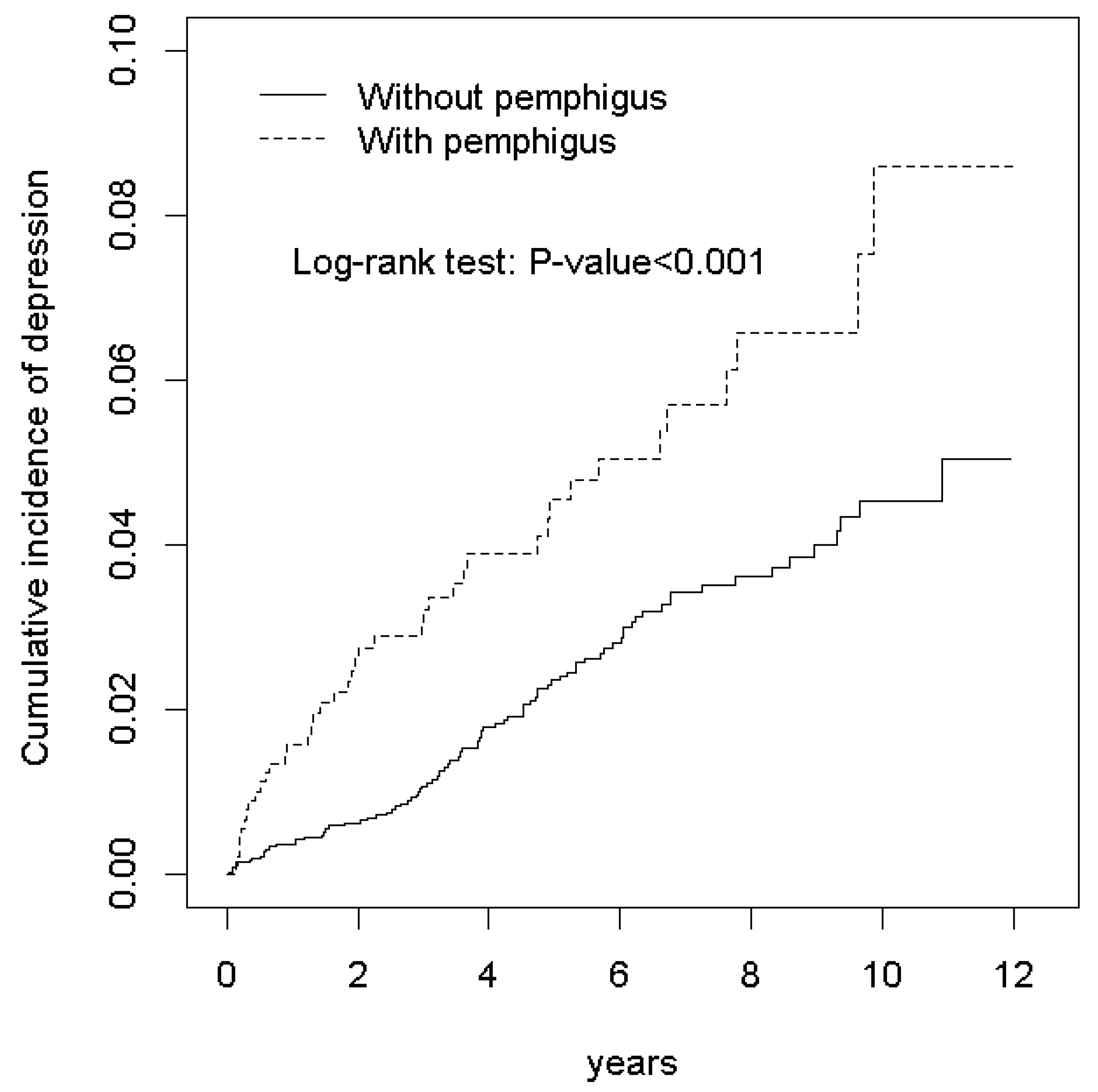
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hietanen, J.; Salo, O.P. Pemphigus: An epidemiological study of patients treated in Finnish hospitals between 1969 and 1978. Acta Derm. Venereol 1982, 62, 491–496. [Google Scholar]
- Pisanti, S.; Sharav, Y.; Kaufman, E.; Posner, L. Pemphigus vulgaris: Incidence in Jews of different ethnic groups, according to age, sex, and initial lesion. Oral Surgery Oral Med. Oral Pathol. 1974, 38, 382–387. [Google Scholar] [CrossRef]
- Langan, S.; Smeeth, L.; Hubbard, R.; Fleming, K.; Smith, C.J.P.; West, J. Bullous pemphigoid and pemphigus vulgaris—Incidence and mortality in the UK: Population based cohort study. BMJ 2008, 337, 160–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chee, S.-N.; Murrell, D.F. Pemphigus and Quality of Life. Dermatol. Clin. 2011, 29, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Wohl, Y.; Mashiah, J.; Kutz, A.; Hadj-Rabia, S.; Cohen, A.D. Pemphigus and depression comorbidity: A case control study. Eur. J. Dermatol. EJD 2015, 25, 602–605. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.S.-T.; Lee, C.-S.; Gunnell, D.; Lee, W.-C.; Cheng, A.T.-A. Changing trends in the prevalence of common mental disorders in Taiwan: A 20-year repeated cross-sectional survey. Lancet 2013, 381, 235–241. [Google Scholar] [CrossRef]
- Aamir, S. Co-morbid anxiety and depression among pulmonary tuberculosis patients. J. Coll. Physicians Surg. Pak. 2010, 20, 703–704. [Google Scholar]
- Iessa, N.; Murray, M.; Curran, S.; Wong, I.C.K. Asthma and suicide-related adverse events: A review of observational studies. Eur. Respir. Rev. 2011, 20, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Moser, D.K.; Dracup, K.; Evangelista, L.; Zambroski, C.H.; Lennie, T.A.; Chung, M.L.; Doering, L.V.; Westlake, C.; Heo, S. Comparison of prevalence of symptoms of depression, anxiety, and hostility in elderly patients with heart failure, myocardial infarction, and a coronary artery bypass graft. Heart Lung 2010, 39, 378–385. [Google Scholar] [CrossRef] [Green Version]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef]
- Dixon, L.J.; Lee, A.A.; Viana, A.G.; McCowan, N.K.; Brodell, R.T.; Tull, M.T. Anxiety Sensitivity in Dermatological Patients. Psychosomatics 2016, 57, 498–504. [Google Scholar] [CrossRef] [PubMed]
- A Gupta, M.; Gupta, A.; Schork, N.J.; Ellis, C.N. Depression modulates pruritus perception: A study of pruritus in psoriasis, atopic dermatitis, and chronic idiopathic urticaria. Psychosom. Med. 1994, 56, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Dalgard, F.J.; Svensson, Å.; Gieler, U.; Tomas-Aragones, L.; Lien, L.; Poot, F.; Jemec, G.B.E.; Misery, L.; Szabo, C.; Linder, D.; et al. Dermatologists across Europe underestimate depression and anxiety: Results from 3635 dermatological consultations. Br. J. Dermatol. 2018, 179, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Mahdanian, A.; Shalileh, K.; Ashrafinia, N.; Arbabi, M.; Ghodsi, Z.; Noormohammadi, N.; Darvish, F.; Chams, C. Mental health in patients with pemphigus: An issue to worth consideration. Indian J. Dermatol. 2011, 56, 541–545. [Google Scholar] [CrossRef]
- Kayani, M.; Aslam, A. Bullous pemphigoid and pemphigus vulgaris. BMJ 2017, 357, j2169. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.J.; Lee, H.E.; Chang, C.H.; Chen, C.B. IgG/IgA Pemphigus Presenting with Mixed Clinical Features of Pemphigus Erythematosus and IgA Pemphigus. Dermatol. Sin. 2019, 37, 226–228. [Google Scholar]
- Ivars, M.; Espana, A.; Alzuguren, P.; Pelacho, B.; Lasarte, J.J.; Lopez-Zabalza, M.J. The involvement of ADAM10 in mucocutaneous pemphigus vulgaris acantholysis depends on the autoantibody profile in each patient. Br. J. Dermatol. 2019. [Google Scholar] [CrossRef]
- Paolino, G.; Didona, D.; Magliulo, G.; Iannella, G.; Didona, B.; Mercuri, S.R.; Moliterni, E.; Donati, M.; Ciofalo, A.; Granata, M.; et al. Paraneoplastic Pemphigus: Insight into the Autoimmune Pathogenesis, Clinical Features and Therapy. Int. J. Mol. Sci. 2017, 18, 2532. [Google Scholar] [CrossRef] [Green Version]
- Kasperkiewicz, M.; Ellebrecht, C.T.; Takahashi, H.; Yamagami, J.; Zillikens, D.; Payne, A.S.; Amagai, M. Pemphigus. Nat. Rev. Dis. Primers 2017, 3, 17026. [Google Scholar] [CrossRef] [Green Version]
- Tavakolpour, S. Current and future treatment options for pemphigus: Is it time to move towards more effective treatments? Int. Immunopharmacol. 2017, 53, 133–142. [Google Scholar] [CrossRef]
- Hughes, J.E.; Barraclough, B.M.; Hamblin, L.G.; White, J.E. Psychiatric Symptoms in Dermatology Patients. Br. J. Psychiatry 1983, 143, 51–54. [Google Scholar] [CrossRef]
- Johnson, F.Y.A.; Mostaghimi, H. Co-morbidity between dermatologic diseases and psychiatric disorders in Papua New Guinea. Int. J. Dermatol. 1995, 34, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.E.; Martires, K.J.; Ho, R.S.; Cohen, B.B.E. Psoriasis and the Risk of Depression in the US Population. JAMA Dermatol. 2016, 152, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallerand, I.A.; Lewinson, R.T.; Parsons, L.; Hardin, J.; Haber, R.M.; Lowerison, M.W.; Barnabe, C.; Patten, S.B. Assessment of a Bidirectional Association Between Major Depressive Disorder and Alopecia Areata. JAMA Dermatol. 2019, 155, 475. [Google Scholar] [CrossRef]
- Silverberg, J. Comorbidities and the impact of atopic dermatitis. Ann. Allergy Asthma Immunol. 2019, 123, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.V.; Murrell, D.F. Psychosocial impact of inherited and autoimmune blistering diseases. Int. J. Women’s Dermatol. 2018, 4, 49–53. [Google Scholar] [CrossRef]
- Gudi, V.; White, M.; Cruickshank, N.; Herriot, R.; Edwards, S.; Nimmo, F.; Ormerod, A. Annual incidence and mortality of bullous pemphigoid in the Grampian Region of North-east Scotland. Br. J. Dermatol. 2005, 153, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Ghodsi, S.Z.; Chams-Davatchi, C.; Daneshpazhooh, M.; Valikhani, M.; Esmaili, N. Quality of life and psychological status of patients with pemphigus vulgaris using Dermatology Life Quality Index and General Health Questionnaires. J. Dermatol. 2011, 39, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Paradisi, A.; Sampogna, F.; Di Pietro, C.; Cianchini, G.; Didona, B.; Ferri, R.; Abeni, D.; Tabolli, S. Quality-of-life assessment in patients with pemphigus using a minimum set of evaluation tools. J. Am. Acad. Dermatol. 2009, 60, 261–269. [Google Scholar] [CrossRef]
- Stetler, C.A.; Miller, G.E. Depression and Hypothalamic-Pituitary-Adrenal Activation: A Quantitative Summary of Four Decades of Research. Psychosom. Med. 2011, 73, 114–126. [Google Scholar] [CrossRef]
- Shao, C.-C.; Chang, C.-P.; Chou, L.-F.; Chen, T.-J.; Hwang, S.-J. The ecology of medical care in Taiwan. J. Chin. Med. Assoc. 2011, 74, 408–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Pemphigus | p-Value | |
|---|---|---|---|
| No | Yes | ||
| N = 3674 | N = 926 | ||
| n (%) | n (%) | ||
| Age group (year) | 0.92 | ||
| 20−49 | 1768 (48.1) | 442 (47.7) | |
| 50−64 | 1012 (27.6) | 253 (27.3) | |
| ≥65 | 894 (24.3) | 231 (25.0) | |
| Age, mean ± SD a (year) | 52.6 ± 16.5 | 52.9 ± 16.6 | 0.58 |
| Sex | 0.97 | ||
| Women | 1956 (53.2) | 493 (53.2) | |
| Men | 1718 (46.8) | 433 (46.8) | |
| Monthly income b | 0.99 | ||
| <15,000 | 819 (22.3) | 206 (22.3) | |
| 15,000−19,999 | 1663 (45.3) | 418 (45.1) | |
| ≥20,000 | 1192 (32.4) | 302 (32.6) | |
| Urbanization level c | 0.99 | ||
| 1 (highest) | 1197 (32.6) | 302 (32.6) | |
| 2 | 1141 (31.1) | 288 (31.1) | |
| 3 | 592 (16.1) | 149 (16.1) | |
| 4 (lowest) | 744 (20.3) | 187 (20.2) | |
| Occupation d | 0.99 | ||
| Office worker | 2058 (56.0) | 519 (56.1) | |
| Laborer | 1291 (35.1) | 325 (35.1) | |
| Other | 325 (8.85) | 82 (8.86) | |
| Comorbidity | |||
| HTN | 204 (5.55) | 282 (30.5) | <0.001 |
| DM | 75 (2.04) | 93 (10.0) | <0.001 |
| HL | 100 (2.72) | 180 (19.4) | <0.001 |
| Asthma/COPD | 143 (3.89) | 82 (8.86) | <0.001 |
| CLD | 642 (17.5) | 163 (17.6) | 0.93 |
| CKD | 58 (1.58) | 14 (1.51) | 0.88 |
| Cancer | 91 (2.48) | 24 (2.59) | 0.84 |
| Medicines | |||
| Steroids | 3404 (92.7) | 926 (100.0) | <0.001 |
| Azathioprin | 3 (0.08) | 423 (45.7) | <0.001 |
| Event | PY | Rate # | Crude HR (95% CI) | Adjusted HR & (95% CI) | |
|---|---|---|---|---|---|
| Pemphigus | |||||
| No | 91 | 20,282 | 4.49 | 1.00 | 1.00 |
| Yes | 41 | 4606 | 8.90 | 1.98 (1.37, 2.86) *** | 1.99 (1.32, 3.00) ** |
| Age, year | |||||
| 20−49 | 63 | 12,921 | 4.88 | 1.00 | 1.00 |
| 50−64 | 25 | 6656 | 3.76 | 0.77 (0.48, 1.22) | 0.71 (0.45, 1.14) |
| ≥65 | 44 | 5311 | 8.28 | 1.69 (1.15, 2.49) ** | 1.42 (0.92, 2.21) |
| Gender | |||||
| Women | 78 | 13,893 | 5.61 | 1.00 | |
| Men | 54 | 10,995 | 4.91 | 0.87 (0.62, 1.23) | |
| Monthly income a | |||||
| <15,000 | 42 | 5408 | 7.77 | 2.05 (1.29, 3.24) ** | 1.81 (1.07, 3.06) * |
| 15,000−19,999 | 58 | 11,028 | 5.26 | 1.39 (0.90, 2.14) | 1.17 (0.71, 1.93) |
| ≥20,000 | 32 | 8452 | 3.79 | 1.00 | 1.00 |
| Urbanization level b | |||||
| 1 (highest) | 47 | 8435 | 5.57 | 1.00 | |
| 2 | 38 | 7570 | 5.02 | 0.90 (0.59, 1.38) | |
| 3 | 18 | 3871 | 4.65 | 0.83 (0.48, 1.44) | |
| 4 (lowest) | 29 | 5013 | 5.79 | 1.04 (0.65, 1.65) | |
| Occupation c | |||||
| Office worker | 66 | 14,034 | 4.70 | 1.00 | 1.00 |
| Laborer | 48 | 8594 | 5.59 | 1.19 (0.82, 1.72) | 1.21 (0.76, 1.93) |
| Other | 18 | 2260 | 7.97 | 1.69 (1.01, 2.85) * | 1.10 (0.61, 1.98) |
| Comorbidity | |||||
| HTN | |||||
| No | 114 | 22,817 | 5.00 | 1.00 | 1.00 |
| Yes | 18 | 2071 | 8.69 | 1.73 (1.05, 2.85) * | 0.75 (0.41, 1.42) |
| DM | |||||
| No | 126 | 24,163 | 5.21 | 1.00 | 1.00 |
| Yes | 6 | 725 | 8.27 | 1.59 (0.70, 3.58) | |
| HL | |||||
| No | 117 | 23,580 | 4.96 | 1.00 | 1.00 |
| Yes | 15 | 1308 | 11.5 | 2.30 (1.34, 3.94) ** | 1.48 (0.78, 2.82) |
| Asthma/COPD | |||||
| No | 121 | 23,912 | 5.06 | 1.00 | 1.00 |
| Yes | 11 | 976 | 11.3 | 2.20 (1.19, 4.09) * | 1.40 (0.72, 2.69) |
| CLD | |||||
| No | 99 | 20,806 | 4.76 | 1.00 | 1.00 |
| Yes | 33 | 4082 | 8.08 | 1.69 (1.14, 2.51) ** | 1.61 (1.07, 2.43) * |
| CKD | |||||
| No | 130 | 24,611 | 5.28 | 1.00 | 1.00 |
| Yes | 2 | 277 | 7.21 | 1.36 (0.34, 5.51) | |
| Cancer | |||||
| No | 129 | 24,456 | 5.27 | 1.00 | 1.00 |
| Yes | 3 | 432 | 6.95 | 1.30 (0.41, 4.08) | |
| Medicines Steroids | |||||
| No | 3 | 1313 | 2.28 | 1.00 | 1.00 |
| Yes | 129 | 23,575 | 5.47 | 2.39 (0.76, 7.50) | |
| Azathioprin | |||||
| No | 115 | 22,784 | 5.05 | 1.00 | 1.00 |
| Yes | 17 | 2104 | 8.08 | 1.60 (0.96, 2.67) |
| Pemphigus | ||||||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | |||||||
| Event | PY | Rate a | Event | PY | Rate a | Crude HR (95% CI) | Adjusted HR b (95% CI) | |
| Age group | ||||||||
| 20−49 | 42 | 10,411 | 4.03 | 21 | 2510 | 8.37 | 2.07 (1.23, 3.49) ** | 1.86 (1.06, 3.26) * |
| 50−64 | 16 | 5405 | 2.96 | 9 | 1251 | 7.20 | 2.41 (1.06, 5.45) * | 1.98 (0.75, 5.26) |
| ≥65 | 33 | 4466 | 7.39 | 11 | 845 | 13.0 | 1.75 (0.88, 3.47) | 1.709 (0.75, 3.87) |
| Sex | ||||||||
| Female | 53 | 11,264 | 4.71 | 25 | 2629 | 9.51 | 2.02 (1.26, 3.25) ** | 2.09 (1.24, 3.54) ** |
| Male | 38 | 9018 | 4.21 | 16 | 1977 | 8.09 | 1.91 (1.07, 3.43) * | 1.87 (0.97, 3.60) |
| Monthly income c | ||||||||
| <15,000 | 28 | 4484 | 6.24 | 14 | 925 | 15.1 | 2.42 (1.27, 4.60) ** | 2.28 (1.14, 4.58) * |
| 15,000−19,999 | 42 | 8987 | 4.67 | 16 | 2041 | 7.84 | 1.68 (0.94, 2.99) | 1.57 (0.81, 3.04) |
| ≥20,000 | 21 | 6811 | 3.08 | 11 | 1640 | 6.71 | 2.16 (1.04, 4.49) * | 2.29 (1.03, 5.10) * |
| Urbanization level d | ||||||||
| 1 (highest) | 33 | 6846 | 4.82 | 14 | 1589 | 8.81 | 1.81 (0.97, 3.38) | 2.04 (1.05, 3.94) * |
| 2 | 24 | 6167 | 3.89 | 14 | 1403 | 9.98 | 2.59 (1.34, 5.01) ** | 1.73 (0.79, 3.76) |
| 3 | 13 | 3160 | 4.11 | 5 | 711 | 7.04 | 1.69 (0.60, 4.73) | 1.85 (0.62, 5.52) |
| 4 (lowest) | 21 | 4109 | 5.11 | 8 | 903 | 8.86 | 1.70 (0.75, 3.83) | 2.29 (0.90, 5.81) |
| Occupation category e | ||||||||
| Office worker | 42 | 11,441 | 3.67 | 24 | 2593 | 9.25 | 2.53 (1.53, 4.17) *** | 2.49 (1.41, 4.39) ** |
| Laborer | 36 | 6998 | 5.14 | 12 | 1596 | 7.52 | 1.46 (0.76, 2.81) | 1.38 (0.66, 2.88) |
| Other | 13 | 1843 | 7.05 | 5 | 417 | 12.0 | 1.71 (0.61, 4.80) | 1.68 (0.55, 5.09) |
| Comorbidity f | ||||||||
| No | 61 | 15,770 | 3.87 | 20 | 2765 | 7.23 | 1.87 (1.13, 3.11) * | 2.13 (1.28, 3.57) ** |
| Yes | 30 | 4512 | 6.65 | 21 | 1841 | 11.4 | 1.709 (0.97, 2.97) | 1.73 (0.99, 3.03) |
| Follow-up | ||||||||
| <6 months | 7 | 1825 | 3.83 | 9 | 447 | 20.1 | 5.23 (1.95, 14.0) ** | 4.33 (1.42, 13.2) * |
| ≥6 months | 84 | 18,457 | 4.55 | 32 | 4159 | 7.69 | 1.69 (1.13, 2.54) * | 1.76 (1.121, 2.75) * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, Y.-M.; Fang, H.-Y.; Lin, C.-L.; Shieh, S.-H. The Risk of Depression in Patients with Pemphigus: A Nationwide Cohort Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 1983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061983
Hsu Y-M, Fang H-Y, Lin C-L, Shieh S-H. The Risk of Depression in Patients with Pemphigus: A Nationwide Cohort Study in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(6):1983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061983
Chicago/Turabian StyleHsu, Yi-Min, Hsin-Yu Fang, Cheng-Li Lin, and Shwn-Huey Shieh. 2020. "The Risk of Depression in Patients with Pemphigus: A Nationwide Cohort Study in Taiwan" International Journal of Environmental Research and Public Health 17, no. 6: 1983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061983