Social Relations, Community Engagement and Potentials: A Qualitative Study Exploring Resident Engagement in a Community-Based Health Promotion Intervention in a Deprived Social Housing Area


Abstract
:1. Introduction
Aim of the Study
- What motives do residents have for engaging in the intervention, and what do they perceive to be the outcomes of their engagement?
- What barriers and what potentials for improvement are identified in relation to resident engagement in the intervention?
2. Materials and Methods
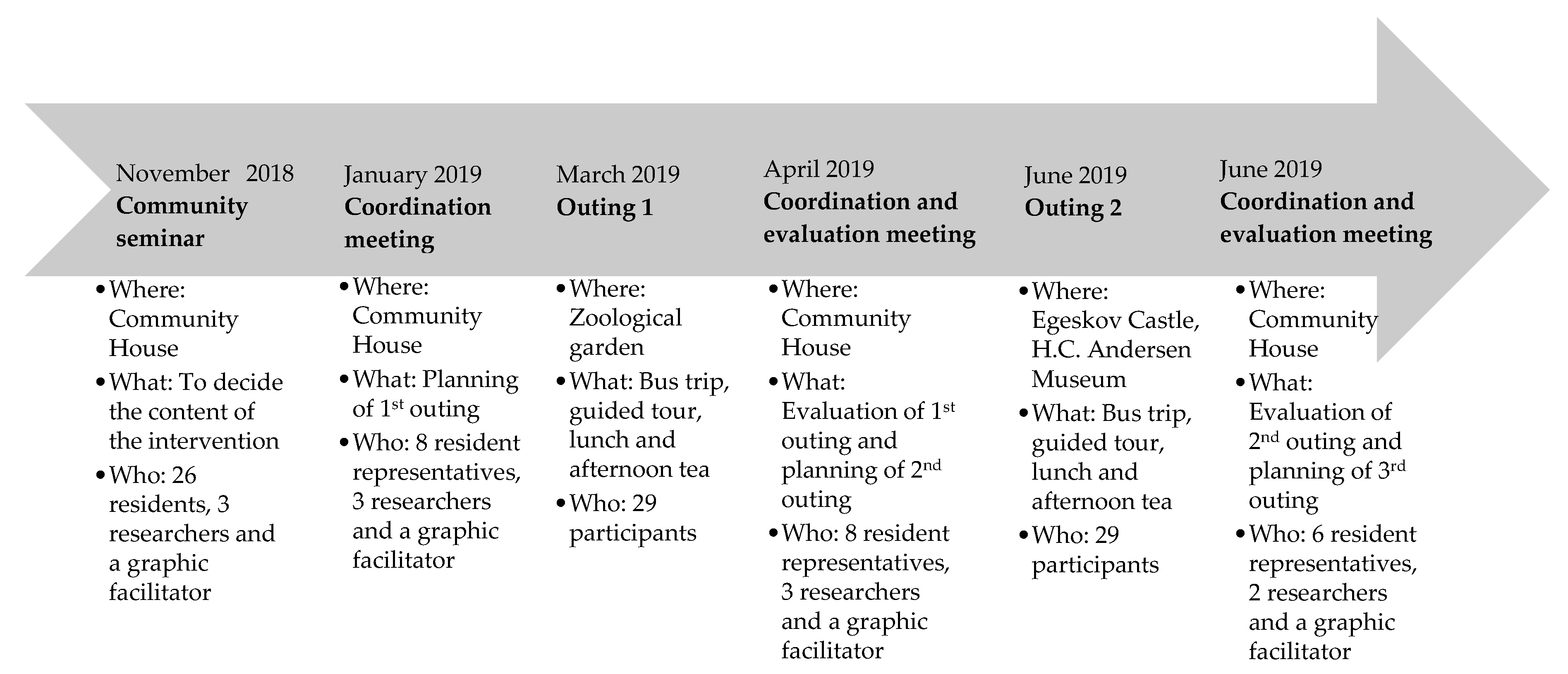
2.1. Study Setting
2.2. Selection of Participants
2.3. Data Collection
2.4. Data Analysis Procedures
2.5. Ethical Considerations
3. Results
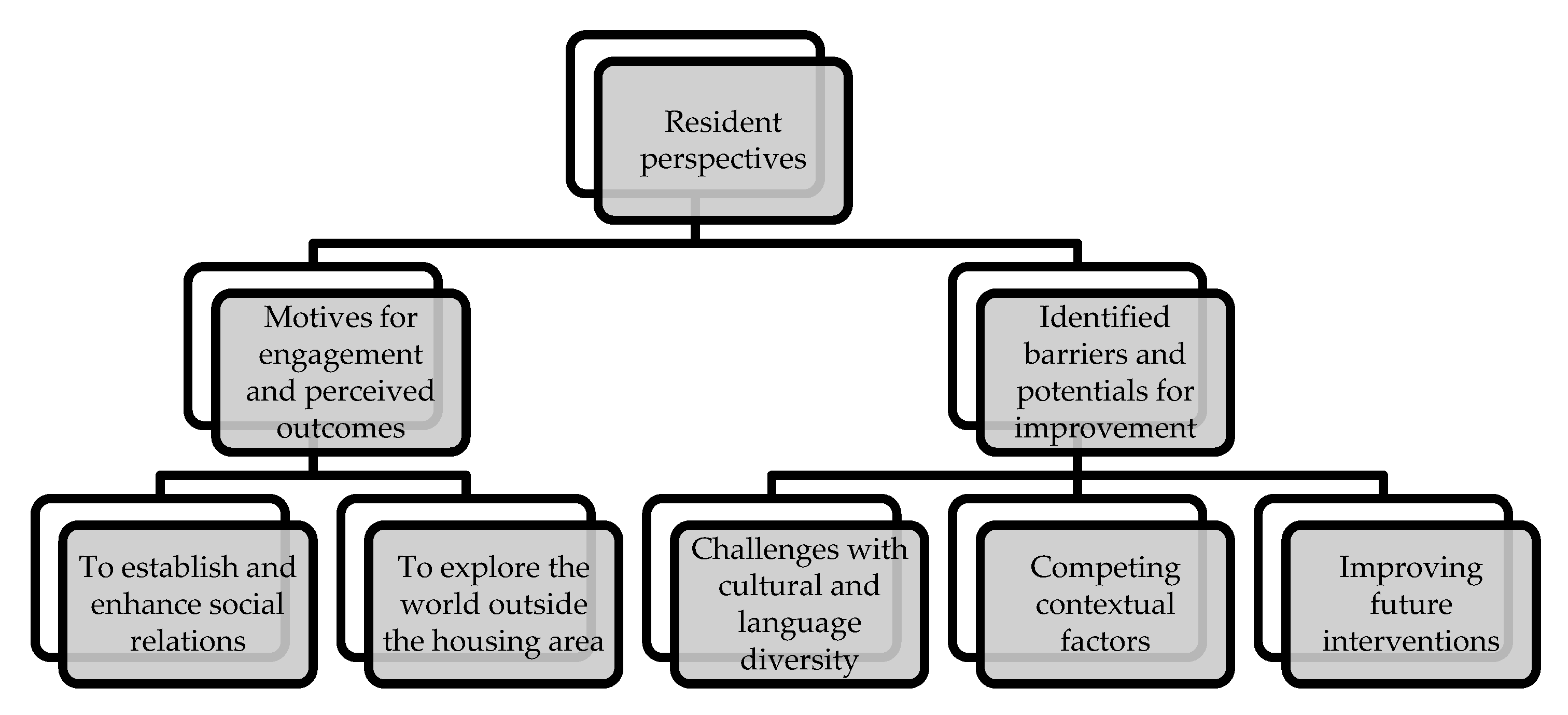
3.1. Motives for Engagement and Perceived Outcomes
3.1.1. To Establish and Enhance Social Relations
“The children are grown-ups now, and they have left home. My husband goes to work in the morning, and comes back in the evening. I am home alone during the daytime.”(Gizem)
“So I genuinely hope that I get to know new people during this outing to the zoo. I have to admit that this is the purpose of my engagement in the intervention.”(Karen)
“If we get some of the Turkish women on board, I think it will be good for us. I believe that we need to include them a little more. Also, the other migrants in this housing area.”(Rose)
“You see, Karen is also over 45, so I thought that it could be very nice if she wanted to come along. Then we could talk to each other, and get to know each other better during the outing. So, I think it is interesting that in that way people can get to know each other better.”(Vagn)
“I met one of the women from the housing area in a supermarket the other day, and she said, ‘Hello’. What is more, she opened her arms. We talked about the outing, and our opinions about it, and we agreed that it was a good outing.”(Kaj)
“I think that these outings can be a stepping-stone to make progress. But as I told you, I would probably like it if a club was set up for everyone here in this housing area.”(Lone)
3.1.2. To Explore the World Outside the Housing Area
“It is about getting out and seeing something new, instead of sitting here and staring at these four walls. And to get to experience something.”(Wilma)
“You need something to happen once in a while. You need to get a bit outside the corner down there [laughs] and experience that: ‘God, there is also a world outside this place!’ And then there is the thing about getting a break in your weekly routine. Walking around in the housing area is all very well, but you cannot avoid that it somehow affects you that every time you stare out of the window you look [whistles] directly down at the sidewalk there”.(Kaj)
“I am very excited. I love it. And, as old as I am, just as curious to try something new. I am filled with zest for life. In Turkish, we have a saying that sounds something like this: ‘It is not the people who read a lot that also know a lot, but it is the people who travel widely who know the most. You have to get out and experience new places, and process the experiences in your mind [laughs]. We need some activities that bring us out [of the housing area] and provide us with new knowledge”.(Dilara)
“So I am looking forward to getting to revisit Egeskov Castle. Because it is probably 10 to 15 years ago, since I was last there. I get the usual experience of experiencing some culture. I am also a fan of historic stuff, and I will of course enjoy experiencing that again, because I have not seen it for some time now.”(Martin)
3.2. Identified Barriers and Potentials for Improvement
3.2.1. Challenges with Cultural and Language Diversity
“The Danes did not look at us at all. I asked a woman whether she was also going on the outing, and she did not even look at me. It is as if they are afraid of us. I get this feeling. The more you try to get closer to the Danes, the more you get pushed away.”(Gizem)
“I am very doubtful about [being able to] make friends with residents of different origin. Because there was a core group of especially Turkish women who stayed by themselves. I think the ethnic Danes are more open to talking with other people. I am at least open to talking with other people. But it seems as if they [Turkish women] are a more closed circle.”(Vagn)
3.2.2. Competing Contextual Factors
“I risk losing my apartment, because it might be demolished. I cannot stop thinking that I need to find a new place. I also think: why I should get involved [in this housing area]? I mean, it does not matter [if I need to move] anyway.”(Karen)
“The children and young people do not have any education in our housing area. They are involved in some sort of criminality. They [the public sector] are not protecting our young people. What do they want to do with us [older adults]? They need to take care of the young people”.(Gizem)
3.2.3. Improving Future Interventions
“We need some activities where you are able to team up with other residents, so I would be together with some female residents of Turkish origin. Then we would have to talk together. Then we would be forced to spend time together [with the others].”(Vagn)
“For the past 10 years there have been many, many interventions. However, they have always found an excuse for calling the housing area a ‘ghetto’ or giving it a bad reputation, but the housing area is not at all like that.”(Gizem)
4. Discussion
4.1. Social Relations and Community Engagement as Motives and Perceived Outcomes
4.2. Cultural and Language Diversity as Barriers to Meeting other Residents
4.3. Sustainability of the Intervention and Recommendations for Future Interventions
4.4. Methodological Considerations
4.5. Implications for Policy, Practice and Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Pemberton, S.; Humphris, R. Locality, neighbourhood and health: A literature review. In IRiS Working Paper Series No. 13; Institute for Research into Superdiversity: Birmingham, UK, 2016. [Google Scholar]
- Bonevski, B.; Randell, M.; Paul, C.; Chapman, K.; Twyman, L.; Bryant, J.; Brozek, I.; Hughes, C. Reaching the hard-to-reach: A systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med. Res. Methodol. 2014, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellaway, A.; Benzeval, M.; Green, M.; Leyland, A.; Macintyre, S. “Getting sicker quicker”: Does living in a more deprived neighbourhood mean your health deteriorates faster? Health Place 2012, 18, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, M.; Wendel-Vos, W.; van Poppel, M.; Kemper, H.; van Mechelen, W.; Maas, J. Health benefits of green spaces in the living environment: A systematic review of epidemiological studies. Urban For. Urban Green. 2015, 14, 806–816. [Google Scholar] [CrossRef]
- Cubbin, C.; LeClere, F.B.; Smith, G.S. Socioeconomic status and injury mortality: Individual and neighbourhood determinants. J. Epidemiol. Community Health 2000, 54, 517–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, M.; Poulsen, E.K.; Rytter, A.S.; Kristiansen, T.M.; Bak, C.K. Experiences with recruitment of marginalized groups in a danish health promotion program: A document evaluation study. PLoS ONE 2016, 11, e0158079. [Google Scholar] [CrossRef] [Green Version]
- Saunders, P.; Campbell, P.; Webster, M.; Thawe, M. Analysis of small area environmental, socioeconomic and health data in collaboration with local communities to target and evaluate ‘Triple win’ interventions in a deprived community in Birmingham UK. Int. J. Environ. Res. Public Health 2019, 16, 4331. [Google Scholar] [CrossRef] [Green Version]
- Skovgaard Nielsen, R.; Deichmann Haagerup, C. The Danish social housing sector: Recent changes and future challenges. Crit. Hous. Anal. 2017, 4, 142–149. [Google Scholar] [CrossRef]
- Kelaher, M.; Warr, D.J.; Feldman, P.; Tacticos, T. Living in “Birdsville”: Exploring the impact of neighbourhood stigma on health. Health Place 2010, 16, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Garthwaite, K.; Bambra, C. ‘It’s like being in Tattooville’: An ethnographic study of territorial stigma and health in a post-industrial town in the North East of England. Health Place 2018, 54, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Bender, A.M.; Kawachi, I.; Jørgensen, T.; Pisinger, C. Neighborhood deprivation is strongly associated with participation in a population-based health check. PLoS ONE 2015, 10, e0129819. [Google Scholar] [CrossRef] [PubMed]
- Srivarathan, A.; Jensen, A.N.; Kristiansen, M. Community-based interventions to enhance healthy aging in disadvantaged areas: Perceptions of older adults and health care professionals. BMC Health Serv. Res. 2019, 19, 7. [Google Scholar] [CrossRef]
- Boag-Munroe, G.; Evangelou, M. From hard to reach to how to reach: A systematic review of the literature on hard-to-reach families. Res. Pap. Educ. 2012, 27, 209–239. [Google Scholar] [CrossRef]
- Eakin, E.G.; Bull, S.S.; Glasgow, R.E.; Mason, M. Reaching those most in need: A review of diabetes self-management interventions in disadvantaged populations. Diabetes Metab. Res. Rev. 2002, 18, 26–35. [Google Scholar] [CrossRef]
- Sinclair, A.; Alexander, H.A. Using outreach to involve the hard-to-reach in a health check: What difference does it make? Public Health 2012, 126, 87–95. [Google Scholar] [CrossRef]
- Wallerstein, D. What Is the Evidence on Effectiveness of Empowerment to Improve Health? Health Evidence Network Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- Wallerstein, N.B.; Duran, B. Using Community-Based Participatory Research to Address Health Disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Liljas, A.E.M.; Walters, K.; Jovicic, A.; Iliffe, S.; Manthorpe, J.; Goodman, C.; Kharicha, K. Strategies to improve engagement of ‘hard to reach’ older people in research on health promotion: A systematic review. BMC Public Health 2017, 17, 349. [Google Scholar] [CrossRef] [Green Version]
- Teufel-Shone, N.I.; Schwartz, A.L.; Hardy, L.J.; de Heer, H.D.; Williamson, H.J.; Dunn, D.J.; Polingyumptewa, K.; Chief, C. Supporting new community-based participatory research partnerships. Int. J. Environ. Res. Public Health 2019, 16, 44. [Google Scholar] [CrossRef] [Green Version]
- Pawlowski, C.S.; Winge, L.; Carroll, S.; Schmidt, T.; Wagner, A.M.; Nørtoft, K.P.J.; Lamm, B.; Kural, R.; Schipperijn, J.; Troelsen, J. Move the Neighbourhood: Study design of a community-based participatory public open space intervention in a Danish deprived neighbourhood to promote active living. BMC Public Health 2017, 17, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cyril, S.; Smith, B.J.; Possamai-Inesedy, A.; Renzaho, A.M.N. Exploring the role of community engagement in improving the health of disadvantaged populations: A systematic review. Glob. Health Action 2015, 8, 29842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, R.; Christensen, U.; Mathisen, J.; Sørensen, K.S.; Srivarathan, A.; Molbo, D.; Halby, K.; Kristiansen, M. Health, well-being and social relations in a changing neighbourhood: Protocol for a prospective, multimethods study of the consequences of large structural changes in an ethnic diverse social housing area in Denmark. BMJ Open 2019, 9, e030936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- South, J.; Phillips, G. Evaluating community engagement as part of the public health system. J. Epidemiol. Community Health 2014, 68, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Høghøj, M. Between Utopia and Dystopia: A Socio-Cultural History of Modernist Mass Housing in Denmark, C. 1945–1985. Ph.D. Thesis, Aarhus University, Aarhus, Denmark, March 2019. [Google Scholar]
- Larsen, T.S. Copenhagen’s west end a “Paradise Lost”: The political production of territorial stigmatization in Denmark. Environ. Plan. A 2014, 46, 1386–1402. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Jensen, S.Q. Othering, identity formation and agency. Qual. Stud. 2011, 2, 63–78. [Google Scholar] [CrossRef] [Green Version]
- Wacquant, L. Territorial Stigmatization in the Age of Advanced Marginality. Thesis Elev. 2007, 91, 66–77. [Google Scholar] [CrossRef]
- Wacquant, L.; Slater, T.; Pereira, V.B. Territorial stigmatization in action. Environ. Plan. A 2014, 46, 1270–1280. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- The Government of Denmark. Ét Danmark Uden Parallelsamfund-Ingen Ghettoer I 2030; The Government of Denmark: Copenhagen, Denmark, 2018.
- Ministry of Transport and Housing. Liste over Ghettoområder Pr. 1. December 2019. Available online: https://www.trm.dk/publikationer/2019/liste-over-ghettoomraader-pr-1-december-2019/ (accessed on 6 January 2020).
- Attree, P.; French, B.; Milton, B.; Povall, S.; Whitehead, M.; Popay, J. The experience of community engagement for individuals: A rapid review of evidence. Health Soc. Care Community 2011, 19, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Hindhede, A.L. Neighbourhood renewal, participation, and social capital in deprived areas: Unintended consequences in a Nordic context. Eur. Soc. 2016, 18, 535–559. [Google Scholar] [CrossRef]
- Derges, J.; Clow, A.; Lynch, R.; Jain, S.; Phillips, G.; Petticrew, M.; Renton, A.; Draper, A. “Well London” and the benefits of participation: Results of a qualitative study nested in a cluster randomised trial. BMJ Open 2014, 4, e003596. [Google Scholar] [CrossRef]
- Salway, S.; Chowbey, P.; Such, E.; Ferguson, B. Researching health inequalities with Community Researchers: Practical, methodological and ethical challenges of an ‘inclusive’ research approach. Res. Involv. Engagem. 2015, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Kearns, A.; Parkinsion, M. The Significance of Neighbourhood. Urban Stud. 2001, 38, 2103–2110. [Google Scholar] [CrossRef]
- Romeo-Velilla, M.; Ellis, N.; Hurst, G.; Grogan, S.; Gidlow, C. A qualitative study of disengagement in disadvantaged areas of the UK: ‘You come through your door and you lock that door’. Health Place 2018, 52, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Johansen, M.L.E.; Jensen, S.B. “They want us out”: Urban regeneration and the limits of integration in the Danish welfare state. Crit. Anthropol. 2017, 37, 297–316. [Google Scholar] [CrossRef]
- Jensen, S.Q.; Christensen, A.D. Territorial stigmatization and local belonging: A study of the Danish neighbourhood Aalborg East. City 2012, 16, 74–92. [Google Scholar] [CrossRef]
- Emmel, N.; Hughes, K.; Greenhalgh, J.; Sales, A. Accessing socially excluded people-Trust and the gatekeeper in the researcher-participant relationship. Sociol. Res. Online 2007, 12, 43–55. [Google Scholar] [CrossRef] [Green Version]
- Squires, A. Methodological challenges in cross-language qualitative research: A research review. Int. J. Nurs. Stud. 2009, 46, 277–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Participant Pseudonym | Age Categories in Years | Sex | Country of Birth | Employment Status | Marital Status | Duration of Residence in the Housing Area in Years |
|---|---|---|---|---|---|---|
| Gizem | 50–59 | Female | Turkey | Unemployed | Married | 30–39 |
| Lone | 60–69 | Female | Denmark | Unemployed | Single | 10–19 |
| Karen | 50–59 | Female | Denmark | Unemployed | Single | 10–19 |
| Vagn | 70–79 | Male | Denmark | Retired | Widowed | 30–39 |
| Dilara | 60–69 | Female | Turkey | Retired | Married | 30–39 |
| Wilma | 60-69 | Female | Denmark | Retired | Single | 10–19 |
| Rose | 80–89 | Female | Denmark | Retired | Single | 20–29 |
| Kaj | 70–79 | Male | Denmark | Employed | Single | <10 |
| Martin | 60–69 | Male | Denmark | Employed | Single | 10–19 |
| Themes Explored in Participant Observations | Themes Explored in Pre-Intervention Interviews | Themes Explored in Post-Intervention Interviews |
|---|---|---|
Non-human actors and context
| Background information
| The specific intervention
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srivarathan, A.; Lund, R.; Christensen, U.; Kristiansen, M. Social Relations, Community Engagement and Potentials: A Qualitative Study Exploring Resident Engagement in a Community-Based Health Promotion Intervention in a Deprived Social Housing Area. Int. J. Environ. Res. Public Health 2020, 17, 2341. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072341
Srivarathan A, Lund R, Christensen U, Kristiansen M. Social Relations, Community Engagement and Potentials: A Qualitative Study Exploring Resident Engagement in a Community-Based Health Promotion Intervention in a Deprived Social Housing Area. International Journal of Environmental Research and Public Health. 2020; 17(7):2341. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072341
Chicago/Turabian StyleSrivarathan, Abirami, Rikke Lund, Ulla Christensen, and Maria Kristiansen. 2020. "Social Relations, Community Engagement and Potentials: A Qualitative Study Exploring Resident Engagement in a Community-Based Health Promotion Intervention in a Deprived Social Housing Area" International Journal of Environmental Research and Public Health 17, no. 7: 2341. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072341