Effectiveness of Mobile Applications Running on Smartphones to Promote Physical Activity: A Systematic Review with Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Selection of Studies and Data Extraction
2.4. Risk of Bias and Quality Assessment in the Included Studies
2.5. Data Synthesis and Analysis
2.6. Risk of Bias Across Studies
3. Results
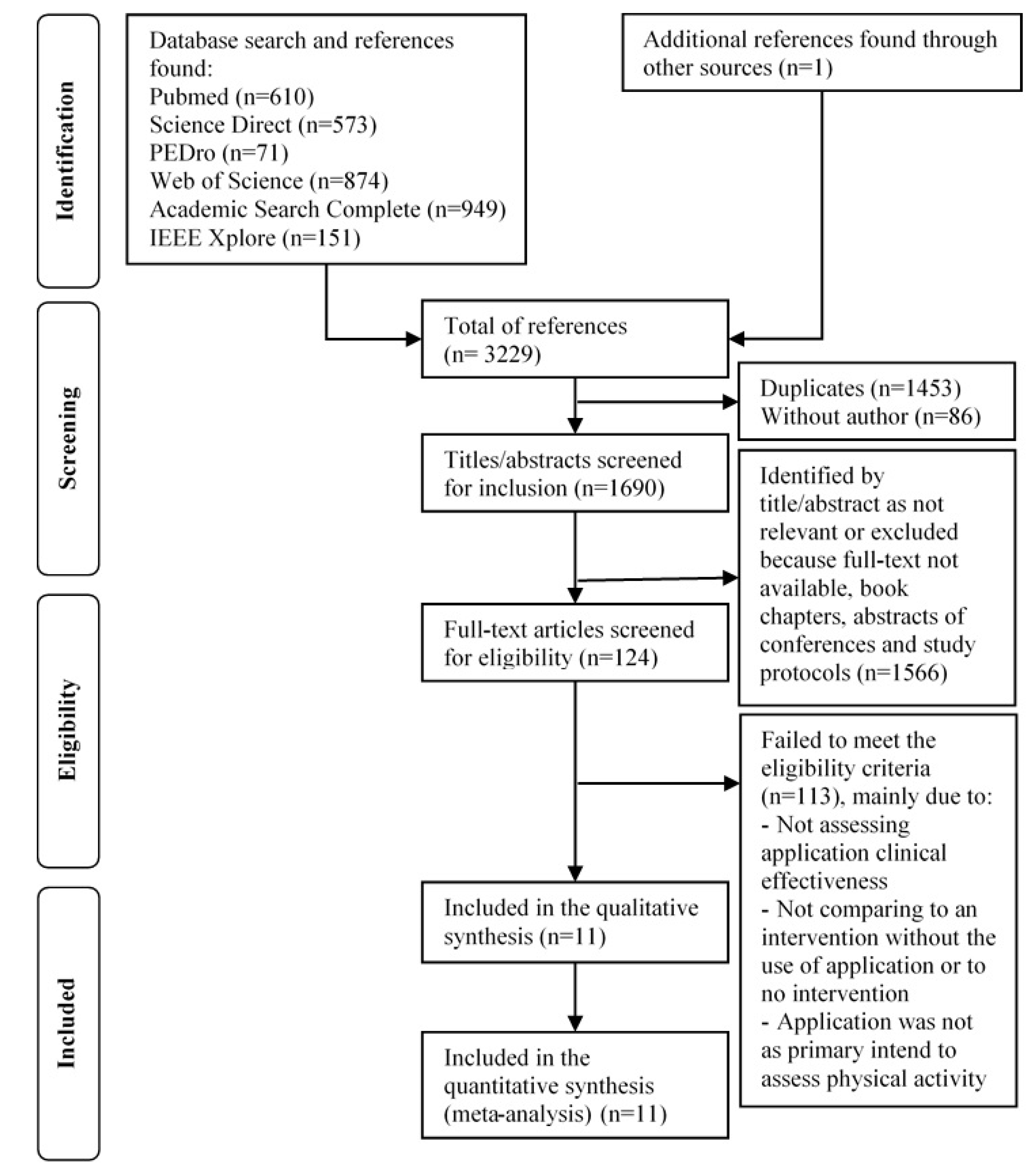
3.1. Study Selection
3.2. Description of the Included Studies
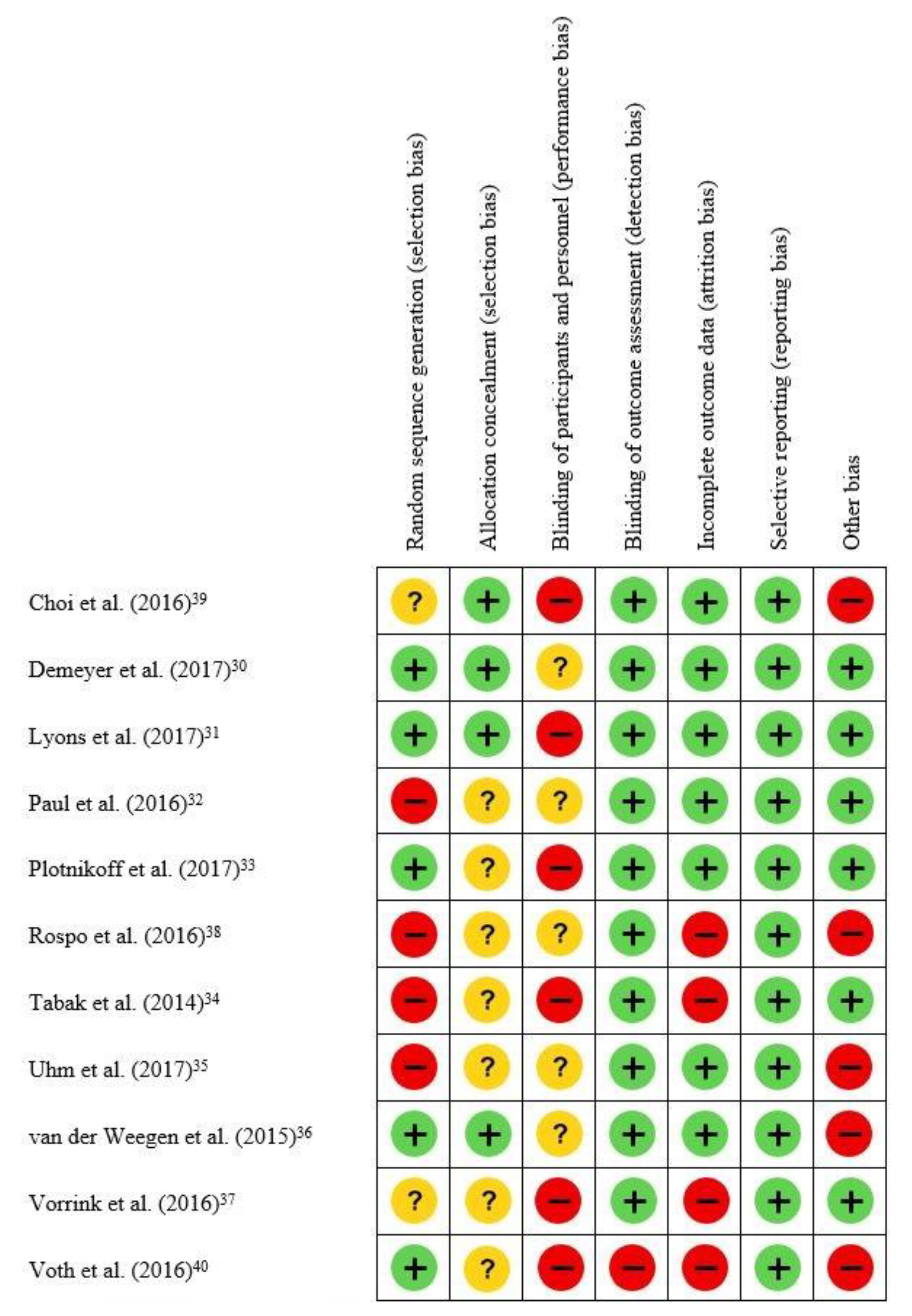
3.3. Risk of Bias of Included Studies and Quality of Evidence
3.4. Primary Outcome: Physical activity
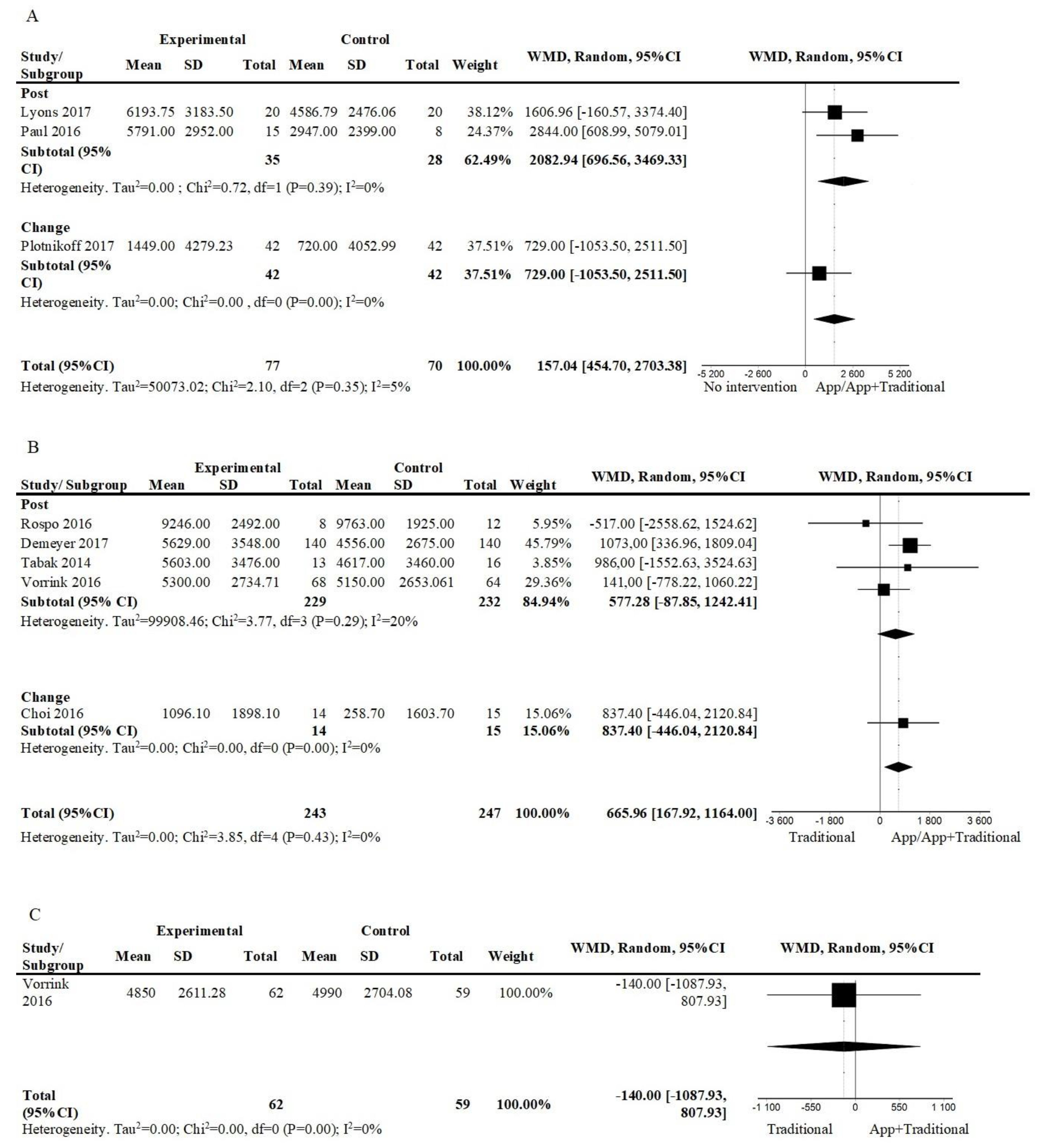
3.4.1. Number of Steps
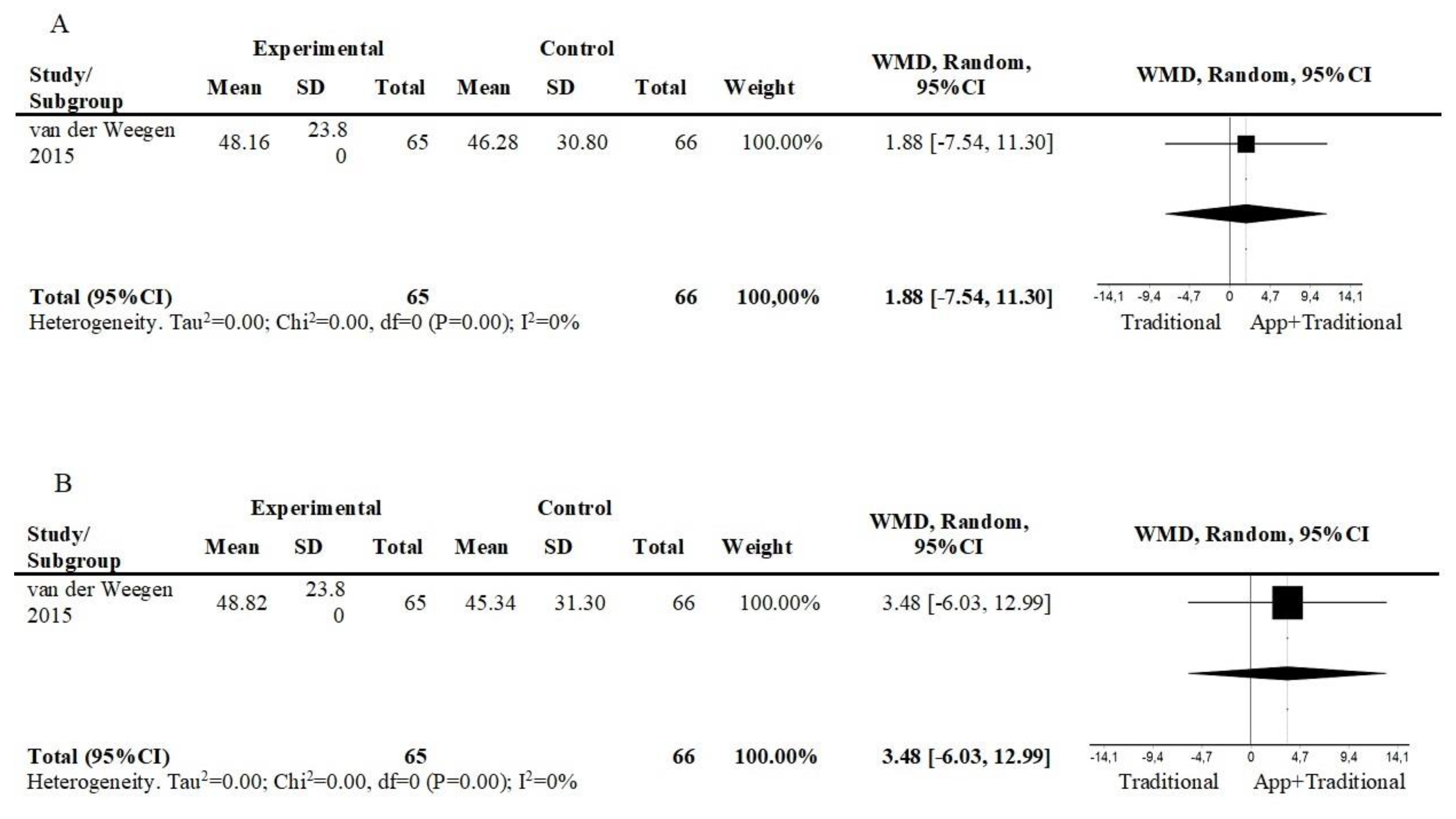
3.4.2. Minutes in Moderate to Vigorous Physical Activity
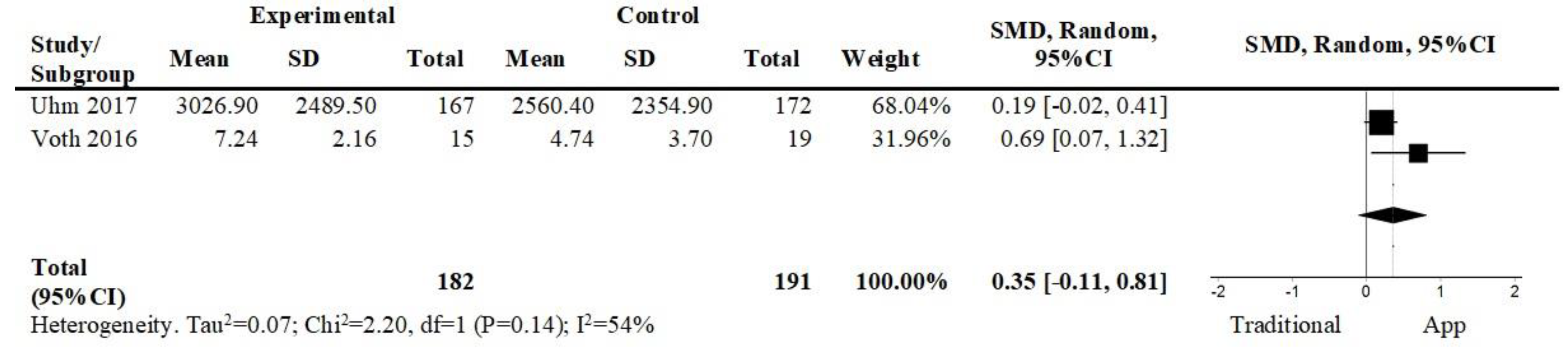
3.4.3. Self-Reported Physical Activity
3.5. Secondary Outcomes
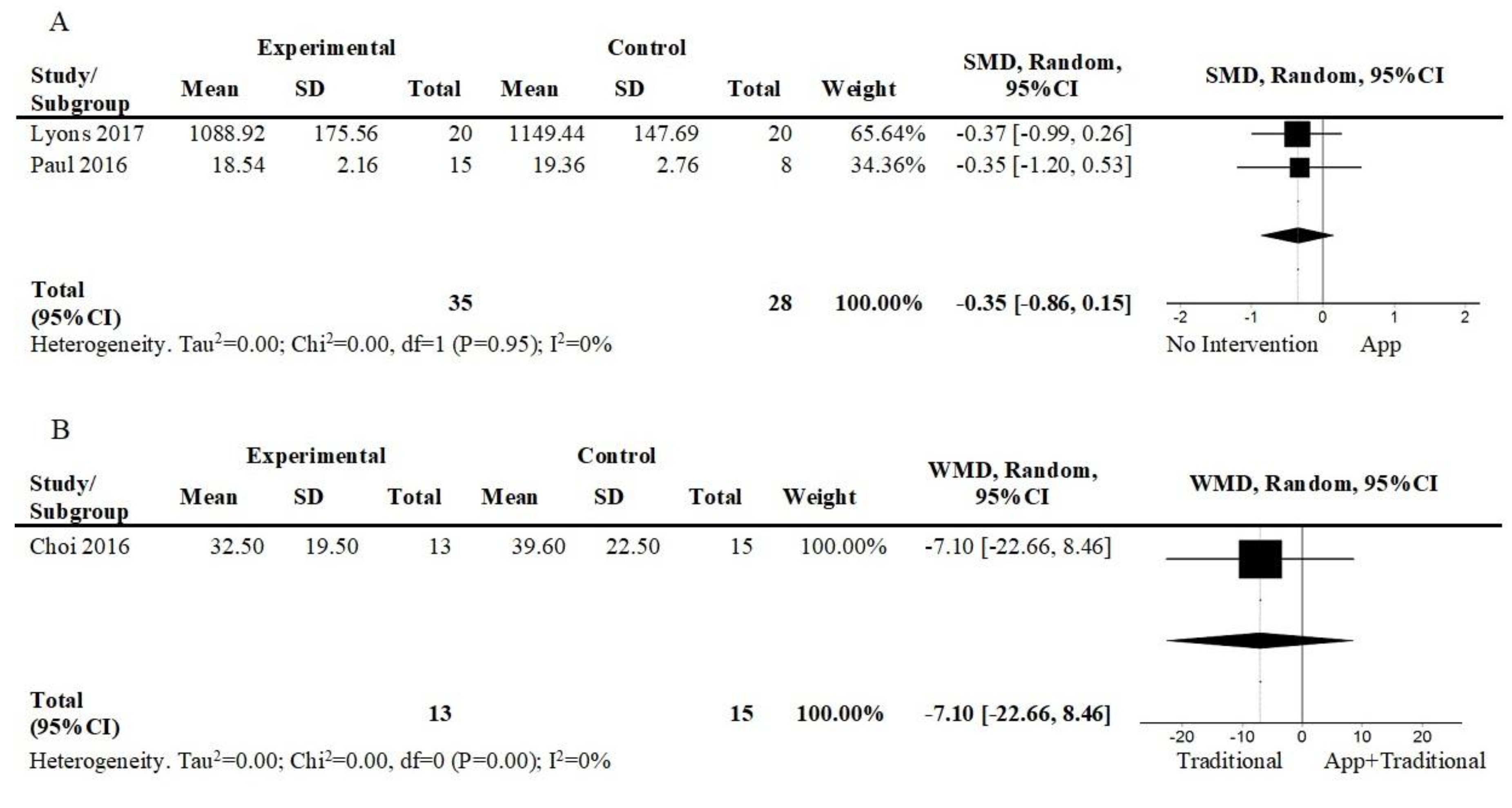
3.5.1. Sedentarism
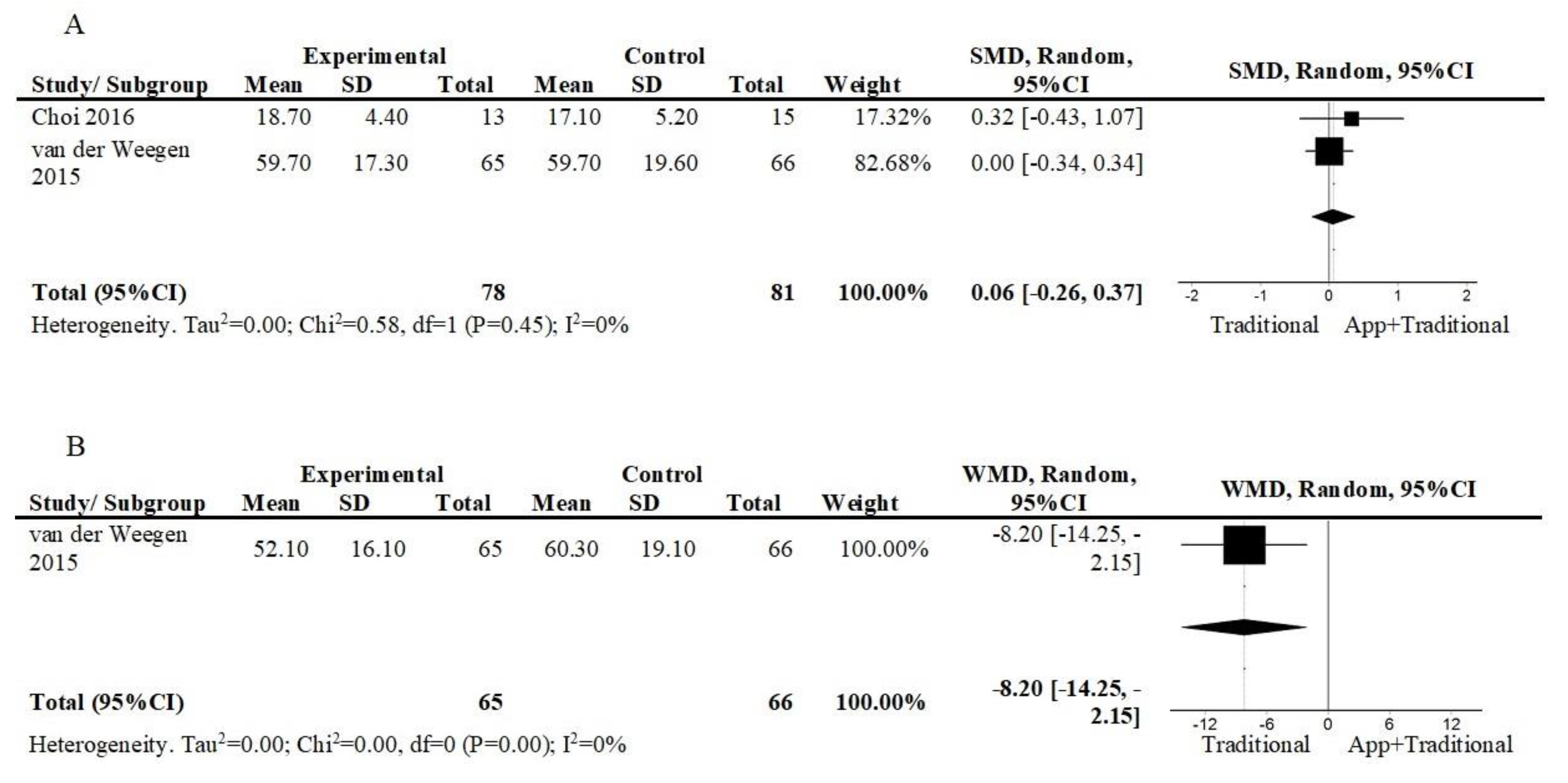
3.5.2. Self-efficacy in Exercise/Physical Activity
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Eime, R.; Young, J.; Harvey, J.; Charity, M.; Payne, W. A systematic review of the psychological and social benefits of participation in sport for children andadolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 15, 1–21. [Google Scholar]
- Loprinzi, P.; Cardinal, B.; Loprinzi, K.; Lee, H. Benefits and environmental determinants of physical activity in children and adolescents. Obes. Facts. 2012, 5, 597–610. [Google Scholar] [CrossRef] [PubMed]
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 8, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stessman, J.; Hammerman-Rozenberg, R.; Cohen, A.; Ein-Mor, E.; Jacobs, J. Physical activity, function, and longevity among the very old. Arch. Intern. Med. 2009, 169, 1476–1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogra, S.; Baker, J.; Ardern, C.I. The Role of Physical Activity and Body Mass Index in the Health Care Use of Adults With Asthma. Ann Allergy Asthma Immunol. 2009, 102, 462–468. [Google Scholar] [CrossRef]
- Jacobs, J.; Rottenberg, Y.; Cohen, A.; Stessman, J. Physical activity and health service utilization among older people. J. Am. Med. Dir. Assoc. 2013, 14, 125–129. [Google Scholar] [CrossRef]
- Christmas, C.; Andersen, R. Exercise and older patients: Guidelines for the clinician. J. Am. Geriatr. Soc. 2000, 48, 318–324. [Google Scholar] [CrossRef]
- Statista Number of Smartphone Users Worldwide from 2014 to 2020 (in Billions). Available online: https://www.researchgate.net/figure/Number-of-smartphone-users-worldwide-from-2014-to-2020-in-billions-Statista-2018i_fig3_339029096 (accessed on 20 February 2020).
- AppBrain Google Play Stas:Top Categories. Available online: https://www.appbrain.com/stats/android-market-app-categories (accessed on 20 February 2020).
- PocketGamer.biz App Store Metrics: Application Category Distribution. Available online: https://www.pocketgamer.biz/metrics/app-store/categories/ (accessed on 20 February 2020).
- Middelweerd, A.; Mollee, J.S.; van der Wal, C.N.; Brug, J.; te Velde, S.J. Apps to promote physical activity among adults: A review and content analysis. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 97. [Google Scholar] [CrossRef] [Green Version]
- Paglialonga, A.; Lugo, A.; Santoro, E. An overview on the emerging area of identification, characterization, and assessment of health apps. J. Biomed. Inform. 2018, 83, 97–102. [Google Scholar] [CrossRef]
- Khaylis, A.; Yiaslas, T.; Bergstrom, J.; Gore-Felton, C. A Review of Efficacious Technology-Based Weight-Loss Interventions: Five Key Components. Telemed. e-Health 2010, 16, 931–938. [Google Scholar] [CrossRef] [Green Version]
- Halloway, S.; Wilbur, J.; Schoeny, M.E.; Semanik, P.A.; Marquez, D.X. Combined Effects of Sedentary Behavior and Moderate-to-Vigorous Physical Activity on Cardiovascular Health in Older, Community-Dwelling Latinos. J. Aging Phys. Act. 2016, 24, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Parschau, L.; Fleig, L.; Koring, M.; Lange, D.; Knoll, N.; Schwarzer, R.; Lippke, S. Positive experience, self-efficacy, and action control predict physical activity changes: A moderated mediation analysis. Br. J. Health Psychol. 2013, 18, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Fernández, B.R.; Montenegro, E.M.; Knoll, N.; Schwarzer, R. Self-Efficacy, Action Control, and Social Support Explain Physical Activity Changes Among Costa Rican Older Adults. J. Phys. Act. Heal. 2014, 11, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Telecommunication Union About Mobile Technology and IMT-2000. Available online: https://www.itu.int/osg/spu/imt-2000/technology.html/ (accessed on 20 February 2020).
- Islam, M.; Islam, M.; Mazumder, T. Mobile Application and Its Global Impact. Int. J. Eng. Technol. 2010, 10, 72–78. [Google Scholar]
- Caspersen, C.; Powell, K.; Christenson, G. Physical activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Heal. Rep. 1985, 100, 126–131. [Google Scholar]
- Vanhees, L.; Lefevre, J.; Philippaerts, R.; Martens, M.; Huygens, W.; Troosters, T.; Beunen, G. How to assess physical activity? How to assess physical fitness? J. Cardiovasc. Prev. Rehabil. 2005, 12, 102–114. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.W.; de Bie, R.A.; Kessels, A.G.H.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.; Sherrington, C.; Herbert, R.; Moseley, A.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized. Phys Ther 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Volume Second Edi; Lawrence Erlbaum Associates: New York, NY, USA, 1988; ISBN 0805802835. [Google Scholar]
- Cochran, W.G. The Combination of Estimates from Different Experiments. Biometrics 1954, 10, 101. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.; Hill, S. How to GRADE the Quality of the Evidence (Version 3.0). Cochrane Consumers and Communication Group. 2016. Available online: http://cccrg.cochrane.org/author-re (accessed on 20 February 2020).
- Demeyer, H.; Louvaris, Z.; Frei, A.; Rabinovich, R.A.; de Jong, C.; Gimeno-Santos, E.; Loeckx, M.; Buttery, S.C.; Rubio, N.; Van der Molen, T.; et al. Physical activity is increased by a 12-week semiautomated telecoaching programme in patients with COPD: A multicentre randomised controlled trial. Thorax 2017, 72, 415–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons, E.J.; Swartz, M.C.; Lewis, Z.H.; Martinez, E.; Jennings, K. Feasibility and Acceptability of a Wearable Technology Physical Activity Intervention With Telephone Counseling for Mid-Aged and Older Adults: A Randomized Controlled Pilot Trial. JMIR mHealth uHealth 2017, 5, e28. [Google Scholar] [CrossRef]
- Paul, L.; Wyke, S.; Brewster, S.; Sattar, N.; Gill, J.M.R.; Alexander, G.; Rafferty, D.; McFadyen, A.K.; Ramsay, A.; Dybus, A. Increasing physical activity in stroke survivors using STARFISH, an interactive mobile phone application: A pilot study. Top. Stroke Rehabil. 2016, 23, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Plotnikoff, R.C.; Wilczynska, M.; Cohen, K.E.; Smith, J.J.; Lubans, D.R. Integrating smartphone technology, social support and the outdoor physical environment to improve fitness among adults at risk of, or diagnosed with, Type 2 Diabetes: Findings from the ‘eCoFit’ randomized controlled trial. Prev. Med. (Baltim). 2017, 105, 404–411. [Google Scholar] [CrossRef]
- Tabak, M.; Vollenbroek-Hutten, M.M.; van der Valk, P.D.; van der Palen, J.; Hermens, H.J. A telerehabilitation intervention for patients with Chronic Obstructive Pulmonary Disease: A randomized controlled pilot trial. Clin. Rehabil. 2014, 28, 582–591. [Google Scholar] [CrossRef]
- Uhm, K.E.; Yoo, J.S.; Chung, S.H.; Lee, J.D.; Lee, I.; Kim, J.I.; Lee, S.K.; Nam, S.J.; Park, Y.H.; Lee, J.Y.; et al. Effects of exercise intervention in breast cancer patients: Is mobile health (mHealth) with pedometer more effective than conventional program using brochure? Breast Cancer Res. Treat. 2017, 161, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Van der Weegen, S.; Verwey, R.; Spreeuwenberg, M.; Tange, H.; van der Weijden, T.; de Witte, L. It’s LiFe! Mobile and Web-Based Monitoring and Feedback Tool Embedded in Primary Care Increases Physical Activity: A Cluster Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e184. [Google Scholar] [CrossRef] [Green Version]
- Vorrink, S.N.W.; Kort, H.S.M.; Troosters, T.; Zanen, P.; Lammers, J.-W.J. Efficacy of an mHealth intervention to stimulate physical activity in COPD patients after pulmonary rehabilitation. Eur. Respir. J. 2016, 48, 1019–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rospo, G.; Valsecchi, V.; Bonomi, A.G.; Thomassen, I.W.; van Dantzig, S.; La Torre, A.; Sartor, F. Cardiorespiratory Improvements Achieved by American College of Sports Medicine’s Exercise Prescription Implemented on a Mobile App. JMIR mHealth uHealth 2016, 4, e77. [Google Scholar] [CrossRef]
- Choi, J.; Lee, J.H.; Vittinghoff, E.; Fukuoka, Y. mHealth Physical Activity Intervention: A Randomized Pilot Study in Physically Inactive Pregnant Women. Matern. Child Health J. 2016, 20, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Voth, E.C.; Oelke, N.D.; Jung, M.E. A Theory-Based Exercise App to Enhance Exercise Adherence: A Pilot Study. JMIR mHealth uHealth 2016, 4, e62. [Google Scholar] [CrossRef] [PubMed]
- GRADE working Group Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [CrossRef] [PubMed] [Green Version]
- Muellmann, S.; Forberger, S.; Möllers, T.; Bröring, E.; Zeeb, H.; Pischke, C.R. Effectiveness of eHealth interventions for the promotion of physical activity in older adults: A systematic review. Prev. Med. (Baltim.) 2018, 108, 93–110. [Google Scholar] [CrossRef]
- Bossen, D.; Veenhof, C.; Dekker, J.; de Bakker, D. The Effectiveness of Self-Guided Web-Based Physical Activity Interventions Among Patients With a Chronic Disease: A Systematic Review. J. Phys. Act. Heal. 2014, 11, 665–677. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence—indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef]

 —Low risk of bias;
—Low risk of bias;  —high risk of bias;
—high risk of bias;  —Unclear risk of bias.
—Low risk of bias; —high risk of bias; —Unclear risk of bias.
—Unclear risk of bias.
—Low risk of bias; —high risk of bias; —Unclear risk of bias.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | 1 * | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Choi et al. [39] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7/10 |
| Demeyer et al. [30] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6/10 |
| Lyons et al. [31] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7/10 |
| Paul et al. [32] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5/10 |
| Plotnikoff et al. [33] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 5/10 |
| Rospo et al. [38] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 2/10 |
| Tabak et al. [34] | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 4/10 |
| Uhm et al. [35] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 3/10 |
| van der Weegen et al. [36] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7/10 |
| Vorrink et al. [37] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 5/10 |
| Voth et al. [40] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4/10 |
| Quality Assessment | Number of Participants | Effect Size | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Outcome | Studies (n) | Design | Risk of bias | Inconsistency | Indirectness | Imprecision | App/App+ traditional | No/traditional intervention | Absolute (95% CI) | Quality |
| Number of steps short term (app/app+traditional vs. no intervention) | 3 | 2 RCT+ 1 Quasi-RCT | Serious * | Not serious | Serious † | Serious ‡ | 77 | 70 | WMD 157.04 [454.70, 2703.38] | +ooo Very low |
| Number of steps short term (app/app+traditional vs. traditional) | 5 | 4 RCT+ 1 Quasi-RCT | Serious * | Not serious | Serious † | Not serious | 243 | 247 | WMD 665.96 [167.92, 1164.00] | ++oo Low |
| Number of steps follow-up (app+traditional vs. traditional) | 1 | RCT | Serious * | Not serious | Not serious | Serious ‡ | 62 | 59 | WMD −140.00 [−1087.93, 807.93] | ++oo Low |
| Minutes in MVPA short term | 1 | RCT | Not serious | Not serious | Serious † | Serious ‡ | 65 | 66 | WMD 1.88 [−7.54, 11.30] | ++oo Low |
| Minutes in MVPA follow-up | 1 | RCT | Not serious | Not serious | Serious † | Serious ‡ | 65 | 66 | WMD 3.48 [−6.03, 12.99] | ++oo Low |
| Self-reported PA short term | 2 | 1 RCT+ 1 Quasi-RCT | Serious * | Serious § | Not serious | Serious ‡ | 182 | 191 | SMD 0.35 [−0.11, 0.81] | +ooo Very low |
| Sedentarism short term (app vs. no intervention) | 2 | 1 RCT+ 1 Quasi-RCT | Serious * | Not serious | Not serious | Serious ‡ | 35 | 28 | SMD −0.35 [−0.86, 0.15] | +ooo Very low |
| Sedentarism short term (app+traditional vs. traditional) | 1 | RCT | Not serious | Not serious | Serious † | Serious ‡ | 13 | 15 | WMD −7.10 [−22.66, 8.46] | ++oo Low |
| Self-efficacy—short term | 2 | RCT | Not serious | Not serious | Serious † | Serious ‡ | 78 | 81 | SMD 0.06 [−0.26, 0.37] | ++oo Low |
| Self-efficacy—follow-up | 1 | RCT | Not serious | Not serious | Not serious | Serious ‡ | 65 | 66 | WMD −8.20 [−14.25, 2.15] | ++oo Low |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, A.G.; Simões, P.; Queirós, A.; P Rocha, N.; Rodrigues, M. Effectiveness of Mobile Applications Running on Smartphones to Promote Physical Activity: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2251. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072251
Silva AG, Simões P, Queirós A, P Rocha N, Rodrigues M. Effectiveness of Mobile Applications Running on Smartphones to Promote Physical Activity: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(7):2251. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072251
Chicago/Turabian StyleSilva, Anabela G., Patrícia Simões, Alexandra Queirós, Nelson P Rocha, and Mário Rodrigues. 2020. "Effectiveness of Mobile Applications Running on Smartphones to Promote Physical Activity: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 7: 2251. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072251