The Night Effect of Anger: Relationship with Nocturnal Blood Pressure Dipping

 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Assessment Tools
2.2.1. Physiological Measures
2.2.2. Ambulatory Blood Pressure Monitor (ABPM)
2.2.3. Socio-Demographic and Anamnestic Information
2.2.4. Spielberger State–Trait Anger Expression Inventory (STAXI)
3. Procedure
Statistical Analyses
4. Results
4.1. Demographical, Lifestyles, and Physiological Variables
4.2. Correlations
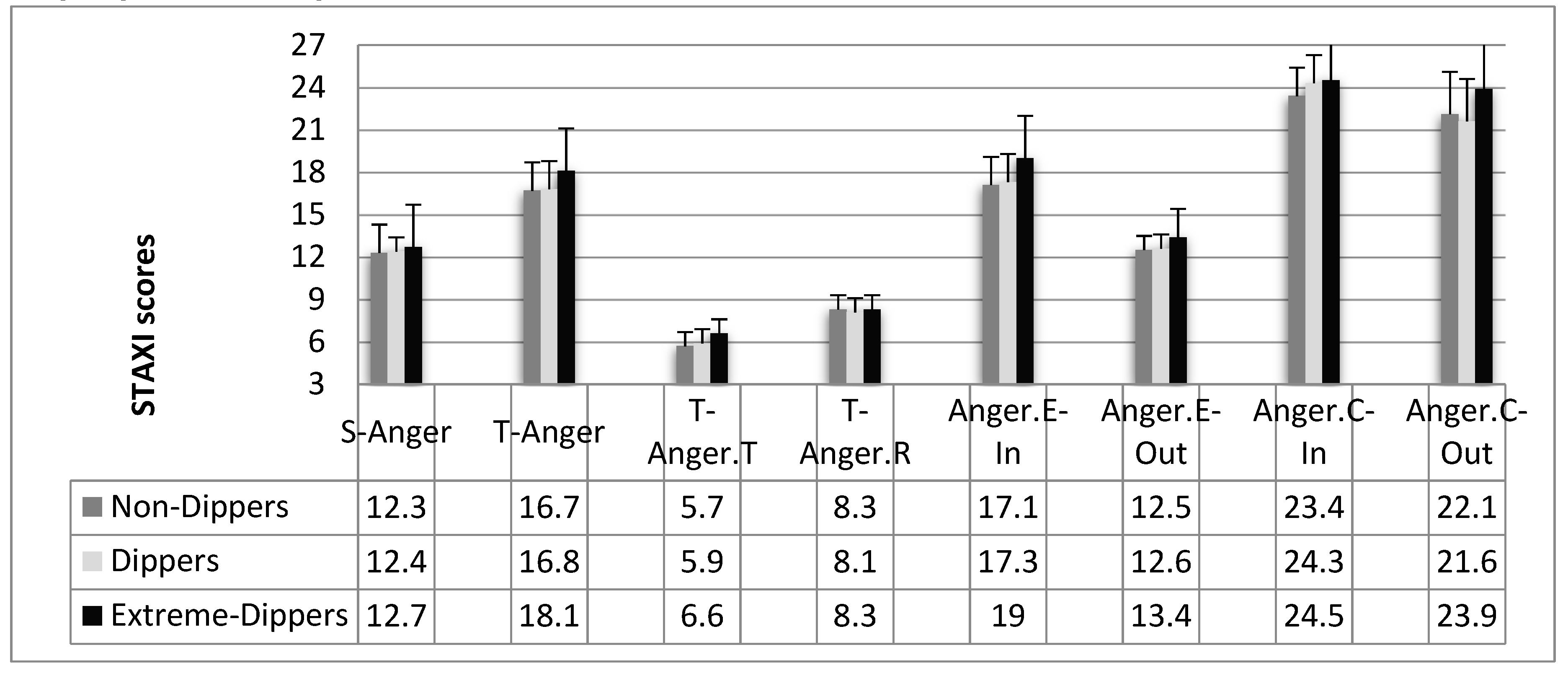
4.3. Anger
4.4. Relationship between Anger and the Dipper Phenomenon in Normotensive, Untreated, and Treated Hypertensive Participants
5. Discussion
Limits
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kario, K.; Schwartz, J.E.; Pickering, T.G. Changes of nocturnal blood pressure dipping status in hypertensives by nighttime dosing of α-adrenergic blocker, doxazosin: Results from the HALT Study. Hypertension 2000, 35, 787–794. [Google Scholar] [CrossRef] [Green Version]
- Bishop, G.D.; Pek, J.; Ngau, F. Blunted cardiovascular responses to daytime activities as related to reduced nocturnal blood pressure decline. Ann. Behav. Med. 2006, 31, 248–253. [Google Scholar] [CrossRef]
- Fagard, R.H.; Celis, H.; Thijs, L.; Staessen, J.A.; Clement, D.L.; De Buyzere, M.L.; De Bacquer, D.A. Daytime and nighttime blood pressure as predictors of death and cause-specific cardiovascular events in hypertension. Hypertension 2008, 51, 55–61. [Google Scholar] [CrossRef]
- Smolensky, M.H.; Haus, E. Circadian rhythms and clinical medicine with applications to hypertension. Am. J. Hypert. 2001, 14, 280S–290S. [Google Scholar] [CrossRef] [Green Version]
- Douma, L.G.; Gumz, M.L. Circadian clock-mediated regulation of blood pressure. Free Radic. Biol. Med. 2018, 119, 108–114. [Google Scholar] [CrossRef]
- Santilli, F.; Simeone, P.; D’ardes, D.; Davì, G. The deadly line linking sympathetic overdrive, dipping status and vascular risk: Critical appraisal and therapeutic implications. Hypertens. Res. 2016, 39, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Hermida, R.C.; Ayala, D.E.; Mojón, A.; Fernández, J.R. Influence of circadian time of hypertension treatment on cardiovascular risk: Results of the MAPEC study. Chronobiol. Int. 2010, 27, 1629–1651. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, R.; Fabbian, F. Rene e ritmi circadiani: Un nuovo mondo? G. Ital. Nefrol. 2013, 30, 1724–5590. [Google Scholar]
- O’Brien, E.; Coats, A.; Owens, P.; Petrie, J.; Padfield, P.L.; Littler, W.A.; Mee, F. Use and interpretation of ambulatory blood pressure monitoring: Recommendations of the British Hypertension Society. BMJ 2000, 320, 1128–1134. [Google Scholar] [CrossRef] [Green Version]
- Pickering, T.G.; Kario, K. Nocturnal non-dipping: What does it augur? Curr. Opin. Nephrol. Hypertens. 2001, 10, 611–616. [Google Scholar] [CrossRef]
- Sherwood, A.; Steffen, P.R.; Blumenthal, J.A.; Kuhn, C.; Hinderliter, A.L. Nighttime blood pressure dipping: The role of the sympathetic nervous system. Am. J. Hypertens. 2002, 15, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Sherwood, A.; Routledge, F.S.; Wohlgemuth, W.K.; Hinderliter, A.L.; Kuhn, C.M.; Blumenthal, J.A. Blood pressure dipping: Ethnicity, sleep quality, and sympathetic nervous system activity. Am. J. Hypertens. 2011, 24, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Sayk, F.; Becker, C.; Teckentrup, C.; Fehm, H.L.; Struck, J.; Wellhoener, J.P.; Dodt, C. To dip or not to dip: On the physiology of blood pressure decrease during nocturnal sleep in healthy humans. Hypertension 2007, 49, 1070–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakano, Y.; Oshima, T.; Ozono, R.; Higashi, Y.; Sasaki, S.; Matsumoto, T.; Kambe, M. Non-dipper phenomenon in essential hypertension is related to blunted nocturnal rise and fall of sympatho-vagal nervous activity and progress in retinopathy. Auton. Neuro 2001, 88, 181–186. [Google Scholar] [CrossRef]
- Kario, K.; Matsuo, T.; Kobayashi, H.; Imiya, M.; Matsuo, M.; Shimada, K. Nocturnal fall of blood pressure and silent cerebrovascular damage in elderly hypertensive patients: Advanced silent cerebrovascular damage in extreme dippers. Hypertension 1996, 27, 130–135. [Google Scholar] [CrossRef]
- Routledge, F.S.; McFetridge-Durdle, J.A.; Dean, C.R. Night-time blood pressure patterns and target organ damage: A review. Can. J. Cardiol. 2007, 23, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Koroboki, E.; Manios, E.; Psaltopoulou, T.; Vemmos, K.; Michas, F.; Alexaki, E.; Zakopoulos, N. Circadian variation of blood pressure and heart rate in normotensives, white-coat, masked, treated and untreated hypertensives. Hell. J. Cardiol. 2012, 53, 432–438. [Google Scholar]
- Harshfield, G.A.; Wilson, M.E.; Hanevold, C.; Kapuku, G.K.; Mackey, L.; Gillis, D.; Treiber, F.A. Impaired stress-induced pressure natriuresis increases cardiovascular load in African American youths. Am. J. Hypertens. 2002, 15, 903–906. [Google Scholar] [CrossRef] [Green Version]
- Campbell, T.S.; Séguin, J.R.; Vitaro, F.; Tremblay, R.E.; Ditto, B. Childhood socioeconomic position and blood pressure dipping in early adulthood: A longitudinal study. Ann. Behav. Med. 2013, 46, 227–231. [Google Scholar] [CrossRef]
- Barton, D.A.; Dawood, T.; Lambert, E.A.; Esler, M.D.; Haikerwal, D.; Brenchley, C.; Socratous, F.; Kaye, D.M.; Schlaich, M.P.; Hickie, I.; et al. Sympathetic activity in major depressive disorder: Identifying those at increased cardiac risk? J. Hypertens. 2007, 25, 2117–2124. [Google Scholar] [CrossRef]
- Roth, W.T.; Doberenz, S.; Dietel, A.; Conrad, A.; Mueller, A.; Wollburg, E.; Kim, S. Sympathetic activation in broadly defined generalized anxiety disorder. J. Psychiatr. Res. 2008, 42, 205–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forte, G.; Favieri, F.; Casagrande, M. Heart Rate Variability and Cognitive Function: A Systematic Review. Front. Neuros. 2019, 13, 710. [Google Scholar] [CrossRef] [PubMed]
- Forte, G.; De Pascalis, V.; Favieri, F.; Casagrande, M. Effects of Blood Pressure on Cognitive Performance: A Systematic Review. J. Clin. Med. 2020, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casagrande, M.; Boncompagni, I.; Mingarelli, A.; Favieri, F.; Forte, G.; Germanò, R.; Germanò, G.; Guarino, A. Coping styles in individuals with hypertension of varying severity. Stress Health 2019, 35, 560–568. [Google Scholar] [CrossRef]
- Casagrande, M.; Mingarelli, A.; Guarino, A.; Favieri, F.; Boncompagni, I.; Germanò, R.; Germanò, G.; Forte, G. Alexithymia: A facet of uncontrolled hypertension. Int. J. Psychophysiol. 2019, 146, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Jula, A.; Salminen, J.K.; Saarijärvi, S. Alexithymia: A facet of essential hypertension. Hypertension 1999, 33, 1057–1061. [Google Scholar] [CrossRef] [Green Version]
- Shen, B.J.; Countryman, A.J.; Spiro, A.; Niaura, R. The prospective contribution of hostility characteristics to high fasting glucose levels: The moderating role of marital status. Diabetes Care 2008, 31, 1293–1298. [Google Scholar] [CrossRef] [Green Version]
- Surtees, P.G.; Wainwright, N.W.; Khaw, K.T.; Day, N.E. Functional health status, chronic medical conditions and disorders of mood. Br. J. Psychiatry 2003, 183, 299–303. [Google Scholar] [CrossRef] [Green Version]
- Todarello, O.; Taylor, G.J.; Parker, J.D.; Fanelli, M. Alexithymia in essential hypertensive and psychiatric outpatients: A comparative study. J. Psychosom. Res. 1995, 39, 987–994. [Google Scholar] [CrossRef]
- Mezick, E.J.; Matthews, K.A.; Hall, M.; Kamarck, T.W.; Strollo, P.J.; Buysse, D.J.; Reis, S.E. Low life purpose and high hostility are related to an attenuated decline in nocturnal blood pressure. Health Psychol. 2010, 29, 196. [Google Scholar] [CrossRef] [Green Version]
- Thomas, K.S.; Nelesen, R.A.; Dimsdale, J.E. Relationships between hostility, anger expression, and blood pressure dipping in an ethnically diverse sample. Psychosom. Med. 2004, 66, 298–304. [Google Scholar] [PubMed] [Green Version]
- Tomfohr, L.; Pung, M.A.; Edwards, K.M.; Dimsdale, J.E. Racial differences in sleep architecture: The role of ethnic discrimination. Biol. Psychol. 2012, 89, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, L.B.; Blumenthal, J.A.; Hinderliter, A.L.; Sherwood, A. The effect of job strain on nighttime blood pressure dipping among men and women with high blood pressure. Scand. J. Work Environ. Health 2013, 39, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kario, K.; Pickering, T.G.; Matsuo, T.; Hoshide, S.; Schwartz, J.E.; Shimada, K. Stroke prognosis and abnormal nocturnal blood pressure falls in older hypertensives. Hypertension 2001, 38, 852–857. [Google Scholar] [CrossRef] [Green Version]
- Troxel, W.M.; Buysse, D.J.; Monk, T.H.; Begley, A.; Hall, M. Does social support differentially affect sleep in older adults with versus without insomnia? J. Psychosom. Res. 2010, 69, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Linden, W.; Klassen, K.; Phillips, M. Can psychological factors account for a lack of nocturnal blood pressure dipping? Ann. Behav. Med. 2008, 36, 253–258. [Google Scholar] [CrossRef]
- Germanò, G.; Psimenos, A.; Sarullo, F.; Venditti, A.; Pecchioli, V.; Asmar, R. Validation of four automatic devices for self-measurement of blood pressure according to the International Protocol: The Pic Indolor Personal Check, Comfort Check, My Check and Travel Check. Blood Press. 2009, 18, 15–23. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Boehm, M.; Galderisi, M. 2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press. 2013, 22, 193–278. [Google Scholar] [CrossRef] [Green Version]
- Risk, N.C.D. Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- O’Brien, E.; Asmar, R.; Beilin, L.; Imai, Y.; Mancia, G.; Mengden, T.; Pickering, T. Practice guidelines of the European Society of Hypertension for clinic, ambulatory and self blood pressure measurement. J. Hypertens. 2005, 23, 697–701. [Google Scholar]
- Loredo, J.S.; Nelesen, R.; Ancoli-Israel, S.; Dimsdale, J.E. Sleep quality and blood pressure dipping in normal adults. Sleep 2004, 27, 1097–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, E.D.; Ruoff, B.E. Commonly used formulas and calculations. In Clinical Procedures in Emergency Medicine; Elsevier: Amsterdam, The Netherlands, 2004; pp. 1333–1343. [Google Scholar]
- Spielberger, C.D. State-Trait anxiety inventory. In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Comunian, A.L.; Spielberger, C.D. STAXI, State-Trait Anger Expression Inventory: Manuale. Firenze: O.S. Organizzazioni Speciali; Giunti O.S.: Firenze, Italy, 1992. [Google Scholar]
- Schum, J.L.; Jorgensen, R.S.; Verhaeghen, P.; Sauro, M.; Thibodeau, R. Trait anger, anger expression, and ambulatory blood pressure: A meta-analytic review. J. Behav. Med. 2003, 26, 395–415. [Google Scholar] [CrossRef] [PubMed]
- Pavek, K.; Taube, A. Personality characteristics influencing determinacy of day and night blood pressure and heart rate. Blood Press. 2009, 18, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Helmers, K.F.; Baker, B.; O’kelly, B.; Tobe, S. Anger expression, gender, and ambulatory blood pressure in mild, unmedicated adults with hypertension. Ann. Behav. Med. 2000, 22, 60–64. [Google Scholar] [CrossRef]
- Fagard, R.H.; Thijs, L.; Staessen, J.A.; Clement, D.L.; De Buyzere, M.L.; De Bacquer, D.A. Night–day blood pressure ratio and dipping pattern as predictors of death and cardiovascular events in hypertension. J. Hum. Hypertens. 2009, 23, 645. [Google Scholar] [CrossRef] [Green Version]
- Cuspidi, C.; Tadic, M.; Sala, C. Targeting Nocturnal Hypertension: The Emerging Role of Home Blood Pressure. Am. J. Hypertens. 2019, 32, 727–729. [Google Scholar] [CrossRef]
- Palatini, P.; Saladini, F.; Mos, L.; Fania, C.; Mazzer, A.; Cozzio, S.; Zanata, G.; Garavelli, G.; Biasion, T.; Spinella, P.; et al. Short-term blood pressure variability outweighs average 24-h blood pressure in the prediction of cardiovascular events in hypertension of the young. J. Hypertens. 2019, 37, 1419–1426. [Google Scholar] [CrossRef]
- Pierdomenico, S.D.; Pierdomenico, A.M.; Coccina, F.; Lapenna, D.; Porreca, E. Circadian blood pressure changes and cardiovascular risk in elderly-treated hypertensive patients. Hypertens. Res. 2016, 39, 805–811. [Google Scholar] [CrossRef]
- Fujiwara, T.; Tomitani, N.; Sato, K.; Okura, A.; Suzuki, N.; Kario, K. The relationship between a blunted morning surge and a reversed nocturnal blood pressure dipping or “riser” pattern. J. Clin. Hypertens. 2017, 19, 1108–1114. [Google Scholar] [CrossRef] [Green Version]
- Steele, M.S.; Mcgarvey, S.T. Anger expression, age, and blood pressure in modernizing Samoan adults. Psychosom. Med. 1997, 59, 632–637. [Google Scholar] [CrossRef]
- Sullman, M.J. The expression of anger on the road. Saf. Sci. 2015, 72, 153–159. [Google Scholar] [CrossRef]
- Phillips, L.H.; Henry, J.D.; Hosie, J.A.; Milne, A.B. Age, anger regulation and well-being. Aging Ment. Health 2006, 10, 250–256. [Google Scholar] [CrossRef]
- Dubielski, Z.; Zamojski, M.; Wiechecki, B.; Możeńska, O.; Petelczyc, M.; Kosior, D.A. The current state of knowledge about the dipping and non-dipping hypertension. Arter. Hypertens. 2016, 20, 33–43. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Bliziotis, I.A. Home blood pressure monitoring in the diagnosis and treatment of hypertension: A systematic review. Am. J. Hypertens. 2011, 24, 123–134. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, L.; Ottaviani, C.; Goldstein, I.B.; Shapiro, D. Effects of dipping and psychological traits on morning surge in blood pressure in healthy people. J. Hum. Hypertens. 2012, 26, 228. [Google Scholar] [CrossRef] [PubMed]
- Kayano, H.; Koba, S.; Matsui, T.; Fukuoka, H.; Toshida, T.; Sakai, T.; Kobayashi, Y. Anxiety disorder is associated with nocturnal and early morning hypertension with or without morning surge. Circ. J. 2012, 1204031677. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Non-Dippers | Dippers | Extreme Dippers | F | p | |
|---|---|---|---|---|---|
| N (Womem/Men) | 42 (22/20) | 65 (36/29) | 44 (26/18) | ||
| Age | 60 (8.74) | 56 (10.38) | 55 (8.76) | 3.35 | 0.04 |
| Years of Education | 11.64 (3.33) | 12.66 (3.95) | 13.41 (4.56) | 1.93 | 0.15 |
| Smoking Cigarettes (number per day) | 0.21 (0.57) | 0.54 (0.90) | 0.27 (0.58) | 3.09 | 0.05 |
| Alcohol’s Consumption (number per day) | 0.30 (0.46) | 0.37 (0.52) | 0.34 (0.52) | 0.24 | 0.79 |
| Body Mass Index (BMI) | 27.07 (5.19) | 25.81 (4.33) | 26.43 (3.87) | 1.02 | 0.36 |
| Systolic Blood Pressure | 140.21 (25.73) | 142.03 (19.04) | 141.70 (14.81) | 0.11 | 0.89 |
| Diastolic Blood Pressure | 89.58 (12.88) | 91.48 (12.15) | 92.63 (9.66) | 0.75 | 0.48 |
| Diurnal Mean Arterial Pressure (MAP) | 96.21 (10.59) | 97.78 (8.79) | 100.86 (7.32) | 3.04 | 0.05 |
| Nocturnal Mean Arterial Pressure Night | 90.85 (10.02) | 82.77 (7.20) | 75.57 (5.61) | 42.46 | 0.0001 |
| Night/Day MAP ratio | 0.95 (0.03) | 0.85 (0.03) | 0.75 (0.04) | 416.1 | 0.0001 |
| Normotensive Participants, N (%) | 9 (21.4%) | 9 (13.8%) | 7 (16.0%) | ||
| Hypertensive Untreated Participants, (N (%) | 7 ab (16.7%) | 21 (32.4%) | 20 (45.4%) | ||
| Hypertensive Treated Participants, (N (%) | 26 a (61.9%) | 35 (53.8%) | 17 (38.6%) |
| (1) | (2) | (3) | (4) | (5) | (6) | |
|---|---|---|---|---|---|---|
| (1) Age | — | |||||
| (2) Years of Education | −0.14 | — | ||||
| (3) BMI | 0.01 | −0.15 | — | |||
| (4) Smoking Cigarettes | −0.03 | −0.04 | −0.12 | — | ||
| (5) Alcohol Consumption | −0.17 * | 0.08 | −0.02 | 0.19 * | — | |
| (6) Night/Day MAP Ratio | 0.21 ** | −0.12 | 0.05 | −0.02 | −0.01 | — |
| (7) T.Anger | −0.28 *** | −0.14 | 0.10 | 0.07 | 0.05 | −0.18 * |
| (8) T-Anger.T | −0.24 ** | −0.10 | 0.03 | 0.13 | 0.002 | −0.23 ** |
| (9) T-Anger.R | −0.19 * | −0.15 | 0.12 | 0.004 | 0.07 | −0.05 |
| (10) Anger.E-In | −0.17 * | 0.19 * | 0.03 | 0.09 | −0.07 | −0.18 * |
| (11) Anger.E-Out | −0.19 * | −0.11 | 0.14 | 0.10 | 0.02 | −0.13 |
| (12) Anger.C-In | 0.01 | 0.13 | 0.175 | −0.09 | −0.12 | −0.04 |
| (13) Anger.C-Out | −0.16 * | −0.03 | −0.05 | 0.15 | 0.05 | −0.12 |
| Non-Dippers | Dippers | Extreme Dippers | F | p | |
|---|---|---|---|---|---|
| STAXI | |||||
| S-Anger | 12.28 (3.92) | 12.39 (3.28) | 12.70 (4.99) | 0.13 | 0.88 |
| T-Anger | 16.66 (3.80) | 16.78 (4.34) | 18.12 (4.96) | 1.56 | 0.21 |
| T-Anger.T | 5.67 (1.68) | 5.89 (1.63) | 6.64 (2.39) | 3.19 | 0.04 |
| T-Anger.R | 8.26 (2.64) | 8.12 (2.86) | 8.32 (2.83) | 0.07 | 0.93 |
| Anger.E-In | 17.07 (4.09) | 17.26 (3.99) | 19.03 (4.81) | 2.04 | 0.05 |
| Anger.E-Out | 12.52 (2.80) | 12.61 (3.11) | 13.41 (3.88) | 1.12 | 0.33 |
| Anger.C-In | 23.44 (6.26) | 24.33 (5.53) | 24.51 (5.35) | 0.44 | 0.64 |
| Anger.C-Out | 22.15 (7.94) | 21.55 (7.74) | 23.93 (8.92) | 1.15 | 0.32 |
| Non-Dippers | Dippers | Extreme Dippers | χ2 | p | |
|---|---|---|---|---|---|
| Normotensive Participants | |||||
| S-Anger | 11.22 (1.30) | 12.89 (3.02) | 14.57 (9.16) | <1 | 0.63 |
| T-Anger | 16.00 (3.64) | 13.67 (1.66) | 20.42 (6.26) | 6.08 | 0.04 |
| T-Anger.T | 5.67 (1.66) | 5.00 (0.50) | 8.00 (2.58) | 8.89 | 0.01 |
| T-Anger.R | 7.33 (1.87) | 5.89 (1.36) | 9.28 (2.98) | 6.08 | 0.04 |
| Anger.E-In | 16.00 (4.06) | 18.00 (2.34) | 19.14 (5.39) | 1.21 | 0.54 |
| Anger.E-Out | 13.44 (3.24) | 12.67 (2.18) | 1.85 (4.29) | 1.16 | 0.55 |
| Anger.C-In | 21.13 (6.73) | 24.52 (4.44) | 24.34 (3.54) | 2.11 | 0.34 |
| Anger.C-Out | 24.32 (8.26) | 22.14 (6.10) | 26.65 (10.17) | 2.36 | 0.31 |
| Hypertensive Untreated Participants | |||||
| S-Anger | 12.28 (3.14) | 12.09 (3.59) | 12.06 (2.58) | <1 | 0.73 |
| T-Anger | 18.14 (5.58) | 16.61 (4.62) | 18.87 (5.38) | 4.27 | 0.11 |
| T-Anger.T | 6.57 (2.63) | 6.19 (1.43) | 6.70 (2.45) | <1 | 0.98 |
| T-Anger.R | 8.57 (3.31) | 7.76 (3.19) | 8.65 (3.01) | 4.41 | 0.11 |
| Anger.E-In | 15.29 (1.60) | 16.46 (3.58) | 19.38 (5.26) | 5.42 | 0.06 |
| Anger.E-Out | 12.43 (3.05) | 13.57 (3.66) | 13.30 (3.76) | <1 | 0.68 |
| Anger.C-In | 21.28 (8.09) | 23.17 (5.21) | 24.05 (6.43) | <1 | 0.82 |
| Anger.C-Out | 22.43 (11.76) | 22.85 (7.91) | 24.63 (8.66) | <1 | 0.90 |
| Hypertensive Treated Participants | |||||
| S-Anger | 12.65 (4.66) | 12.43 (3.21) | 12.71 (5.05) | 2.45 | 0.29 |
| T-Anger | 16.49 (3.34) | 17.68 (4.33) | 16.29 (3.22) | 1.19 | 0.54 |
| T-Anger.T | 5.42 (1.33) | 5.94 (1.86) | 6.00 (2.12) | <1 | 0.88 |
| T-Anger.R | 8.50 (2.70) | 8.91 (2.68) | 7.52 (2.48) | 7.24 | 0.02 |
| Anger.E-In | 17.92 (4.43) | 17.55 (4.54) | 18.59 (4.26) | <1 | 0.94 |
| Anger.E-Out | 12.23 (2.63) | 12.03 (1.87) | 12.53 (3.64) | <1 | 0.84 |
| Anger.C-In | 24.83 (5.37) | 24.97 (5.96) | 25.11 (4.74) | 1.77 | 0.41 |
| Anger.C-Out | 21.32 (6.79) | 20.61 (8.07) | 22.00 (8.86) | <1 | 0.87 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casagrande, M.; Favieri, F.; Guarino, A.; Di Pace, E.; Langher, V.; Germanò, G.; Forte, G. The Night Effect of Anger: Relationship with Nocturnal Blood Pressure Dipping. Int. J. Environ. Res. Public Health 2020, 17, 2705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082705
Casagrande M, Favieri F, Guarino A, Di Pace E, Langher V, Germanò G, Forte G. The Night Effect of Anger: Relationship with Nocturnal Blood Pressure Dipping. International Journal of Environmental Research and Public Health. 2020; 17(8):2705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082705
Chicago/Turabian StyleCasagrande, Maria, Francesca Favieri, Angela Guarino, Enrico Di Pace, Viviana Langher, Giuseppe Germanò, and Giuseppe Forte. 2020. "The Night Effect of Anger: Relationship with Nocturnal Blood Pressure Dipping" International Journal of Environmental Research and Public Health 17, no. 8: 2705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082705